Nouran Mohsen Ahmed Fahmy *1 , Gamal Fouad Saleh Zaki 2 , Waleed AM Al Taher 3 , Tarek Samir SalahEldin Shabana 4 , Sarah Hamdy Mohamed Ali 5
Authors affiliations:
Background: Bipolar hip hemiarthroplasty is the most common surgical intervention for femoral neck fractures. Optimum postoperative analgesia with the least complications is critical in enhancing functional rehabilitation. In this study, an evaluation of the effectiveness of SIFI block under ultrasound guidance in relation to multimodal intravenous analgesia in controlling postoperative pain in bipolar hip hemiarthroplasty was conducted.
Methodology: Sixty subjects were randomly assigned to receive multimodal analgesia or a SIFI block. Total consumption of morphine in 24 postoperative hours, duration to first request for rescue analgesia, pain evaluation, duration to ambulation, and complications' rate, respectively, were secondary and principal measured outcomes in both groups.
Results: Consumption of morphine in SIFI group was significantly less (P < 0.001), and request for rescue analgesia in SIFI group developed much later (P < 0.001). Scores for pain in SIFI group were consistently less when compared with the multimodal group (P < 0.001). Duration to ambulation, however, did not exhibit any significant variation between groups (P = 0.591). Application of SIFI block showed a reduced postoperative complications' incidence.
Conclusion: The study concludes that SIFI under ultrasound guidance yields better analgesia, less consumption of opiates, and fewer complications when compared with multimodal analgesia. These observations promote its use as a strong form of analgesia in bipolar hip hemiarthroplasty cases.
Keywords: Suprainguinal fascia iliaca; Multimodal analgesia; Hip hemiarthroplasty; Postoperative complications; Morphine consumption
Citation: Fahmy NMA, Zaki GFS, Shabana TSS, Ali SHM. Suprainguinal fascia iliaca block vs. multimodal analgesia for pain control following hip hemiarthroplasty. Anaesth. pain intensive care 2025;30(2):147-159. DOI: 10.35975/apic.v30i2.3120
Received: March 10, 2025; Revised: August 28, 2025; Accepted: February 02, 2026
The efficient postoperative management of hip hemiarthroplasty (HHA) pain is important for optimizing recovery, minimizing complications, and enhancing overall patient outcomes, particularly in the older population.1 Hip fractures cause significant morbidity and mortality, and, therefore, effective postoperative pain management is important in allowing early mobilization, minimizing postoperative delirium, and preventing cardiopulmonary complications secondary to prolonged immobility.2,3 Despite its importance, attaining an ideal balance between effective analgesia and minimizing complications secondary to opioid use is a significant challenge. Although effective for pain, opioids have many complications, including respiratory depression, nausea, emesis, ileus, and hyperalgesia secondary to the administration of opioids.4 In an attempt to maximize postoperative pain management in orthopedic surgical practice therefore, increased use of opioid-sparing techniques, including multimodal and regional anesthetic techniques, has gained prominence in an attempt to maximize postoperative pain management in such settings.
Multimodal analgesia has long been considered to be the gold standard for postoperative pain management in hip surgery.5 This technique involves concurrent administration of a variety of drugs acting through a variety of mechanisms, allowing for synergistic pain relief with concurrent reduced use of opioids.6 Common multimodal protocols include acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, and opioids according to individual patient requirements.7 In spite of its efficacy in minimizing opioid use, multimodal therapy fails to abolish altogether the use of opioids, and a proportion of patients will develop breakthrough pain necessitating supplementary use of opioids.8 As a consequence, regional anesthetic techniques have become increasingly popular alternatives and adjuncts to multimodal therapy, providing localized pain relief with fewer systemic complications.9
The suprainguinal fascia iliaca (SIFI) block is a new and developing modality of regional anesthetic for postoperative pain management in hip surgery.10 First developed in 2011, this intervention was developed following an anatomical study designed to maximize the effectiveness of the traditional fascia iliaca block through selective stimulation of femoral, obturator, and lateral femoral cutaneous nerves.11 Unlike an infrainguinal approach, suprainguinal delivery enables a larger distribution of local anesthetic, including lumbar and sacral plexus structures involved in the innervation of the hip.12 Consequently, SIFI block yields a superior level of analgesia compared with a traditional fascia iliaca block and is accompanied by a significant postoperative reduction in the use of opioids in hip surgical patients.13
Recent research has emphasized the efficacy of SIFI block in minimizing opioid use and improving postoperative pain management in hip surgery settings. Vermeylen et al.14 conducted a randomized controlled trial that showed that subjects who received SIFI block showed a significantly lesser demand for morphine in addition to enhanced postoperative pain evaluation compared with subjects who received conventional multimodal analgesia. In addition, SIFI block has been associated with accelerated mobilization, a critical constituent in preventing postoperative complications such as deep vein thrombosis, pneumonia, and pressure sore.15,16 All these observations have suggested that SIFI block could have significant advantages over conventional multimodal analgesia, particularly in older adults with hip hemiarthroplasty.
Nevertheless, growing evidence in favor of regional anesthetic techniques, a lack of direct comparisons in the current literature continues to surround the effectiveness of SIFI block over multimodal intravenous analgesia in bipolar hip hemiarthroplasty specifically. With growing concern over minimizing perioperative use of opioids, it is critical to evaluate the efficacy, safety, and overall effectiveness of these two modalities of analgesia in terms of rehabilitation function. In an attempt to bridge such a gap, the current investigation aims to compare efficacy, opioid-sparing efficacy, and patient satisfaction with SIFI block with multimodal intravenous analgesia in hip hemiarthroplasty subjects. By comparing these two modalities in a logical and sequential manner, the current investigation could generate clinically relevant information that can benefit anesthesiologists, orthopedists, and pain clinicians in optimizing perioperative pain management in terms of its refinement. In addition, such observations could have a larger impact in terms of optimizing postoperative pain in terms of its management in orthopedic surgical cases and in developing opioid-saving techniques in older adults.
The primary objective of this study is to evaluate overall opioid use in the first 24 postoperative hours in bipolar hip hemiarthroplasty patients who receive either multimodal intravenous analgesia or an ultrasound-guided suprainguinal fascia iliaca (SIFI) block. This investigation aims to understand to what level, if any, the SIFI block can reduce opioid dependence and enable enhanced postoperative pain management. The secondary objectives involved the evaluation of first request times for opioids, a marker for SIFI block efficacy duration in comparison with multimodal analgesia, and postoperative severity of pain measured with the use of a Visual Analog Scale (VAS) at several postoperative times, allowing for a proper analysis of postoperative intensity of pain over 24 postoperative hours. The investigation included postoperative mobilization timing, emphasizing early mobilization to reduce complications and enhance long-term rehabilitation. Any postoperative complications, including hematoma, hypotension, bradycardia, and postoperative nausea and vomiting (PONV), were documented in an evaluation of SIFI block safety in comparison with traditional multimodal analgesia. By investigating these objectives, this study aims to present significant clinical evidence for best practice in postoperative hip hemiarthroplasty pain management. The results can contribute to optimizing opioid-saving protocols for postoperative pain, with a view to enhancing patient outcomes and raising the level of care in orthopedic surgical practice.
This randomized, prospective, comparative study was conducted at Ain Shams University Hospitals between December 2022 and December 2023. The study protocol was approved by the Research Ethics Committee of the Faculty of Medicine, Ain Shams University (FMASU MD 12/2023, FWA 000017585) and was registered in the Pan African Clinical Trial Registry (PACTR202305920421968). Written informed consent was obtained from all participants before enrolment. The study followed the Declaration of Helsinki guidelines.
A total of 60 patients, aged 40 to 70 years, scheduled for hip hemiarthroplasty under spinal anesthesia were included in the study. Patients were randomly assigned to one of two equal groups (30 patients per group) using a computer-generated randomization table: Group C, which served as the Control group and received Multimodal Analgesia, and Group F served as the intervention group and received SIFI Block.
