İbrahim Öztürk, MD1, Selen Öztürk, MD2
1Medeniyet University Göztepe Education and Research Hospital, Department of Anesthesiology and Reanimation, Istanbul, (Turkey)
2Dr. Siyami Ersek Cardiovascular Surgery Education and Research Hospital, Department of Cardiovascular Surgery, Istanbul, (Turkey)
Correspondence: İbrahim Öztürk, MD, Medeniyet University Göztepe Education & Research Hospital, Department of Anesthesiology & Reanimation, Istanbul, (Turkey); Phone: +90 5333120185; E-mail: drozturk28@gmail.com
ABSTRACT
Objective: Postoperative a trial fibrillation is the most commonly observed arrythmia following cardiac surgery. Both atrial fibrillation and preoperative anemia have been related to high rate of mortality and postoperative morbidity. In this systematic review and meta-analysis, we aimed to analyze whether levels of preoperative hemoglobin or hematocrit were useful biomarkers for development of postoperative atrial fibrillation after cardiac surgery or not.
Methodology: The literature screening was performed from PubMed database without any date limitation. All patients who underwent open cardiac surgery procedures were considered.
Outcome measures included the association between preoperative levels of hemoglobin/hematocrit and atrial fibrillation after cardiac surgery. The results of trials were evaluated with random or fixed effect model according to the heterogeniety. The statistical evaluation was performed by using Open Meta Analyst programme.
Results: A total of 9948 articles were found after database searching. 17 articles were included in meta-analysis consisting of 5934 patients who fulfilled inclusion criteria. The rate of postoperative atrial fibrillation was 35.6% (2114 cases out of 5934).Effect size was observed as heterogenous for studies including hematocrit (Q(df): 30.76, p<0.001, I2 :73.99%). However, it was not observed as heterogeneous for studies including hemoglobin (Q(df): 11.10, p:0.26, I2:18.96%). Analysis results of studies including hematocrit according to random effect model were SMD: 0.013, 95% CI -0.21-0.18 and p: 0.89 (p>0.05). And analysis results of studies including hemoglobin according to fixed effect model were SMD: 0.172, 95% CI -0.23- -0.11 and p<0.001.
Conclusion: The results of quantitative analysis showed that preoperative hemoglobin is associated with development of atrial fibrillation,but hematocrit is not.However, more studies may be required including both hemoglobin and hematocrit in the same trials to clearly establish this association.
Keywords: Arrhythmias, Cardiac; Atrial Fibrillation;Hemoglobin;Hematocrit;Cardiac Surgery;Meta-Analysis
Citation:Öztürkİ, Öztürk S. Association between postoperative atrial fibrillation and the levels of hemoglobin or hematocrit: a systematic review and meta-analysis.Anaesth Pain & Intensive Care 2015;19(3):--
PROSPERO registration number is CRD42015023382.
INTRODUCTİON
Postoperative atrial fibrillation (POAF) is one of the most important event among postoperative complications and also it is the most commonly observed arrythmia following cardiac surgery. Vilareal et al1 demonstrated that atrial fibrillation had been an independent risk factor responsible for increasing in-hospital mortality, stroke and length of hospital stay after cardiac surgery.
The rate of POAF depends upon type of surgery (cardiac surgery or not) and also the type of applied cardiac surgical procedures. Incidence of POAF is approximately 3% after non-cardiac surgery, andchanges between 9.8%-74% after cardiac surgery.2-4
In recent studies, Miceli et al5 reported that preoperative anemia had been related with increased rate of mortality and postoperative morbidity after cardiac surgery. The risk of death, post operativerenal dysfunction, postoperative stroke, atrial fibrillation and length of hospital stay > 7 days were greater than control group in anemic patients. Therefore, we hypothesized that preoperative levels of hemoglobin/hematocrit could be appropriate markers for prediction of atrial fibrillation. This study was aimed to analyze the association of preoperative hemoglobin or hematocrit for development of postoperative atrial fibrillation after cardiac surgery.
METHODOLOGY
Search strategy:We performed the database searching in accordance with the guideline of Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA).6 We used the electronic database search to determine whether the levels of preoperative hemoglobin or hematocrit could predict development of POAF after cardiac surgery or not. Two authors searched database until 16 February 2015. No limitation was set for publication date. PubMed was used as electronic database.
