Aparna Girwalkar-Bagle*, Widhya Thatte**, Shital Choudhari***,
*Associate professor; **Professor & Head of Department; ***Resident
Department of Anesthesiology, Dr. D. Y. Patil Medical College, Pimpri, Pune, Maharashtra (India)
Correspondence: Dr. Aparna Girwalkar-Bagle, Flat No.103, Aster 1, Sukhawani Campus, Opposite Vallabhnagar Bus Stand, Pimpri, Pune, Maharashtra (India); Mobile: +91-9922504009; E-mail: draparnabagle@gmail.com
ABSTRACT
Background & Aim: Caudal block is the regional anesthetic technique that is used most frequently in pediatric surgery and bupivacaine and levobupivacaine are widely utilized in this technique. Opioid drugs have been added to local anesthetic solutions to prolong duration of analgesia but ideal combination were not found. We compared the postoperative analgesic efficacy of equal concentrations of bupivacaine or levobupivacaine plus tramadol in pediatric patients.
Objectives: Following objectives were monitored during study time of first analgesic requirement postoperatively, CHIPPS score for first 24 hrs, analgesic requirement in first 24 hrs, hemodynamic parameters and any side effects.
Methodology:Sixty children aged 2 to 5 years who were undergoing inguinal herniorrhaphy or orchidopexy received bupivacaine 0.25% plus tramadol 2 mg/kg (1 ml/kg) (BT group) or levobupivacaine 0.25% plus tramadol 2 mg/kg (1 ml/kg) (LT group) by the caudal route after general anaesthesia. The primary outcome of the study was to compare the duration and quality of postoperative analgesia. The postoperative pain relief was evaluated by the Children and Infants Postoperative Pain Scale (CHIPPS) at 2, 4, 6, 12, and 24 h postoperatively. In addition, the time of first analgesic requirement was noted.
Results: The CHIPPS scores were not statistically different between the groups. The duration of analgesia and requirements for rescue analgesia was similar. Urinary retention and motor blockade were observed more often in the BT group but statistically not significant. There were no significant differences between groups for arterial pressures and heart rate after caudal block and during the operation.
Conclusion: Caudal bupivacaine plus tramadol and levobupivacaine plus tramadol have similar postoperative analgesic efficacy.
Key Words: Bupivacaine; Levobupivacaine; Tramadol; Anesthesia; Caudal blockade
Citation:Girwalkar-Bagle A, Thatte W, Choudhari S. Preemptive caudal anaesthesia in children with bupivacaine-tramadol and levobupivacaine-tramadol: a randomized, double-blind, prospective study. Anaesth Pain & Intensive Care 2015;19(1):13-19
INTRODUCTION
A caudal block is a type of epidural block, but the space is entered at its most distal point via the sacral hiatus, situated on the posterior aspect of the sacrum at S4.1
Caudal block is useful adjunct to general anesthesia for lower abdominal surgery in children as it provides intraoperative analgesia, smooth recovery period and good postoperative pain relief which reduces perioperative analgesic requirement. Caudal blockade was used most frequently in pediatric surgery and bupivacaine and levobupivacaine are widely utilized in this technique.1,2 A large number of clinical studies have proven the clinical effectiveness and safety of bupivacaine and levobupivacaine.3-6 However, the single caudal block with local anesthetics provides only a short duration of analgesia and therefore the use of different additives has been advocated in order to prolong the period of postoperative analgesia. Opioid or nonopioid drugs as tramadol have been added to local anesthetic solutions to prolong caudal analgesia by a single injection.7-12 Tramadol, a synthetic 4-phenyl-piperidine analogue of codeine. Tramadol acts by inhibiting serotonin uptake resulting in analgesia almost equivalent to that of pethidine in potency while lacking the depressant effect on respiratory system. Tramadol has a selective spinal action.13 Tramadol has been shown to provide effective and long lasting analgesia after epidural administration in adults and children.11 So the purpose of this study was to compare the duration of postoperative analgesia using caudally administered bupivacaine tramadol and levobupivacaine tramadol combination in children undergoing inguinal herniorraphy and orchidopexy surgeries.
METHODOLOGY
This prospective randomized double blind study was conducted at Dr. D. Y. Patil Medical College, Pimpri, Pune from January 2014 to October 2014 after college ethical committee clearance. Informed written consent of parents was obtained.
A total of 60 ASA status I children aged 2 to 5 years who were scheduled for elective inguinal herniorrhaphy or orchidopexy were enrolled. Children in whom caudal block was contraindicated (infection at the site of block, bleeding diathesis, pre-existing neurological or spinal disease, or abnormalities of the sacrum) or with a known allergy to local anesthetics were excluded.
