Ultrasound guided transversus abdominis plane (TAP) block is better than local wound infiltration for postoperative pain management in inguinal hernia repair
Abstract
Background & Objective:
Transversus abdominis plane (TAP) block has been shown to provide good postoperative pain relief following various abdominal and inguinal surgeries. We evaluated the effectiveness of ultrasound guided TAP block against conventional local anesthetic wound infiltration for better postoperative analgesia in patients undergoing inguinal hernia repair.
Methodology:
This prospective randomized controlled study was conducted after approval from ethical review board. A total of 100 adult male patients, American Society of Anesthesiologists (ASA) physical status 1 or 2 were randomized either to Group I (TAP) (n = 50) receiving ultrasound guided TAP block with 0.5% bupivacaine 1.5 mg/kg or Group II (LAI) (n = 50) receiving similar dose as conventional local anesthetic wound infiltration. Inj. tramadol was used as rescue analgesic if needed. Pain score was recorded by visual analogue scale (VAS) on emergence, then 2 hourly for 8 hours followed by 4 hourly for 24 hours postoperatively. Mean pain score, total dose of rescue analgesic/24 hours and procedure related complications, including postoperative nausea / vomiting, were recorded.
Results:
There was no significant difference between the baseline characteristics of both groups. Mean pain scores in Group I (TAP) and II (LAI) were 2.1 ± 1.2 and 4.8 ± 1.5 respectively (P < 0.001) and corresponding opiate requirement was significantly less in Group I (TAP) 17.2 ± 68.4 mg of tramadol vs 136.4 ± 86.3mg of tramadol in Group II (LAI) (P < 0.001). Nausea / vomiting were observed in 21.7 vs. 78.3% of patients in Group I (TAP) and Group II (LAI) respectively. No procedure related complications were noted in any patient.
Conclusion:
Ultrasound guided TAP block is found to be safe and an effective modality of providing postoperative analgesia with significantly less post-operative nausea vomiting and opiate requirement when compared to local anesthetic wound infiltration.
Key words: Pain; PONV; Local anesthesia; Postoperative pain
Citation:
Talib MT, Sikander RI, Ahsan MF. Ultrasound guided transversus abdominis plane (TAP) block is better than local wound infiltration for postoperative pain management in inguinal hernia repair. Anaesth Pain & Intensive Care 2015;19(4)-
INTRODUCTION
Pain is the most common symptom to compel a patient to seek medical opinion. To alleviate postoperative pain is the responsibility of primary care team to make the patient comfortable and to decrease the morbidities associated with prolong hospital stay or prevent it from converting into chronic pain.[1]
Pain was labeled as the “fifth vital sign” by American Pain Society in 1995.[2],[3] Around 40-60% patients experience moderate to severe postoperative pain costing 100 billion dollars in American health care system each year.[4]–[5]
Local anesthetic infiltration at the site of surgery has been one of the most commonly used modality for postoperative pain relief.[6]It has evolved technically into the nerve blocks with more defined anatomical localization and relatively precise infiltration. It may relieve postoperative pain for up to 24 hours.[7]
Transversus abdominis plane (TAP) block is a regional anesthesia technique that provides analgesia by blocking neural afferents to the parietal peritoneum, skin and muscles of the anterior abdominal wall.[8] It involves blocking T6-L1 mid/lower thoracic and upper lumbar spinal [ilioinguinal (IIN) / illiohypogastric (IHN)] nerves travelling in the plane between internal oblique and transversus abdominis muscle.
Traditional landmark approach (i.e. triangle of Petit) of TAP block was first described by Kuppuvelumani et al.[9] in 1993 while formally documented by Rafi in 2001.[10] Hebbard et al. in 2007 subsequently described an ultrasound-guided approach to the TAP block.[11] It has been found to be an effective and safe postoperative adjunct analgesia technique in a variety of general, gynecological, urological , plastic and pediatric surgeries.[12],[13],[14],[15],[16]
Our literature search did not reveal any study on the use of TAP block for post-operative analgesia in Pakistan although there was one case report on its use for surgery in a high risk patient.[17] The objective of this study was to determine the effectiveness of ultrasound guided transversus abdominis plane (TAP) block in comparison to conventional local anesthetic infiltration (LAI) technique in postoperative pain management after lower abdominal surgery.
