Uday Gollamudi 1 , Pravallika Rallapalli 2
Authors affiliations:
Bispectral Index (BIS) monitoring has gained popularity during the recent past, in selected cases. It uses a processed Electroencephalograph (EEG) to provide a value between 0 and 100, indicating brain activity and anesthetic depth. Monitoring the depth of anesthesia is a critical aspect of ensuring patient safety during medical procedures. The bispectral index (BIS) monitor is pivotal in this process. Maintaining BIS values within the range of 40 to 60 is essential to prevent anesthesia awareness and mitigate potential long-term psychological consequences.
Keywords: Anesthesia; Bispectral Index monitoring; Brain activity; Electroencephalograph
Citation: Gollamudi U, Rallapalli P. Importance of BIS monitoring in sedation procedures and to attain optimum depth of anesthesia: a case series. Anaesth. pain intensive care 2026;30(2):362-66. DOI: 10.35975/apic.v30i2.3135
Received: October 15, 2025; Revised: November 12, 2025; Accepted: November 16, 2025
BIS monitoring involves the application of 4 electrodes on the forehead. The skin on the forehead is first cleaned with an alcohol swab, and then 2 to 5 seconds of digital pressure is applied over the sensor leads.1 The sensor is comprised of disposable wet gel electrodes. EMG activity of the frontalis muscle is measured by lead 4, which is the ground electrode as well. The information is displayed on the BIS view monitor providing insights into their anesthesia depth. Monitoring the depth of anesthesia is very important during any procedure. Anesthesia that's too deep can cause hemodynamic changes, and anesthesia that is too light carries the risk of recall or awareness during anesthesia..2 Awareness during anesthesia is a very serious complication with potential long-term psychological sequelae such as anxiety and posttraumatic stress disorder..3 When the bispectral index (BIS) value is maintained below 60, it decreases the incidence of anesthesia awareness..3 The BIS monitor is the first FDA-approved method to assess the hypnotic effects of drugs..4 Precisely assessing the depth of anesthesia remains a persistent challenge for clinical anesthesiologists. BIS represents a significant development in the objective assessment of the depth of anesthesia, providing valuable real-time feedback to anesthesia providers..5 Conventional monitoring of anesthetic depth is primarily assessed by the patient's clinical signs and symptoms, such as changes in heart rate, blood pressure, and limb movements..6, 7Lacking objective data support, these methods also face challenges in continuous monitoring due to low specificity and sensitivity..6Such limitations may lead to inaccurate and untimely assessments, potentially resulting in either excessive or insufficient anesthesia, which significantly impacts patients' mental health, disease recovery, and long-term survival rates..6
The Bispectral Index (BIS) offers an objective and precise method for monitoring the depth of anesthesia,.8 which is a crucial component of some Enhanced Recovery After Surgery (ERAS) guidelines..9,10 ERAS is an evidence-based approach to surgical care aimed at improving the quality of perioperative care and supporting quick recovery..10,11

Figure 1: Patient’s head showing placement of electrodes
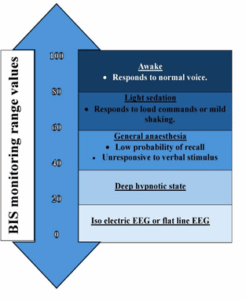
Figure-2: BIS monitoring range values
CASE 1:
A 35 year old female patient was diagnosed with bipolar disorder along with psychosis. No improvement was noticed after taking oral treatment medications for 10 days, hence the patient was posted for electroconvulsive therapy (ECT) therapy under anesthesia. ECT was planned for the patient, and written informed consent was obtained from the patient's husband. Pre-anesthetic checkup was done for the patient. The patient was kept nil by mouth for 8 hrs. The objective of ECT is to induce seizure with the minimum required electric intensity, fitting the condition of each patient, to treat specific psychiatric disorders.
