Ristiawan Muji Laksono, Isngadi Isngadi, Arya Hari Murti
Department of Anesthesiology & Critical Care, Saiful Anwar General Hospital, Faculty of Medicine, Universitas Brawijaya, Malang, East Java, (Indonesia)
E:mail: is_dr@yahoo.com; aryaharimurti@gmail.com
Correspondence:
Ristiawan Muji Laksono, MD
Jalan Jaksa Agung Suprapto No. 2, Malang, East Java, (Indonesia) 65112; E-mail: ristiawanm@yahoo.com
ABSTRACT
Background and purpose: Adequate postoperative pain management, intended not only to facilitate surgery, but also to prevent development of chronic pain, remains the prime concern of the anesthesiologists. Intravenous administration of paracetamol as preemptive analgesia for general surgery has not shown consistent outcomes. The purpose of the present study was to determine the effects of paracetamol as a preemptive analgesia in patients undergoing a major oncologic surgery.
Methodology: Subjects were patients undergoing major oncology surgery with the criteria of mild to moderate pain. Forty patients involved in the study were divided into a control group (n = 20) of patients not administered with preemptive analgesia and a group of patients who received intravenous paracetamol as a preemptive analgesia (n = 20). Pain intensity was measured by the visual analog scale and analgesic consumption was recorded.
Results: In the group administered with intravenous paracetamol, there was a significant decline in the visual analog scores and analgesic consumption as compared to the control group not administered with intravenous paracetamol (p < 0.05).
Conclusions: Administration of intravenous paracetamol at certain doses was capable of suppressing post-major oncologic surgery pain and analgesic consumption. Thus, paracetamol infusion could be used as a preemptive analgesic for major oncologic surgery.
Key words: Pain; Preemptive Analgesia; Tumor; Operation; Acetaminophen.
Citation: Laksono RM, Isngadi I, Murti AH. Intravenous paracetamol as a preemptive analgesia to reduce postoperative pain after major oncologic surgery. Anaesth. pain & intensive care 2019;23(1):28-32
Received – 11 September 2018; Reviewed – 01, 4 October 2018; Corrected – 12 December 2018; Re-reviewed – 20, 26 December 2018, 9 January 2019; Accepted 31 January 2019
INTRODUCTION
Postoperative pain affects millions of patients worldwide. Pain is a very subjective experience with various dimensions. It is known that an inadequate postoperative pain management does not only delay the recovery but also increases morbidity and mortality. Some patients may even develop a chronic pain with increased morbidity1,2 Cancer is a universal public health problem. The World Health Organization estimates that by 2030 there will be 27 million new cases of cancer and 17 million cancer deaths. In this context, there has been an increase in operative chemotherapy, and as a result, the patient requires a better postoperative pain management to prevent chronic pain.3
Paracetamol, also called acetaminophen (IUPAC name: N-(4-hydroxyphenyl) ethanamide), is the most commonly used antipyretic and pain reliever. Since 1955 the drug was available in single or combination formulas with other compounds.4 Paracetamol has been widely used to control postoperative pain. Despite the unknown mechanism of action, paracetamol is capable of controlling pain through inhibiting prostaglandin synthesis in the central nervous system and acting at the periphery by blocking pain.5 In 2011, the formula of intravenous paracetamol was approved by the US Food and Drug Administration. Paracetamol IV is indicated for the management of mild to moderate pain, moderate to severe pain with the help of opioid analgesics, and reduction of fever in patients aged two years or older.6
Intravenous paracetamol has been widely used in various surgeries. Previous studies have shown that in patients with laparoscopic cholecystectomy, administration of paracetamol as a preemptive analgesia has been capable of reducing postoperative pain by up to 40%.7 Other studies have demonstrated the benefits of intravenous paracetamol in lowering moderate-to-severe postoperative orthopedic pain and it has been well tolerated.8 In total abdominal hysterectomy surgery, administration of preemptive intravenous paracetamol at a dose of 1 gram produced a good quality of postoperative analgesia.9 Intravenous administration of paracetamol as preemptive analgesia for cancer surgery has not shown consistent outcomes. Even in a preemptive dose of 1 gram, it has been incapable of reducing pain intensity.10 In breast cancer surgery, administration of paracetamol has been shown to decrease postoperative pain.11 For brain tumor surgery, paracetamol has the lowest quality in pain reduction, despite the very minimal side effects of nausea and vomiting.12 A similar finding was found in laryngeal cancer surgery.13 Therefore, we conducted the present study to investigate the effect of administration of paracetamol as a preemptive analgesia in patients receiving major oncology surgery.