The sample size was calculated using STATA 10 with a 5% alpha error and 80% power, based on prior data showing mean oxycodone consumption of 61.4 ± 15.8 mg in the control group and 40.0 ± 10.0 mg in the FICB group, assuming a common standard deviation of 2. A minimum of 30 patients/group (total 60) was required, accounting for a 20% dropout rate.
Patients were excluded if they had spinal abnormalities affecting spinal anesthesia, refused participation, had bleeding disorders or coagulopathy, an infection at the injection site, or a known allergy to local anesthetics. Additional exclusions included multiple fractures complicating pain assessment, neuromuscular disorders altering pain perception, significant cognitive impairment affecting pain reporting, preoperative long-acting opioid use impacting analgesic outcomes, or failed spinal anesthesia requiring conversion to general anesthesia.
Postoperative data collection was performed at structured time points to ensure a comprehensive assessment of pain control and functional recovery. Data were recorded every 15 minutes during the first hour in the Post-Anesthesia Care Unit (PACU), followed by every two hours for the first 12–24 hours postoperatively.
The primary outcome was to compare total opioid consumption between the two groups measured as the cumulative amount of morphine (mg) administered within the first 24 hours postoperatively.
The secondary outcomes included multiple parameters to assess postoperative pain management, functional recovery, and safety.
Time to first opioid request (on-demand analgesia for breakthrough pain): The duration from the surgery completion to the initial request for IV morphine administration was recorded.
Postoperative pain assessment: Pain intensity was measured using the Visual Analog Scale (VAS) at structured time points. VAS scores were documented every 15 minutes during the first hour in the Post-Anesthesia Care Unit (PACU), followed by every two hours for the first 12 hours postoperatively and then at 24 hours post-surgery. Visual Analog Scale (VAS) is a 10-cm linear scale, with 0 cm representing “no pain” and 10 cm indicating “worst possible pain.” A single-blind observer recorded the VAS scores at specified intervals. If a patient reported a VAS score of ≥3, a rescue dose of IV morphine (3 mg) was administered. Suppose the VAS score remained ≥5 after the initial dose; an additional 2 mg of IV morphine was given. If, after the second dose, the VAS score remained >5 in Group F, the block was deemed unsuccessful, and the patient was excluded from the study.
Onset of ambulation: Defined as the ability to walk independently or with assistive devices, the time to the first successful ambulation attempt will be assessed for both groups.
Complications related to the nerve block: Patients were closely monitored for any postoperative complications, including hematoma, hypotension, bradycardia, and PONV, and were systematically recorded within the first 24 hours postoperatively. If hypotension occurred, defined as a drop in blood pressure by ≥20% from baseline, it was managed with titrated doses of IV ephedrine (10–30 mg diluted in 10 mL of normal saline 0.9%) and administered as needed. In cases of bradycardia (heart rate <60 bpm) accompanied by signs of poor perfusion, IV atropine (0.5 mg) was administered. If postoperative nausea and vomiting (PONV) occurred, IV ondansetron (4 mg diluted in 10 mL of normal saline 0.9%) was administered gradually over 10 minutes to prevent further discomfort.
All patients underwent preoperative assessment, during which they were instructed to fast for eight hours before surgery. Upon arrival at the operating theatre, intravenous (IV) access was established under strict aseptic conditions, and Lactated Ringer's solution was infused at a rate of 10 mL/kg to maintain adequate intravascular volume. Sedation was administered using titrated increments of IV midazolam (1 mg per dose) and fentanyl (50 µg per dose) to ensure patient comfort before spinal anesthesia. Continuous hemodynamic monitoring was performed throughout the surgical procedure using non-invasive blood pressure (NIBP), heart rate (HR), electrocardiogram (ECG), and pulse oximetry (SpO₂) to ensure patient safety and stability.
2.1. Spinal Anesthesia Protocol
Spinal anesthesia was performed under strict aseptic conditions with a 25-gauge Quincke spinal needle at the L3-L4 or L4-L5 intervertebral space. A volume of 2-2.5 mL of 0.5% heavy bupivacaine was given, with the dose adjusted according to the patient's height to achieve an optimal spread of anesthesia. Additionally, 25 µg of fentanyl was added to increase analgesic efficacy and prolong sensory blockade. The beginning of the sensory block was confirmed by establishing a loss of sensation using a cold sensation test with an ice pack. It was noted to ensure an adequate block level prior to surgical incision that the highest dermatome level at which the patient could not feel the cold stimulus was recorded. The surgeon was allowed to start the operation when an appropriate block level of sensitivities was established. The patient was excluded from the study in case of failure of spinal anesthesia and performance of general anesthesia to avoid bias in postoperative analgesia and opioid consumption results.
2.2. Group C (Multimodal Analgesia Protocol)
The drug prophylaxis with multi-modal analgesia was thus given to Group C pre-operatively with optimized pain management on the principle of minimum opioid intake. Oral premedication was prescribed with 75 mg pregabalin and 200 mg oral celecoxib one hour pre-operatively, while 1 gm intravenous paracetamol was administered, followed by a repeat every six hours up to the first postoperative 24 hours. Intravenous ketorolac 30 mg was then given every six hours to enhance analgesia further. Care was taken not to exceed a total daily dose of 120 mg. Intravenous morphine 3 mg was given at the end of the surgery to provide immediate postoperative analgesia. On the second postoperative day, all patients were switched to oral paracetamol 500 mg every six hours as their main analgesic agent.
2.3. SIFI Block (Group F)
Following surgery, patients in Group F received an ultrasound-guided suprainguinal fascia iliaca (SIFI) block using the technique originally described by Hebbard (2011). The patient was positioned supine with the hip extended to facilitate anatomical landmark identification and optimal ultrasound imaging. The anterior superior iliac spine (ASIS) was palpated, and a high-frequency linear ultrasound probe was positioned just inferior and medial to the ASIS, perpendicular to the inguinal ligament—a commonly recommended orientation for enhanced visualization. In patients with higher body mass index (BMI), a low-frequency curved ultrasound probe was used to ensure deeper tissue penetration and optimal imaging quality. A 22-gauge, 4-inch echogenic needle was introduced in-plane under real-time ultrasound guidance. As the needle was advanced, tactile resistance loss was encountered upon piercing the fascia iliaca, followed by entry into the iliacus muscle beneath. This technique ensures optimal anesthetic spread and effective blockade of the femoral, obturator, and lateral femoral cutaneous nerves.
Upon the penetration of fascia iliaca, confirmation of the typical "pop" was noticed. The needle was then partially retracted and redirected at the outer edge of the iliacus muscle. A volume of 1–2 mL of saline or local anesthetic was then injected to verify proper placement, as evidenced by the appropriate spread between the fascia iliaca and the iliacus muscle. After confirmation of satisfactory spread, 40 mL of 0.25% bupivacaine was injected in divided doses using intermittent aspiration to prevent intravenous injection. The injection was placed to direct the local anesthetic upward, which allows separation between the iliacus muscle and the fascia iliaca and, thus, adequate spreading of the anesthetic. The skin was prepared prior to performing the block with chlorhexidine or povidone-iodine antiseptic solution to decrease the risk of infection. It was done in complete asepsis. This ensured that the patient's safety was addressed and followed with the best clinical practice.
2.4. statistical analysis
Data were analyzed using IBM SPSS Statistics Version 22.0. Numerical variables were reported as mean ± standard deviation (SD) for normally distributed data and median (interquartile range, IQR) for non-normally distributed data, while categorical variables were presented as frequency and percentage. The independent t-test was used for normally distributed numerical comparisons, the Mann-Whitney U test for non-normally t-test was used for normally distributed numerical comparisons, the Mann-Whitney U test for non-normally distributed data, and the chi-square (χ²) test for categorical variables. Kaplan-Meier survival analysis assessed the time to first rescue analgesia, with group differences evaluated using the log-rank test. A p-value > 0.05 was considered non-significant, p = 0.05 was significant, and p < 0.01 was highly significant.