The first few cycles of ECT were given without BIS monitoring and at the time of procedure the seizure duration attained was not adequate. The depth of anesthesia has been shown to impact seizure characteristics and level of stimulation energy. Deep anesthesia may reduce the antidepressant effect of ECT.12 and increase the risk of cognitive side effects..13 Light anesthesia might result in awareness .14 but leads to improved seizures quality. .15 Since then monitoring of BIS value has been adopted. The patient was monitored with the help of pulse oximetry, non-invasive blood pressure, five-lead ECG monitor and BIS monitor during the procedure. Baseline vitals were within normal limits and BIS monitor showed value of 95. Injection glycopyrrolate 0.2 mg intravenous (IV) and injection ondansetron 4 mg IV were given. The patient was pre-oxygenated with 100% oxygen for 3 min using Bain's circuit. The patient was induced with 60 mg propofol IV, remifentanil 100 mcg IV and muscle relaxation by 50 mg of succinylcholine IV. The patient was ventilated manually with 100% oxygen using a tight-fitting facemask and Bain's circuit. After 60 sec of succinylcholine administration, the BIS monitor showed a valve of 50 and then a mouth gag was inserted to prevent the tongue bite. Electric stimulation was provided and seizure duration was 30-70 sec. After ECT was given, bag-mask ventilation was resumed until the patient had adequate spontaneous respirations and till BIS value was above 90. During the procedure, the patient had transient hypertension (140-160/90-100 mmHg), and tachycardia (120–130) and the BIS value was around 80, recovery was uneventful. The patient had undergone another six sessions of ECT in next 2 weeks. After six sessions, psychiatric symptoms were markedly improved. Two weeks later, the patient was discharged with oral olanzapine 7.5 mg once-a-day.
BIS monitoring during ECT is important because it helps to standardize anesthetic depth, potentially optimizing seizure quality, duration and also facilitating faster recovery. Titration of anesthetic drugs may be especially useful in ECT to optimize electrical and clinical responses and reduce side effects.
CASE 2:
A 28 years old women with history of 2 previous normal deliveries and laparoscopic appendectomy was posted for laparoscopic tubectomy but the patient had history of awareness during the surgery when she was undergoing lap appendectomy. This would have happened because the patient would have been in lighter plane of anesthesia during the surgical procedure and due to this she has developed post-traumatic stress. Now we have counselled the patient and gave assurance to her. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2 mg/kg iv, remifentanil 100 µg iv, succinylcholine 100 mg iv, Patient was preoxygenated with 100 % oxygen along with 3 % sevoflurane for 3 mins using Bain's circuit and then BUSKA LMA was placed when the patient BIS value was around 30 after which patient was connected to ventilator and maintenance of anesthesia was done with propofol and ketamine iv intermittently along with sevoflurane as inhalational agent. The BIS was maintained throughout the procedure between 40-50 and once the procedure was completed inhalational agent was cutoff and we stopped maintenance dosage, after 15 mins the BIS value came upto 80 and then we removed the LMA and bag mask ventilation was continued till the BIS reading came to 90. Patient was then shifted to recovery and was comfortable. When asked about the awareness during the procedure she replied that she was comfortable and didn’t have any awareness. Hence BIS monitoring is an important tool for providing optimum anesthesia experience to the patient.
CASE 3:
A 25 years old women had lump in the breast for which fibroadenoma surgery was planned. Previously she had undergone laparoscopic cholecystectomy in outside hospital under general anesthesia, during which she had history of delayed recovery post procedure and was kept on ventilator in postoperative care unit. Now we have counselled the patient and gave assurance to her. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2 mg/kg iv, remifentanil 100 µg iv, atracurium 0.5 mg/kg iv then the patient was preoxygenated with 100% oxygen along with 3 % sevoflurane for 3 min using Bain's circuit. We avoided succinylcholine because of history of delayed recovery. When BIS value reading was around 40 the patient was intubated with 7 size ETT with the help of direct laryngoscopy. Patient was connected to ventilator with a mixture of oxygen and air along with sevoflurane for maintenance of anesthesia. Maintenance dose of atracurium was given only when the BIS reading was in the low 60’s. Post procedure reversal was given and the patient was extubated. Recovery from anesthesia was uneventful.