Patients were randomly assigned to bupivacaine-tramadol group (Group BT) and levobupivacaine-tramadol group (Group LT). Patients were fasted for 6 hrs before the procedure. Clear fluids were allowed up to 3 hrs before the procedure. Peripheral IV access was secured. Patients received premedication with inj. ondansetron 0.1 mg/kg inj. glycopyrrolate 0.004 mg/kg, inj. midazolam 0.02 mg/kg and inj. fentanyl 1µg/kg IV. Induction with inj. propofol 2 mg/kg and inj. suxamethonium 2 mg/kg was done. Anesthesia was maintained with nitrous oxide, oxygen and 1-1.5% sevoflurane after endotracheal intubation. The patients were placed in a left lateral position and caudal blockade was performed under sterile conditions using a 22G hypodermic needle. Verification of successful needle placement was based on four predictors: ability to locate sacral hiatus, pop on piercing the ligament, lack of resistance to injection, and lack of subcutaneous swelling. The children in Group BT received a caudal injection of bupivacaine 0.25% plus tramadol 2 mg/kg , while those in the Group LT received a caudal injection of levobupivacaine 0.25% plus tramadol 2 mg/kg resulting in a total volume of 1 ml/kg. Study drugs were prepared by an anesthetist not involved in the trial using unlabeled syringes. The study remained blind until completion and researchers were only made aware of group allocations after statistical analysis.
Heart rate, noninvasive blood pressure and peripheral oxygen saturation were recorded before anesthesia and at 5 min intervals after caudal block. Skin incision was performed 15-20 min after caudal anesthesia. Effective analgesia was defined as hemodynamic change < 20% as compared to baseline values in response to surgical incision. In case of inadequate perioperative analgesia, supplementary fentanyl 1 µg/kg was administered (these patients were excluded from study). After surgery, patients were transferred to the recovery room.
The postoperative pain relief was evaluated using Children's and Infant's Postoperative Pain Scale (CHIPPS) (Table 1) at 2, 4, 6, 12, and 24 hr and by measuring the duration of analgesia. Postoperative assessments were made by nursing staff unaware of group allocation. Residual motor block was evaluated using a modified Bromage Scale (no motor block- score 0; able to move knees and feet- score 1; able to move feet- score 2; complete motor block of limb- score 3) 2 and 4 houers after surgery. In the case of a CHIPPS score of 4 or more, paracetamol 30 mg/kg was administered rectally. The duration of analgesia was defined by noting the time from caudal injection to the time of first analgesic requirement. Side effects (emesis, urinary retention, motor weakness, and sedation), time to first analgesic and the total number of analgesic doses required in the first 24 hr were recorded. Sedation score was assessed based on eye opening (spontaneous eye opening-0; eye opening to verbal stimuli-1; eye opening to physical stimuli-2 and unresponsive-3) at 2 and 4 hours. All patients were observed in the hospital for at least 24 hr for possible side effects of caudal block.
Table 1: Children and infants postoperative pain scale14
| Item |
Structure |
Points |
| Crying |
None |
0 |
| Facial expression |
Relaxed/smiling |
0 |
| Posture of the trunk |
Neutral |
0 |
| Posture of the legs |
Neutral |
0 |
Statistical analysis
Statistical analysis were performed using a statistical software (SPSS) version 2013. All results were expressed as mean ± SD (standard deviation). Unpaired t test was used to compare demographic variables, duration of analgesia, duration of surgery and intraoperative hemodynamic variables. The p-values were generated using chi square test for comparison of proportions. A p-value of less than 0.05 was considered statistically significant.
RESULTS
A total of 60 children were enrolled in the study and randomized in two groups of 30 each. Caudal block was successful in almost all of group and no patient required additional analgesic intraoperative.
Table 2: Demographic data, type of surgery and duration of surgery
|
Parameters |
Group BT |
Group LT |
P value |
| Age (years) |
3.93 ± 0.86 |
3.9 ± 0.88 |
0.89 |
| Weight (kg) |
15.53 ± 5.3 |
14.11 ± 5.07 |
0.56 |
| Gender(Male/Female) |
30 / 0 |
30 / 0 |
|
| Type of surgery (Orchidopexy / Inguinal herniorrhaphy) |
10 / 20 |
13 / 17 |
0.42 |
| Duration of operation ( min ) |
52 ± 13.9 |
58.9 ± 25.4 |
0.87 |
Both groups were comparable in respect to age, weight, sex, type and duration of surgery.