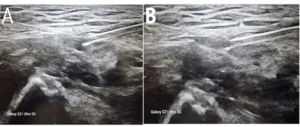
Figure 1. Ultrasound-Guided Suprainguinal Fascia Iliaca Block (SIFI)
Representative ultrasound images demonstrating the suprainguinal fascia iliaca block (SIFI) technique. (A) Pre-injection ultrasound scan depicting the anatomical structures prior to local anesthetic administration. (B) Post-injection ultrasound scan illustrating the diffusion of local anesthetic within the fascia iliaca compartment, effectively targeting the femoral, obturator, and lateral femoral cutaneous nerves.
The study included a total of 60 patients, who were randomly assigned into two equal groups (Group C and Group F, n = 30 each). There were no statistically significant differences in demographic and baseline characteristics between the two groups (P > 0.05) (Table 1). The mean age was 62.67 ± 6.28 years in Group C and 62.17 ± 6.73 years in Group F (P = 0.767). The distribution of sex was also comparable between the groups (P = 0.435), as was the body mass index (BMI) (P = 0.870). Additionally, the ASA classification was evenly distributed between ASA I, II, and III patients, with no significant differences between the groups (P = 1.000).
Total opioid consumption within the first 24 hours was significantly lower in Group F compared to Group C (P < 0.001). Patients in Group C required an average of 6.97 ± 0.81 mg of morphine, while those in Group F consumed only 4.20 ± 0.89 mg.
The time to first rescue analgesia was significantly longer in Group F compared to Group C (P < 0.001). Patients in Group C required their first rescue dose at 4.13 ± 0.73 hours, whereas Group F experienced a significantly delayed Postoperative pain perception, assessed using the Visual Analog Scale (VAS-10), showed significant differences between the two groups at multiple time points (P < 0.001) (Table 2, Figure 4). During the first six hours postoperatively, patients in Group C experienced significantly higher VAS scores compared to Group F at 30 minutes, 45 minutes, 60 minutes, 2 hours, and 6 hours (P < 0.001 for all comparisons). Beyond the six-hour mark, VAS scores remained slightly higher in Group C; however, the differences were not statistically significant (P > 0.05). At 24 hours postoperatively, pain scores between the two groups were comparable, with no significant differences observed (P > 0.05). The mean time to ambulation was 20.67 ± 5.71 hours in Group C and 21.47 ± 5.76 hours in Group F, with no statistically significant difference between the groups (P = 0.591).
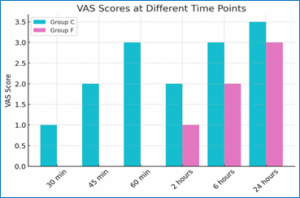
Figure 1: VAS Scores at Different Time Points.
Although Group C exhibited higher rates of hypotension, bradycardia, and postoperative nausea and vomiting (PONV) compared to Group F, none of these differences reached statistical significance (P > 0.05, Table 3). Similarly, the incidence of hematoma, hypotension, bradycardia, and PONV was higher in Group C, but the differences remained non-significant.
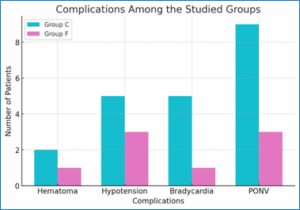
Figure 2: Complications observed in the two groups
This study aimed to evaluate the efficacy of ultrasound-guided suprainguinal fascia iliaca (SIFI) block compared to multimodal intravenous analgesia in patients undergoing bipolar hip hemiarthroplasty (BHA). Our findings demonstrate that SIFI block significantly reduced total opioid consumption within the first 24 hours postoperatively, prolonged the time to first rescue analgesia, and lowered postoperative pain scores. Furthermore, while no significant difference in the onset of ambulation was observed between the two groups, patients in the SIFI group experienced fewer opioid-related side effects, albeit not to a statistically significant extent. The superior analgesic effect observed in the SIFI group can be attributed to its ability to target the femoral, obturator, and lateral femoral cutaneous nerves, which play a crucial role in hip innervation. These findings are consistent with the growing body of evidence now available that supports regional anesthesia techniques as an integral component of multi-modal pain management approaches. The most important result of the study is the statically lower total opioid consumption within the first 24 h following surgery in Group F (SIFI Block) compared to Group C (Multimodal Analgesia), with a p-value of less than 0.001. This is a sign of the clinical efficiency of the SIFI Block in reducing postoperative opioid consumption, which has s significant implications for enhanced recovery pathways and opioid stewardship in perioperative care. These findings are in concordance with many previous studies that highlight the opioid-sparing effect of FICB in orthopedic surgery.17,18 Desmet et al. (2017) demonstrated that SIFI block is associated with significantly reduced opioid consumption and uperior postoperative pain relief compared with standard multimodal analgesia after s THA.19 The SIFI Block is a variety of regional anesthesia techniques that ensure targeted analgesia by interrupting the nociceptive transmission at the neural level and, consequently, reducing the need for opioid analgesics.20,21 Local anesthetic regional nerve blocks have been confirmed by various studies earlier to uperior postoperative pain relief compared with standard multimodal analgesia after
THA.19 The SIFI Block is a variety of regional anesthesia techniques that ensure targeted analgesia by interrupting the nociceptive transmission at the neural level and, consequently, reducing the need for opioid analgesics.20,21 Local anesthetic regional nerve blocks have been confirmed by various studies earlier to decrease postoperative opioid consumption and its side effects.22,23 For instance, Krosch et al. (2024) and Winoker et al (2022).24, 25 established that peripheral nerve blocks markedly decrease the need for opioids and enhance patient satisfaction while minimizing opioid-related complications like postoperative nausea and vomiting, and respiratory depression. The clinical significance of opioid reduction is not limited to the period of immediate postoperative recovery. Opioid-induced side effects include ileus, cognitive dysfunction, and delayed ambulation; all of them impede rehabilitation and prolong the stay in hospitals.26 The SIFI Block contributes to an improved functional outcome with reduced opioid dependence, hence advocating the concepts of multimodal analgesia, which has always called for opioid-sparing techniques.27,28 This becomes all the more important in light of the ongoing opioid crisis, wherein excessive opioid exposure during the postoperative period can predispose patients to long-term dependence and abuse.29,30 Additionally, the SIFI Block could be included as part of the routine management for perioperative pain, meeting all the criteria of the ERAS recommendation for opioid minimization to enhance early recovery and discharge.31,32 The probable reduction in opioid consumption may further contribute to early mobilization, reduced incidence of postoperative ileus, and increased overall patient satisfaction and trajectory toward recovery.33-35 From the health economics point of view, one can also expect cost savings with regional nerve blocks such as SIFI Block by avoiding opioid-related complications and healthcare costs associated with these complications.36,37 These would include hospital readmissions, extended lengths of stay, and increased numbers of additional interventions because of opioid-induced adverse effects. In fact, several regional anesthesia techniques are proven cost-effective by various studies and thus see routine application in perioperative care.38,39
The time to first rescue analgesia being significantly longer in Group F (11.48 ± 1.13 hours) compared with Group C (4.13 ± 0.73 hours) (P < 0.001) underlines the higher efficacy of the SIFI Block in prolonging postoperative analgesia. This finding is particularly relevant in the context of enhanced recovery after surgery protocols, where optimization of pain management plays a very important role in improving clinical outcomes. A delayed need for rescue analgesia provides the clinical advantage of improved patient comfort, less frequent pain-related nursing interventions, and thus increased overall patient satisfaction,.40 Moreover, avoiding the significant early onset of postoperative pain will limit the risk of central sensitization, known to play a determining role in the progression from acute to chronic postsurgical pain.41 Our findings further support the added value of the SIFI Block compared with only multimodal systemic analgesia, showing, in this sense, a clear benefit from regional anesthesia techniques in prolonging effective analgesia. Prolonged pain relief with the block decreases opioid consumption and contributes to a more stable hemodynamic profile by the attenuation of sympathetic activation secondary to pain.42,43 This is particularly advantageous in populations that are prone to opioid-related side effects, such as elderly patients or those with inherent respiratory compromise. Moreover, the prolonged duration of analgesia has important implications for postoperative rehabilitation. Effective pain control is a cornerstone of early mobilization and physiotherapy, both of which are important components of accelerated recovery pathways.44 Patients who experience prolonged analgesia with regional techniques may show better adherence to rehabilitation protocols, thereby reducing the risk of complications such as thromboembolism, pulmonary infections, and joint stiffness.45 Moreover, the possibility of an easier recovery process enabled by prolonged regional analgesia may also result in shorter lengths of hospital stay and decreased costs of care.46