CASE 4:
A 45 years old male with cancer tongue and buccal mucosa with METS extending to the neck was posted for hemiglossectomy, hemimandibulectomy with fibular graft along with neck dissection and chest graft. Surgeons want deep postoperative sedation for at least 1 day. Patient had Mallampati grade 4. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2mg/kg iv, remifentanil 100 µg iv, succinylcholine 100 mg iv, Patient was preoxygenated with 100% oxygen along with 3 % sevoflurane for 3 mins using Bain's circuit. Nasal intubation was done with north nasal tube of size 7.5. Tube fixed after bilateral air entry checked and was equal. Foleys catheter was placed. Maintenance of anesthesia throughout the procedure was done with the help of atracurium infusion along with sevoflurane as inhalation agent. BIS reading was maintained between 40-50 throughout the procedure. But as the graft was placed the surgeons wanted patient to be kept in deep sedation post operatively for 24 hrs. Atracurium infusion was continued post operatively, iv fentanyl was started at the rate of 4 µg/kg and doses were titrated depending on BIS score. Monitoring was continued postoperatively. Patent connected to ventilator on ACVC mode. BIS monitoring was continued for 24 hrs postoperatively with values between 50-60. After 24 hrs infusions were stopped and patient extubated after giving reversal. Recovery was uneventful.
CASE 5:
A 30 year old male was admitted with features of raised intracranial pressure. MRI brain revealed third ventricle mass about 2 cms with epicentre in the pineal gland with mass effect and hydrocephalus. She was planned for an endoscopic third ventriculostomy and biopsy. After placing standard monitors induction and intubation were done with standard anesthesia drugs without giving any muscle relaxant. Total intravenous anesthesia with propofol was maintained with titrated doses so that BIS value was between 40-50. Neuroendoscope was introduced through right frontal burr hole and irrigated with ringer lactate solution. Within 15 seconds of insertion of neuroendoscope, the BIS value dropped from 40 to 5, mean arterial pressure increased from 90 to 130 mmHg, heartrate raised from 70 to 150/ min. Changes were notified to the surgeon, neuroendoscope was removed and lateral ventricle decompressed with a ventriculoperitoneal (VP) shunt needle. BIS improved from 5 to 35 within a minute and reached baseline within 2 minutes. After this neuroendoscope was reintroduced, ventriculostomy and biopsy was done. After the completion of the procedure the patent woke up without any delay and post extubation GCS was 15. Post procedure the CT of the brain revealed mild pneumoventricle with reduction in hydrocephalus.
CASE 6:
A 48 years old female with encephalitis, adrenal insufficiency, left lung collapse and in septic shock is intubated and connected to mechanical ventilator for the past 10 days and is posted for tracheostomy. Standard monitors were connected along with BIS monitor. Routine premedication was given and patients endotracheal tube connected to bain circuit and patient was manually ventilated with intermittent dose of etomidate and remifentanil based on BIS value at the time of procedure. Just before insertion of tracheostomy tube the endotracheal tube was pulled out, now Bain circuit was connected to tracheostomy tube and once the tube was confirmed is in place the subsequent doses of anesthetic drugs were stopped and patient was shifted to MICU and connected to mechanical ventilator for further management.
CASE 7:
A 22 year old male with right brachial plexus injury was posted for intercostal nerve to musculocutaneous nerve transfer using sural nerve graft on the right arm. Anesthetic management was tailored to avoid muscle relaxants to enable intraoperative neuromonitoring, so our emphasis was on intravenous and inhalational anesthesia. Standard monitors were connected along with BIS monitor for monitoring patient vitals. Patient was given routine premedication and after that preoxygenated with inhalation at 4% sevoflurane for 3mins along with propofol at 2 mg/kg IV, remifentanil 100 µg IV and ketamine at 1 mg/kg IV. BIS reading came to 30 after 3 mins and at this point patient was intubated and connected to ventilator, maintenance of anesthesia was done with the help of mixture of propofol 4 mg/mL, ketamine 10 mg/mL and remifentanil 6 µg/mL in a 50 mL syringe. Initially patient was kept on infusion at a rate 6 mL/hr but the BIS reading was between 55-65, so the infusion dose was increased to 9 mL/hr and BIS reading reduced to 50 and throughout the procedure which lasted a total of 8 hrs the patients BIS reading was maintained between 45-55. Infusion was stopped 30 mins prior to the completion of procedure and inhalation was stopped at the time of dressing. Patient was extubated intraoperatively when the BIS reading was around 90 and was shifted to recovery with stable vitals.
The Bispectral Index (BIS) offers an objective and precise method for monitoring the depth of anesthesia,.which is a crucial component of some Enhanced Recovery After Surgery (ERAS) guidelines.. ERAS is an evidence-based approach to surgical care aimed at improving the quality of perioperative care and supporting quick recovery. It is recommended that the facility of BIS monitoring be available at all secondary and tertiary level surgical set-ups for optimum safety of the patients and satisfaction of the anesthesia and the surgical teams.
