*Professor; **Assistant Professor
Department of Anesthesiology & Intensive Care, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh (India)
Correspondence: Dr. S.K.Malhotra, MD, Professor of Anesthesiology & Intensive Care, Postgraduate Institute of Medical Education and Research (PGIMER), Sector 12, Chandigarh, 160012, (India); E-mail: drskmalhotra@yahoo.com
ABSTRACTFailed intubation is prevalent in obstetric patients, more so during the last trimester of pregnancy when physiological factors may worsen the problems that lead to difficult intubation. If securing the airway is not managed efficiently it may have disastrous effects on mother and the fetus. During last few years, management of airway in obstetrics and training in this field has undergone numerous changes. The postgraduate students have been getting lesser exposure to intubation in pregnant patients. As regional anesthesia is increasingly popular in obstetrics, acquiring dexterity in conducting general anesthesia is becoming difficult. There should be a methodical approach to train in managing difficult obstetric airway. Various novel airway devices are now being suggested as an alternative to conventional intubation using laryngoscope. In addition, devices such as simulators should be employed to so that difficult or failed intubation may be managed with required skill. Other vital aspects to deal with this situation include a difficult airway cart that contains alternative airway devices, a comprehensive but practically easy algorithm and a regular drill or training to deal with difficult airway in obstetric patients.
Key words: Failed intubation; Airway; Cesarean section; Anesthesia, general
Citation: Malhotra SK, Samra T. Failed intubation in obstetrics. Anaesth Pain & Intensive Care 2014;18(4):424-29
INTRODUCTIONIn obstetric population, the failed intubation is not that common but once it occurs it may lead to significant morbidity, both in mother and fetus. Failed intubation is defined as failure to achieve tracheal intubation during a rapid sequence induction for obstetric anesthesia, thereby initiating a failed intubation drill.1As compared to non-obstetric patients, chances of failed/difficult intubation are 4 to 8 fold in pregnant. In one survey in United Kingdom, carried over a period of two years, one in 224 obstetric patients had failed intubation.2In various countries, GA for Cesarean section has considerably decreased(from 55% to 9.4%) and is employed only when stress to mother or fetus is imminent and carries risk.3However, the overall rate of Cesarean section has increased at the same time.4With the reduction in the number of obstetric GAs, there is an apprehension that the opportunity to get training in administering GA in obstetric patients has declined.5Due to popularity of regional anesthesia for Cesarean section, indications of GA (Table 1) have become limited.3 Table 1: Indications of GA for Cesarean Section
_______________________________________________- Urgent delivery (Maternal/fetal distress)
- Obstetrician /maternal request
- Failed regional block
- Possible hemodynamic instability
- Sepsis
- Coagulopathy
In Confidential Enquiries of Maternal Deaths, conducted between 2006 to 2008, two out of six deaths were due to airway problems.6
Causative Factors to Failed Intubation:
The evaluation of airway may not definitely predict the failed/difficult airway but Mallampatti score successfully assessed the difficult airway in 59% of the obstetric airways.7Intubation problems may worsen due to physiological changes to airway in pregnancy.8The situations that may predispose to difficult airway may include Cesarean section in the past, twin pregnancies, obesity and preeclampsia.9Presence offever or prolonged labor may also contribute.
CONTRIBUTING FACTORSThe hospitals where GA for Cesarean is administered more frequently, the incidence of failed intubation is less, probably due to more experience. 10In one review it was concluded that there is no data to confirm that intubation is more difficult than non-pregnant patients.11 But once the failed intubation occurs in obstetric patient, consequences are more disastrous.12
Factors already present:- Failed intubation in the past
- Receding chin
- Restricted mouth opening
- Limited neck extension ( ankylosing spondylitis)
- Protruding teeth
- Short Neck
- Obesity
- Turner syndrome, high arched palate
- Rise in oxygen consumption
- FRC reduction (up to 20%)
- Rapid desaturation during induction
- Upper airway edema
- Airway changes during pregnancy
- Enlarged breasts
- Risk of airway trauma – due to increased blood supply
- Higher risk of aspiration
- Increased weight
Obstetric patients with epidural may be converted to GA in 2.2% cases.4 Failed intubations may be due to failed regional anesthesia in 17% cases (UKOSS study). So, the patients with epidural must be monitored frequently, particularly before giving top-up. 13
Changes in obstetric airway:
Following retention of fluid during pregnancy and other changes in airway, there is reduction of pharyngeal volume. This leads to increase in Mallampati score. 7
Other changes include weight gain, increase in breast size, mucosal edema of respiratory tract, and enlargement of nasal and oropharyngeal mucosa. Also there is edema of and larynx.So, if Cesarean section is indicated, airway must be re-evaluated.