Keywords or combinations of them (e.g. cardiac surgery, heart surgery, valve surgery, coronary artery bypass grafting, postoperative atrial fibrillation, hemoglobin and hematocrit) were used for searching. Searching was limited to English language only and the articles in other languages were excluded. The methods of studies were limited within the spheres of ‘clinical trial, comparative study, multicenter study, observational study, randomized controlled trial, controlled clinical trial and evaluation studies’.
Selection of studies: The studies, regardless of the sample size, included were retrospective or prospective clinical studies.Inclusion criteria were: (i) clinical study, (ii) open cardiac surgery with off-pump or extra corporeal circulation, (iii) article in English. Exclusion criteria were: (i) experimental studies or case series(ii) articles in other than English language, and (iii) non-cardiac surgery. The articles, associated with the issue of our review but not containing the knowledge about the levels of hemoglobin or hematocrit, were also excluded. Articles containing data with figures, not numerical values, were excluded.
Data extraction: Two reviewers independently extracted data from relevant studies. We extracted publication information (first author's name, publication year, patient population, type of surgery, sample size, type of study methods). Disagreement was resolved by consensus. The mean and standard deviations of both hemoglobin and hematocrit and sample size of groups with POAF and without POAF were recorded as data.
We registrated to University of York Center of systematic reviews and dissemination. PROSPERO registration number is CRD 42015023382.
Statistical analysis:
The meta-analysis programme, Open Meta Analysist, was used for statistical analysis. The standard mean differences (SMD) and 95% confidence interval (CI) was used for analysis. The heterogeneity was evaluated with the statistics of I2. Heterogeneity was accepted as significant if I2 ≥25% and heterogeneity was evaluated with the analysis of moderators. Meta-analysis was applied by using fixed or random effect models. We performed random effect model in the presence of heterogeneity (I2>25%) and fixed effect model in absence of heterogeneity (I2<25%). Publication bias was evaluated with Begg test.
RESULTS
Flow diaphragm of database searching was shown in Figure 1.
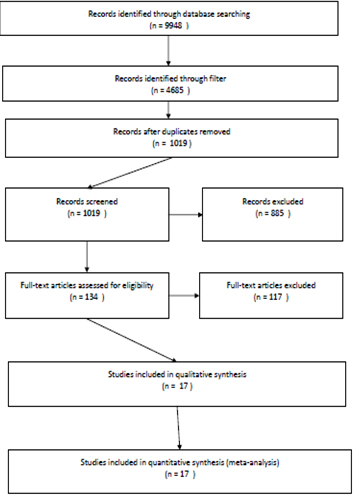 Figure 1: Flow diaphragm of search
Figure 1: Flow diaphragm of search
Records identified through database searching were 9948 and records identified through database searching with filter were 4685. After duplicates were removed, 1019 records remained. Unrelated records (n=885) were excluded after screening. Full-text of 134 articles were assessed for eligibility and 117 of them were excluded because of absence of detailed data about hemoglobin and hematocrit in each group. 17 articles were included to quantitative synthesis.(7-23) Demographical features of studies were summarized in Table 1. The ratio of development of POAF was 35.6% (2114 cases of 5934).
Table 1: Summary of studies ıncluded
Analysis results of studies including hematocrit according to random effect model were SMD: 0.013, 95% CI -0.21-0.18 and p: 0.89 (p>0.05). And analysis results of studies including hemoglobin according to fixed effect model were SMD: 0.172, 95% CI -0.23- -0.11 and p<0.001.
Effect size was observed as heterogeneous for studies including hematocrit (Q(df): 30.76, p<0.001, I2:73.99%). However, it was not observed as heterogeneous for studies including hemoglobin (Q(df): 11.10, p:0.26, I2:18.96%).Results were summarized in Figure 2 and 3.
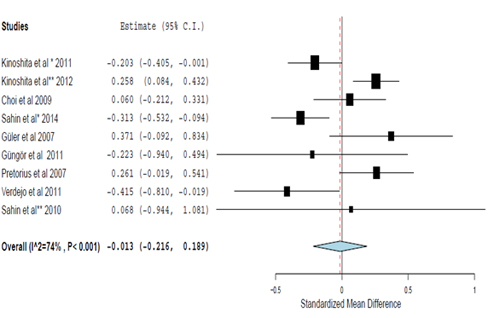
Figure 2: Analysis of studies including hematocrit
The result of evaluation of publication bias was not significant for hematocrit including studies (tau 2=0.06). However, there was publication bias for hemoglobin including studies (tau 2=0.004).