The high reduction in VAS scores at all time points within the first six postoperative hours in Group F (P < 0.001) underlines that SIFI Block is effective in providing superior early analgesia compared to a multi-modal regimen alone. This finding is especially relevant since a well-established correlation exists between early postoperative pain intensity and long-term surgical outcomes. Poorly controlled pain in the immediate postoperative period may be provocative of exaggerated neuroendocrine stress responses leading to increased systemic inflammation, immunosuppression, and risk of complications, including delayed wound healing and cardiovascular instability.47 Severe acute pain is a well-recognized risk factor for the development of CPSP, and central sensitization plays an important role in the transition of pain from acute injury to chronic status.48,49 By effectively reducing early pain, the SIFI Block may thus reduce these risks and contribute to a smoother postoperative trajectory.50,51 Despite its robust initial analgesic effect, the progressive convergence of pain scores between the groups beyond the six-hour mark, with no statistically significant difference by 24 hours (P = 0.567), suggests a time-limited benefit. Similarly, Khan et al. (2021) demonstrated that FICB reduced postoperative pain scores and opioid intake after hip arthroplasty, reinforcing the efficacy of regional anesthesia. Madubishi et al. (2016) compared FICB with intravenous fentanyl, reporting that patients in the FICB group had significantly lower VAS scores and required fewer rescue analgesic doses.52, 53 This supports our finding that regional anesthesia contributes to prolonged pain relief and a reduction in breakthrough pain episodes. Moreover, Gola et al. (2021) evaluated opioid consumption in THA patients, concluding that FICB significantly decreased opioid intake and improved pain management compared to PCA-based analgesia.54 Conversely, Bang et al. (2016) reported no significant difference in pain scores between FICB and non-FICB groups when all patients received PCA, suggesting that the efficacy of regional anesthesia may depend on the overall analgesic regimen used.53 Our findings also align with those of Wang et al.56 who demonstrated that patients receiving ultrasound-guided SIFI block exhibited lower pain scores at rest and during movement, with reduced fentanyl consumption over 48 hours following total hip arthroplasty. This further confirms the effectiveness of SIFI block in enhancing postoperative analgesia and reducing opioid dependency. While the SIFI Block is considered highly effective for pain management during the early postoperative period, this often wears out with time, and an overall multimodal analgesic approach has to be incorporated to ensure adequate pain control.57 The transient nature of this block emphasizes the need for strategies aimed at prolonging its duration, particularly in surgeries associated with prolonged postoperative pain.
The absence of a statistically significant difference in time to ambulation between the two groups (P = 0.591) would suggest that while the SIFI Block significantly enhances early postoperative analgesia, it does not equate to a measurable improvement in early functional recovery. This finding highlights the complex interplay between pain control and mobility, reinforcing the notion that postoperative ambulation is influenced by multiple factors beyond analgesia alone.58 One possible explanation for similar ambulation times may be related to surgical stress and physiological responses to trauma. Even in the setting of adequate pain control, systemic inflammatory responses and autonomic dysfunction subsequent to surgery contribute to delayed mobilization.59 Surgical stress is associated with high levels of pro-inflammatory cytokines, altered muscular function, and fluid shifts that may negatively affect a patient's ability or desire to ambulate early.60 Furthermore, in many instances, patient-specific psychosocial factors, such as fear of movement due to pain and phobia of complications, contribute to the avoidance of movements irrespective of sufficient analgesia.61 Another important determinant relates to the effects of standardized rehabilitation programs. Early mobilization, at a fixed time postoperatively, regardless of pain, is an institutionalized feature of postoperative care in many of the enhanced recovery after surgery programs.62-64 The uniformity of these protocols across both groups may have minimized the potential impact of superior analgesia on actual time to ambulation. Moreover, healthcare provider encouragement, physiotherapy support, and institutional mobility guidelines likely played a role in maintaining similar ambulation timelines between the two groups.
Our results that postoperative complications such as hypotension, bradycardia, and postoperative nausea and vomiting (PONV) were slightly higher in Group C than in Group F, although not statistically significant (P > 0.05), provide important insights into the potential advantages of regional anesthesia techniques in mitigating systemic side effects. The lower incidence of these complications in Group F may be attributed to the reduced opioid consumption associated with the SIFI Block, aligning with existing literature that links opioid use to increased risks of PONV, respiratory depression, and hemodynamic instability. Opioids exert their effects by binding to central and peripheral opioid receptors, leading to nausea and vomiting via stimulation of the chemoreceptor trigger zone, as well as causing vasodilation and bradycardia due to their sympatholytic properties.65,66 Therefore, the SIFI Block, by reducing opioid requirements, may also contribute to a more stable perioperative physiological profile. The mild reduction in bradycardia and hypotension in Group F also indicates that the SIFI Block did not result in significant autonomic disturbances-an important consideration in the evaluation of safety for regional anesthesia techniques.67 Unlike neuraxial anesthesia, which can cause severe hypotension due to sympathetic blockade, peripheral nerve blocks tend to exhibit a more favorable hemodynamic profile because they provide regional analgesia without widespread autonomic suppression.68,69 In fact, this finding is particularly important in high-risk populations such as elderly patients and those with multiple comorbidities undergoing major orthopedic procedures such as hip hemiarthroplasty. Patients tend to develop perioperative cardiovascular instability associated more so with advanced age that encompasses a stage of autonomic dysregulation along with hypertension or pre-existing heart ischemic disorders. By offering effective analgesia while preserving hemodynamic stability, the SIFI Block emerges as a potentially safer alternative to more systemic analgesic approaches.70
Despite its strengths, this study has several limitations that must be acknowledged. The sample size was relatively small, with only 60 patients, which, while sufficient to detect differences in pain scores and opioid consumption, may limit the generalizability of the findings to broader populations. Future studies with larger cohorts are necessary to validate these results. Additionally, this study was conducted at a single tertiary care center, meaning that variations in surgical technique, anesthetic management, and rehabilitation protocols could impact the external validity of the findings. Another limitation is the short-term follow-up, as the study focused solely on pain outcomes within the first 24 hours postoperatively, preventing the assessment of long-term functional recovery and potential chronic pain development. Lastly, the study was not double-blinded, meaning that both patients and healthcare providers were aware of the intervention received, which may have introduced bias in pain score reporting. Future studies incorporating multicenter designs, larger sample sizes, longer follow-up durations, and blinding protocols would strengthen the evidence base and further refine postoperative pain management strategies.
7. Data availability
Numerical data generated during this study is available on request.
8. Ethical considerations
Approved by Ain Shams University Ethics Committee (FMASU MD 12/2023, FWA 000017585) and registered in PACTR (PACTR202305920421968). Written consent was obtained.
9. Competing interests
None
11. Authors' contributions
All authors contributed to the study and approved the final manuscript. The corresponding author, Nouran Mohsen Ahmed Fahmy, will handle all communications with the journal at every stage of the refereeing and publication process, including post-publication responsibilities.
Authors affiliations:
- Nouran Mohsen Ahmed Fahmy, MSc. Assistant Lecturer of Anesthesia, Intensive Care, and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; ORCID: 0009-0007-8188-5312; Email: mohsen@med.asu.edu.eg; Tel: +20 100 319 4054
- Gamal Fouad Saleh Zaki, MD, PhD. Professor of Anesthesia, Intensive Care, and Pain Management, Faculty of Medicine, Ain Shams University; Email: gamalzaki@gmail.com
- Waleed AM Al Taher, MD, PhD. Professor of Anesthesia, Intensive Care, and Pain Management, Faculty of Medicine, Ain Shams University; Email: Waleedaltaher@hotmail.com
- Tarek Samir SalahEldin Shabana, MD, PhD. Assistant Professor of Anesthesia, Intensive Care, and Pain Management, Faculty of Medicine, Ain Shams University; Email: shabana@hotmail.com
- Sarah Hamdy Mohamed Ali, MD. Lecturer of Anesthesia, Intensive Care, and Pain Management, Faculty of Medicine, Ain Shams University; Email: 84@gmail.com
ABSTRACT
Background: Bipolar hip hemiarthroplasty is the most common surgical intervention for femoral neck fractures. Optimum postoperative analgesia with the least complications is critical in enhancing functional rehabilitation. In this study, an evaluation of the effectiveness of SIFI block under ultrasound guidance in relation to multimodal intravenous analgesia in controlling postoperative pain in bipolar hip hemiarthroplasty was conducted.
