*Head, Department of Anesthesiology, Karnataka Institute of Medical Sciences, P B Road, Vidyanagar, Hubli, Karnataka 580022, (India)
**Junior Consultant, Medical ICU, AJ Hospital and Research Centre, Kuntikana, Mangalore, (India)
Correspondence: Dr. SafiyaI.Shaikh, 7-Narayanpur, Opposite TV Tower, Haliyal Road, Dharwad-580008 (India)
ABSTRACT
Background & Objectives: Caudal analgesia is an accepted and popular method of providing intra and postoperative analgesia for abdominal, perineal and lower limb surgeries in children. Caudal epidural block with bupivacaine is one of the most common regional anesthetic technique used in children.Several adjuncts such as opioids, ketamine, midazolam and neostigmine have been used with bupivacaine to prolong its action and thus extend the duration of postoperative analgesia provided by ‘single shot’ caudal technique. Clonidine, an α2 agonist has extensively been used in neuraxial blocks and peripheral nerve blocks to prolong the action of bupivacaine without significant respiratory depression after systemic, epidural and spinal administration. Hence, this study was conducted to know the efficacy and safety of clonidine as an adjuvant to bupivacaine in single shot caudal block in children.
Methodology: This study was conducted among 60 children in the age group of 1-12 years coming for various elective sub-umbilical surgeries. They were divided into two groups of 30 each. Group A received caudal 0.25% bupivacaine plain with 0.5 ml Normal saline and Group B received caudal 0.25% bupivacaine 1 ml/Kg with clonidine 1µg/Kg as an adjuvant made to 0.5 ml with normal saline. The various parameters studied were intraoperative hemodynamic changes, onset of action, duration of postoperative analgesia, postoperative analgesic requirement, duration of postoperative sedation and incidence of side effects. Pain and sedation assessment was done at 0, 1, 2, 3, 4, 8, 12, 16, 20 and 24 hour after surgery.
Results: The groups were similar in age, sex and weight. The hemodynamic parameters like heart rate (HR), mean arterial pressure (MAP), oxygen saturation (SpO2) were also similar between the two groups before and after administering caudal block. The mean duration of analgesia in group B (506.67 ± 43.81min) was significantly longer (p< 0.001) than in group A (270.67 ± 43.70min). The pain score in the two groups were similar upto 3 hrs but was higher in Group A as compared to Group B. The duration of sedation is significant for upto 4 hrs in Group B than Group A. The number of rescue analgesics used was significantly more in Group A as compared to Group B. Incidence of bradycardia, hypotension, vomiting were not significant in both the groups.
Conclusion: This study showed that the addition of clonidine in the dose of 1μg/kg to 0.25% bupivacaine plain 1ml/kg prolonged the duration of analgesia with better sedation in children with less post operative analgesic requirement after a single shot caudal block with minimal side effects in children.
Key words: Anesthesia, Caudal;Caudal block;Anesthesia, Epidural;Clonidine;Adrenergic alpha-2 Receptor Agonists; Pediatric; Bupivacaine; Randomized Controlled Trial
Citation: Shaikh SI, Atlapure BB. Clonidine as an adjuvant for bupivacaine in caudal analgesia for sub-umbilical surgery: A prospective randomized double blind study. Anaesth Pain & Intensive Care 2015;19(3):240-246
INTRODUCTION Pain is defined by the international association for study of pain as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”.<sup>1</sup> The inability to react and to answer questions as adults do has contributed to the false impression that children do not feel pain as much as adults do.<sup>2</sup>
It is now established that newborn infants, even preterm, can appreciate pain and react to it with tachycardia, hypertension, increased neuro-endocrine response and intracranial pressure.<sup>3</sup>
Regional anesthetic techniques reduce the overall intra-operative requirement of both inhaled and intravenous anesthetic agents and allow more rapid return of the consciousness while providing effective postoperative pain relief with minimal sedation.<sup>4</sup> Caudal epidural block is one of the most popular and commonly performed regional blocks in pediatric anesthesia.<sup>5</sup> It is a safe and reliable technique that can be used with general anesthesia for intraoperative and postoperative analgesia in patients undergoing short surgical procedures below the umbilicus.<sup>6</sup> The main disadvantage of caudal analgesia is duration of action after a single injection which is limited by duration of action of local anesthetics. Placement of a catheter has an inherent risk of infection. Prolongation of caudal analgesia using a single-shot technique has been achieved by the addition of various adjuvants such as opioids, ketamine, neostigmine, midazolam and α-2 agonists. Many of these adjuvants have side effects like respiratory depression, vomiting, pruritus etc.<sup>7,8</sup> Bupivacaine is the most commonly used local anesthetic for this purpose. The limitation of bupivacaine is the short duration of action, about four to six hours, when administered as a ‘single shot technique’.