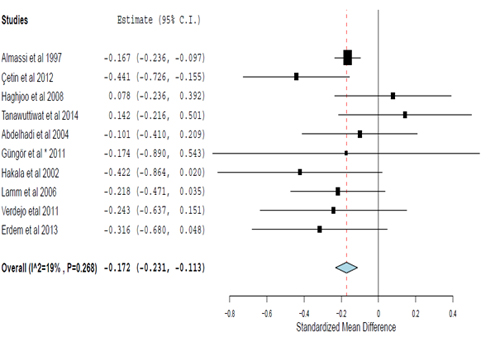
Figure 3: Analysis of studies including hemoglobin
The methods of studies (retrospective or prospective) and types of surgery (coronary artery bypass grafting surgery, valve surgery or combined CABG and valve surgery) were used as moderators for evaluation of the heterogeneity. Heterogeneity depended on the types of surgery (isolated CABGI2 =74%, combined CABG and valve surgery I2 =74%,) and the methods of trials (retrospective I2 =91%, prospective I2 =74%).
DISCUSSION
World Health Organization24 defined anemia as hemoglobin level lower than 12 g/dL in women and 13 g/dL in men.24 However, various socio demographic and life style factors affect hemoglobin levels in pregnancy,25 and also smoking can affect values of hemoglobin.26 The mean hemoglobin levels for smokers are greater than non-smokers in both men and women.26 In report of WHO prevalence of anemia is 30.2% for non-pregnant women and 12.7% for men.The prevalence of anemia in the surgical population has been reported as high as 24% in cardiac surgery.5
Preoperative anemia was associated with morbidity and mortality after cardiac surgery. In a recent study, preoperative anemia was demonstrated as an independent predictor of mortality and post operative renal dysfunction and length of hospital stay > 7 days in multi variable logistic regression.5 On the other hand, Mirhosseini et al27 showed anemia had not effect on the incidence of atrial fibrillation, early complications and mortality in patients undergoing off-pump CABG.27 Chua et al28 found anemia as a risk factor in univariate analysis but not in multivariate analysis for POAF. Hernández-Leiva et al29 showed an association between POAF and hemoglobin with multivariate hemoglobin analysis (adjusted odds ratio:0.75 95% CI (0.28-2.01)).
For diagnosis and follow up anemia in clinical practice, both hemoglobin and hematocrit are usually used and also their levels can direct decision of blood transfusion.In this meta-analysis, we used two measures usually selected for diagnosis of anemia and also determination of blood transfusion decision in clinical practice. The accepted simple relationship between them is conventionally formulated as hematocrit (%)=hemoglobin(g/dL)x3.29However, conventional formula is not always accurate for all ages and for all levels of hemoglobin.30 Flores-Torres et al31 estimated the level of as hemoglobin=(Hematocrit/3.135)+ 0.257.
In our analysis, the main difference for prediction of POAF between preoperative hemoglobin and hematocrit, depends on the absence of fixed formula to convert them to each other. They must be separately evaluated in those similar risk analysis. On the other hand, we think that the main reason of heterogeneous of studies including hematocrit smaller sample size of studies to evaluate POAF.
Determination of certain decision whether preoperative levels of hemoglobin or hematocrit predict POAF or not, is difficult because of two reasons. First, POAF is multifactorial complication of cardiovascular surgery. And second, limited numbers of trials that contain both hematocrit and hemoglobin in the same one.
Almassi et al7 found POAF was associated not only with hemoglobin level and also with age, blood pressure, creating in levels, cardiopulmonary bypass time and ischemic time in univariate analysis.In a current study, hematocrit and age is determined as predictors.10 Çetin et al showed age and gender were also predictors ofPOAF.8 Systemic diseases including diabetes mellitus11,18 and chronic obstructive lung disease 7 were found as risk factors for POAF in three studies.
The main predictor of POAF was age in most of the trials.7,8,10-12,16-20,22 However age was not significantly related to POAF according to multivariate analysis in three trials.13-15,20
Limitations:
The main limitation of our analysis was the limited data of studies. Except two studies15,21 all of them included only hemoglobin or hematocrit. Therefore, it was difficult to analysis them on the same conditions (studies). Because of that reason, more trials about POAF including both preoperative hemoglobin and hematocrit levels, can certainly determine whether there is a difference between these measures or not.
CONCLUSION
Although there are limited studies, preoperative hemoglobin levels can predict POAF following cardiac surgery but not hematocrit. However, there is a need for more studies including both hemoglobin and hematocrit.