Methodology: Sixty subjects were randomly assigned to receive multimodal analgesia or a SIFI block. Total consumption of morphine in 24 postoperative hours, duration to first request for rescue analgesia, pain evaluation, duration to ambulation, and complications' rate, respectively, were secondary and principal measured outcomes in both groups.
Results: Consumption of morphine in SIFI group was significantly less (P < 0.001), and request for rescue analgesia in SIFI group developed much later (P < 0.001). Scores for pain in SIFI group were consistently less when compared with the multimodal group (P < 0.001). Duration to ambulation, however, did not exhibit any significant variation between groups (P = 0.591). Application of SIFI block showed a reduced postoperative complications' incidence.
Conclusion: The study concludes that SIFI under ultrasound guidance yields better analgesia, less consumption of opiates, and fewer complications when compared with multimodal analgesia. These observations promote its use as a strong form of analgesia in bipolar hip hemiarthroplasty cases.
Keywords: Suprainguinal fascia iliaca; Multimodal analgesia; Hip hemiarthroplasty; Postoperative complications; Morphine consumption
Citation: Fahmy NMA, Zaki GFS, Shabana TSS, Ali SHM. Suprainguinal fascia iliaca block vs. multimodal analgesia for pain control following hip hemiarthroplasty. Anaesth. pain intensive care 2025;30(2):147-159. DOI: 10.35975/apic.v30i2.3120
Received: March 10, 2025; Revised: August 28, 2025; Accepted: February 02, 2026
1. INTRODUCTION
The efficient postoperative management of hip hemiarthroplasty (HHA) pain is important for optimizing recovery, minimizing complications, and enhancing overall patient outcomes, particularly in the older population.1 Hip fractures cause significant morbidity and mortality, and, therefore, effective postoperative pain management is important in allowing early mobilization, minimizing postoperative delirium, and preventing cardiopulmonary complications secondary to prolonged immobility.2,3 Despite its importance, attaining an ideal balance between effective analgesia and minimizing complications secondary to opioid use is a significant challenge. Although effective for pain, opioids have many complications, including respiratory depression, nausea, emesis, ileus, and hyperalgesia secondary to the administration of opioids.4 In an attempt to maximize postoperative pain management in orthopedic surgical practice therefore, increased use of opioid-sparing techniques, including multimodal and regional anesthetic techniques, has gained prominence in an attempt to maximize postoperative pain management in such settings.
Multimodal analgesia has long been considered to be the gold standard for postoperative pain management in hip surgery.5 This technique involves concurrent administration of a variety of drugs acting through a variety of mechanisms, allowing for synergistic pain relief with concurrent reduced use of opioids.6 Common multimodal protocols include acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, and opioids according to individual patient requirements.7 In spite of its efficacy in minimizing opioid use, multimodal therapy fails to abolish altogether the use of opioids, and a proportion of patients will develop breakthrough pain necessitating supplementary use of opioids.8 As a consequence, regional anesthetic techniques have become increasingly popular alternatives and adjuncts to multimodal therapy, providing localized pain relief with fewer systemic complications.9
The suprainguinal fascia iliaca (SIFI) block is a new and developing modality of regional anesthetic for postoperative pain management in hip surgery.10 First developed in 2011, this intervention was developed following an anatomical study designed to maximize the effectiveness of the traditional fascia iliaca block through selective stimulation of femoral, obturator, and lateral femoral cutaneous nerves.11 Unlike an infrainguinal approach, suprainguinal delivery enables a larger distribution of local anesthetic, including lumbar and sacral plexus structures involved in the innervation of the hip.12 Consequently, SIFI block yields a superior level of analgesia compared with a traditional fascia iliaca block and is accompanied by a significant postoperative reduction in the use of opioids in hip surgical patients.13
Recent research has emphasized the efficacy of SIFI block in minimizing opioid use and improving postoperative pain management in hip surgery settings. Vermeylen et al.14 conducted a randomized controlled trial that showed that subjects who received SIFI block showed a significantly lesser demand for morphine in addition to enhanced postoperative pain evaluation compared with subjects who received conventional multimodal analgesia. In addition, SIFI block has been associated with accelerated mobilization, a critical constituent in preventing postoperative complications such as deep vein thrombosis, pneumonia, and pressure sore.15,16 All these observations have suggested that SIFI block could have significant advantages over conventional multimodal analgesia, particularly in older adults with hip hemiarthroplasty.
Nevertheless, growing evidence in favor of regional anesthetic techniques, a lack of direct comparisons in the current literature continues to surround the effectiveness of SIFI block over multimodal intravenous analgesia in bipolar hip hemiarthroplasty specifically. With growing concern over minimizing perioperative use of opioids, it is critical to evaluate the efficacy, safety, and overall effectiveness of these two modalities of analgesia in terms of rehabilitation function. In an attempt to bridge such a gap, the current investigation aims to compare efficacy, opioid-sparing efficacy, and patient satisfaction with SIFI block with multimodal intravenous analgesia in hip hemiarthroplasty subjects. By comparing these two modalities in a logical and sequential manner, the current investigation could generate clinically relevant information that can benefit anesthesiologists, orthopedists, and pain clinicians in optimizing perioperative pain management in terms of its refinement. In addition, such observations could have a larger impact in terms of optimizing postoperative pain in terms of its management in orthopedic surgical cases and in developing opioid-saving techniques in older adults.
The primary objective of this study is to evaluate overall opioid use in the first 24 postoperative hours in bipolar hip hemiarthroplasty patients who receive either multimodal intravenous analgesia or an ultrasound-guided suprainguinal fascia iliaca (SIFI) block. This investigation aims to understand to what level, if any, the SIFI block can reduce opioid dependence and enable enhanced postoperative pain management. The secondary objectives involved the evaluation of first request times for opioids, a marker for SIFI block efficacy duration in comparison with multimodal analgesia, and postoperative severity of pain measured with the use of a Visual Analog Scale (VAS) at several postoperative times, allowing for a proper analysis of postoperative intensity of pain over 24 postoperative hours. The investigation included postoperative mobilization timing, emphasizing early mobilization to reduce complications and enhance long-term rehabilitation. Any postoperative complications, including hematoma, hypotension, bradycardia, and postoperative nausea and vomiting (PONV), were documented in an evaluation of SIFI block safety in comparison with traditional multimodal analgesia. By investigating these objectives, this study aims to present significant clinical evidence for best practice in postoperative hip hemiarthroplasty pain management. The results can contribute to optimizing opioid-saving protocols for postoperative pain, with a view to enhancing patient outcomes and raising the level of care in orthopedic surgical practice.
2. METHODOLOGY
This randomized, prospective, comparative study was conducted at Ain Shams University Hospitals between December 2022 and December 2023. The study protocol was approved by the Research Ethics Committee of the Faculty of Medicine, Ain Shams University (FMASU MD 12/2023, FWA 000017585) and was registered in the Pan African Clinical Trial Registry (PACTR202305920421968). Written informed consent was obtained from all participants before enrolment. The study followed the Declaration of Helsinki guidelines.
A total of 60 patients, aged 40 to 70 years, scheduled for hip hemiarthroplasty under spinal anesthesia were included in the study. Patients were randomly assigned to one of two equal groups (30 patients per group) using a computer-generated randomization table: Group C, which served as the Control group and received Multimodal Analgesia, and Group F served as the intervention group and received SIFI Block.
The sample size was calculated using STATA 10 with a 5% alpha error and 80% power, based on prior data showing mean oxycodone consumption of 61.4 ± 15.8 mg in the control group and 40.0 ± 10.0 mg in the FICB group, assuming a common standard deviation of 2. A minimum of 30 patients/group (total 60) was required, accounting for a 20% dropout rate.