METHODOLOGY
The present study was approved by the Ethics Committee for Health Research of Saiful Anwar Hospital, Medicine Faculty of Brawijaya University, Malang, East Java, Indonesia (Number 452/EC/KEPK/12/2016).
This randomized controlled study enrolled patients undergoing major surgical oncology with the criteria of mild to moderate pain (visual analog scale score of 47). We included patients who were willing to participate in the study and who signed the informed consent, aged 1945 y, minimum education of junior high school graduate, having no contraindication to paracetamol, a Visual Analogue Scale (VAS) score of 0 prior to the induction, and ASA physical status of III. Exclusion criteria were patients suffering from or having a history of diseases effecting hepatic and renal functions, receiving drugs capable of causing drug interactions with paracetamol, contraindications to the anesthetic drugs used in this study (allergic to ranitidine and propofol and disorders of cardiac conduction system such as AV block), surgery lasting more than 4 h, and an Aldrete score in the recovery room of < 9 for more than 2 h.
Anesthesia was induced using intravenous midazolam (0.05 mg/kg body weight) fentanyl (3 g/kg), 2% lidocaine (1.5 mg/kg), propofol (2 mg/kg), and atracurium (0.5 mg/kg). Five minutes prior to the surgical incision, subject received an additional dose of fentanyl of 1 g/kg. In order to prevent pain during surgery, a maintenance dose of fentanyl of 1 g/kg was administered every 60 min intermittently after the second administration of fentanyl (administration prior to surgical incision) and stopped 60 min prior to the completion of the surgery. Maintenance of anesthesia was performed using inhaled anesthetics, consisting of oxygen, N2O and isoflurane or sevoflurane at 1 MAC. In order to decrease the effects of postoperative nausea and vomiting each patient received dexamethasone 0.3 mg/kg and ondansetron 0.15 mg/ kg.
The preemptive analgesia used in the present study was intravenous paracetamol (10 mg/ml) administered in a dose of 15 mg/kg intravenously. As a placebo, 100 ml of 0.9% sodium chloride intravenous fluid was infused to patients of control group. Paracetamol and 0.9% NaCl were given at the same time prior to the incision during the induction of anesthesia.
Degree of pain was measured using the Visual Analogue Scale (VAS). Since the VAS scores strongly correlate well with the Verbal Numerical Scale (SNV), the technique of measuring the degree of pain was performed by asking the patients to determine the degree of pain experienced ranging from 0 (no pain) to 10 (unimaginable pain). The VAS scores were determined by asking the patients to mark the scale on the VAS ruler and subsequently confirmed against the objective condition seen from the patient’s face and adjusted to the pain scale image according to the Wong Baker Faces scale. VAS assessment was done when Aldrete score reached 9. The assessment was done by a blinded anesthesiologist.
Statistical analysis:
Data are presented in mean ± standard deviation (SD) and differences between treatment groups are analyzed by means of the Mann-Whitney test using SPSS 19.0 statistical package software. A p-value < 0.05 is considered statistically significant. RESULTS Respondents’ demographic characteristics, diagnosis, surgical procedure, medication history, and duration of surgery are presented in Table 1. No significant differences were found for gender, age, body mass index, education, diagnosis, surgical procedures, anesthesia physical status (ASA), medication history, and duration of surgery between the study groups (p > 0.05).
Table 1: Demographic characteristics of the subjects. Data given as mean ±SD or n (%)
Data were analyzed by student-t test
Figure 1 shows the difference in VAS score between the two study groups. The paracetamol group showed a significant decrease in the VAS score relative to the control group (p < 0.05).