Author Contribution:IO and SO shared concept, data acquisition, statistical analysis and manuscript preparation
REFERENCES
1Medeniyet University Göztepe Education and Research Hospital, Department of Anesthesiology and Reanimation, Istanbul, (Turkey)
2Dr. Siyami Ersek Cardiovascular Surgery Education and Research Hospital, Department of Cardiovascular Surgery, Istanbul, (Turkey)
Correspondence: İbrahim Öztürk, MD, Medeniyet University Göztepe Education & Research Hospital, Department of Anesthesiology & Reanimation, Istanbul, (Turkey); Phone: +90 5333120185; E-mail: drozturk28@gmail.com
ABSTRACT
Objective: Postoperative a trial fibrillation is the most commonly observed arrythmia following cardiac surgery. Both atrial fibrillation and preoperative anemia have been related to high rate of mortality and postoperative morbidity. In this systematic review and meta-analysis, we aimed to analyze whether levels of preoperative hemoglobin or hematocrit were useful biomarkers for development of postoperative atrial fibrillation after cardiac surgery or not.
Methodology: The literature screening was performed from PubMed database without any date limitation. All patients who underwent open cardiac surgery procedures were considered.
Outcome measures included the association between preoperative levels of hemoglobin/hematocrit and atrial fibrillation after cardiac surgery. The results of trials were evaluated with random or fixed effect model according to the heterogeniety. The statistical evaluation was performed by using Open Meta Analyst programme.
Results: A total of 9948 articles were found after database searching. 17 articles were included in meta-analysis consisting of 5934 patients who fulfilled inclusion criteria. The rate of postoperative atrial fibrillation was 35.6% (2114 cases out of 5934).Effect size was observed as heterogenous for studies including hematocrit (Q(df): 30.76, p<0.001, I2 :73.99%). However, it was not observed as heterogeneous for studies including hemoglobin (Q(df): 11.10, p:0.26, I2:18.96%). Analysis results of studies including hematocrit according to random effect model were SMD: 0.013, 95% CI -0.21-0.18 and p: 0.89 (p>0.05). And analysis results of studies including hemoglobin according to fixed effect model were SMD: 0.172, 95% CI -0.23- -0.11 and p<0.001.
Conclusion: The results of quantitative analysis showed that preoperative hemoglobin is associated with development of atrial fibrillation,but hematocrit is not.However, more studies may be required including both hemoglobin and hematocrit in the same trials to clearly establish this association.
Keywords: Arrhythmias, Cardiac; Atrial Fibrillation;Hemoglobin;Hematocrit;Cardiac Surgery;Meta-Analysis
Citation:Öztürkİ, Öztürk S. Association between postoperative atrial fibrillation and the levels of hemoglobin or hematocrit: a systematic review and meta-analysis.Anaesth Pain & Intensive Care 2015;19(3):--
PROSPERO registration number is CRD42015023382.
INTRODUCTİON
Postoperative atrial fibrillation (POAF) is one of the most important event among postoperative complications and also it is the most commonly observed arrythmia following cardiac surgery. Vilareal et al1 demonstrated that atrial fibrillation had been an independent risk factor responsible for increasing in-hospital mortality, stroke and length of hospital stay after cardiac surgery.
The rate of POAF depends upon type of surgery (cardiac surgery or not) and also the type of applied cardiac surgical procedures. Incidence of POAF is approximately 3% after non-cardiac surgery, andchanges between 9.8%-74% after cardiac surgery.2-4
In recent studies, Miceli et al5 reported that preoperative anemia had been related with increased rate of mortality and postoperative morbidity after cardiac surgery. The risk of death, post operativerenal dysfunction, postoperative stroke, atrial fibrillation and length of hospital stay > 7 days were greater than control group in anemic patients. Therefore, we hypothesized that preoperative levels of hemoglobin/hematocrit could be appropriate markers for prediction of atrial fibrillation. This study was aimed to analyze the association of preoperative hemoglobin or hematocrit for development of postoperative atrial fibrillation after cardiac surgery.
METHODOLOGY
Search strategy:We performed the database searching in accordance with the guideline of Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA).6 We used the electronic database search to determine whether the levels of preoperative hemoglobin or hematocrit could predict development of POAF after cardiac surgery or not. Two authors searched database until 16 February 2015. No limitation was set for publication date. PubMed was used as electronic database.
Keywords or combinations of them (e.g. cardiac surgery, heart surgery, valve surgery, coronary artery bypass grafting, postoperative atrial fibrillation, hemoglobin and hematocrit) were used for searching. Searching was limited to English language only and the articles in other languages were excluded. The methods of studies were limited within the spheres of ‘clinical trial, comparative study, multicenter study, observational study, randomized controlled trial, controlled clinical trial and evaluation studies’.
