Tomoki Nishiyama, MD, PhD
Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa-ku, Tokyo, 140-0001 (Japan)
Correspondence: Tomoki Nishiyama, MD, PhD: Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa-ku, Tokyo, 140-0001 (Japan); Tel: +81-3-5781-0700, Fax. +81-3-5781-0828; E-mail: nishit-tky@umin.ac.jp
ABSTRACT
Background: There are no standard wound catheters to provide constant diffusion to give effective infiltration of local anesthetics. We developed two new catheters and compared the diffusion from these two catheters as a preliminary study.
Methodology: The catheter-A was divided into four equal lumens inside. It has four holes of 0.1 mm in diameter, one hole in each lumen with an interval of 20 mm and 90 degrees angle starting at 10 mm from the tip of the catheter. The catheter-B is a single-lumen catheter that has a first hole of 0.3 mm in diameter at 10 mm from the tip and has another 9 holes of 0.1 mm in diameter with an interval of 10 mm and 180 degrees angle starting at 10 mm from the first hole. Both had 1 mm external diameter. Each catheter was put on the test tubes. A dye was infused at a rate of 2, 4, or 10 ml/h.
Results: The catheter-A had almost homogenous diffusion from all holes at all flow rates, but the catheter-B had uneven diffusion.
Conclusions: A four-lumen catheter might be better than a single lumen catheter to provide more homogenousdiffusion.
Key words: wound infiltration, catheter, postoperative analgesia
Citation: Nishiyama T. In vitro comparison of the diffusion from two new multi-hole wound catheters: A preliminary study. Anaesth Pain & Intensive Care 2015;19(1):19-23
INTRODUCTION
Continuous wound or peri-neural infusion of local anesthetic is increasingly used for post-operative pain management.1,2 However, its usefulness is still controversial.3,4 One of the reasons of the controversy might be that there is no good catheter to diffuse local anesthetic effectively. For continuous wound or peri-neural infusion of local anesthetic, an epidural catheter or a wound catheter is used.5,6 An epidural catheter has only one or a few holes at the tip of the catheter, therefore, it can be used only for a small wound. Now there are three commercially available multi-hole wound catheters.6, 7 However, no catheter was proven to be the best one to deliver the effective diffusion of local anesthetics. Only two studies investigated the diffusion of multi-hole wound catheters. Hansen et al.6 compared diffusion from their original catheter with that from two commercially available catheters. We have developed new wound catheters, and diffusion ability of one of them was compared with a commercially available catheter using animal muscles.8 However, in that study, the difference of dye diffusion could not be recognized clearly.The present preliminary study was performed to compare diffusion from two of our newly developed multi-hole wound catheters using a simple model with test tubes to let the difference visible at a glance.
METHODOLOGY
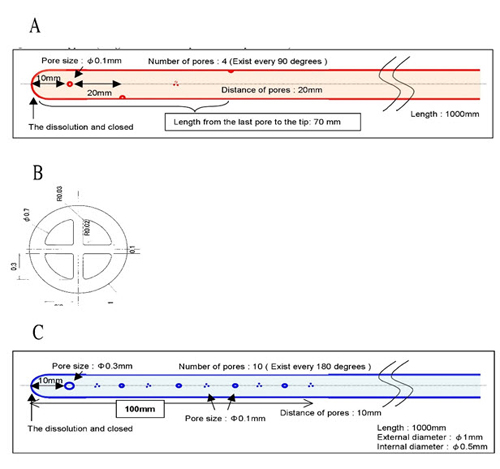
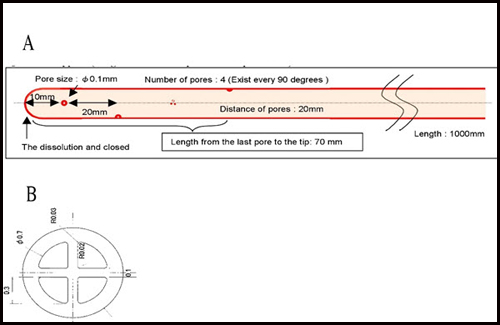
A new four-lumen multi-hole catheter (catheter-A) was made with 1 mm external diameter and the lumen was divided into four equal lumens. It has four holes of 0.1 mm in diameter, one hole in each lumen with an interval of 20 mm and 90 degrees angle starting at 10 mm from the tip of the catheter. The last hole was 70 mm from the tip of the catheter (Figure 1 A, B). Another new single-lumen multi-hole catheter (catheter-B) was made to have a 1 mm external diameter and 0.5 mm internal diameter. It has a first hole of 0.3 mm in diameter at 10 mm from the tip and has other 9 holes of 0.1 mm in diameter with an interval of 10 mm and 180 degrees angle starting at 10 mm from the first hole. The length with holes was 100 mm (Figure 1 C).