Aspiration prophylaxis:During pregnancy, uterus pushes the stomach and esophagus is displaced into thorax. This leads to decrease in lower esophageal tone increasing the chances of aspiration of gastric contents. The emptying time is delayed during pregnancy and incidence of reflux is enhanced. All these factors necessitate the administration of aspiration prophylaxis that includes antacids and gastroprokinetic agent, such as, metoclopramide.
Training for securing obstetric airway:
It has been observed that junior residents are not getting enough experience in administration of general anesthesia in obstetric patients, particularly for Cesarean section. Owing to lesser complications, regional anesthesia has become more popular in pregnant patients. That is the reason, the trainees get less chances to learn GA in obstetrics.14The trainees also have pressure from obstetricians to administer anesthesia quickly and difficult/failed intubations 15It has been observed that incidence of failed intubation is more in hours outside the normal working period.
Failed intubation training can be effectively learnt using simulators. The drills have proved useful to enhance communication, improve team-spirit and situational awareness. There is no alternative to practical hands on training. Therefore, opportunity of teaching must be utilized by both teachers and trainees.
PREPARATION FOR OBSTETRIC ANESTHESIA
All the anesthetists should be familiar with difficult airway cart, its contents and how to use them. The anesthetist on duty must check equipment and drugs required for rapid sequence intubation. If the anesthetist observes that intubation is likely to be difficult, he must call for assistance.
Positioning: Positioning of the obstetric patient is a vital aspect for successful intubation using rapid sequence induction. A ramp is a good choice if a difficult airway is likely. All the obese patients should lie down on ramp so that the sternum and ear align i.e. ‘Ear-to-sternal notch position’. This position also helps to keep the breasts away during laryngoscopy.
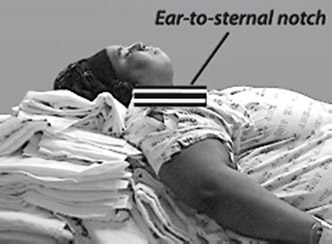
Figure 1: Ear-to-sternal notch position (Courtesy: Airway Cam Portal, Radnor PA, USA)
It is mandatory to keep the patient in left lateral lift to avoid supine hypotensive syndrome.
Difficult airway cart is a must to manage the potential difficulty in intubation. All the devices should be checked. The laryngoscope blade should be of proper size. Special blades like McCoy, may be helpful. Polio blade or short-handled blade may be suitable if large breasts are encountered. Videolaryngoscope may be of extra help if anterior and high larynx is present. Include gum elastic bougie and cricothyrotomy kit, too in the cart.
Aspiration prophylaxis is a must for an obstetric patient that may include antacid such as ranitidine and metoclopramide as these patients are likely to have reflux and are at high risk of aspiration.16
Rapid Sequence Induction (RSI) is generally employed for intubation. This is preceded by preoxygenation as FRC is decreased and oxygen consumption is increased leading to desaturation at the time of intubation. The mask-seal should be adequate and preoxygenation is achieved by three minutes of tidal ventilation or eight deep breaths.
Suxamethonium (1-1.5 mg/kg) should be kept ready. One must have an alternative plan in case failed intubation is encountered.