Selection of studies: The studies, regardless of the sample size, included were retrospective or prospective clinical studies.Inclusion criteria were: (i) clinical study, (ii) open cardiac surgery with off-pump or extra corporeal circulation, (iii) article in English. Exclusion criteria were: (i) experimental studies or case series(ii) articles in other than English language, and (iii) non-cardiac surgery. The articles, associated with the issue of our review but not containing the knowledge about the levels of hemoglobin or hematocrit, were also excluded. Articles containing data with figures, not numerical values, were excluded.
Data extraction: Two reviewers independently extracted data from relevant studies. We extracted publication information (first author's name, publication year, patient population, type of surgery, sample size, type of study methods). Disagreement was resolved by consensus. The mean and standard deviations of both hemoglobin and hematocrit and sample size of groups with POAF and without POAF were recorded as data.
We registrated to University of York Center of systematic reviews and dissemination. PROSPERO registration number is CRD 42015023382.
Statistical analysis:
The meta-analysis programme, Open Meta Analysist, was used for statistical analysis. The standard mean differences (SMD) and 95% confidence interval (CI) was used for analysis. The heterogeneity was evaluated with the statistics of I2. Heterogeneity was accepted as significant if I2 ≥25% and heterogeneity was evaluated with the analysis of moderators. Meta-analysis was applied by using fixed or random effect models. We performed random effect model in the presence of heterogeneity (I2>25%) and fixed effect model in absence of heterogeneity (I2<25%). Publication bias was evaluated with Begg test.
RESULTS
Flow diaphragm of database searching was shown in Figure 1.
Figure 1: Flow diaphragm of search
Records identified through database searching were 9948 and records identified through database searching with filter were 4685. After duplicates were removed, 1019 records remained. Unrelated records (n=885) were excluded after screening. Full-text of 134 articles were assessed for eligibility and 117 of them were excluded because of absence of detailed data about hemoglobin and hematocrit in each group. 17 articles were included to quantitative synthesis.(7-23) Demographical features of studies were summarized in Table 1. The ratio of development of POAF was 35.6% (2114 cases of 5934).
Table 1: Summary of studies ıncluded
|
Reference |
Year |
Study design |
Surgery |
POAF (n) |
Non-POAF (n) |
| Abdelhadi12 |
2004 |
Prospective |
CABG+ valve |
60 |
121 |
| Güngör15 |
2011 |
Prospective |
CABG |
10 |
30 |
| Hakala16 |
2002 |
Prospective |
CABG |
31 |
57 |
| Lamm19 |
2006 |
Prospective |
CABG+ valve |
99 |
154 |
| Verdejo21 |
2011 |
Prospective |
CABG+ valve |
32 |
112 |
| Erdem14 |
2013 |
Retrospective |
CABG |
38 |
127 |
| Almassi7 |
1997 |
Retrospective |
CABG+ valve |
1143 |
2712 |
| Çetin8 |
2012 |
Prospective |
CABG |
62 |
210 |
| Haghjoo22 |
2008 |
Prospective |
CABG |
46 |
256 |
| Tanawuttiwat23 |
2014 |
Retrospective |
Valve |
52 |
71 |
| Choi13 |
2009 |
Prospective |
CABG |
66 |
249 |
| Kinoshita17 |
2011 |
Retrospective |
CABG |
121 |
431 |
| Kinoshita18 |
2012 |
Retrospective |
CABG |
159 |
646 |
| Pretorius20 |
2007 |
Prospective |
CABG+ valve |
67 |
186 |
| Şahin10 |
2014 |
Prospective |
CABG |
96 |
501 |
| Şahin9 |
2010 |
Prospective |
CABG |
5 |
15 |
| Güler11 |
2007 |
Prospective |
CABG |
27 |
56 |
Effect size was observed as heterogeneous for studies including hematocrit (Q(df): 30.76, p<0.001, I2:73.99%). However, it was not observed as heterogeneous for studies including hemoglobin (Q(df): 11.10, p:0.26, I2:18.96%).Results were summarized in Figure 2 and 3.
Figure 2: Analysis of studies including hematocrit
The result of evaluation of publication bias was not significant for hematocrit including studies (tau 2=0.06). However, there was publication bias for hemoglobin including studies (tau 2=0.004).