Several adjuncts such as opioids, ketamine, midazolam, clonidine and neostigmine have been used with bupivacaine to prolong its action, and thus extend the duration of postoperative analgesia provided by the ‘single shot’ caudal technique.
Clonidine, an α-2 agonist has extensively been used in neuraxial blocks and peripheral nerve blocks to prolong the action of bupivacaine. It is one of the most commonly used additives with bupivacaine for caudal analgesia in children. However, the role of clonidine in improving and prolonging the analgesia produced by caudal bupivacaine is highly variable in different published studies.<sup>9</sup> We conducted this study to determine the efficacy of clonidine as an adjuvant to bupivacaine in caudal analgesia for sub-umbilical surgeries.
METHODOLOGY This prospective randomized double blind study was conducted at Karnataka Institute of Medical Sciences, Hubli from January 2013 to December 2013. This study included 60 children, of both genders, coming for various elective sub-umbilical surgical procedures such as herniotomy, circumcision, orchidopexy, urethroplasty etc. After obtaining clearance from the hospital ethical committee a written informed consent was obtained from parents before commencing the study. Patients in the age group of 1 to 12 years, ASA Grade1 and 2 status, giving informed written consent were scheduled to undergo elective sub-umbilical, perineal and lower limb surgeries. Patients aged more than 12 years, ASA Grade 3 or more and any contraindications to epidural anesthesia like sacral spine abnormalities, local site infection & coagulation abnormalities, hematological diseases, neurologic, psychiatric disease, severe renal and hepatic derangement, on anticoagulants, anti-psychotic drugs, tricyclic antidepressants, alpha-2 adrenergic agonists and beta blockers and parental refusal were excluded from the study.
Patients were randomly allocated to two different groups A and B of thirty each. Randomization was done by simple lottery method. Sample size calculation was done using power analysis of the study suiting the non-parametric data comparison by Student’s -t test. All health-care personnel, the patients, and their parents or guardians were blinded to the caudal medications administered. All medications were prepared by anesthesiologists not participating in the study except for preparing the drugs. The anesthesiologist who administered anesthesia also monitored the patient peri-operatively, but was unaware of the study drug.
Group A(n = 30) received bupivacaine 0.25%, 1ml/kg + 0.5ml normal saline.
Group B(n = 30) received bupivacaine 0.25%, 1ml/kg + clonidine 1μg/kg making the volume 0.5 ml with normal saline.
The aim of this study was to assess the efficacy and the safety of addition of clonidine as an adjuvant to bupivacaine on postoperative analgesia in pediatric patients following single shot caudal block in sub-umbilical surgeries. We studied the hemodynamic changes, the duration of postoperative analgesia, postoperative sedation, the rescue analgesic requirement and the incidence of side effects e.g. hypotension, bradycardia, respiratory depression and postoperative nausea and vomiting. All patients were visited on the pre-operative day and relevant demographic data collected. A thorough preoperative evaluation was done including history, general physical examination, systemic examination, airway assessment and spine. Baseline vital parameters were noted. Relevant laboratory investigations were done in all patients. Informed consent was obtained from the appropriate person. Solid foods were restricted for 6 hours, breast milk for 4 hours and clear fluids for 2 hours prior to surgery. All patients were pre-medicated with syrup Midazolam 0.5mg/kg, 30 min prior to induction.
In the operation theatre standard monitoring was instituted. The continuous monitoring of heart rate (HR), electrocardiogram (ECG), mean arterial pressure (MAP) and oxygen saturation (SpO2) were done and recorded before surgery and every 5 min till the end of surgery. Once Intravenous access was secured and an appropriate crystalloid infusion was started according to the calculated requirements. Patient was induced with inj. glycopyrrolate 0.01 mg/kg IV as premedication and inj. propofol 2 mg/kg along with 1-3% halothane in oxygen using appropriate sized anatomical face mask and Jackson Rees circuit. Halothane concentration was titrated in nitrous oxide and oxygen to maintain adequate depth of anesthesia.