Authors affiliations:
- Uday Gollamudi, Associate Professor, Apollo Institute of Medical Sciences and Research, Jubilee Hills, Hyderabad, Telangana, India; Email: gollamudiudayreddy@gmail.com; {ORCID:0000-0002-8509-3546}
- Pravalllika Rallapalli, Junior Resident, Nagar, Hydershakote, Hyderabad, Telangana, India; Email; rallapallipravallika@gmail.com; {ORCID:0009-0003-4079-3551}
ABSTRACT
Bispectral Index (BIS) monitoring has gained popularity during the recent past, in selected cases. It uses a processed Electroencephalograph (EEG) to provide a value between 0 and 100, indicating brain activity and anesthetic depth. Monitoring the depth of anesthesia is a critical aspect of ensuring patient safety during medical procedures. The bispectral index (BIS) monitor is pivotal in this process. Maintaining BIS values within the range of 40 to 60 is essential to prevent anesthesia awareness and mitigate potential long-term psychological consequences.
Keywords: Anesthesia; Bispectral Index monitoring; Brain activity; Electroencephalograph
Citation: Gollamudi U, Rallapalli P. Importance of BIS monitoring in sedation procedures and to attain optimum depth of anesthesia: a case series. Anaesth. pain intensive care 2026;30(2):362-66. DOI: 10.35975/apic.v30i2.3135
Received: October 15, 2025; Revised: November 12, 2025; Accepted: November 16, 2025
1. INTRODUCTION
BIS monitoring involves the application of 4 electrodes on the forehead. The skin on the forehead is first cleaned with an alcohol swab, and then 2 to 5 seconds of digital pressure is applied over the sensor leads.1 The sensor is comprised of disposable wet gel electrodes. EMG activity of the frontalis muscle is measured by lead 4, which is the ground electrode as well. The information is displayed on the BIS view monitor providing insights into their anesthesia depth. Monitoring the depth of anesthesia is very important during any procedure. Anesthesia that's too deep can cause hemodynamic changes, and anesthesia that is too light carries the risk of recall or awareness during anesthesia..2 Awareness during anesthesia is a very serious complication with potential long-term psychological sequelae such as anxiety and posttraumatic stress disorder..3 When the bispectral index (BIS) value is maintained below 60, it decreases the incidence of anesthesia awareness..3 The BIS monitor is the first FDA-approved method to assess the hypnotic effects of drugs..4 Precisely assessing the depth of anesthesia remains a persistent challenge for clinical anesthesiologists. BIS represents a significant development in the objective assessment of the depth of anesthesia, providing valuable real-time feedback to anesthesia providers..5 Conventional monitoring of anesthetic depth is primarily assessed by the patient's clinical signs and symptoms, such as changes in heart rate, blood pressure, and limb movements..6, 7Lacking objective data support, these methods also face challenges in continuous monitoring due to low specificity and sensitivity..6Such limitations may lead to inaccurate and untimely assessments, potentially resulting in either excessive or insufficient anesthesia, which significantly impacts patients' mental health, disease recovery, and long-term survival rates..6
The Bispectral Index (BIS) offers an objective and precise method for monitoring the depth of anesthesia,.8 which is a crucial component of some Enhanced Recovery After Surgery (ERAS) guidelines..9,10 ERAS is an evidence-based approach to surgical care aimed at improving the quality of perioperative care and supporting quick recovery..10,11
Figure 1: Patient’s head showing placement of electrodes
Figure-2: BIS monitoring range values
2. CASE SERIES
CASE 1:
A 35 year old female patient was diagnosed with bipolar disorder along with psychosis. No improvement was noticed after taking oral treatment medications for 10 days, hence the patient was posted for electroconvulsive therapy (ECT) therapy under anesthesia. ECT was planned for the patient, and written informed consent was obtained from the patient's husband. Pre-anesthetic checkup was done for the patient. The patient was kept nil by mouth for 8 hrs. The objective of ECT is to induce seizure with the minimum required electric intensity, fitting the condition of each patient, to treat specific psychiatric disorders.