Patients were excluded if they had spinal abnormalities affecting spinal anesthesia, refused participation, had bleeding disorders or coagulopathy, an infection at the injection site, or a known allergy to local anesthetics. Additional exclusions included multiple fractures complicating pain assessment, neuromuscular disorders altering pain perception, significant cognitive impairment affecting pain reporting, preoperative long-acting opioid use impacting analgesic outcomes, or failed spinal anesthesia requiring conversion to general anesthesia.
Postoperative data collection was performed at structured time points to ensure a comprehensive assessment of pain control and functional recovery. Data were recorded every 15 minutes during the first hour in the Post-Anesthesia Care Unit (PACU), followed by every two hours for the first 12–24 hours postoperatively.
The primary outcome was to compare total opioid consumption between the two groups measured as the cumulative amount of morphine (mg) administered within the first 24 hours postoperatively.
The secondary outcomes included multiple parameters to assess postoperative pain management, functional recovery, and safety.
Time to first opioid request (on-demand analgesia for breakthrough pain): The duration from the surgery completion to the initial request for IV morphine administration was recorded.
Postoperative pain assessment: Pain intensity was measured using the Visual Analog Scale (VAS) at structured time points. VAS scores were documented every 15 minutes during the first hour in the Post-Anesthesia Care Unit (PACU), followed by every two hours for the first 12 hours postoperatively and then at 24 hours post-surgery. Visual Analog Scale (VAS) is a 10-cm linear scale, with 0 cm representing “no pain” and 10 cm indicating “worst possible pain.” A single-blind observer recorded the VAS scores at specified intervals. If a patient reported a VAS score of ≥3, a rescue dose of IV morphine (3 mg) was administered. Suppose the VAS score remained ≥5 after the initial dose; an additional 2 mg of IV morphine was given. If, after the second dose, the VAS score remained >5 in Group F, the block was deemed unsuccessful, and the patient was excluded from the study.
Onset of ambulation: Defined as the ability to walk independently or with assistive devices, the time to the first successful ambulation attempt will be assessed for both groups.
Complications related to the nerve block: Patients were closely monitored for any postoperative complications, including hematoma, hypotension, bradycardia, and PONV, and were systematically recorded within the first 24 hours postoperatively. If hypotension occurred, defined as a drop in blood pressure by ≥20% from baseline, it was managed with titrated doses of IV ephedrine (10–30 mg diluted in 10 mL of normal saline 0.9%) and administered as needed. In cases of bradycardia (heart rate <60 bpm) accompanied by signs of poor perfusion, IV atropine (0.5 mg) was administered. If postoperative nausea and vomiting (PONV) occurred, IV ondansetron (4 mg diluted in 10 mL of normal saline 0.9%) was administered gradually over 10 minutes to prevent further discomfort.
All patients underwent preoperative assessment, during which they were instructed to fast for eight hours before surgery. Upon arrival at the operating theatre, intravenous (IV) access was established under strict aseptic conditions, and Lactated Ringer's solution was infused at a rate of 10 mL/kg to maintain adequate intravascular volume. Sedation was administered using titrated increments of IV midazolam (1 mg per dose) and fentanyl (50 µg per dose) to ensure patient comfort before spinal anesthesia. Continuous hemodynamic monitoring was performed throughout the surgical procedure using non-invasive blood pressure (NIBP), heart rate (HR), electrocardiogram (ECG), and pulse oximetry (SpO₂) to ensure patient safety and stability.
2.1. Spinal Anesthesia Protocol
Spinal anesthesia was performed under strict aseptic conditions with a 25-gauge Quincke spinal needle at the L3-L4 or L4-L5 intervertebral space. A volume of 2-2.5 mL of 0.5% heavy bupivacaine was given, with the dose adjusted according to the patient's height to achieve an optimal spread of anesthesia. Additionally, 25 µg of fentanyl was added to increase analgesic efficacy and prolong sensory blockade. The beginning of the sensory block was confirmed by establishing a loss of sensation using a cold sensation test with an ice pack. It was noted to ensure an adequate block level prior to surgical incision that the highest dermatome level at which the patient could not feel the cold stimulus was recorded. The surgeon was allowed to start the operation when an appropriate block level of sensitivities was established. The patient was excluded from the study in case of failure of spinal anesthesia and performance of general anesthesia to avoid bias in postoperative analgesia and opioid consumption results.
2.2. Group C (Multimodal Analgesia Protocol)
The drug prophylaxis with multi-modal analgesia was thus given to Group C pre-operatively with optimized pain management on the principle of minimum opioid intake. Oral premedication was prescribed with 75 mg pregabalin and 200 mg oral celecoxib one hour pre-operatively, while 1 gm intravenous paracetamol was administered, followed by a repeat every six hours up to the first postoperative 24 hours. Intravenous ketorolac 30 mg was then given every six hours to enhance analgesia further. Care was taken not to exceed a total daily dose of 120 mg. Intravenous morphine 3 mg was given at the end of the surgery to provide immediate postoperative analgesia. On the second postoperative day, all patients were switched to oral paracetamol 500 mg every six hours as their main analgesic agent.
2.3. SIFI Block (Group F)
Following surgery, patients in Group F received an ultrasound-guided suprainguinal fascia iliaca (SIFI) block using the technique originally described by Hebbard (2011). The patient was positioned supine with the hip extended to facilitate anatomical landmark identification and optimal ultrasound imaging. The anterior superior iliac spine (ASIS) was palpated, and a high-frequency linear ultrasound probe was positioned just inferior and medial to the ASIS, perpendicular to the inguinal ligament—a commonly recommended orientation for enhanced visualization. In patients with higher body mass index (BMI), a low-frequency curved ultrasound probe was used to ensure deeper tissue penetration and optimal imaging quality. A 22-gauge, 4-inch echogenic needle was introduced in-plane under real-time ultrasound guidance. As the needle was advanced, tactile resistance loss was encountered upon piercing the fascia iliaca, followed by entry into the iliacus muscle beneath. This technique ensures optimal anesthetic spread and effective blockade of the femoral, obturator, and lateral femoral cutaneous nerves.
Upon the penetration of fascia iliaca, confirmation of the typical "pop" was noticed. The needle was then partially retracted and redirected at the outer edge of the iliacus muscle. A volume of 1–2 mL of saline or local anesthetic was then injected to verify proper placement, as evidenced by the appropriate spread between the fascia iliaca and the iliacus muscle. After confirmation of satisfactory spread, 40 mL of 0.25% bupivacaine was injected in divided doses using intermittent aspiration to prevent intravenous injection. The injection was placed to direct the local anesthetic upward, which allows separation between the iliacus muscle and the fascia iliaca and, thus, adequate spreading of the anesthetic. The skin was prepared prior to performing the block with chlorhexidine or povidone-iodine antiseptic solution to decrease the risk of infection. It was done in complete asepsis. This ensured that the patient's safety was addressed and followed with the best clinical practice.
2.4. statistical analysis
Data were analyzed using IBM SPSS Statistics Version 22.0. Numerical variables were reported as mean ± standard deviation (SD) for normally distributed data and median (interquartile range, IQR) for non-normally distributed data, while categorical variables were presented as frequency and percentage. The independent t-test was used for normally distributed numerical comparisons, the Mann-Whitney U test for non-normally t-test was used for normally distributed numerical comparisons, the Mann-Whitney U test for non-normally distributed data, and the chi-square (χ²) test for categorical variables. Kaplan-Meier survival analysis assessed the time to first rescue analgesia, with group differences evaluated using the log-rank test. A p-value > 0.05 was considered non-significant, p = 0.05 was significant, and p < 0.01 was highly significant.
Figure 1. Ultrasound-Guided Suprainguinal Fascia Iliaca Block (SIFI)
Representative ultrasound images demonstrating the suprainguinal fascia iliaca block (SIFI) technique. (A) Pre-injection ultrasound scan depicting the anatomical structures prior to local anesthetic administration. (B) Post-injection ultrasound scan illustrating the diffusion of local anesthetic within the fascia iliaca compartment, effectively targeting the femoral, obturator, and lateral femoral cutaneous nerves.