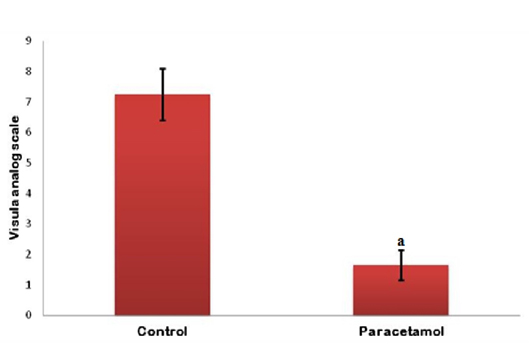
Figure 1: Comparison of pain scored measured by the visual analog scale in both study groupsa:
p < 0.05 relative to the control group
Figure 2 shows the difference in analgesic treatment between the two study groups. The paracetamol group showed a significant decrease in the analgesic treatment relative to the control group (p < 0.05).
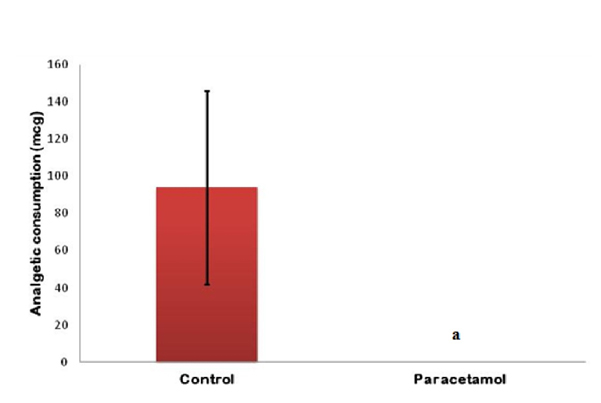
Figure 2: Comparison of analgesic consumption in both study groups:
p < 0.05 relative to the control group DISCUSSION Paracetamol is a widely prescribed analgesic. Intravenous administration in the present study was aimed at avoiding variations associated with gastric absorption and hepatic metabolism resulting in higher plasma concentrations and better analgesic efficacy than oral administration.14 In our study, gender, age, body mass index, education level, diagnosis, surgical procedures, physical status anesthesia (ASA), history of medication, and duration of surgery of the two study groups did not differ significantly (p > 0.05); thus, both groups were comparable. With regard to VAS scores, the group administered with intravenous paracetamol showed significantly lower scores than the group not administered with intravenous paracetamol (p < 0.05). This suggests that administration of intravenous paracetamol is useful to control pain associated with major oncologic surgery. This study extends previous findings on the benefits of intravenous paracetamol as a preemptive analgesia. An earlier study showed that in breast cancer surgery, administration of paracetamol decreases postoperative pain.11 However, in abdominal cancer surgery, paracetamol administration in a preemptive dose (1 gram) was not able to reduce pain intensity in another study.9 This study is inconsistent in terms of a decrease in pain with that of the brain and larynx cancer surgery.12,13], which is thought to be caused by the type of cancer. In our study, intravenous paracetamol also significantly decreased analgesic consumption compared to the control group. This indicates that the duration of effectiveness of intravenous paracetamol can suppress the need for analgesics in cases of major oncologic surgery. This finding is consistent with previous studies.15,16
LIMITATIONS
The limitations of our study were the administration of only single dose of paracetamol and a small sample size. A larger sample size and a multi-center study will be authenticative to show similar results or otherwise.
CONCLUSION
In conclusion, pre-emptive administration of intravenous paracetamol is capable of reducing post-major oncologic surgery pain and total narcotic analgesic consumption. Thus, it can be a useful preemptive analgesic of choice for major oncologic surgery.
Conflict of interest statement: All authors declared that there is no conflict of interest in the study and publication of this article.
