Lumbosacral plexus entrapment syndrome. Part two: Symptomology and rehabilitative trials
Abstract
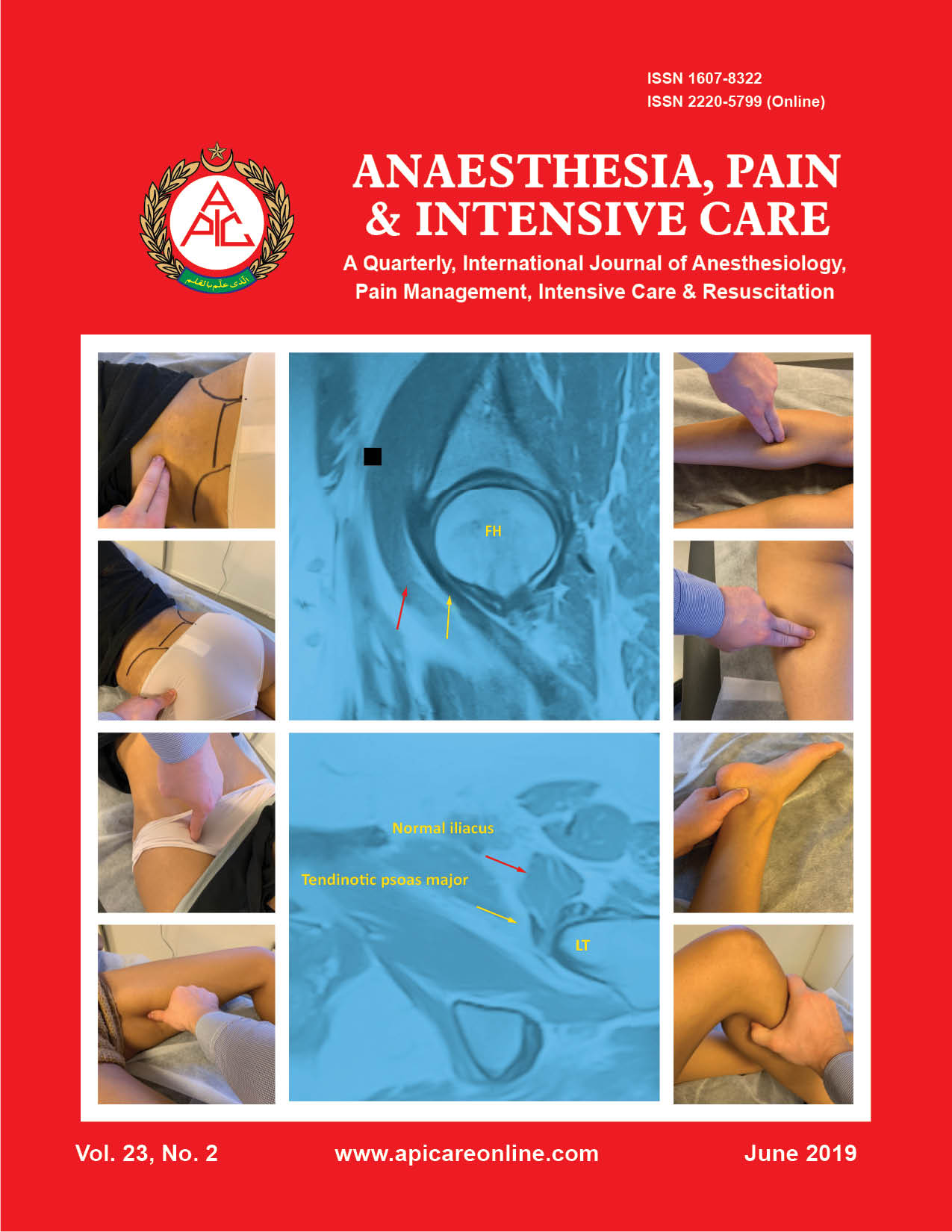
Background: Lumbosacral plexus entrapment syndrome (LPES) is a little-known but common cause of chronic lumbopelvic and lower extremity pain. The authors document the clinical course of 61 patients who were diagnosed and treated for LPES between May 2016 and October 2018. The study is aimed to evaluate the efficacy of our proposed diagnostic and conservative treatment protocol for LPES, clinically.
Methodology: This is a retrospective cohort study of patients suffering from LPES. Patients were included in this study if they compatible symptoms with LPES with symptoms of low back, pelvic, groin, genital, thigh or calf pain after other more common etiologies have been excluded. Additionally, these patients had at least 5 positive provocative Tinel’s tests applied to various lumbopelvic and lower extremity (LPLE) nerve branches yielding => 7 (numeric rating scale) NRS, and weakness of one or more myotomes of the lower body. The group in its entirety was treated with gentle strengthening of the psoas major and piriformis muscles. The primary outcome measure was patient reported satisfaction and improvement including: Full, significant, moderate, slight, or no improvement in pain and symptoms. Patients were followed for up to two years.
Results: The most common complaints amongst the patient pool were low back, groin, pelvic, posterior/lateral calf pain. Additionally, 17 patients (28%) stated that everything in the LPLE hurts, consistent with plexalgia. 13 patients were lost to follow-up as they did not reschedule treatment, for unknown reasons. Amongst the remaining 48 patients, 25 recovered fully (52%), 12 significantly (25%), and five moderately (10,4%). Five patients had a slight improvement (10,4%), and two no improvement whatsoever (4%). The average recovery times were mostly consistent with the time of affliction. Patients with a symptom duration of less than one year, generally recovered within 4 months. One to four years, within 10,5 months. Five to nine years, 7,5 months. And, finally, more than 10 years, within 18 months.
Conclusion: Non-specific pain syndromes in the LPLE where other causes have been excluded, may be attributable to underlying LPES. In this study, a high correlation between the diagnostic & interventional protocols, and beneficial patient outcomes were demonstrated. However, more statistical and long-term research is needed.
Citation: Larsen K, Chien GCC. Lumbosacral plexus entrapment syndrome. Part Two: Symptomology and rehabilitative trials. Anaesth pain & intensiv care 2019;23(2):138-144