3.RESULTS
The study included a total of 60 patients, who were randomly assigned into two equal groups (Group C and Group F, n = 30 each). There were no statistically significant differences in demographic and baseline characteristics between the two groups (P > 0.05) (Table 1). The mean age was 62.67 ± 6.28 years in Group C and 62.17 ± 6.73 years in Group F (P = 0.767). The distribution of sex was also comparable between the groups (P = 0.435), as was the body mass index (BMI) (P = 0.870). Additionally, the ASA classification was evenly distributed between ASA I, II, and III patients, with no significant differences between the groups (P = 1.000).
| Table 1: Comparative demographic characteristics | |||
| Characteristics | Group C
(n = 30) |
Group F
(n = 30) |
P-value |
| Age (years) | 62.67 ± 6.28 | 62.17 ± 6.73 | 0.767 |
| Gender: Female Male |
15 (50.0%) | 19 (63.3%) | 0.435 |
| 15 (50.0%) | 11 (36.7%) | ||
| BMI (kg/m2) | 26.83 ± 3.98 | 27.14 ± 3.86 | 0.870 |
| ASA I | 10 (33.3%) | 9 (30.0%) | 1.000 |
| ASA II | 16 (53.3%) | 18 (60.0%) | |
| ASA III | 4 (13.3%) | 3 (10.0%) | |
| Data Presented as mean ± SD or n (%); P < 0.05 considered as significant | |||
Total opioid consumption within the first 24 hours was significantly lower in Group F compared to Group C (P < 0.001). Patients in Group C required an average of 6.97 ± 0.81 mg of morphine, while those in Group F consumed only 4.20 ± 0.89 mg.
The time to first rescue analgesia was significantly longer in Group F compared to Group C (P < 0.001). Patients in Group C required their first rescue dose at 4.13 ± 0.73 hours, whereas Group F experienced a significantly delayed Postoperative pain perception, assessed using the Visual Analog Scale (VAS-10), showed significant differences between the two groups at multiple time points (P < 0.001) (Table 2, Figure 4). During the first six hours postoperatively, patients in Group C experienced significantly higher VAS scores compared to Group F at 30 minutes, 45 minutes, 60 minutes, 2 hours, and 6 hours (P < 0.001 for all comparisons). Beyond the six-hour mark, VAS scores remained slightly higher in Group C; however, the differences were not statistically significant (P > 0.05). At 24 hours postoperatively, pain scores between the two groups were comparable, with no significant differences observed (P > 0.05). The mean time to ambulation was 20.67 ± 5.71 hours in Group C and 21.47 ± 5.76 hours in Group F, with no statistically significant difference between the groups (P = 0.591).
| Table 2: Comparative Postoperative VAS Scores | |||
| Time Point | Group C
(n = 30) |
Group F
(n = 30) |
P-value |
| VAS (30 min) | 1 (0-2) | 0 (0-0) | < 0.001* |
| VAS (45 min) | 2 (2-3) | 0 (0-1) | < 0.001* |
| VAS (60 min) | 3 (2-3) | 0 (0-0) | < 0.001* |
| VAS (2 hours) | 2 (1-3) | 1 (0-1) | < 0.001* |
| VAS (6 hours) | 3 (3-4) | 2 (2-2) | < 0.001* |
| VAS (24 hours) | 3.5 (3-5) | 3 (3-5) | 0.567 |
| Data presented as mean (Range); *Significant at P < 0.001 | |||
Figure 1: VAS Scores at Different Time Points.
Although Group C exhibited higher rates of hypotension, bradycardia, and postoperative nausea and vomiting (PONV) compared to Group F, none of these differences reached statistical significance (P > 0.05, Table 3). Similarly, the incidence of hematoma, hypotension, bradycardia, and PONV was higher in Group C, but the differences remained non-significant.
| Table 3: Postoperative complications. | |||
| Complication | Group C
(n = 30) |
Group F
(n = 30) |
P-value |
| Hematoma | 2 (6.7%) | 1 (3.3%) | 1.000 |
| Hypotension | 5 (16.7%) | 3 (10.0%) | 0.706 |
| Bradycardia | 5 (16.7%) | 1 (3.3%) | 0.195 |
| PONV | 9 (30.0%) | 3 (10.0%) | 0.104 |
Figure 2: Complications observed in the two groups
4. DISCUSSION
This study aimed to evaluate the efficacy of ultrasound-guided suprainguinal fascia iliaca (SIFI) block compared to multimodal intravenous analgesia in patients undergoing bipolar hip hemiarthroplasty (BHA). Our findings demonstrate that SIFI block significantly reduced total opioid consumption within the first 24 hours postoperatively, prolonged the time to first rescue analgesia, and lowered postoperative pain scores. Furthermore, while no significant difference in the onset of ambulation was observed between the two groups, patients in the SIFI group experienced fewer opioid-related side effects, albeit not to a statistically significant extent. The superior analgesic effect observed in the SIFI group can be attributed to its ability to target the femoral, obturator, and lateral femoral cutaneous nerves, which play a crucial role in hip innervation. These findings are consistent with the growing body of evidence now available that supports regional anesthesia techniques as an integral component of multi-modal pain management approaches. The most important result of the study is the statically lower total opioid consumption within the first 24 h following surgery in Group F (SIFI Block) compared to Group C (Multimodal Analgesia), with a p-value of less than 0.001. This is a sign of the clinical efficiency of the SIFI Block in reducing postoperative opioid consumption, which has s significant implications for enhanced recovery pathways and opioid stewardship in perioperative care. These findings are in concordance with many previous studies that highlight the opioid-sparing effect of FICB in orthopedic surgery.17,18 Desmet et al. (2017) demonstrated that SIFI block is associated with significantly reduced opioid consumption and uperior postoperative pain relief compared with standard multimodal analgesia after s THA.19 The SIFI Block is a variety of regional anesthesia techniques that ensure targeted analgesia by interrupting the nociceptive transmission at the neural level and, consequently, reducing the need for opioid analgesics.20,21 Local anesthetic regional nerve blocks have been confirmed by various studies earlier to uperior postoperative pain relief compared with standard multimodal analgesia after
THA.19 The SIFI Block is a variety of regional anesthesia techniques that ensure targeted analgesia by interrupting the nociceptive transmission at the neural level and, consequently, reducing the need for opioid analgesics.20,21 Local anesthetic regional nerve blocks have been confirmed by various studies earlier to decrease postoperative opioid consumption and its side effects.22,23 For instance, Krosch et al. (2024) and Winoker et al (2022).24, 25 established that peripheral nerve blocks markedly decrease the need for opioids and enhance patient satisfaction while minimizing opioid-related complications like postoperative nausea and vomiting, and respiratory depression. The clinical significance of opioid reduction is not limited to the period of immediate postoperative recovery. Opioid-induced side effects include ileus, cognitive dysfunction, and delayed ambulation; all of them impede rehabilitation and prolong the stay in hospitals.26 The SIFI Block contributes to an improved functional outcome with reduced opioid dependence, hence advocating the concepts of multimodal analgesia, which has always called for opioid-sparing techniques.27,28 This becomes all the more important in light of the ongoing opioid crisis, wherein excessive opioid exposure during the postoperative period can predispose patients to long-term dependence and abuse.29,30 Additionally, the SIFI Block could be included as part of the routine management for perioperative pain, meeting all the criteria of the ERAS recommendation for opioid minimization to enhance early recovery and discharge.31,32 The probable reduction in opioid consumption may further contribute to early mobilization, reduced incidence of postoperative ileus, and increased overall patient satisfaction and trajectory toward recovery.33-35 From the health economics point of view, one can also expect cost savings with regional nerve blocks such as SIFI Block by avoiding opioid-related complications and healthcare costs associated with these complications.36,37 These would include hospital readmissions, extended lengths of stay, and increased numbers of additional interventions because of opioid-induced adverse effects. In fact, several regional anesthesia techniques are proven cost-effective by various studies and thus see routine application in perioperative care.38,39