METHODOLOGY
This randomized controlled study (RCT) was carried out over a period of six months from June 2014 to Dec 2014 in Anesthesia department of PIMS, a tertiary care hospital in Islamabad where 500 inguinal herniorhapphies are performed annually. WHO sample size calculator was used for sample size calculation with 95% confidence interval and absolute precision of 0.09. Calculated sample size (n) was 97.4 After due approval from ethical review board and written consent, 100 male patients (female were excluded to control the confounding factor as male to female ratio in inguinal hernia is 10:1 and even very few report to hospital in our society) with ASA (American Society of Anesthesiologist) physical status of I-II, 12 to 80 yrs of age with diagnosis of inguinal hernia, planned for unilateral repair were included in the study. All the patients, fasting < 6 hours, coagulopathies, renal insufficiency, congestive heart failure, contraindications to local anesthetic, chronic opioid dependence, drug addictions and BMI >30 kg/m 2 were excluded. Patients were divided into two groups, randomized by lottery method. Group I received ultrasound guided TAP block and Group II received local anesthetic wound infiltration, 50 patients in each group. For the purpose of study and to control confounding factors all patients underwent general anesthesia, co-induction with 1mg of Midazolam, 1.5 µg/kg of Fentanyl and Propofol 2-2.5 mg/kg intravenously and maintained with inhaled anesthetics (Sevoflurane) in 50 % oxygen with air. Airway was maintained with Laryngeal Mask Airway (LMA) and mechanical ventilation was continued on Continuous mandatory ventilation (CMV) mode. Morphine 0.1 mg/kg was given before incision. 1gm infusion paracetamol with diclofenac 75 mg intravenous was given per-operatively.
Group I patients received ultrasound guided TAP block immediately after completion of procedure with 1.5 mg/kg of 0.5% Bupivacaine. TAP block was done under ultrasound guidance with “Fazone CB” by Fujifilm using linear probe (7-12 MHz) oriented transversely to the anterolateral abdominal wall where the three muscle layers were most distinct. Probe was then moved postero-laterally towards the mid-axillary line just superior to iliac crest (triangle of Petit) after recognizing the plane between internal oblique and transversus abdominis muscle. The 25 G spinal needle was used as block needle, introduced anteriorly via in-plane approach, advanced under ultrasound visualization. Drug was injected; hypo-echoic deposition of injectate with hydro-dissection of transversus abdominis plane confirmed the placement.
While Group II patients received the similar dose as local anesthetic wound infiltration achieved by injecting local anesthetic in and around the wound margins using 20 ml syringe with 25 G needle. There was only one operator for the Tap block while surgeons were responsible for the Local anesthetic infiltration (LAI) in Group II. Patients were assessed for pain in recovery area (PACU) as soon they became conscious and then 2 hourly for next 8 hours and then 4 hourly up to 24 hours in wards. Pain score was calculated by Visual analogue scale (VAS) used as scale of 1 – 10 cm. For descriptive purpose and rescue analgesia, score of 0 was taken as no pain, < 3 was considered as minimal pain requiring no rescue analgesia, 3.1 – 6 was considered as moderate pain while 6.1-10 as severe pain and was treated with opiate as rescue analgesia. Average pain score of 24 hours was calculated for individual patient and then used in statistical analysis. Paracetamol 15 mg/kg 6 hourly and Diclofenac 1 mg/kg 12 hourly was given as intravenous infusion to all patients in both groups. Tramadol was used as a recuse analgesia. Tramadol was given in incremental doses of 20 mg every 10 min up to maximum 250 mg/hour and 400 mg / 24 hours in patients with moderate and severe pain. Total dose was considered mild, moderate and high when up to 100mg, 100-300 mg and greater than 300 mg respectively. Mean pain score and mean opiate dose requirement were calculated in both groups. Frequency of being nauseated or active vomiting was monitored in both groups. Patients were also monitored for any procedure (TAP & LAI) related complications. Chi square test was used for qualitative variables while Independent samples t- test was used to compare means. P value of less than or equal to 0.05 was considered statistically significant. Data were analyzed with the help of statistical software SPSS Ver.15.0.