While the patient was breathing spontaneously, he/she was gently placed in left lateral position; vitals were checked again including adequacy of breathing.Under strict aseptic conditions, after confirmation of caudal epidural space the study drug was injected by using a sterile 27G hypodermic needle according to the group allocation.
The inhaled concentration of halothane was adjusted to achieve hemodynamic changes within 30% of the baseline values. No other narcotics, analgesics or sedatives were used intra-operatively. An intra-operative decrease of MAP or HR by 30% from the baseline value was defined as hypotension or bradycardia respectively, recorded and treated by fluid bolus, mephentermine or atropine as necessary.
At the end of surgery, 100% oxygen through a face mask was administered for 3-5 min. Once the vitals were stable and the child was awake, the child was shifted and placed in lateral position in the postoperative recovery room and monitored for four hours with SpO2, respiratory rate, NIBP and heart rate every 5 minutes. After that the child was shifted to the ward. Complications like dural puncture, vascular puncture, nausea and vomiting were noted.
Postoperative analgesia was assessed by using the pediatric observational FLACC pain scale with its 0–10 score range.Each child’s pain intensity was assessed upon arrival and then every hourly till the time of discharge from the PACU and then every 4 h for the first 24 h after caudal block.<sup>10</sup>
If the FLACC pain scale score was noted at any time to be 4 or more, paracetamol suppository 40 mg /kg rectally was administered as loading dose to achieve a FLACC scale score of 3 or less and then followed by 20 mg/kg every 6 hrs.The duration of adequate caudal analgesia defined as time interval between the administration of caudal block and the first requirement of supplementary analgesia for the patient was recorded.
Sedation was assessed using the sedation score where the duration of sedation was defined as the time from the onset of analgesia to spontaneous eye opening.(Sedation score <1).Sedation score as taken as 0, 1, 2 or 3 according to child’s alertness, and arousability, and it was noted whether the child was in normal sleep, recorded as X.
Statistical analysis: Descriptive statistical analysis was carried out. Data entry was done using MS Excel 2007 computer software. Data were analyzed using SPSS version 17. Numerical variables are presented as mean and standard deviation (SD). Categorical variables are presented as frequency (%). The difference between the two groups with regards to continuous variables was assessed by Student’s- t test and categorical variables by Chi-square test.Non parametric parameters were analyzed by Mann-Whitney Test.For all the tests,p value of 0.05 and less was considered statistical significant and a value of 0.001 and less was considered as statistically highly significant. We intended to study the safety and efficacy of clonidine as an adjuvant to bupivacaine in both the groups in pediatric caudal block and compared the duration of analgesia between the two groups.