The first few cycles of ECT were given without BIS monitoring and at the time of procedure the seizure duration attained was not adequate. The depth of anesthesia has been shown to impact seizure characteristics and level of stimulation energy. Deep anesthesia may reduce the antidepressant effect of ECT.12 and increase the risk of cognitive side effects..13 Light anesthesia might result in awareness .14 but leads to improved seizures quality. .15 Since then monitoring of BIS value has been adopted. The patient was monitored with the help of pulse oximetry, non-invasive blood pressure, five-lead ECG monitor and BIS monitor during the procedure. Baseline vitals were within normal limits and BIS monitor showed value of 95. Injection glycopyrrolate 0.2 mg intravenous (IV) and injection ondansetron 4 mg IV were given. The patient was pre-oxygenated with 100% oxygen for 3 min using Bain's circuit. The patient was induced with 60 mg propofol IV, remifentanil 100 mcg IV and muscle relaxation by 50 mg of succinylcholine IV. The patient was ventilated manually with 100% oxygen using a tight-fitting facemask and Bain's circuit. After 60 sec of succinylcholine administration, the BIS monitor showed a valve of 50 and then a mouth gag was inserted to prevent the tongue bite. Electric stimulation was provided and seizure duration was 30-70 sec. After ECT was given, bag-mask ventilation was resumed until the patient had adequate spontaneous respirations and till BIS value was above 90. During the procedure, the patient had transient hypertension (140-160/90-100 mmHg), and tachycardia (120–130) and the BIS value was around 80, recovery was uneventful. The patient had undergone another six sessions of ECT in next 2 weeks. After six sessions, psychiatric symptoms were markedly improved. Two weeks later, the patient was discharged with oral olanzapine 7.5 mg once-a-day.
BIS monitoring during ECT is important because it helps to standardize anesthetic depth, potentially optimizing seizure quality, duration and also facilitating faster recovery. Titration of anesthetic drugs may be especially useful in ECT to optimize electrical and clinical responses and reduce side effects.
CASE 2:
A 28 years old women with history of 2 previous normal deliveries and laparoscopic appendectomy was posted for laparoscopic tubectomy but the patient had history of awareness during the surgery when she was undergoing lap appendectomy. This would have happened because the patient would have been in lighter plane of anesthesia during the surgical procedure and due to this she has developed post-traumatic stress. Now we have counselled the patient and gave assurance to her. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2 mg/kg iv, remifentanil 100 µg iv, succinylcholine 100 mg iv, Patient was preoxygenated with 100 % oxygen along with 3 % sevoflurane for 3 mins using Bain's circuit and then BUSKA LMA was placed when the patient BIS value was around 30 after which patient was connected to ventilator and maintenance of anesthesia was done with propofol and ketamine iv intermittently along with sevoflurane as inhalational agent. The BIS was maintained throughout the procedure between 40-50 and once the procedure was completed inhalational agent was cutoff and we stopped maintenance dosage, after 15 mins the BIS value came upto 80 and then we removed the LMA and bag mask ventilation was continued till the BIS reading came to 90. Patient was then shifted to recovery and was comfortable. When asked about the awareness during the procedure she replied that she was comfortable and didn’t have any awareness. Hence BIS monitoring is an important tool for providing optimum anesthesia experience to the patient.
CASE 3:
A 25 years old women had lump in the breast for which fibroadenoma surgery was planned. Previously she had undergone laparoscopic cholecystectomy in outside hospital under general anesthesia, during which she had history of delayed recovery post procedure and was kept on ventilator in postoperative care unit. Now we have counselled the patient and gave assurance to her. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2 mg/kg iv, remifentanil 100 µg iv, atracurium 0.5 mg/kg iv then the patient was preoxygenated with 100% oxygen along with 3 % sevoflurane for 3 min using Bain's circuit. We avoided succinylcholine because of history of delayed recovery. When BIS value reading was around 40 the patient was intubated with 7 size ETT with the help of direct laryngoscopy. Patient was connected to ventilator with a mixture of oxygen and air along with sevoflurane for maintenance of anesthesia. Maintenance dose of atracurium was given only when the BIS reading was in the low 60’s. Post procedure reversal was given and the patient was extubated. Recovery from anesthesia was uneventful.
CASE 4:
A 45 years old male with cancer tongue and buccal mucosa with METS extending to the neck was posted for hemiglossectomy, hemimandibulectomy with fibular graft along with neck dissection and chest graft. Surgeons want deep postoperative sedation for at least 1 day. Patient had Mallampati grade 4. Pre-anesthetic check-up was done for the patient. The patient was kept nil by mouth for 8 hrs.