RESULTS
Total 100 patients were included in the study, divided into two groups. Both groups had 50 patients in each. Mean age in Group I and Group II were 52.80 ± 15.27 years and 47.30 ± 15.26 years respectively (P = 0.075). Weight and ASA scores were also not statistically significant between two groups as shown in Table 1. In Group I (n =50) 92% (46) patients had minimal pain, 6% (3) patients had moderate pain and only 2% (1) patient had the severe pain when compared to 16% (8), 78% (39) and 6% (3) in group 2 respectively as shown in detail in Table 2.
PONV was seen in 21.7% (10) patient in Group I and 78.3% (36) in Group II (P < 0.001). No other procedure related complications were seen in any group.
Table 1: Patient demographic data
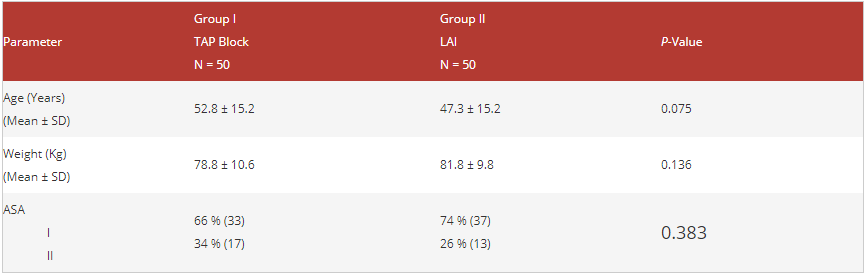
Table 2: Pain score and corresponding opiate dose required. Data given as n (%)
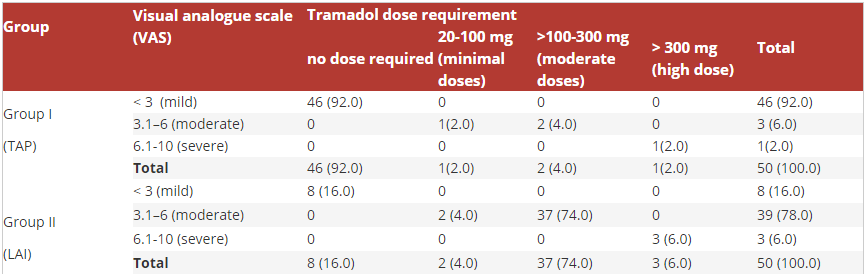
Table 3: Mean pain score and opiate requirement in 24 hours

TAP block has recently seen a great interest as an effective means of managing postoperative pain especially in lower abdominal surgeries and decreasing postoperative opioid requirement.[1] Pain has become a concern by all the specialties as it increases the length of stay of the patient in hospital and increases morbidity due to prolonged stay, immobilization, and psychological effects and nonetheless increased financial burden on healthcare system. Many pain management modalities such as LAI,12 epidural analgesia,[2] peripheral nerve block,[3] intravenous patient-controlled analgesia[4] and TAP block have been used for this purpose.[5],[6]Recent implication of different imaging modalities to pain management procedures has brought sophistication to conventional TAP block. Ultrasound guided TAP block is more and more commonly being used in lower abdominal surgeries and is described as an effective technique for reducing postoperative pain and morphine consumption after lower abdominal surgery.20,[24],[25] Meanwhile, LAI is a convenient postoperative analgesia method, which has been widely performed.[10]
Postoperative pain alleviation in terms of mean visual analogue scale (VAS) pain score and decrease in requirement of mean opioid dose was evaluated in both groups in our study. We found significantly lower pain scores in the TAP group in first 24 hours postoperatively. The results of our study are consistent with the observations by other studies in context of analgesia after inguinal hernia repair following TAP block when used in direct comparison with local anesthetic infiltration,24 adjunct to local anesthetic,[27]IIN / IHN block or used with conscious sedation for ambulatory inguinal hernia repair;[28],[29],[30] furthermore TAP block studies for other lower abdominal procedures also showed reduced pain scores when compared to LAI.14,26,27,[31]
Innervation of the anterolateral abdominal wall arises from intercostal nerves (T7-T11), the subcostal nerve (T12), and the IHN and IIN (L1). These nerves travel in transversus abdominis plane in their course of distribution. The IIN (L1) communicates with the IHN in TAP near the anterior part of the iliac crest. It supplies the upper and medial part of the thigh and part of the skin covering the genitalia. The IHN supplies the skin over the inguinal region.[32] These nerves are anesthetized when bathed with local anesthetic injected in the plane between internal oblique muscle and transversus abdominis muscle under visualization.