Author contributions: RML, II, AHM - Conceived and designed the experiments; conducted the study; analyzed and interpreted the data; manuscript preparation and editing
REFERENCES
1. Garcia JBS, Bonilla P, Kraychette DC, Flores FC, de Valtolina EDP, Guerrero C. Optimizing post-operative pain management in Latin America. Rev Bras Anestesiol. 2017 Jul-Aug;67(4):395-403 [PubMed][Free Full Text]
2. Harsoor SS. Emerging concepts in post-operative management. Indian J Anesth. 2011 Mar-Apr;55:101-3 [PubMed]
3. Cavalcanti IL, de Carlvalho ACD, Musauer MG, Rodrigues VS, Migon RN, Figueiredo NV, et al. Safety and tolerability of controlled-release oxycodone on postoperative pain in patients submitted to the oncologic head and neck surgery. Rev Col Bras Cir. 2014 Nov-Dec;41(6):393-9 [PubMed][Free Full Text]
4. Tittarelli R, Pellegrini M, Scarpellini MG, Marinelli E, Bruti V, Di Luca MN, et al. Hepatotoxicity of paracetamol and related fatalities. Eur Rev Med Pharmacol Sci. 2017 Mar;21(1 Suppl):95-101 [PubMed][Free Full Text]
5. Allegaert K, van den Anker JN. Perinatal and neonatal use of paracetamol for pain relief. Semin Fetal Neonatal Med. 2017 Oct;22(5):308-13 [PubMed]
6. Gallipani A, Mathis AS, Ghin HL, Fahim G. Adverse effect profile comparison of pain regimens with and without intravenous acetaminophen in total hip and knee arthroplasty patients. SAGE Open Med. 2017; 5: 2050312117699146 [PubMed]
7. Kokhno VN, Shmerko PS, Shakhtarin I. Impact of preemptive analgesia on postoperative pain syndrome in laparoscopic surgery. Anesteziol Reanimatol. 2009;6:68-70.
8. Sinatra RS, Jahr JS, Reynolds LW, Viscusi ER, Groudine SB, Payen-Champenois C. Efficacy and safety of single and repeated administration of 1 gram intravenous acetaminophen injection (paracetamol) for pain management after major orthopedic surgery. Anesthesiology 2005 Apr;102(4):822-31 [PubMed]
9. Arici S, Gurbet A, Turker G, Yavascaoglu B, Sahin S. Preemptive analgesic effects of intravenous paracetamol in total abdominal hysterectomy. Agri. 2009 Apr;21(2):54-61 [PubMed][Free Full Text]
10. Borisov DB, Levin AV, Vyl’iurov IV, Sokolov AV, Nedashkovskii EV. Efficiency of preemptive intravenous paracetamol analgesia in abdominal surgery. Agri 2009;21(2):54-61. Anesteziol Reanimatol 2009;5:38-40.
11. Kampe S, Warm M, Landwehr S, Dagtekin O, Haussmann S, Paul M, et al. Clinical equivalence of IV paracetamol compared to IV dipyrone for postoperative analgesia after surgery for breast cancer. Curr Med Res Open. 2006 Oct;22(10):19491-54 [PubMed]
12. Hassani E, Mahoori A, Sane S, Tolumenhr A. Comparison the effects of paracetamol with sufentanil infusion on postoperative pain control after craniotomy in patients with brain tumor. Adv Biomed Res. 2015 Mar;4:64 [PubMed][Free Full Text]
13. Mom T, Bazin JE, Commun F. Assessment of postoperative pain after laryngeal surgery for cancer. Arch Otolaryngol Head Neck Surg. 1998 Jul;124(7):794-8 [PubMed]
14. Jarde O, Boccard E. Parenteral versus oral route increases paracetamol efficacy. Clin Drug Invest. 1997;14:474–81
15. Abdelmageed WM, Al Taher WM. Preoperative paracetamol infusion reduces sevoflurane consumption during thyroidectomy under general anesthesia with spectral entropy monitoring. Egyptian J Anesthesia 2014;30:115-12 [Free Full Text]
16. Polat R, Peker K, Guloksuz CT, Ergil J, Akkaya T. Comparison of the postoperative analgesic effects of paracetamol-codeine phosphate and naproxen sodium-codeine phosphate for lumbar disk surgery. Kaohsiung J Med Sci 2015 Sep;31(9):468-72 [PubMed][Free Full Text]
Department of Anesthesiology & Critical Care, Saiful Anwar General Hospital, Faculty of Medicine, Universitas Brawijaya, Malang, East Java, (Indonesia)
E:mail: is_dr@yahoo.com; aryaharimurti@gmail.com
Correspondence:
Ristiawan Muji Laksono, MD
Jalan Jaksa Agung Suprapto No. 2, Malang, East Java, (Indonesia) 65112; E-mail: ristiawanm@yahoo.com
ABSTRACT
Background and purpose: Adequate postoperative pain management, intended not only to facilitate surgery, but also to prevent development of chronic pain, remains the prime concern of the anesthesiologists. Intravenous administration of paracetamol as preemptive analgesia for general surgery has not shown consistent outcomes. The purpose of the present study was to determine the effects of paracetamol as a preemptive analgesia in patients undergoing a major oncologic surgery.