Patient was monitored with the help of 5 lead ECG, non-invasive blood pressure, pulse oximetry and BIS monitor. Premedication with iv glycopyrrolate 0.2 mg and iv ondansetron 4 mg were given. The patient induced with propofol 2mg/kg iv, remifentanil 100 µg iv, succinylcholine 100 mg iv, Patient was preoxygenated with 100% oxygen along with 3 % sevoflurane for 3 mins using Bain's circuit. Nasal intubation was done with north nasal tube of size 7.5. Tube fixed after bilateral air entry checked and was equal. Foleys catheter was placed. Maintenance of anesthesia throughout the procedure was done with the help of atracurium infusion along with sevoflurane as inhalation agent. BIS reading was maintained between 40-50 throughout the procedure. But as the graft was placed the surgeons wanted patient to be kept in deep sedation post operatively for 24 hrs. Atracurium infusion was continued post operatively, iv fentanyl was started at the rate of 4 µg/kg and doses were titrated depending on BIS score. Monitoring was continued postoperatively. Patent connected to ventilator on ACVC mode. BIS monitoring was continued for 24 hrs postoperatively with values between 50-60. After 24 hrs infusions were stopped and patient extubated after giving reversal. Recovery was uneventful.
CASE 5:
A 30 year old male was admitted with features of raised intracranial pressure. MRI brain revealed third ventricle mass about 2 cms with epicentre in the pineal gland with mass effect and hydrocephalus. She was planned for an endoscopic third ventriculostomy and biopsy. After placing standard monitors induction and intubation were done with standard anesthesia drugs without giving any muscle relaxant. Total intravenous anesthesia with propofol was maintained with titrated doses so that BIS value was between 40-50. Neuroendoscope was introduced through right frontal burr hole and irrigated with ringer lactate solution. Within 15 seconds of insertion of neuroendoscope, the BIS value dropped from 40 to 5, mean arterial pressure increased from 90 to 130 mmHg, heartrate raised from 70 to 150/ min. Changes were notified to the surgeon, neuroendoscope was removed and lateral ventricle decompressed with a ventriculoperitoneal (VP) shunt needle. BIS improved from 5 to 35 within a minute and reached baseline within 2 minutes. After this neuroendoscope was reintroduced, ventriculostomy and biopsy was done. After the completion of the procedure the patent woke up without any delay and post extubation GCS was 15. Post procedure the CT of the brain revealed mild pneumoventricle with reduction in hydrocephalus.
CASE 6:
A 48 years old female with encephalitis, adrenal insufficiency, left lung collapse and in septic shock is intubated and connected to mechanical ventilator for the past 10 days and is posted for tracheostomy. Standard monitors were connected along with BIS monitor. Routine premedication was given and patients endotracheal tube connected to bain circuit and patient was manually ventilated with intermittent dose of etomidate and remifentanil based on BIS value at the time of procedure. Just before insertion of tracheostomy tube the endotracheal tube was pulled out, now Bain circuit was connected to tracheostomy tube and once the tube was confirmed is in place the subsequent doses of anesthetic drugs were stopped and patient was shifted to MICU and connected to mechanical ventilator for further management.
CASE 7:
A 22 year old male with right brachial plexus injury was posted for intercostal nerve to musculocutaneous nerve transfer using sural nerve graft on the right arm. Anesthetic management was tailored to avoid muscle relaxants to enable intraoperative neuromonitoring, so our emphasis was on intravenous and inhalational anesthesia. Standard monitors were connected along with BIS monitor for monitoring patient vitals. Patient was given routine premedication and after that preoxygenated with inhalation at 4% sevoflurane for 3mins along with propofol at 2 mg/kg IV, remifentanil 100 µg IV and ketamine at 1 mg/kg IV. BIS reading came to 30 after 3 mins and at this point patient was intubated and connected to ventilator, maintenance of anesthesia was done with the help of mixture of propofol 4 mg/mL, ketamine 10 mg/mL and remifentanil 6 µg/mL in a 50 mL syringe. Initially patient was kept on infusion at a rate 6 mL/hr but the BIS reading was between 55-65, so the infusion dose was increased to 9 mL/hr and BIS reading reduced to 50 and throughout the procedure which lasted a total of 8 hrs the patients BIS reading was maintained between 45-55. Infusion was stopped 30 mins prior to the completion of procedure and inhalation was stopped at the time of dressing. Patient was extubated intraoperatively when the BIS reading was around 90 and was shifted to recovery with stable vitals.