TAP block reduced postoperative morphine requirement and associated side effects that may be detrimental to patient’s recovery.[33] It also reduced the overall post-operative nausea and vomiting (PONV) when compared to LAI group, may be due to decrease opiates consumption. Similar results are seen in other studies reducing both 24hrs postoperative morphine requirements and PONV.28,[34],[35]
No complications related to TAP block were observed; however, TAP block associated known complications are block failure, vascular injury, abdominal visceral and nerve injuries.[36] With Ultrasound-guided TAP block Transversus abdominis plane is well located and control of needle and deposition of drug is well guided under imaging as a result lower complications and clinically significant results are seen.
Our study was limited by small sample size, specific gender and a specific procedure. The pain score observation is limited up to 24 hours post-surgery. As to our best knowledge this is the first study on TAP block from our country. It may serve as a pilot test for further studies. Furthermore Ultrasound guided TAP block is bit time consuming and operator skill dependent and has more financial impacts than the cheap, quick and simple local anesthetic wound infiltration for which its suitability has to be justified especially in our already stretched out health system.
CONCLUSION
In our experience ultrasound guided TAP block was found to be a better modality for postoperative analgesia in inguinal hernia repair. We observed major benefit with TAP block in terms of significantly decreased overall opiate requirement and associated PONV. Our results are comparable to many studies but some studies are also there with inconsistent results to this observation; perhaps large RCT’s may help.
Acknowledgment: We express our sincere gratitude to our colleagues, Head of Department and ethical review board for making it possible.
Conflict of Interest: The authors have no personal or financial conflicts of interest.
Source of Funding: There was no source of funding.
Author contribution: MTT: Study design, literature review, preparing the manuscript, clinical investigator, analyzing the data, manuscript correction, revisions and re-submission of revised manuscripts up to the acceptance of the manuscripts.
RIM: Co-investigator, interventionist, data collection, proof reading and critically reviewed the article.
MFA: Collected data, intellectual input, care provider from surgical side to study patients in ward and follow up.
Reference
- Lavand P. Chronic pain after surgery: State of the art. Presse Med. 2015 May;44(5):486-91. [PubMed]
- Campbell J. Pain: the fifth vital sign. Presidential address, American Pain Society, Los Angeles, California, Nov 11, 1995.
- National Pharmaceutical Council and the Joint Commission on Accreditation of Healthcare Organizations. “Pain: Current understanding of assessment, management, and treatments.” 2001. [Free full text]
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: Results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–40.[PubMed]
- Walid MS, Donahue SN, Darmohray DM, Hyer LA Jr, Robinson JS Jr. The fifth vital sign-what does it mean? Pain Pract. 2008;6:417-422.
- Coughlin SM, Karanicolas PJ, Emmerton-Coughlin HM, Kanbur B, Kanbur S, Colquhoun PH:Better late than never? Impact of local analgesia timing on postoperative pain in laparoscopic surgery: a systematic review and metaanalysis. Surg Endosc2010, 24(12):3167-3176.