RESULTS: There was no significant differences in the demographic data of the patients between the two groups(p>0.05)(Table 1). Hemodynamic parameters e.g. heart rate, SBP, DBP, MAP and SpO2 were recorded once in every 5 min till the end of the surgery and the results were compared between both the groups. The differences between the two groups were not significant. The heart rate parameters are depicted in Table 2.
Table 1: Demographic data (Mean±SD)
|
Parameter |
Group A |
Group B |
P value |
| Age (months) |
74.40±37.34 |
58.30±27.92 |
>0.05 |
| Male : Female |
28 : 2 |
27 : 3 |
|
| Weight (kg) |
14±.12 |
14.67±3.87 |
Time intervals (min) |
Group A (Mean ± SD) |
Group B (Mean ± SD) |
Mean difference |
t-value |
p-value |
| Baseline | 120.47 ± 18.27 |
128.30 ± 24.36 |
-7.83 |
-1.4090 |
0.1642 |
| 5 | 126.43 ± 14.74 |
123.87 ± 21.20 |
2.57 |
0.5445 |
0.5882 |
| 10 | 115.73 ± 14.64 |
116.03 ± 19.27 |
-0.30 |
-0.0679 |
0.9461 |
| 15 | 114.83 ± 14.73 |
111.57 ± 18.36 |
3.27 |
0.7600 |
0.4503 |
| 30 | 114.83 ± 14.73 |
110.10 ± 18.26 |
4.73 |
1.1048 |
0.2738 |
| 45 | 114.83 ± 14.73 |
110.27 ± 18.15 |
4.57 |
1.0698 |
0.2891 |
| 60 | 114.83 ± 14.73 |
110.27 ± 18.15 |
4.57 |
1.0698 |
0.2891 |
| 90 | 114.83 ± 14.73 |
110.27 ± 18.15 |
4.57 |
1.0698 |
0.2891 |
| 120 | 114.83 ± 14.73 |
110.27 ± 18.15 |
4.57 |
1.0698 |
0.2891 |
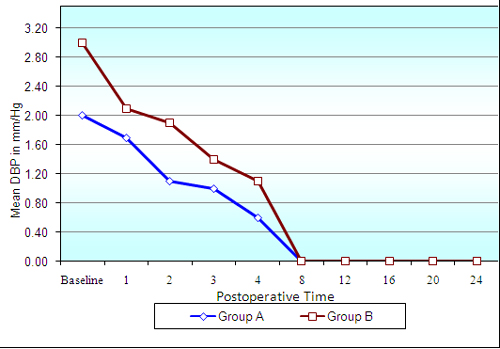
Figure 1: Comparison of changes in sedation scores
The pediatric observational FLACC pain score was below 4 at the end of first and second hour in both the groups and did not require any analgesia. The FLACC pain score was 4 at 4 hrs in Group A and at 12 hrs in Group B.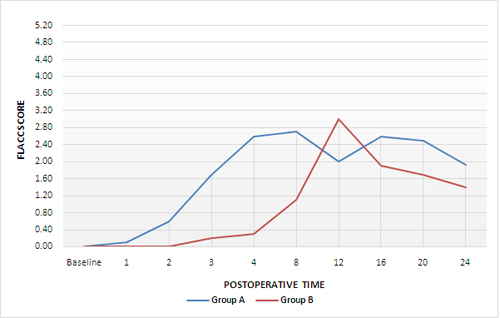
Figure 2: Comparison of changes in FLACC score in both groups (p<0.05 significant)
The total duration of postoperative analgesia in Group A was 270.67 ± 43.70 min, while in Group B, it was 506.67 ± 43.81 minutes. This difference between the two groups is highly significant and is shown in Figure 3.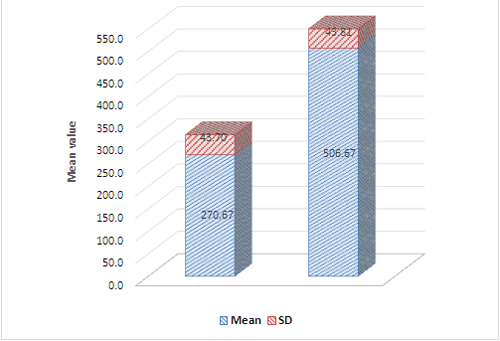
Figure 3: Comparison of duration of analgesia in min
[t-value-20.8884; P-value 0.00001], p<0.05 is significantIn Group A, 2(6.67%) children required one dose of rescue analgesia, 24 (46.7%) children required two doses and 4 (13.3%) required three doses of rescue analgesics. In Group B, 24 (80%) children required only single dose, 6 (20%) required two doses of rescue analgesics. The difference is statistically highly significant as depicted in Figure 4.
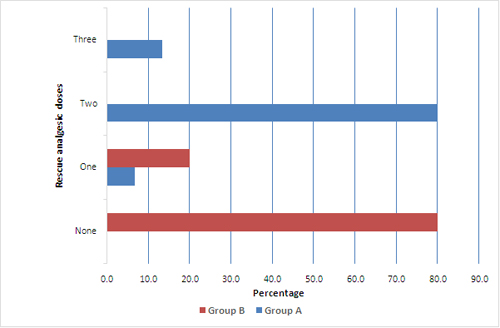
Figure 4: Comparison of percentage of patients needing rescue analgesic in two groups
Chi-square= 54.0003; p=0.00001*The incidence of bradycardia was seen in no child in Group A compared 1(3.33%) in Group B. Hypotension was observed in 1(3.3%) child in Group A while none in Group B. Nausea and vomiting was present in 1(3.33%) children in Group A compared to 2(6.67%) in Group B. These differences were statistically not significant. There was no incidence of other complications such as dural or vessel puncture, urinary retention and respiratory depression in any of the two groups. The incidence of complications is shown in Table 3.