STRATEGY TO MANAGE FAILED INTUBATION
Failed intubation in obstetric patients is not so common. The Difficult Airway Society (DAS) has recommended guidelines to manage failed intubationin adults and children but not for obstetric patients. In case of failed intubation in such patient group, each institute should have its own flow chart for failed intubation strategy. (Figure 1)
In an event of failed intubation the surgical team should be informed and help should be sought. Two attempts for intubation should not be exceeded to avoid injury to airway and “can’t intubate, can’t ventilate” condition. Our primary goal should be to maintain airway and oxygenation.17
While undertaking mask ventilation Sellick maneuver should be employed. An oral and/or nasal airway should be handy if ventilation is not satisfactory. In case oxygen saturation is not being maintained (<90%), a supraglottic device (SGD) must be considered. Most commonly used device is classic LMA. Proseal LMA is equally effective. I-gel has also been used. Both, Proseal LMA and I-gel come with a gastric channel for passing a suction catheter through it to aspirate the gastric secretions.
While placing LMA, Sellick maneuver must be taken off. Once the ventilation is achieved, discuss with surgeon whether to proceed to delivery or wake the patient and go for awake fiberoptic intubation. If it is decided to go ahead with delivery, then spontaneous ventilation is preferred. SGD may also be used to intubate directly (e.g Intubating LMA or air-Q LMA) or introduce fiberoptic scope through SGD for intubation. Another way is to use Aintree catheter over a pediatric fiberoptic scope through classic LMA. Once the fiberoptic scope reaches trachea, both fiberoptic and LMA are removed and ETT passed over Aintree catheter just like over a bougie.
In case, SGD does not help in ventilation, situation becomes ‘Can’t intubate, can’t ventilate’ and a surgical approach to airway management. This may achieved by cannula cricothyrotomy or transtracheal jet ventilation. Surgical cricothyrodotomy may also be considered though it is a rare scenario. 18 One must use the device which is familiar and you have practiced it frequently.19
Choice of Supraglottic Device:
An ideal SGD in obstetric patients is the one that can prevent the regurgitation of gastric contents. LMA ProSeal, LMA Supreme, or I-gel are commonly recommended. Intubating SGD may also be used such as Intubating LMA or air-Q. As the maintenance of oxygen saturation and ventilation is vital, the device used should be the one to which the anesthesiologist is familiar with. In situation where failed intubation in obstetrics is encountered, LMA ProSeal is an ideal choice since it has better seal-pressure and aspiration port is provided, too.20 Sometimes the insertion of LMA may be difficult especially when the patient is light. If ventilation can be carried out effectively, the decision to go ahead with surgical procedure should be made. In case ventilation is not achievable, the subsequent step of failed intubation algorithm must be followed.
DIFFICULT INTUBATION GUIDELINES
There has been extensive work and consideration of the importance of tackling difficult airway through various guidelines in non-pregnant patients but no such plan for unanticipated difficult airway has been suggested for obstetric population. 18
Since there is no consensus strategy, the institutes offering obstetric services should chalk out their own guidelines and drills. They must possess proper equipment and devices to manage difficult airway. A routine training and drills must be carried out.
In the absence of an approach, hospitals providing obstetric services must have their own guidelines, appropriate and easily accessible airway equipment, and regular teaching and training in the management of airway problems.