Figure 1: Comparison of pulse rate between two groups
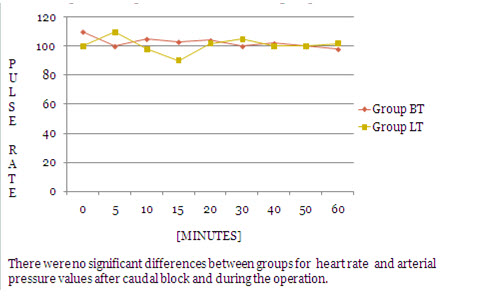
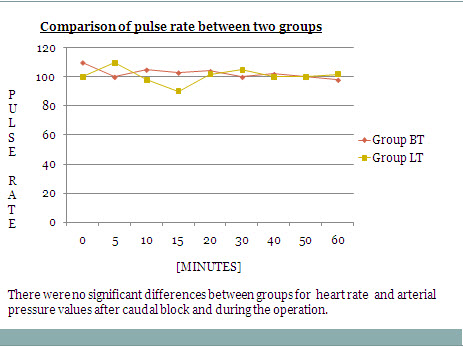
Figure 2: Comparison of mean blood pressure between two groups
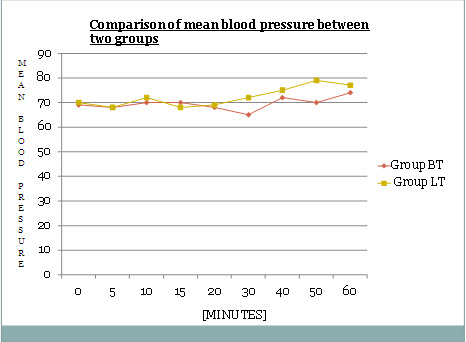
Intraoperative pulse rate and mean blood pressure were comparable in both the groups and changes in both were not clinically significant clinically as well statistically.
Table 3: CHIPPS scores for the first 24 postoperative hours
| Time Intervals |
Group BT (n=30) |
Group LT (n=30) |
P value |
| 2 h |
0.23 ± 0.34 |
0.13± 0.34 |
1.000 |
| 4 h |
0.20 ± 0.40 |
0.23 ± 0.50 |
0.786 |
| 6 h |
2.2 ± 0.92 |
0.93 ± 1.22 |
9.21 |
| 12 h |
3.3 ± 1.46 |
4.00 ± 2.06 |
0.200 |
| 24 h |
2.86± 1.43 |
2.63± 1.35 |
0.529 |
No statistically significant difference in CHIPPS pain scoring between groups could be detected at any measurement time (Table 3).
Table 4: The first analgesic requirement times
|
Group BT (n=30) |
Group LT (n=30) |
P value | |
| Time to first analgesic (hours) |
21.41 ± 6.62 |
17.79 ± 6.76 |
0.0625 |
Postoperative pain relief, which was the primary end-point of the study, was similar between the two groups. The first analgesic requirement time was 21.41 ± 6.62 hours for Group BT while it was 17.79 ± 6.76 hours for Group LT. This difference was not significant statistically
Table 5: Analgesic Requirement in first 24 hours
|
Number of doses of paracetamol received in 24 hrs |
Group BT (n=30) |
Group LT (n=30) |
P-value |
| 0 |
18 (70%) |
14 (46.66%) |
0.438 |
| 1 |
9 (20%) |
11 (36%) |
0.784 |
| 2 |
3 (10%) |
5 (16%) |
0.704 |
| Average no of doses per patient in 24 hrs |
0.5 ± 0.68 |
0.7 ± 0.74 |
0.160 |
18 patients in Group BT and 14 patients in Group LT did not required any analgesic in first 24 hours. While 9 and 11 patients required single dose of paracetamol in 24 hours in Group BT and Group LT respectively.
Table 6: Side effects [n(%)]
|
Side Effect |
BT Group |
LT Group |
P Value |
| Nausea, Vomiting |
1 (3.3) |
0 (0) |
1.00 |
| Sedation score at 2 hoursScore 0Score 1 |
13 (43.33) 17 (56.66) |
14 (46.66) 16 (53.33) |
1.00 |
| Urinary retention |
3 (10) |
0 (0) |
0.23 |
| Residual motor blockade (Bromage scale ) at 2 hrsScore 0 Score 1 Score 2Score 3 |
25 (83.33) 04 (13.33)01 (3.33) - |
28 (93.33) 02 (6.66)0 (0) - |
0.63 |
Sedation score was comparable in both the groups. Almost 50% of patients in both of the groups were sleeping comfortably and arousable with verbal commands.