Methodology: Subjects were patients undergoing major oncology surgery with the criteria of mild to moderate pain. Forty patients involved in the study were divided into a control group (n = 20) of patients not administered with preemptive analgesia and a group of patients who received intravenous paracetamol as a preemptive analgesia (n = 20). Pain intensity was measured by the visual analog scale and analgesic consumption was recorded.
Results: In the group administered with intravenous paracetamol, there was a significant decline in the visual analog scores and analgesic consumption as compared to the control group not administered with intravenous paracetamol (p < 0.05).
Conclusions: Administration of intravenous paracetamol at certain doses was capable of suppressing post-major oncologic surgery pain and analgesic consumption. Thus, paracetamol infusion could be used as a preemptive analgesic for major oncologic surgery.
Key words: Pain; Preemptive Analgesia; Tumor; Operation; Acetaminophen.
Citation: Laksono RM, Isngadi I, Murti AH. Intravenous paracetamol as a preemptive analgesia to reduce postoperative pain after major oncologic surgery. Anaesth. pain & intensive care 2019;23(1):28-32
Received – 11 September 2018; Reviewed – 01, 4 October 2018; Corrected – 12 December 2018; Re-reviewed – 20, 26 December 2018, 9 January 2019; Accepted 31 January 2019
INTRODUCTION
Postoperative pain affects millions of patients worldwide. Pain is a very subjective experience with various dimensions. It is known that an inadequate postoperative pain management does not only delay the recovery but also increases morbidity and mortality. Some patients may even develop a chronic pain with increased morbidity1,2 Cancer is a universal public health problem. The World Health Organization estimates that by 2030 there will be 27 million new cases of cancer and 17 million cancer deaths. In this context, there has been an increase in operative chemotherapy, and as a result, the patient requires a better postoperative pain management to prevent chronic pain.3
Paracetamol, also called acetaminophen (IUPAC name: N-(4-hydroxyphenyl) ethanamide), is the most commonly used antipyretic and pain reliever. Since 1955 the drug was available in single or combination formulas with other compounds.4 Paracetamol has been widely used to control postoperative pain. Despite the unknown mechanism of action, paracetamol is capable of controlling pain through inhibiting prostaglandin synthesis in the central nervous system and acting at the periphery by blocking pain.5 In 2011, the formula of intravenous paracetamol was approved by the US Food and Drug Administration. Paracetamol IV is indicated for the management of mild to moderate pain, moderate to severe pain with the help of opioid analgesics, and reduction of fever in patients aged two years or older.6
Intravenous paracetamol has been widely used in various surgeries. Previous studies have shown that in patients with laparoscopic cholecystectomy, administration of paracetamol as a preemptive analgesia has been capable of reducing postoperative pain by up to 40%.7 Other studies have demonstrated the benefits of intravenous paracetamol in lowering moderate-to-severe postoperative orthopedic pain and it has been well tolerated.8 In total abdominal hysterectomy surgery, administration of preemptive intravenous paracetamol at a dose of 1 gram produced a good quality of postoperative analgesia.9 Intravenous administration of paracetamol as preemptive analgesia for cancer surgery has not shown consistent outcomes. Even in a preemptive dose of 1 gram, it has been incapable of reducing pain intensity.10 In breast cancer surgery, administration of paracetamol has been shown to decrease postoperative pain.11 For brain tumor surgery, paracetamol has the lowest quality in pain reduction, despite the very minimal side effects of nausea and vomiting.12 A similar finding was found in laryngeal cancer surgery.13 Therefore, we conducted the present study to investigate the effect of administration of paracetamol as a preemptive analgesia in patients receiving major oncology surgery.