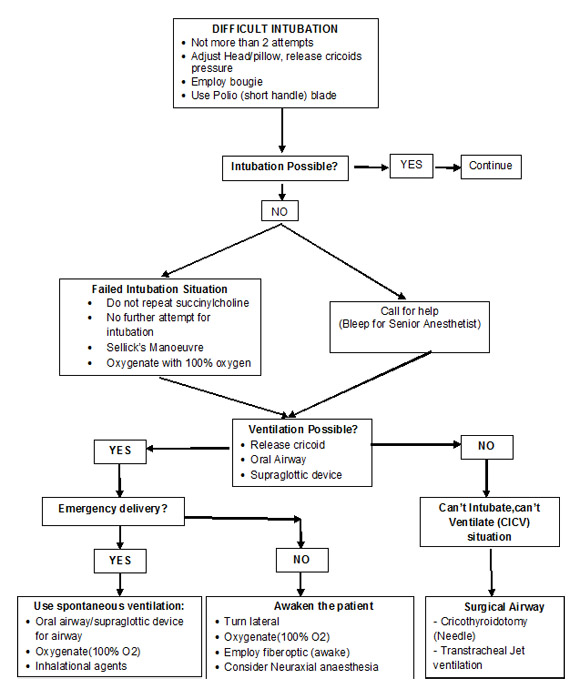
Figure 1: Failed Intubation flowchart in Obstetrics
EMERGENCE FROM ANESTHESIA
In various surveys, the patients admitted in Intensive care after failed intubation, were those with co-existing diseases and not due to airway problems, as such. The recovery from anesthesia in an obstetric patient who had difficult airway may have the risk of aspiration as well as the problem in re-intubation, if required.21 The extubation of a difficult airway should be handled with skill and dexterity with all the monitoring on and preferably on the operating table, where all the facilities for re-intubation are available. After the patient is completely awake and adequate laryngeal and pharyngeal reflexes emerge, the patient should be shifted to post-anesthesia care unit. In case, airway edema is present, steroids may be considered. Constant monitoring for oxygen saturation and ventilation must be carried out in immediate postoperative period. Detailed documentation of the difficulties faced in securing airway should be undertaken. Later, the patient should be explained regarding her difficult airway so that she is aware about this aspect for any future intervention.
FUTURE ADVANCESVarious studies have revealed that if Sellick manoeuvre is applied properly, there are least chances of increasing intragastric pressure. If a careful mask ventilation is employed it would ensure oxygen saturation that would be helpful in case a difficult airway is encountered. Adequate muscle relaxation provides adequate mask ventilation. However, second dose of suxamethonium is discouraged so that one is not tempted to try intubation for more than two times and concentrate on other plans to ensure ventilation and oxygenation.22 After failure of intubation and patient becoming light, it becomes difficult to insert a supraglottic device. Administration of muscle relaxant at this point is controversial. Sugammadex is showing the encouraging results in such situations in obstetrics as it may rapidly reverse the action of relaxants like rocuronium. In case the upper airway obstruction is present, reversal of muscle relaxant does not ensure that spontaneous breathing would be restored.
KEY POINTS- Management of obstetric airway is difficult since most of the anesthesiologists are not exposed to general anaesthesia for Cesarean section, thereby less experienced.
- Adequate positioning and preoxygenation plays a vital role in dealing with difficult airway management in obstetrics.
- Once failed intubation is encountered, one must ensure ventilation and oxygenation.
- Remember it is the ventilation that saves the patient not the intubation.
- Anesthesiologist must use the airway device he is familiar with. Videolaryngoscope is a useful tool in the current era.
- One must be familiar about the strategies in case of failed intubation.
- It is mandatory for every institute to prepare its own guidelines/flowchart depending on the airway devices available in the institute.
- Balki M, Cooke ME, Dunington S, Salman A, Goldszmidt E. Unanticipated difficult airway in obstetric patients: development of a new algorithm for formative assessment in high-fidelity simulation.Anesthesiology 2012 Oct;117(4):883-97. [PubMed]
- Quinn AC, Milne D, Columb M, Gorton H, Knight M. Failed tracheal intubation in obstetric anaesthesia: 2 year national case-control study in the UK. Br J Anaesth 2013;110:74 -80. [PubMed] [Free full text]
- McDonnell NJ, Paech MJ, Clavisi OM, Scott KL; ANZCA Trials Group. Difficult and failed intubation in obstetric anaesthesia: an observational study of airway management and complications associated with general anaesthesia for caesarean section. Int J Obstet Anesth 2008;17:292–297. [PubMed] doi: 10.1016/j.ijoa.2008.01.017
- Health and social care information centre: HES Online: NHS maternity statistics 2011-2012.