Figure 3: Analysis of studies including hemoglobin
The methods of studies (retrospective or prospective) and types of surgery (coronary artery bypass grafting surgery, valve surgery or combined CABG and valve surgery) were used as moderators for evaluation of the heterogeneity. Heterogeneity depended on the types of surgery (isolated CABGI2 =74%, combined CABG and valve surgery I2 =74%,) and the methods of trials (retrospective I2 =91%, prospective I2 =74%).
DISCUSSION
World Health Organization24 defined anemia as hemoglobin level lower than 12 g/dL in women and 13 g/dL in men.24 However, various socio demographic and life style factors affect hemoglobin levels in pregnancy,25 and also smoking can affect values of hemoglobin.26 The mean hemoglobin levels for smokers are greater than non-smokers in both men and women.26 In report of WHO prevalence of anemia is 30.2% for non-pregnant women and 12.7% for men.The prevalence of anemia in the surgical population has been reported as high as 24% in cardiac surgery.5
Preoperative anemia was associated with morbidity and mortality after cardiac surgery. In a recent study, preoperative anemia was demonstrated as an independent predictor of mortality and post operative renal dysfunction and length of hospital stay > 7 days in multi variable logistic regression.5 On the other hand, Mirhosseini et al27 showed anemia had not effect on the incidence of atrial fibrillation, early complications and mortality in patients undergoing off-pump CABG.27 Chua et al28 found anemia as a risk factor in univariate analysis but not in multivariate analysis for POAF. Hernández-Leiva et al29 showed an association between POAF and hemoglobin with multivariate hemoglobin analysis (adjusted odds ratio:0.75 95% CI (0.28-2.01)).
For diagnosis and follow up anemia in clinical practice, both hemoglobin and hematocrit are usually used and also their levels can direct decision of blood transfusion.In this meta-analysis, we used two measures usually selected for diagnosis of anemia and also determination of blood transfusion decision in clinical practice. The accepted simple relationship between them is conventionally formulated as hematocrit (%)=hemoglobin(g/dL)x3.29However, conventional formula is not always accurate for all ages and for all levels of hemoglobin.30 Flores-Torres et al31 estimated the level of as hemoglobin=(Hematocrit/3.135)+ 0.257.
In our analysis, the main difference for prediction of POAF between preoperative hemoglobin and hematocrit, depends on the absence of fixed formula to convert them to each other. They must be separately evaluated in those similar risk analysis. On the other hand, we think that the main reason of heterogeneous of studies including hematocrit smaller sample size of studies to evaluate POAF.
Determination of certain decision whether preoperative levels of hemoglobin or hematocrit predict POAF or not, is difficult because of two reasons. First, POAF is multifactorial complication of cardiovascular surgery. And second, limited numbers of trials that contain both hematocrit and hemoglobin in the same one.
Almassi et al7 found POAF was associated not only with hemoglobin level and also with age, blood pressure, creating in levels, cardiopulmonary bypass time and ischemic time in univariate analysis.In a current study, hematocrit and age is determined as predictors.10 Çetin et al showed age and gender were also predictors ofPOAF.8 Systemic diseases including diabetes mellitus11,18 and chronic obstructive lung disease 7 were found as risk factors for POAF in three studies.
The main predictor of POAF was age in most of the trials.7,8,10-12,16-20,22 However age was not significantly related to POAF according to multivariate analysis in three trials.13-15,20
Limitations:
The main limitation of our analysis was the limited data of studies. Except two studies15,21 all of them included only hemoglobin or hematocrit. Therefore, it was difficult to analysis them on the same conditions (studies). Because of that reason, more trials about POAF including both preoperative hemoglobin and hematocrit levels, can certainly determine whether there is a difference between these measures or not.
CONCLUSION
Although there are limited studies, preoperative hemoglobin levels can predict POAF following cardiac surgery but not hematocrit. However, there is a need for more studies including both hemoglobin and hematocrit.
Author Contribution:IO and SO shared concept, data acquisition, statistical analysis and manuscript preparation
REFERENCES
- Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, et al. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol 2004;43(5):742-8.[PubMed] [Free full text]
- Siebert J, Anisimowicz L, Lango R, Rogowski J, Pawlaczyk R, Brzezinski M,et al. Atrial fibrillation after coronaryartery bypass grafting: does the type of procedure influencethe early postoperative incidence? Eur J Cardiothorac Surg2001;19(4):455-9. [PubMed] [Free full text]
- Bhave PD, Goldman LE, Vittinghoff E, Maselli J, Auerbach A. Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery. Am Heart J 2012 ;164(6):918-24. [PubMed] [Free full text] doi: 10.1016/j.ahj.2012.09.004.