- Gupta A:Local anaesthesia for pain relief after laparoscopic cholecystectomy–a systematic review. Best Pract Res Clin Anaesthesiol 2005, 19(2):275-292.
- Charlton S, Cyna AM, Middleton P, Griffiths JD. Perioperative transversus abdominis plane (TAP) blocks for analgesia after abdominal surgery. Cochrane Database Syst Rev. 2010 Dec 8;(12):CD007705
- Kuppuvelumani P, Jaradi H, Delilkan A: Abdominal nerve blockade for postoperative analgesia after caesarean section. Asia Oceania J Obstet Gynaecol 1993, 19(2):165-169.
- Rafi AN: Abdominal field block: a new approach via the lumbar triangle. Anaesthesia 2001, 56(10):1024-1026.
- HebbardP, Fujiwara Y, Shibata Y, Royse C. Ultrasound Guided Transversus Abdominis Plane (TAP) Anaesth Intensive Care. 2007 Aug;35(4): 616-7.
- Albrecht E, Kirkham KR, Endersby RV, Chan VW, Jackson T, Okrainec A, Penner T, Jin R, Brull R: Ultrasound-guided Transversus Abdominis Plane (TAP) block for laparoscopic gastric-bypass surgery:a prospective randomized controlled double-blinded trial. Obes Surg 2013, 23(8):1309-1314.
- Atim A, Bilgin F, Kilickaya O, Purtuloglu T, Alanbay I, Orhan ME, Kurt E: The efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing hysterectomy. Anaesth Intensive Care 2011, 39(4):630-634.
- Skjelsager A, Ruhnau B, Kistorp TK, Kridina I, Hvarness H, Mathiesen O, Dahl JB: Transversus abdominis plane block or subcutaneous wound infiltration after open radical prostatectomy: a randomized study. Acta Anaesthesiol Scand 2013, 57(4):502-508.
- Araco A, Pooney J, Araco F, Gravante G: Transversus abdominis plane block reduces the analgesic requirements after abdominoplasty with flank liposuction. Ann Plast Surg 2010, 65(4):385-388.
- Sahin L, Sahin M, Gul R, Saricicek V, Isikay N: Ultrasound-guided transversus abdominis plane block in children: a randomised comparison with wound infiltration. Eur J Anaesthesiol2013, 30(7):409-414.
- Ismail S, Khan MR, Urooj S. Use of transversus abdominis plane block as an anesthetic technique in a high risk patient for abdominal wall surgery. J Anaesthesiol Clin Pharmacol. 2013 Oct;29(4):581-2.
- El-Dawlatly AA, Turkistani A, Kettner SC, Machata AM, Delvi MB, Thallaj A, Kapral S, Marhofer P. Ultrasound-guided transversus abdominis plane block: description of a new technique and comparison with conventional systemic analgesia during laparoscopic cholecystectomy.Br J Anaesth. 2009;102(6):763–767.
- Ventham NT, Hughes M, O’Neill S, Johns N, Brady RR, Wigmore SJ. Systematic review and meta-analysis of continuous local anaesthetic wound infiltration versus epidural analgesia for postoperative pain following abdominal surgery.Br J Anaesth. 2013;100(10):1280–1289.
- Fowler SJ, Christelis N. High volume local infiltration analgesia compared to peripheral nerve block for hip and knee arthroplasty-what is the evidence?Anaesth Intensive Care. 2013;41(4):458–462.
- Gousheh SM, Nesioonpour S, Javaher Foroosh F, Akhondzadeh R, Sahafi SA, Alizadeh Z. Intravenous paracetamol for postoperative analgesia in laparoscopic cholecystectomy.Anesth Pain Med. 2013;3(1):214–21.
- Petersen PL, Stjernholm P, Kristiansen VB, Torup H, Hansen EG, Mitchell AU, Moeller A, Rosenberg J, Dahl JB, Mathiesen O. The beneficial effect of transversus abdominis plane block after laparoscopic cholecystectomy in day-case surgery: a randomized clinical trial.Anesth Analg. 2012;115(3):527–533
- Salman AE, Yetisir F, Yurekli B, Aksoy M, Yildirim M, Kilic M. The efficacy of the semi-blind approach of transversus abdominis plane block on postoperative analgesia in patients undergoing inguinal hernia repair: a prospective randomized double-blind study.Local Reg Anesth. 2013;6:1–7.