3. CONCLUSION
The Bispectral Index (BIS) offers an objective and precise method for monitoring the depth of anesthesia,.which is a crucial component of some Enhanced Recovery After Surgery (ERAS) guidelines.. ERAS is an evidence-based approach to surgical care aimed at improving the quality of perioperative care and supporting quick recovery. It is recommended that the facility of BIS monitoring be available at all secondary and tertiary level surgical set-ups for optimum safety of the patients and satisfaction of the anesthesia and the surgical teams.
- Ethical considerations
- Conflict of interest
- Funding
- Authors’ contribution
8. REFERENCES
- Johansen JW. Update on bispectral index monitoring. Best Pract Res Clin Anaesthesiol. 2006 Mar;20(1):81-99. [PubMed]
- Froese L, Dian J, Gomez A, Batson C, Sainbhi AS, Zeiler FA. Association Between Processed Electroencephalogram-Based Objectively Measured Depth of Sedation and Cerebrovascular Response: A Systematic Scoping Overview of the Human and Animal Literature. Front Neurol. 2021;12:692207. [PMC free article] [PubMed]
- Avidan MS, Zhang L, Burnside BA, Finkel KJ, Searleman AC, Selvidge JA, Saager L, Turner MS, Rao S, Bottros M, Hantler C, Jacobsohn E, Evers AS. Anesthesia awareness and the bispectral index. N Engl J Med. 2008 Mar 13;358(11):1097-108. [PubMed]
- Ge SJ, Zhuang XL, Wang YT, Wang ZD, Li HT. Changes in the rapidly extracted auditory evoked potentials index and the bispectral index during sedation induced by propofol or midazolam under epidural block. Br J Anaesth. 2002 Aug;89(2):260.[PubMed]
- Ferreira AL, Mendes JG, Nunes CS, Amorim P. [Evaluation of Bispectral Index time delay in response to anesthesia induction: an observational study]. Braz J Anesthesiol. 2019 Jul-Aug;69(4):377-382. [PMC free article] [PubMed]
- Dutta H., Suchismita M., Baisakhi L., Sarbari S., Uday S. M., Sarmila G. Monitoring of general anesthesia by qCON and qNOX indices versus conventional clinical parameters in urological surgery: a randomized controlled clinical trial. Asian Journal of Medical Sciences . 2024;15(3):20–25. doi: 10.3126/ajms.v15i3.59955. [DOI] [Google Scholar]
- Bajaj P. Depth of anaesthesia: clinical applications. Indian Journal of Anaesthesia . 2007;51:p. 461. [Google Scholar]
- Mathur S., Patel J., Goldstein S., Hendrix J. M., Jain A. Bispectral Index . St. Petersburg, FL, USA: StatPearls Publishing; 2023. [PubMed] [Google Scholar]
- BISTM for Enhanced Recovery after Surgery Medtronic. 2021. https://www.medtronic.com/covidien/en-us/clinical-solutions/bis-enhanced-recovery-after-surgery.html.
- Feldheiser A., Aziz O., Baldini G., et al. Enhanced Recovery after Surgery (ERAS) for gastrointestinal surgery, part 2: consensus statement for anaesthesia practice. Acta Anaesthesiologica Scandinavica . 2016;60(3):289–334. doi: 10.1111/aas.12651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Altman A. D., Helpman L., McGee J., et al. Enhanced recovery after surgery: implementing a new standard of surgical care. Canadian Medical Association Journal . 2019;191(17):E469–E475. doi: 10.1503/cmaj.180635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Baerdemaeker et al.Anaesthesia for patients with mood disorders Curr Opin Anaesth (2005)
- Deiner et al. Electroconvulsive therapy and anaesthesia Int Anesth Clin (2009)
- M. Singh et al. Evaluation of etomidate for seizure duration in electroconvulsivotherapy: a systematic review and meta-analysis J ECT (2015)
- D. MacPherson et al. Cognitive impairment following electroconvulsive therapy — does the choice of anesthetic agent make a difference? J ECT (2008)