METHODOLOGY
The present study was approved by the Ethics Committee for Health Research of Saiful Anwar Hospital, Medicine Faculty of Brawijaya University, Malang, East Java, Indonesia (Number 452/EC/KEPK/12/2016).
This randomized controlled study enrolled patients undergoing major surgical oncology with the criteria of mild to moderate pain (visual analog scale score of 47). We included patients who were willing to participate in the study and who signed the informed consent, aged 1945 y, minimum education of junior high school graduate, having no contraindication to paracetamol, a Visual Analogue Scale (VAS) score of 0 prior to the induction, and ASA physical status of III. Exclusion criteria were patients suffering from or having a history of diseases effecting hepatic and renal functions, receiving drugs capable of causing drug interactions with paracetamol, contraindications to the anesthetic drugs used in this study (allergic to ranitidine and propofol and disorders of cardiac conduction system such as AV block), surgery lasting more than 4 h, and an Aldrete score in the recovery room of < 9 for more than 2 h.
Anesthesia was induced using intravenous midazolam (0.05 mg/kg body weight) fentanyl (3 g/kg), 2% lidocaine (1.5 mg/kg), propofol (2 mg/kg), and atracurium (0.5 mg/kg). Five minutes prior to the surgical incision, subject received an additional dose of fentanyl of 1 g/kg. In order to prevent pain during surgery, a maintenance dose of fentanyl of 1 g/kg was administered every 60 min intermittently after the second administration of fentanyl (administration prior to surgical incision) and stopped 60 min prior to the completion of the surgery. Maintenance of anesthesia was performed using inhaled anesthetics, consisting of oxygen, N2O and isoflurane or sevoflurane at 1 MAC. In order to decrease the effects of postoperative nausea and vomiting each patient received dexamethasone 0.3 mg/kg and ondansetron 0.15 mg/ kg.
The preemptive analgesia used in the present study was intravenous paracetamol (10 mg/ml) administered in a dose of 15 mg/kg intravenously. As a placebo, 100 ml of 0.9% sodium chloride intravenous fluid was infused to patients of control group. Paracetamol and 0.9% NaCl were given at the same time prior to the incision during the induction of anesthesia.
Degree of pain was measured using the Visual Analogue Scale (VAS). Since the VAS scores strongly correlate well with the Verbal Numerical Scale (SNV), the technique of measuring the degree of pain was performed by asking the patients to determine the degree of pain experienced ranging from 0 (no pain) to 10 (unimaginable pain). The VAS scores were determined by asking the patients to mark the scale on the VAS ruler and subsequently confirmed against the objective condition seen from the patient’s face and adjusted to the pain scale image according to the Wong Baker Faces scale. VAS assessment was done when Aldrete score reached 9. The assessment was done by a blinded anesthesiologist.
Statistical analysis:
Data are presented in mean ± standard deviation (SD) and differences between treatment groups are analyzed by means of the Mann-Whitney test using SPSS 19.0 statistical package software. A p-value < 0.05 is considered statistically significant. RESULTS Respondents’ demographic characteristics, diagnosis, surgical procedure, medication history, and duration of surgery are presented in Table 1. No significant differences were found for gender, age, body mass index, education, diagnosis, surgical procedures, anesthesia physical status (ASA), medication history, and duration of surgery between the study groups (p > 0.05).