Side effects such as urinary retention were observed 3(10%) patients in Group BT and in no patients in Group LT (p=0.05). In these patients, external manual compression over the bladder was able to express urine; no patient required bladder catheterization. Residual motor blockade of score 1 was found in 4 patients in Group BT and 2 patients in Group LT. while no motor blockade observed postoperatively after 2 hr.
Other side effects like nausea, vomiting occurred in one patient in Group BT. Pruritus was not observed in any of the patients.
DISCUSSION
Caudally administered single dose of local anesthetic during perioperative period has been reported to provide an adequate level of analgesia. Many studies has been reported that the effect of analgesic might vary depending upon the type of surgery , patients age, type and amount of local anesthetic agent.11 Frawley,3 Locatelli B4 ,Ingelmo5and Brechan6 and et al studied 0.25% of bupivacaine, levobupivacaine and ropivacaine and concluded that bupivacaine and levobupivacaine were equally potent and had longer analgesic effect. So we had choosen 0.25% bupivacaine and levobupivacaine for study. Ivani and Yao described dose response relationship for levobupivacaine in caudal block and stated that concentration of 0.2% is optimum for caudal.15,16
Tramadol injected into the epidural space has a prolonged duration of action because of sustained release from epidural fat and other relatively poorly perfused tissues.10 Gunes Y10 found epidural tramadol to provide good analgesia postoperatively and observed very low concentration of tramadol in systemic circulation compared to intravenous administration. Senel et al suggested that the duration of analgesia was longest in children receiving concurrent tramadol 1.5 mg/kg and bupivacaine 0.25%.11 Prakash et al compared three doses of tramadol, administered caudally with bupivacaine.17 In that study, tramadol 2 mg/kg combined with bupivacaine 0.25% provided a longer duration of postoperative analgesia and reduced the requirement for rescue analgesics as compared with tramadol 1 mg/kg or 1.5 mg/kg in children.
Yasser Majid et al and many other authors showed that addition of tramadol to bupivacaine or levobupivacaine for caudal analgesic technique provided longer lasting analgesia and lesser need for resecue analgesic in the postoperative period than when bupivacaine was used as a sole agent.20-23
It has been suggested that there could be a synergistic effect between the local anesthetics and the additives, such as tramadol, rather than simply an additive effect, as the higher the dose of local anesthetics, the greater the additional anesthetic effect. A synergistic interaction between intrathecal clonidine and lidocaine has also studied in rats.8,24,25
In our study we found that caudal block with bupivacaine 0.25% with tramadol 2 mg/kg or levobupivacaine 0.25% with tramadol 2 mg/kg yields 21.41 hrs and 17.79 hrs of analgesia respectively.In our study, the concentration of levobupivacaine was determined as 0.25% equal doses of bupivacaine. This higher concentration may have prolonged analgesia more when compared with many of above study.
One limitation of this study is that we used local anesthetic concentrations of 0.25%. Comparison of local anesthetic potency has been standardized by the use of the minimum local anesthetic concentration (MLAC or ED50).3 To our knowledge, the MLAC of local anesthetics has not been assessed in pediatric patients receiving caudal block.4 Yao et al described a dose-response relationship for levobupivacaine with caudal analgesia, and 0.15% levobupivacaine appeared to represent the optimum clinical dose for caudal block.16 However, the researchers did not evaluate levobupivacaine concentrations of more than 0.18%. In another study, Ivani et al15 found that 0.20% levobupivacaine may give the best caudal block in children. The local anesthetic concentrations used ranged from 0.2-0.25%, and the higher level may have reached the upper flat portion of the dose-response curve where both local anesthetics are effective and potency differences are obscured.4Nasreen Laiq in her study showed only 30% of patients required rescue analgesia in 24 hrs which was comparable with our study.23 In our study 30% in Group BT and 52% in Group LT required rescue analgesia in 24 hrs postoperatively.