- Searle RD, Lyons G. Vanishing experience in training for obstetric general anaesthesia: an observational study. Int J Obstet Anesth 2008;17:233-237. [PubMed] doi: 10.1016/j.ijoa.2008.01.007.
- Cantwell R, Clutton-Brock T, Cooper G, Dawson A, Drife J, Garrod D, et al. The eighth report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. Saving Mothers’ Lives: Reviewing maternal deaths to make motherhood safe. BJOG 2011;118(Suppl. 1):2006-2008. [PubMed]
- Yentis SM. Predicting difficult intubation -worthwhile exercise or pointless ritual? Anaesthesia 2002;57:105-109. [PubMed]
- BoutonnetM, Faitot V, Katz A, Salomon L, Keita H. Mallampati class changes during pregnancy, labour, and after delivery: can these be predicted?Br J Anaesth 2010;104(1):67-70. [PubMed]
- Cook TM, Woodal N, Frerk C. Editor's Choice: Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br J Anaesth 2011;106(5):617-631. [PubMed] doi: 10.1093/bja/aer058.
- Djabatey EA, Barclay PM. Difficult and failed intubation in 3430 obstetric general anaesthetics. Anaesthesia 2009;64:1168–71. [PubMed] doi: 10.1111/j.1365-2044.2009.06060.x.
- Goldszmidt E. Is there a difference between the obstetric and nonobstetric airway. In: Halpern SH, Douglas MJ, eds. Evidence Based Obstetric Anaesthesia. Oxford: Blackwell Publishing Ltd, 2007; pp225–236.
- Sundaram R. Predicting difficult intubation; useful or what? A response to 'Predicting difficult intubation--worthwhile exercise or pointless ritual?', Anaesthesia 2002; 57: 105-109. Anaesthesia. 2003 Jun;58(6):619. [PubMed]
- Bauer ME, Kountanis JA, Tsen LC, et al. Risk factors for failed conversion of labor analgesia to caesarean delivery anaesthesia: a systematic review and meta-analysis of observational trials. Int J Obstet Anesth 2012;21:294-309. [PubMed] doi: 10.1016/j.ijoa.2012.05.007.
- The Confidential Enquiry into Maternal and Child Health (CEMACH).Saving Mothers’Lives: Reviewing Maternal Deaths to make Motherhood Safer 2003–2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH Publications, 2007.
- Jigajinni S. Trainee preparation and worries prior to commencing obstetric on-call. RCOA bulletin 2010;63:18-20. [Online]
- Mhyre JM, Healy D. The unanticipated difficult intubation in obstetrics. Anesth Analg 2011 Mar;112(3):648-652. [PubMed] doi: 10.1213/ANE.0b013e31820a91a6.
- Vasdev GM, Harrison BA, Keegan MT. Management of the difficult and failed airway in obstetric anesthesia. Journal of Anesthesia 2008;22(1):38-48. [PubMed] doi: 10.1007/s00540-007-0577-z.
- Henderson JJ, Popat MT, Latto IP, Pearce AC; Difficult Airway Society. Difficult Airway Society guidelines for the management of the unanticipated difficult intubation. Anaesthesia 2004;59:’’675–694. [PubMed]
- Heard AM, Green RJ, Eakins P. The formulation and intoduction of a ‘can’t intubate, can’t ventilate’ algorithm into clinical practice. Anaesthesia 2009;64:601-608. [PubMed] doi: 10.1111/j.1365-2044.2009.05888.x.
- Halaseh BK, Sukkar ZF, Hassan H, Sia AT, Bushnaq WA, Adarbeh H.The use of ProSeal laryngeal mask airway in caesarean section – experience in 3000 cases.Anaesth Intensive Care 2010;38:1023-1028. [PubMed]
- Brien K O, ConlonC.Failed intubation in obstetrics. Anaesthsia & intensive care medicine 2013;14(8):315–319.
- Rucklidge , Hinton C. Difficult and failed intubation in obstetrics. Contin EducAnaesth Crit Care Pain 2012;12(2):86-91. [Online]