Table 3: Comparison of complications in two groups
Complications |
Group A N (%) |
Group B N (%) |
| Bradycardia | 0.00 |
1 (3.33) |
| Hypotension | 1 (3.33) |
0.00 |
| Nausea and Vomiting | 1 (3.33) |
2 (6.67) |
| No complications | 28 (93.33) |
27 (90) |
| Total | 30 (100) |
30 (100) |
DISCUSSION
Caudal epidural analgesia is one of the most popular and commonly performed regional blocks in pediatric anesthesia. It is a reliable and safe technique that can be used with general anesthesia for intra- and postoperative analgesia in patients undergoing abdominal and lower-limb surgery.7The dose of clonidine for epidural administration is 1–5 µg/kg. We chose a dose of 1 µg/kg of clonidine in our study as there were studies showing that increasing the dose from 1 to 2 µg/kg did not enhance the analgesic efficacy of clonidine11 and the incidence of adverse effects like respiratory depression, bradycardia and hypotension increased with increasing dose.12
Several mechanisms have been suggested for the clonidine-induced prolongation of caudal analgesia with bupivacaine. The anti-nociceptive action is due to the direct suppression of the spinal cord nociceptive neurons by epidural clonidine. Another mechanism is that clonidine crosses the blood brain barrier and interacts with alpha-2 adrenoceptors at spinal and supraspinal sites to produce analgesia. Clonidine also suppresses neurotransmission in peripheral sensory Aδ and C nerve fibres. The final mechanism suggested is pharmacokinetically mediated: clonidine induces vasoconstriction through α-2b adrenoceptors located at the peripheral vascular smooth muscles.13 Clonidine has a α2/α1 selectivity ratio of 1:200 where as another α2 adrenergic agonist, dexmedetomidine has an α2/α1 selectivity ratio of 1:1600.
This effect correlates with the concentration of clonidine in the cerebrospinal fluid but not that in the plasma, and was first demonstrated clinically in 1984-92. The successful use of epidural clonidine in adults led to its evaluation in pediatric caudal epidural block. The resulting studies have consistently shown caudal clonidine to increase the duration of postoperative analgesia.7
Caudal clonidine does appear to have a dose-dependent sedative effect in children.Sedation after epidural clonidine results from activation of α2-adrenoceptors in the locus coeruleus, an important modulator of vigilance. This suppresses the spontaneous firing rate of the nucleus, thereby resulting in increased activity of inhibitory inter-neurones such as GABA-ergic(gamma amino butyric acid)pathways, to produce CNS depression.14
Our study did not correlate with the study by Penon and colleagues where in epidural clonidine was associated with arterial oxygen desaturation. It did not correlate with the studies by Breschan et al and Bouchut JC et al, in which there was oxygen desaturation during the first hour of surgery in 15 patients and risk of postoperative apnea in preterm neonate who had clonidine 1.25 µg/kg respectively. There was no significant difference in the values of arterial oxygen saturation between the two groups in our study.
In children, a mixture of 0.25% bupivacaine with l - 2 µg/kg clonidine has been seen to improve the duration and quality of analgesia provided by caudal block. Although results differ widely, the duration of analgesia provided range from 6.3 hours12 to 16.4 hours6 for 1 µg/kg. One study has shown a mean duration of analgesia of 20.9 ± 7.4 hours in children receiving caudal clonidine with bupivacaine, but a dose of 5 µg/kg of clonidine was used in this study.15
In our study, the duration of analgesia achieved by the addition of clonidine 1 µg/kg to bupivacaine plain 0.25% (1 ml/kg) shows a mean duration of analgesia of 506.67 ± 43.81 minutes. It is comparable to that of El Hennawy16 et al, Jamali17 et al, Cook B 18et al, Motsch J 15et al and Lee JJ19 et al.The slight differences may be the result of a number of factors such as dose of clonidine used as an adjuvant, differences in premedication and volatile anesthetics used; type of surgery; indications for rescue analgesia; assessment of pain and statistical analysis.
Our study is comparable to Parameshwari A13 et al, Jamali17 et al and Lee JJ19 et al as the number of rescue analgesics used is significantly lesser in the clonidine group as compared to the bupivacaine plain group.
The limitation of this study is that we did not assess the maximum maintenance halothane concentration required to achieve hemodynamic parameters like HR and MAP within 30% of baseline value, did not assess the mean time of arousal from anesthesia in both the groups and also did not monitor the end tidal carbon dioxide concentration between the groups.
CONCLUSION
The present study demonstrated that caudal administration of 0.25% bupivacaine (1 ml/kg) with clonidine (1 µg/kg) in children for sub-umbilical surgeries resulted in prolongation of the duration of analgesia and less number of rescue analgesics with better sedation compared with 0.25% bupivacaine (1 ml/kg) alone.
The study showed that there was no significant difference in the hemodynamic parameters or any increase in complications in children undergoing sub-umbilical surgeries.