Table 1: Demographic characteristics of the subjects. Data given as mean ±SD or n (%)
| Characteristics | Control group
(n =20) |
Paracetamol group
(n =20) |
p value |
| Age (year) | 42.75 ± 3.01 | 41.85 ± 3.33 | 0.375 |
| BMI (kg/m2) | 23.68 ± 2.32 | 23.50 ± 2.79 | 0.832 |
| Sex | |||
| Male | 8 (40) | 3 (15) | 0.183 |
| Female | 12 (60) | 17 (85) | |
| Educational level | |||
| Senior high school | 9 (45) | 8 (40) | 0.799 |
| Undergraduate | 11 (55) | 12 (60) | |
| Diagnosis | |||
| Ca breast | 5 (25) | 7 (35) | 0.602 |
| Ca parotid | 5 (25) | 3 (15) | |
| Stroma multinodular non-toxic | 7 (35) | 9 (45) | |
| Stroma uninodular non-toxic | 3 (15) | 1 (5) | |
| Surgery | |||
| Modified radical mastectomy | 0 (00 | 7 (35) | 0.862 |
| Radical mastectomy | 5 (25) | 0 (0) | |
| Partial parotidectomy | 3 (15) | 1 (5) | |
| Subtotal thyroidectomy | 2 (10) | 1 (5) | |
| Total parotidectomy | 5 (25) | 3 (15) | |
| Total thyroidectomy | 5 (25) | 8 (40) | |
| ASA | |||
| II, malignancy | 7 (35) | 10 (50) | 0.698 |
| II, malignancy post chemotherapy | 3 (15) | 0 (0) | |
| II, stroma euthyroid | 10 (50) | 10 (50) | |
| Duration of surgery (hour) | 2.10 ± 0.26 | 2.08 ± 0.18 | 0.968 |
| Medical history | |||
| None | 17 (85) | 20 (100) | 0.429 |
| Chemotherapy | 3 (15) | 0 (0) | |
Figure 1 shows the difference in VAS score between the two study groups. The paracetamol group showed a significant decrease in the VAS score relative to the control group (p < 0.05).
Figure 1: Comparison of pain scored measured by the visual analog scale in both study groupsa:
p < 0.05 relative to the control group
Figure 2 shows the difference in analgesic treatment between the two study groups. The paracetamol group showed a significant decrease in the analgesic treatment relative to the control group (p < 0.05).
Figure 2: Comparison of analgesic consumption in both study groups:
p < 0.05 relative to the control group DISCUSSION Paracetamol is a widely prescribed analgesic. Intravenous administration in the present study was aimed at avoiding variations associated with gastric absorption and hepatic metabolism resulting in higher plasma concentrations and better analgesic efficacy than oral administration.14 In our study, gender, age, body mass index, education level, diagnosis, surgical procedures, physical status anesthesia (ASA), history of medication, and duration of surgery of the two study groups did not differ significantly (p > 0.05); thus, both groups were comparable. With regard to VAS scores, the group administered with intravenous paracetamol showed significantly lower scores than the group not administered with intravenous paracetamol (p < 0.05). This suggests that administration of intravenous paracetamol is useful to control pain associated with major oncologic surgery. This study extends previous findings on the benefits of intravenous paracetamol as a preemptive analgesia. An earlier study showed that in breast cancer surgery, administration of paracetamol decreases postoperative pain.11 However, in abdominal cancer surgery, paracetamol administration in a preemptive dose (1 gram) was not able to reduce pain intensity in another study.9 This study is inconsistent in terms of a decrease in pain with that of the brain and larynx cancer surgery.12,13], which is thought to be caused by the type of cancer. In our study, intravenous paracetamol also significantly decreased analgesic consumption compared to the control group. This indicates that the duration of effectiveness of intravenous paracetamol can suppress the need for analgesics in cases of major oncologic surgery. This finding is consistent with previous studies.15,16
LIMITATIONS
The limitations of our study were the administration of only single dose of paracetamol and a small sample size. A larger sample size and a multi-center study will be authenticative to show similar results or otherwise.
CONCLUSION
In conclusion, pre-emptive administration of intravenous paracetamol is capable of reducing post-major oncologic surgery pain and total narcotic analgesic consumption. Thus, it can be a useful preemptive analgesic of choice for major oncologic surgery.
Conflict of interest statement: All authors declared that there is no conflict of interest in the study and publication of this article.