Figure 1: Catheter-A and catheter-B showing location of holes. The upper (A) is a four-lumen multi-hole catheter with its cross section (B). The lower (C) is a single-lumen multi-hole catheter.
Each catheter was put on the test tubes. A dye was infused at a rate of 2, 4, or 10 ml/h not to overflow the test tube (total flow of 30 ml for catheter-A and 10 ml for catheter-B). Diffusion of dye was optically compared between the two catheters.
RESULTS
The catheter-A had almost homogenous diffusion from all holes at all three infusion rates (Figure 2 A). The catheter-B had a diffusion only at the tip hole at 2 ml/h, a little diffusion was added from the proximal end hole at 4 ml/h, and the proximal end hole had more diffusion than the tip hole at 10 ml/h (Figure 2 B).
Figure 2 A & B: Diffusion from all holes in catheter-A & B at three infusion rates.
DISCUSSION
The present results showed that a four-lumen multi-hole catheter provided more homogenous diffusion of dye from every holes than a single-lumen multi-hole catheter at 2, 4, and 10 ml/h.
In our previous study,8 we investigated the diffusion at 1 and 4 ml/h according to the previous clinical practices.7,9,10 However, Fortier et al.2 used about 10 ml/h for paravertebral block. Therefore, in the present study, we investigated at 2, 4, and 10 ml/h. We used rabbit muscle to mimic clinical situation in the previous study8 to study the diffusion of dye, but the diffusion became obscure, therefore, to make it clearer, we used test tubes in the present study.
The Soaker catheterTM (I Flow, Lake Forest, CA, USA) is a single lumen multi-orifice catheter that is the most often used as a wound catheter. We used the Soaker catheter in our previous study,8 but our new four-lumen catheter was better than the Soaker catheter. However, it is quite complicated to make a four-lumen catheter, therefore, we made another single lumen catheter with different size of the holes from the Soaker catheter.
One of the determinants of peri-neural or wound catheter success is configuration of the catheter. There are few studies of catheter configuration. Anderson et al.11 found that wound spread of a bolus injection through a 15 cm multi-holes catheter was similar to a triple-orifice epidural catheter when placed subfascially following total hip arthroplasty. Fredrickson et al.12 investigated the effects of catheter orifice configuration and found that multi-orifice catheters provided better block than end-hole catheters in interscalene block. This finding is consistent with the studies of epidural catheters.13 Flow from multi-orifice catheter has been shown to depend on the flow rate; below 80 ml/h, multi-orifice catheter functions like single-orifice catheters.14 From these reports, multi-orifice catheter is better than single-orifice catheter for bolus injection but not for continuous infusion.
There is only one study to compare different size of the catheter. Campolo et al.15 reported that catheters with small size holes (34.9 – 70.04 µm) distributed the flow more homogenously than catheters with large size holes (282.56 – 360.24 µm). Our new catheters have smaller holes than the Soaker catheter except for the tip hole of our single lumen catheter.
Limitations: There are some limitations of this study. We used each one catheter and did not perform power analysis and statistical analysis. However, dye diffusion is quite clear in the test tube, therefore, each one catheter is enough to get conclusion as an observational preliminary study. The duration of infusion was limited and different between the two catheters not to overflow from the test tube. Further studies with longer infusion, ex. 24 hours are necessary to consider its clinical application. We studied only continuous infusion, Therefore, we need the study of single injection.