Hence low dose clonidine (1 µg/kg) safely prolongs the duration of postoperative analgesia when it is added to bupivacaine 0.25% (1 ml/kg) for single shot caudal block in children for sub-umbilical surgeries.
REFERENCES
- International Association for Study of Pain, Subcommittee on Taxonomy. Pain terms: a list with definitions and notes on usage. Pain 1979;6:249-52. [PubMed][Free full text]
- Maunuksela EL,Olkkola KT. Pediatric Pain Management. IntAnaesthesiolClin 1991;29(1):37-55. [PubMed]
- Steward DJ, editor. Anatomy and Physiology relevant to Paedia tricanaesthesia. In:Manual of paediatricanaesthesia. 4th ed.New York : Churchill Livingstone;1995 pp 9-39.
- Markakis DA. Regional anaesthesia in paediatrics.AnesthesiolClin North America.2000;18(2):355-9,vii. [PubMed]
- Hansen TG, Henneberg SW, Larsen SW, Lund J, Hansen M.CaudalBupivacaine supplemented with caudal or intravenous Clonidine in children undergoinghypospadias repair: a double blind study. Br JAnaesth 2004;92(2):223-7.[PubMed][Free full text]doi:1093/bja/aeh028
- Sanders JC.Paediatric regional anaesthesia, a survey of practice in the United Kingdom.Br J Anaesth 2002;89:707-10.[PubMed][Free full text]doi:1093/bja/89.5.707
- De-Beer DAH, Thomas ML. Caudal additives in children – solutions or problems? Br J Anaesth 2003;90(4):487-98.[PubMed][Free full text]doi:1093/bja/aeg064
- Cook B, Doyle E. The use of additives to local anaesthetic solutions for caudal epidural blockade. PaediatrAnaesth 1996;6:353-9.[PubMed]
- Schecter NL. The under treatment of pain in children: An overview. PediatrClin Nor Am 1989;36(4):781-94.[PubMed]
- Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. PaediatrNurs 1997;23:293–7.[PubMed]
- Klimscha W, Chiari A, Michalek-Sauberer A, Wildling E, Lerche A, Lorber C, et al. The efficacy and safety of a clonidine/bupivacaine combination in caudal blockade for pediatric hernia repair. AnesthAnalg 1998;86(1):54-61.[PubMed]
- Breschan C, Krumpholz R, Likar R, Kraschl R, Schalk HV. Can a dose of 2 mcg/kg caudal clonidine cause respiratory depression in neonates? PaediatrAnaesth 1999;9:81-3.[PubMed]
- Parameshwari A, DhevAnand M, Vakamudi M. Efficacy of clonidine as an adjuvant to bupivacaine for caudal analgesia in children undergoing sub-umbilical surgery. Indian J Anaesth 2010;54:458-63.[PubMed][Free full text]doi: 10.4103/0019-5049.71047.
- Eyres RL, Chalkiadis G, Taylor R. Efficacy and safety of levobupivacaine as caudal anaesthesia in paediatric surgery. Inter Monitor RegAnaesth 1999;11:31A.
- Motsch J, BoÈttiger BW, Bach A, BoÈhrer H, Skoberne T, Martin E. Caudal clonidine and bupivacaine for combined epidural and general anaesthesia in children. ActaAnaesthesiolScand 1997;41(7):877-83.[PubMed][Free full text]DOI: 10.1111/j.1399-6576.1997.tb04803.x
- El-Hennawy AM, Abd-Elwahab AM, Abd-Elmaksoud Am, El-Ozairy HS, Boulis SR. Addition of clonidine or dexmedetomidine to bupivacaine prolongs caudal analgesia in children. Br J Anaesth 2009;103(2):268-274.[PubMed][Free full text]doi: 10.1093/bja/aep159. Epub2009 Jun 18.
- Jamali S, Monin S, Begon C, Dubousset A, Ecoffey C. Clonidine in paediatric caudal anaesthesia. AnaesthAnalg 1994;78(4):663-6.[PubMed]
- Cook B, Grubb DJ, Aldridge LA, Doyle E. Comparison of the effects of adrenaline, clonidine and ketamine on the duration of caudal analgesia produced by bupivacaine in children. Br J Anaesth 1995;75:698-701.[PubMed][Free full text]doi:1093/bja/75.6.698
- Lee JJ, Rubin AP. Comparison of a bupivacaine-clonidine mixture with plain bupivacaine for caudal analgesia in children. Br J Anaesth 1994;72(3):258-62.[PubMed][Free full text] doi: 10.1093/bja/72.3.258