Author contributions: RML, II, AHM - Conceived and designed the experiments; conducted the study; analyzed and interpreted the data; manuscript preparation and editing
REFERENCES
1. Garcia JBS, Bonilla P, Kraychette DC, Flores FC, de Valtolina EDP, Guerrero C. Optimizing post-operative pain management in Latin America. Rev Bras Anestesiol. 2017 Jul-Aug;67(4):395-403 [PubMed][Free Full Text]
2. Harsoor SS. Emerging concepts in post-operative management. Indian J Anesth. 2011 Mar-Apr;55:101-3 [PubMed]
3. Cavalcanti IL, de Carlvalho ACD, Musauer MG, Rodrigues VS, Migon RN, Figueiredo NV, et al. Safety and tolerability of controlled-release oxycodone on postoperative pain in patients submitted to the oncologic head and neck surgery. Rev Col Bras Cir. 2014 Nov-Dec;41(6):393-9 [PubMed][Free Full Text]
4. Tittarelli R, Pellegrini M, Scarpellini MG, Marinelli E, Bruti V, Di Luca MN, et al. Hepatotoxicity of paracetamol and related fatalities. Eur Rev Med Pharmacol Sci. 2017 Mar;21(1 Suppl):95-101 [PubMed][Free Full Text]
5. Allegaert K, van den Anker JN. Perinatal and neonatal use of paracetamol for pain relief. Semin Fetal Neonatal Med. 2017 Oct;22(5):308-13 [PubMed]
6. Gallipani A, Mathis AS, Ghin HL, Fahim G. Adverse effect profile comparison of pain regimens with and without intravenous acetaminophen in total hip and knee arthroplasty patients. SAGE Open Med. 2017; 5: 2050312117699146 [PubMed]
7. Kokhno VN, Shmerko PS, Shakhtarin I. Impact of preemptive analgesia on postoperative pain syndrome in laparoscopic surgery. Anesteziol Reanimatol. 2009;6:68-70.
8. Sinatra RS, Jahr JS, Reynolds LW, Viscusi ER, Groudine SB, Payen-Champenois C. Efficacy and safety of single and repeated administration of 1 gram intravenous acetaminophen injection (paracetamol) for pain management after major orthopedic surgery. Anesthesiology 2005 Apr;102(4):822-31 [PubMed]
9. Arici S, Gurbet A, Turker G, Yavascaoglu B, Sahin S. Preemptive analgesic effects of intravenous paracetamol in total abdominal hysterectomy. Agri. 2009 Apr;21(2):54-61 [PubMed][Free Full Text]
10. Borisov DB, Levin AV, Vyl’iurov IV, Sokolov AV, Nedashkovskii EV. Efficiency of preemptive intravenous paracetamol analgesia in abdominal surgery. Agri 2009;21(2):54-61. Anesteziol Reanimatol 2009;5:38-40.
11. Kampe S, Warm M, Landwehr S, Dagtekin O, Haussmann S, Paul M, et al. Clinical equivalence of IV paracetamol compared to IV dipyrone for postoperative analgesia after surgery for breast cancer. Curr Med Res Open. 2006 Oct;22(10):19491-54 [PubMed]
12. Hassani E, Mahoori A, Sane S, Tolumenhr A. Comparison the effects of paracetamol with sufentanil infusion on postoperative pain control after craniotomy in patients with brain tumor. Adv Biomed Res. 2015 Mar;4:64 [PubMed][Free Full Text]
13. Mom T, Bazin JE, Commun F. Assessment of postoperative pain after laryngeal surgery for cancer. Arch Otolaryngol Head Neck Surg. 1998 Jul;124(7):794-8 [PubMed]
14. Jarde O, Boccard E. Parenteral versus oral route increases paracetamol efficacy. Clin Drug Invest. 1997;14:474–81
15. Abdelmageed WM, Al Taher WM. Preoperative paracetamol infusion reduces sevoflurane consumption during thyroidectomy under general anesthesia with spectral entropy monitoring. Egyptian J Anesthesia 2014;30:115-12 [Free Full Text]
16. Polat R, Peker K, Guloksuz CT, Ergil J, Akkaya T. Comparison of the postoperative analgesic effects of paracetamol-codeine phosphate and naproxen sodium-codeine phosphate for lumbar disk surgery. Kaohsiung J Med Sci 2015 Sep;31(9):468-72 [PubMed][Free Full Text]