- Abdallah FW, Halpern SH, Margarido CB. Transversus abdominis plane block for postoperative analgesia after Caesarean delivery performed under spinal anaesthesia? A systematic review and meta-analysis.Br J Anaesth. 2012;109(5):679–687.
- Aydogmus M, Sinikoglu S, Naki M, Ocak N, Sanlı N, Alagol A. Comparison of analgesic efficiency between wound site infiltration and ultra-sound-guided transversus abdominis plane block after cesarean delivery under spinal anaesthesia. Hippokratia. 2014 Jan;18(1):28-31.
- Güner Can M, Göz R, Berber İ, Kaspar Ç, Çakır Ü. Ultrasound/Laparoscopic Camera-Guided Transversus Abdominis Plane Block for Renal Transplant Donors: A Randomized Controlled Trial. Ann Transplant. 2015 Jul 23;20:418-23.
- Milone M, Di Minno MN, Musella M, Maietta P, Salvatore G, Iacovazzo C, Milone F. Outpatient inguinal hernia repair under local anaesthesia: feasibility and efficacy of ultrasound-guided transversus abdominis plane block. Hernia. 2013 Dec;17(6):749-55.
- Wang Y, Wu T, Terry MJ, Eldrige JS, Tong Q, Erwin PJ, et al. Improved Perioperative analgesia with Ultrasound-Guided Ilioinguinal/iliohypogastric Nerve or Transversus Abdominis Plane Block for Open Inguinal Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Phys Med Rehabil Int. 2015;2(6): 1055.
- Aveline C, Le Hetet H, Le Roux A, Vautier P, Cognet F, Vinet E, Tison C, Bonnet F. Comparison between ultrasound-guided transversus abdominis plane and conventional ilioinguinal/iliohypogastric nerve blocks for day-case open inguinal hernia repair. Br J Anaesth. 2011 Mar;106(3):380-6. doi: 10.1093/bja/aeq363. Epub 2010 Dec 21. PubMed PMID: 21177284.
- Manatakis D, Stamos N, Dontas I, Agalianos C, Gkiaourakis M, Karvelis M et al. Pilot study of Ambulatory Inguinal Hernia Repair under Ultrasound-guided Transversus Abdominis Plane Block Anesthesia Plus Conscious Sedation. British Journal of Medicine & Medical Research 4(17): 3269-3275, 2014
- Niraj G, Searle A, Mathews M, Misra V, Baban M, Kiani S, Wong M. Analgesic efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing open appendicectomy. Br J Anaesth. 2009 Oct;103(4):601-5.
- Mukhtar k. Transversus Abdominis Plane Block. The Journal of NYSORA 2009; 12: 28-33.
- Jorgensen H, Wetterslev J, Moiniche S, Dahl JB:Epidural local anaesthetics versus opioid-based analgesic regimens on postoperative gastrointestinal paralysis, PONV and pain after abdominal surgery. Cochrane Database Syst Rev 2000, (4):CD001893
- Johns N, O’Neill S, Ventham NT, Barron F, Brady RR, Daniel T. Clinical effectiveness of Transversus Abdominis Plane (TAP) block in abdominal surgery: a systematic review and meta-analysis.Colorectal Dis.2012;14(10):e635–e642.
- Gupta A, Favaios S, Perniola A, Magnuson A, Berggren L. A meta-analysis of the efficacy of wound catheters for post-operative pain management. Acta Anaesthesiol Scand. 2011;55(7):785–796
- Soltani Mohammadi S, Dabir A, Shoeibi G. Efficacy of transversus abdominis plane block for acute postoperative pain relief in kidney recipients: a double-blinded clinical trial. Pain Med. 2014;15(3):460–464.