The residual motor blockade must increase with increasing concentrations of local anesthetics,15 but recent studies have reported contrasting results. Astuto et al26 did not observe motor blockade after surgery and during the study period using ropivacaine 0.25% or levobupivacaine 0.25%. In contrast to these results, Frawley et al3 found 7% motor block in a group receiving 0.25% bupivacaine as compared with an 11% motor blockade in the levobupivacaine 0.25% group at 120 min following caudal anesthesia and no residual motor blockade after that. Locatelli et al4 and Ivani et al demonstrated that bupivacaine 0.25% produced a significant incidence of residual motor block at 2 hrs in recovery from anesthesia as compared with levobupivacaine 0.25%. This difference was lost in the following hours. Breschan et al6 compared the effects of 1ml/kg of 0.2% bupivacaine, levobupivacaine and ropivacaine and found that levobupivacaine and ropivacaine have significant lower motor blockade than bupivacaine in first 2 hrs and no difference after that. In our study we found motor blockade in 5(16%) and 2(6%) patients in Group BT and Group LT respectively at the end of 2 hours and no blockade after that. This difference was not statistically significant.
Postoperative dysuria affected 2% of children after caudal block for inguinal hernia procedures.8 In our study, three patients in the BT group (bupivacaine plus tramadol) had urinary retention, but none of these patients required bladder catheterization. In Engelman and Marsala's meta-analysis study,8 seven of the nine tramadol studies reported urinary difficulties. Pappas et al suggested that a distinct correlation between urinary retention and surgery type exists, with patients undergoing hypospadias repair having the highest incidence of urinary retention that requires therapeutic intervention.30
Effectiveness of caudal analgesia was evaluated intraoperative by mean blood pressure and heart rate. Many studies related to this topic showed that effects of caudal block with local anesthetic or local anesthetic with tramadol on mean blood pressure and heart rate were similar and no difference was found.
CONCLUSION
The addition of tramadol to both levobupivacaine and bupivacaine in caudal block in children prolongs postoperative analgesia without any added side effect.
REFERENCES
- Bernard JD. Regional anaesthesia in children. In: Miller RD , editor. Miller's anesthesia. Philadelphia: Churchill livingstone; 2009. p2532.
- Silvani P, Camporesi A, Agostino MR, Salvo I. Caudal anesthesia in pediatrics: an update. Minerva Anesthesiol. 2006;72: 453–9. [PubMed]
- Frawley GP, Downie S, Huang GH. Levobupivacaine caudal anesthesia in children: a randomized double-blind comparison with bupivacaine. Paediatr Anaesth. 2006;16:754–60. [PubMed]
- Locatelli B, Ingelmo P, Sonzogni V, Zanella A, Gatti V, Spotti A, et all. Randomized, double-blind, phase III, controlled trial comparing levobupivacaine 0.25%, ropivacaine 0.25% and bupivacaine 0.25% by the caudal route in children. Br J Anaesth. 2005;94:366–71. [PubMed]
- Ingelmo PM, Locatelli BG, Sonzogni V, Gattoni C, Cadisco A, Lorini M, et all. Caudal 0.2% ropivacaine less effective during surgery than 0.2% levobupivacaine and 0.2% bupivacaine: a double-blind, randomized, controlled trial. Pediatr Anesth. 2006;16:955–61. [PubMed]
- Breschan C, Jost R, Krumpholz R, Schaumberger F, Stettner H, Marhofer P, et all. A prospective study comparing the analgesic efficacy of levobupivacaine, ropivacaine and bupivacaine in pediatric patients undergoing caudal blockade. Paediatr Anaesth. 2005;15:301–6. [PubMed]
- Kumar P, Rudra A, Pan AK, Acharya A. Caudal additives in pediatrics: A comparison among Midazolam, ketamine and neostigmine co administered with bupivacaine. Anesth Analg 2005;101:69-73. [PubMed]
- Engelman E, Marsala C. Bayesian enhanced meta-analysis of post-operative analgesic efficacy of additives for caudal analgesia in children. Acta Anaesthesiol Scand. 2012;56:817–32 [PubMed]
- Demiraran Y, Kocaman B, Akman Y. A comparison of the postoperative analgesic efficacy of single-dose epidural tramadol versus morphine in children. Br J Anaesth. 2005;95:510–3. [PubMed]