CONCLUSION
In conclusion, the present study suggested that a four-lumen catheter was better than a single-lumen catheter to provide homogenous distribution of continuously infused local anesthetics.
Acknowledgement: The author used no fund and has no conflict of interest.
A part of this study was presented at the American Society of Anesthesiologists Meeting in Washington DC in 2012.
REFERENCES
- Kristensen BS, Fenger-Eriksen C, Pedersen KV, Felsby S. Wound infusion of bupivacaine following radical retropubic prostatectomy: a randomized placebo-controlled clinical study. Eur J Anaesthesiol 2013;30:124-8. [PubMed]
- Fortier S, Hanna HA, Bernard A, Girard C. Comparison between systemic analgesia, continuous wound catheter analgesia and continuous thoracic paravertebral block: a randomized, controlled trial of postthoracotomy pain management. Eur J Anaesthesiol 2012;29:524-30. [PubMed]
- Chester JF, Ravindranath K, White BD, Shanahan D, Taylor RS, Lloyd-Williams K. Wound perfusion with bupivacaine: objective evidence for efficacy in post-operative pain relief. Ann R Coll Surg Engl 1989;71:394-6. [PubMed][Free full text]
- Gibbs P, Puroshotham A, Auld C, Cushieri RJ. Continuous wound perfusion with bupivacaine for postoperative wound pain. Br J Surg 1988;75:923-4. [PubMed]
- Gebhardt R, Mehran RJ, Soliz J, Cata JP, Smallwood AK, Feeley TW. Epidural versus ON-Q local anesthetic-infiltrating catheter for post-thoracotomy pain control. J Cardiothorac Vasc Anesth 2013;27:423-6. [PubMed]
- Hansen B, Lascelles BD, Thomson A, DePuy V. Variability of performance of wound infusion catheters. Vet Anaesth Analg 2013;40:308-15. [PubMed]
- Baulig W, Maurer K, Theusinger OM, Hinselmann V, Baulig B, Spahn DR, et al. Continuous elastomeric pump-based ropivacaine wound instillation after open abdominal aortic surgery: How reliable is the technique? Heart Surg Forum 2011;14:E51-8. [PubMed]
- Nishiyama T. Efficacy of a new four-lumen multi-oriface wound catheter. International Journal of Advance in Medical Science 2013;1:37-40. [Free full text]
- Boulind CE, Ewings P, Bulley SH, Reid JM, Jenkins JT, Blazeby JM, et al. Feasibility study of analgesia via epidural versus continuous wound infusion after laparoscopic colorectal resection. Br J Surg 2013;100:395-402. [PubMed]
- Polglase AL, McMurrick PJ, Simpson PJ, Wale RJ, Carne PW, Johnson W, et al. Continuous wound infusion of local anesthetic for the control of pain after elective abdominal colorectal surgery. Dis Colon Rectum 2007;50:2158-67. [PubMed]
- Andersen Lφ, Kristensen BB, Madsen JL, Otte KS, Husted H, Kehlet H. Wound spread of radiolabeled saline with multi- versus few-hole catheters. Reg Anesth Pain Med 2010;35:200-2. [PubMed]
- Fredrickson MJ, Ball CM, Dalgleish AJ. Catheter orifice configuration influences the effectiveness of continuous peripheral nerve blockade. Reg Anesth Pain Med 2011;36:470-5. [PubMed]
- Dickson MA, Moores C, McClure JH. Comparison of single, end-holed and multi-orifice extradural catheters when used for continuous infusion of local anesthetic during labour. Br J Anaesth 1997;79:297-300. [PubMed]
- Fegley AJ, Lerman J, Wissler R. Epidural multiorifice catheters function as single-orifice catheters: an in vitro study. Anesth Analg 2008;107:1079-81. [PubMed]
Campolo M, Molin D, Rawal N, Soldati A. Protocols to compare infusion distribution of wound catheters. Med Eng Phys 2011;34:326-32. [PubMed]