- Helgadottir S, Sigurdsson MI, Ingvarsdottir IL, Arnar DO, Gudbjartsson T.Atrial fibrillation following cardiac surgery: risk analysis and long-term survival. J Cardiothorac Surg 2012;7:87. [PubMed] [Free full text] doi: 10.1186/1749-8090-7-87.
- Miceli A, Romeo F, Glauber M, de Siena PM, Caputo M, Angelini GD. Preoperativeanemia increases mortality and postoperative morbidity after cardiac surgery. J Cardiothorac Surg. 2014;5;9:137. [PubMed] [Free full text] doi: 10.1186/1749-8090-9-137.
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:2535. [PubMed] [Free full text] doi: 10.1136/bmj.b2535.
- Almassi GH, Schowalter T, Nicolosi AC, Aggarwal A, Moritz TE, Henderson WG, et al. Atrial fibrillation after cardiac surgery: a major morbid event? Ann Surg. 1997;226:501-11. [PubMed] [Free full text]
- Çetin M, Kocaman SA, Erdoğan T, Durakoğlugil ME, Çiçek Y, Bozok Şet al. Fragmented QRS may predict postoperative a trial fibrillation in patients undergoing isolated coronary artery bypass graft surgery. Anadolu Kardiyol Derg. 2012;12(7):576-83. [PubMed] [Free full text]doi: 10.5152/akd.2012.184.
- Sahin V, Kaplan M, Bilsel S, Filizcan U, Cetemen S, Bayserke O,et al. The relation between blood and tissue magnesium levels and development of atrial fibrillation after coronary artery bypass surgery. Anadolu Kardiyol Derg. 2010;10(5):446-51. [PubMed] [Free full text]doi:10.5152/akd.2010.144.
- Sahin İ, Özkaynak B, Karabulut A, Avcı Iİ, Okuyan E, Mert B, et al. Impact of coronary collateral circulation andseverity of coronary artery disease in the development of postoperative atrialfibrillation. Interact Cardiovasc Thorac Surg. 2014;19(3):394-7. [PubMed][Free full text] doi: 10.1093/icvts/ivu158.
- Guler N, Ozkara C, Dulger H, Kutay V, Sahin M, Erbilen E, et al. Do cardiac neuropeptides play a role in the occurrence of atrial fibrillation coronary bypass surgery? Ann Thorac Surg. 2007;83(2):532-7. [PubMed]
- Abdelhadi RH, Gurm HS, Van Wagoner DR, Chung MK. Relation of an exaggeratedrise in white blood cells after coronary bypass or cardiac valve surgery todevelopment of atrial fibrillation postoperatively. Am J Cardiol. 2004:1;93(9):1176-8. [PubMed]
- Choi YS, Shim JK, Hong SW, Kim DH, Kim JC, Kwak YL. Risk factors of atrialfibrillation following off-pump coronary artery bypass graft surgery: predictivevalue of C-reactive protein and transfusion requirement. Eur J Cardiothorac Surg.2009;36(5):838-43. [PubMed] [Free full text]doi: 10.1016/j.ejcts.2009.05.003.
- Erdem K, Ayhan S, Ozturk S, Bugra O, Bozoglan O, Dursin H,et al.Usefulness of the mean platelet volume for predicting new-onset atrialfibrillation after isolated coronary artery bypass grafting. Platelets.2014;25(1):23-6. [PubMed] [Free full text]doi: 10.3109/09537104.2013.767443.
- Gungor H, Ayik MF, Kirilmaz B, Ertugay S, Gul I, Yildiz BS,et al. Serum resistin level: as a predictor of atrial fibrillation aftercoronary artery bypass graft surgery. Coron Artery Dis. 2011;22:484-90. [PubMed] doi: 10.1097/MCA.0b013e32834b67bb. [Free full text]
- Hakala T, Hedman A, Turpeinen A, Kettunen R, Vuolteenaho O, Hippeläinen M, et al. Prediction of atrial fibrillation after coronary artery bypass grafting by measuring atrial peptide levels and preoperative atrial dimensions. Eur JCardiothorac Surg. 2002;22(6):939-43. [PubMed] [Free full text]
- Kinoshita T, Asai T, Takashima N, Hosoba S, Suzuki T, Kambara A, et al. Preoperative C-reactive protein and atrial fibrillation after off-pumpcoronary bypass surgery. Eur J Cardiothorac Surg. 2011;40(6):1298-303. [PubMed] [Free full text] doi: 10.1016/j.ejcts.2011.03.027.