- Gunes Y, Gunduz M, Unlugenc H, Ozalevli M, Ozcengiz D. Comparison of caudal vs intravenous tramadol administered either preoperatively or postoperatively for pain relief in boys. Paediatr Anaesth. 2004;14:324–8. [PubMed]
- Senel AC, Akyol A, Dohman D, Solak M. Caudal bupivacaine-tramadol combination for postoperative analgesia in pediatric herniorrhaphy. Acta Anaesthesiol Scand. 2001;45:786–9. [PubMed]
- Yildiz T, Ozdamar D, Bagus F, Solak M, Toker K. Levobupivacaine-tramadol combination for caudal block in children: a randomized, double-blinded, prospective study. Paediatr Anaesth. 2010;20:524–9. [PubMed]
- Budd K, Langford R. Tramadol revisited. Br J Anaesth. 1999;82:493–5. [PubMed]
- Büttner W, Finke W. Analysis of behavioral and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children: a comprehensive report on seven consecutive studies. Paediatr Anaesth. 2000;10:303–18. [PubMed]
- Ivani G, De Negri P, Lonnqvist PA, Eksborg S, Mossetti V, Grossetti R, et all. A comparison of three different concentrations of levobupivacaine for caudal block in children. Anesth Analg. 2003;97:368–71. [PubMed]
- Yao YS, Qian B, Chen BZ, Wang R, Tan L. The optimum concentration of levobupivacaine for intra-operative caudal analgesia in children undergoing inguinal hernia repair at equal volumes of injectate. Anaesthesia. 2009;64:23–6. [PubMed]
- Prakash S, Tyagi R, Gogia AR, Singh R, Prakash S. Efficacy of three doses of tramadol with bupivacaine for caudal analgesia in paediatric inguinal herniotomy. Br J Anaesth. 2006;97:385–8. [PubMed]
- Prosser DP, Davis A, Booker PD, Murray A. Caudal tramadol for postoperative analgesia in paediatric hypospadias surgery. Br J Anaesth. 1997;79:293–6. [PubMed]
- Büttner W, Finke W. Analysis of behavioral and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children: a comprehensive report on seven consecutive studies. Pediatr Anaesth. 2000;10:303–18. [PubMed]
- Majid Y, Mohammad K. A comparison of caudally administered single dose bupivacaine and bupivacaine- tramadol combination for postoperative analgesia in children. JK Science 2004;6(1):19-22. [Free full text]
- Sezen G, Demiraran Y, Karagoz I, Kucuk A. The assessment of bupivacaine-tramadol and levobupivacaine-tramadol combinations for preemptive caudal anaesthesia in children: a randomized double blind, prospective study. Int J Clin Exp Med 2014;7(5):1391-6. [PubMed][Free full text]
- Samad R, Shah TH. Comparison of caudal tramadol-bupivacaine and ketamine-bupivacaine for postoperative analgesia in children. Journal of surgery Pakistan 2013;18(2):54-8. [Free full text]
- Laiq N, Khan MN, Tahmeedullah, Gandapur YK, Khan S. Comparison of caudal bupivacaine and bupivacaine tramadol for postoperative analgesia in children undergoing hypospadias surgery. Journal of college of physician and surgeon of Pakistan 2009; 19(11):678-81. [Free full text]
- Kawamata T, Omote K, Kawamata M, Iwasaki H, Namiki A. Antinociceptive interaction of intrathecal α2-adrenergic agonists, tizanidine and clonidine, with lidocaine in rats. Anesthesiology 1997;87:436–48. [PubMed][Free full text]
- Hao S, Takahata O, Iwasaki H. Antinociceptive interaction between spinal clonidine and lidocaine in the rat formalin test: an isobolographic analysis. Anesth Analg. 2001; 92:733–8. [PubMed]
- Astuto M, Disma N, Arena C. Levobupivacaine 0.25% compared with ropivacaine 0.25% by the caudal route in children. Eur J Anaesthesiol. 2003;20:826–30. [PubMed]
- Ivani G, DeNegri P, Conio A, Grosseti R, Vitale P, Vercellino C. Comparison of racemic bupivacaine, ropivacaine and levobupivacaine for pediatric caudal anaesthesia; effects on postoperative analgesia and motor block. Reg Anesth pain Med 2002;27:157-61.[PubMed]
- De Negri P, Ivani G, Tirri T, Modano P, Reato C, Eksborg S, et all. A comparision of epidural Bupivacaine, levobupivacaine and ropivacaine on postoperative analgesia and motor blockade. Anesth Analg 2004;99:45-8. [PubMed]
- Kaya Z, Suren M, Arici S, Karman S, Tapar H, Erdemir F. Prospective randomized, double blind comparison of the effects of caudally administered levobupivacaine 0.25% and bupivacaine 0.25% on pain and motor block in children undergoing circumcision surgery. Eur Rev Med Pharmacol Sci 2012;16(1):2014-20. [PubMed] [Free full text]
Pappas AL, Sukhani R, Hatch D. Caudal anesthesia and urinary retention in ambulatory surgery. Anesth Analg 1997;85:706. [PubMed][Free full text]