- Kinoshita T, Asai T, Suzuki T, Kambara A, Matsubayashi K. Preoperativehemoglobin A1c predicts atrial fibrillation after off-pump coronary bypasssurgery. Eur J Cardiothorac Surg. 2012;41(1):102-7. [PubMed] [Free full text] doi: 10.1016/j.ejcts.2011.04.011.
- Lamm G, Auer J, Weber T, Berent R, Ng C, Eber B. Postoperative white blood cell count predicts atrial fibrillation after cardiac surgery. J Cardio thoracVasc Anesth. 2006;20(1):51-6. [PubMed]
- Pretorius M, Donahue BS, Yu C,Roden DM, Brown NJ, et al. Plasminogen activator inhibitor-1 as a predictor of postoperative atrial fibrillation after cardiopulmonary bypass. Circulation. 2007;116(11 Suppl):11-7. [PubMed] [Free full text] doi: 10.1161/CIRCULATIONAHA.106.677906
- Verdejo H, Roldan J, Garcia L, Del Campo A, Becerra E, Chiong M,et al.Systemic vascular cell adhesion molecule-1 predicts the occurrence of post-operative atrial fibrillation. Int J Cardiol. 2011;150(3):270-6. [PubMed] doi: 10.1016/j.ijcard.2010.04.033.
- Haghjoo M, Basiri H, Salek M, Sadr-Ameli MA, Kargar F, Raissi K,et al. Predictors of postoperative a trial fibrillation after coronary artery bypass graft surgery.Indian Pacing Electro physiol J. 2008;1(8):94-101. [Free full text]
- Tanawuttiwat T, O'Neill BP, Cohen MG, Chinthakanan O, Heldman AW, MartinezCA, et al.New-onset atrial fibrillation after aortic valve replacement: comparison of transfemoral, transapical, transaortic, and surgical approaches.J Am Coll Cardiol. 2014;63(15):1510-9. [PubMed] [Free full text] doi: 10.1016/j.jacc.2013.11.046.
- Benoist B, McLean E, Egli I, Cogswell M. Worldwide prevalence of anaemia 1993–2005. Available on http://whqlibdoc.who.int/publications/2008/9789241596657_eng.pdf (Accessed on 16/02/2015).
- Gaillard R, Eilers PH, Yassine S, Hofman A, Steegers EA, Jaddoe VW. Risk factors and consequences of maternal anaemia and elevated haemoglobin levels during pregnancy: a population-based prospective cohort study. Paediatr Perinat Epidemiol. 2014;28:213-26. [PubMed] doi: 10.1111/ppe.12112.
- Nordenberg D, Yip R, Binkin NJ. The effect of cigarette smoking on hemoglobin levels and anemia screening. JAMA. 1990 Sep 26;264(12):1556-9. [PubMed] [Free full text]
- Mir hosseini SJ, Sayegh SA. Effect of preoperative anemia on short term clinical outcomes in diabetic patients after elective off-pump CABG surgery. Acta Med Iran. 2012;50(9):615-8. [PubMed]
- Chua SK, Shyu KG, Lu MJ Hung HF, Cheng JJ, Lee SH,et al. Association between renal function, diastolic dysfunction, and postoperative atrial fibrillation following cardiac surgery. Circ J 2013;77(9):2303–10. [PubMed] [Free full text] doi.org/10.1253/circj.CJ-13-0273
- Hernández-Leiva E, Dennis R, Isaza D, Umaña JP. Hemoglobin and B-type natriuretic peptide preoperative values but not inflammatory markers, are associated with postoperative morbidity in cardiac surgery: a prospective cohort analytic study. J Cardiothorac Surg. 2013;5;8:170. [PubMed] [Free full text] doi: 10.1186/1749-8090-8-170.
- Carneiro IA, Drakeley CJ, Owusu-Agyei S, Mmbando B, Chandramohan D.Haemoglobin and haematocrit: is the threefold conversion valid for assessinganaemia in malaria-endemic settings? Malar J. 2007;22;6:67. [PubMed][Free full text]
- Flores-Torres J, Echeverría-Ortega M, Arria-Bohorquez M, Hidalgo G,Albano-Ramos C, Sanz R,et al. Differences between observed and estimated by hematocrit hemoglobin and its relevance in the diagnosis of anemia among coastal population in Venezuela: analysis of the second national study of human growth and development (SENACREDH). Rev Peru Med Exp Salud Publica. 2011;2891):47-53. [PubMed][Free full text]