The time to first rescue analgesia being significantly longer in Group F (11.48 ± 1.13 hours) compared with Group C (4.13 ± 0.73 hours) (P < 0.001) underlines the higher efficacy of the SIFI Block in prolonging postoperative analgesia. This finding is particularly relevant in the context of enhanced recovery after surgery protocols, where optimization of pain management plays a very important role in improving clinical outcomes. A delayed need for rescue analgesia provides the clinical advantage of improved patient comfort, less frequent pain-related nursing interventions, and thus increased overall patient satisfaction,.40 Moreover, avoiding the significant early onset of postoperative pain will limit the risk of central sensitization, known to play a determining role in the progression from acute to chronic postsurgical pain.41 Our findings further support the added value of the SIFI Block compared with only multimodal systemic analgesia, showing, in this sense, a clear benefit from regional anesthesia techniques in prolonging effective analgesia. Prolonged pain relief with the block decreases opioid consumption and contributes to a more stable hemodynamic profile by the attenuation of sympathetic activation secondary to pain.42,43 This is particularly advantageous in populations that are prone to opioid-related side effects, such as elderly patients or those with inherent respiratory compromise. Moreover, the prolonged duration of analgesia has important implications for postoperative rehabilitation. Effective pain control is a cornerstone of early mobilization and physiotherapy, both of which are important components of accelerated recovery pathways.44 Patients who experience prolonged analgesia with regional techniques may show better adherence to rehabilitation protocols, thereby reducing the risk of complications such as thromboembolism, pulmonary infections, and joint stiffness.45 Moreover, the possibility of an easier recovery process enabled by prolonged regional analgesia may also result in shorter lengths of hospital stay and decreased costs of care.46
The high reduction in VAS scores at all time points within the first six postoperative hours in Group F (P < 0.001) underlines that SIFI Block is effective in providing superior early analgesia compared to a multi-modal regimen alone. This finding is especially relevant since a well-established correlation exists between early postoperative pain intensity and long-term surgical outcomes. Poorly controlled pain in the immediate postoperative period may be provocative of exaggerated neuroendocrine stress responses leading to increased systemic inflammation, immunosuppression, and risk of complications, including delayed wound healing and cardiovascular instability.47 Severe acute pain is a well-recognized risk factor for the development of CPSP, and central sensitization plays an important role in the transition of pain from acute injury to chronic status.48,49 By effectively reducing early pain, the SIFI Block may thus reduce these risks and contribute to a smoother postoperative trajectory.50,51 Despite its robust initial analgesic effect, the progressive convergence of pain scores between the groups beyond the six-hour mark, with no statistically significant difference by 24 hours (P = 0.567), suggests a time-limited benefit. Similarly, Khan et al. (2021) demonstrated that FICB reduced postoperative pain scores and opioid intake after hip arthroplasty, reinforcing the efficacy of regional anesthesia. Madubishi et al. (2016) compared FICB with intravenous fentanyl, reporting that patients in the FICB group had significantly lower VAS scores and required fewer rescue analgesic doses.52, 53 This supports our finding that regional anesthesia contributes to prolonged pain relief and a reduction in breakthrough pain episodes. Moreover, Gola et al. (2021) evaluated opioid consumption in THA patients, concluding that FICB significantly decreased opioid intake and improved pain management compared to PCA-based analgesia.54 Conversely, Bang et al. (2016) reported no significant difference in pain scores between FICB and non-FICB groups when all patients received PCA, suggesting that the efficacy of regional anesthesia may depend on the overall analgesic regimen used.53 Our findings also align with those of Wang et al.56 who demonstrated that patients receiving ultrasound-guided SIFI block exhibited lower pain scores at rest and during movement, with reduced fentanyl consumption over 48 hours following total hip arthroplasty. This further confirms the effectiveness of SIFI block in enhancing postoperative analgesia and reducing opioid dependency. While the SIFI Block is considered highly effective for pain management during the early postoperative period, this often wears out with time, and an overall multimodal analgesic approach has to be incorporated to ensure adequate pain control.57 The transient nature of this block emphasizes the need for strategies aimed at prolonging its duration, particularly in surgeries associated with prolonged postoperative pain.
The absence of a statistically significant difference in time to ambulation between the two groups (P = 0.591) would suggest that while the SIFI Block significantly enhances early postoperative analgesia, it does not equate to a measurable improvement in early functional recovery. This finding highlights the complex interplay between pain control and mobility, reinforcing the notion that postoperative ambulation is influenced by multiple factors beyond analgesia alone.58 One possible explanation for similar ambulation times may be related to surgical stress and physiological responses to trauma. Even in the setting of adequate pain control, systemic inflammatory responses and autonomic dysfunction subsequent to surgery contribute to delayed mobilization.59 Surgical stress is associated with high levels of pro-inflammatory cytokines, altered muscular function, and fluid shifts that may negatively affect a patient's ability or desire to ambulate early.60 Furthermore, in many instances, patient-specific psychosocial factors, such as fear of movement due to pain and phobia of complications, contribute to the avoidance of movements irrespective of sufficient analgesia.61 Another important determinant relates to the effects of standardized rehabilitation programs. Early mobilization, at a fixed time postoperatively, regardless of pain, is an institutionalized feature of postoperative care in many of the enhanced recovery after surgery programs.62-64 The uniformity of these protocols across both groups may have minimized the potential impact of superior analgesia on actual time to ambulation. Moreover, healthcare provider encouragement, physiotherapy support, and institutional mobility guidelines likely played a role in maintaining similar ambulation timelines between the two groups.
Our results that postoperative complications such as hypotension, bradycardia, and postoperative nausea and vomiting (PONV) were slightly higher in Group C than in Group F, although not statistically significant (P > 0.05), provide important insights into the potential advantages of regional anesthesia techniques in mitigating systemic side effects. The lower incidence of these complications in Group F may be attributed to the reduced opioid consumption associated with the SIFI Block, aligning with existing literature that links opioid use to increased risks of PONV, respiratory depression, and hemodynamic instability. Opioids exert their effects by binding to central and peripheral opioid receptors, leading to nausea and vomiting via stimulation of the chemoreceptor trigger zone, as well as causing vasodilation and bradycardia due to their sympatholytic properties.65,66 Therefore, the SIFI Block, by reducing opioid requirements, may also contribute to a more stable perioperative physiological profile. The mild reduction in bradycardia and hypotension in Group F also indicates that the SIFI Block did not result in significant autonomic disturbances-an important consideration in the evaluation of safety for regional anesthesia techniques.67 Unlike neuraxial anesthesia, which can cause severe hypotension due to sympathetic blockade, peripheral nerve blocks tend to exhibit a more favorable hemodynamic profile because they provide regional analgesia without widespread autonomic suppression.68,69 In fact, this finding is particularly important in high-risk populations such as elderly patients and those with multiple comorbidities undergoing major orthopedic procedures such as hip hemiarthroplasty. Patients tend to develop perioperative cardiovascular instability associated more so with advanced age that encompasses a stage of autonomic dysregulation along with hypertension or pre-existing heart ischemic disorders. By offering effective analgesia while preserving hemodynamic stability, the SIFI Block emerges as a potentially safer alternative to more systemic analgesic approaches.70
5. IMITATIONS
Despite its strengths, this study has several limitations that must be acknowledged. The sample size was relatively small, with only 60 patients, which, while sufficient to detect differences in pain scores and opioid consumption, may limit the generalizability of the findings to broader populations. Future studies with larger cohorts are necessary to validate these results. Additionally, this study was conducted at a single tertiary care center, meaning that variations in surgical technique, anesthetic management, and rehabilitation protocols could impact the external validity of the findings. Another limitation is the short-term follow-up, as the study focused solely on pain outcomes within the first 24 hours postoperatively, preventing the assessment of long-term functional recovery and potential chronic pain development. Lastly, the study was not double-blinded, meaning that both patients and healthcare providers were aware of the intervention received, which may have introduced bias in pain score reporting. Future studies incorporating multicenter designs, larger sample sizes, longer follow-up durations, and blinding protocols would strengthen the evidence base and further refine postoperative pain management strategies.
6. CONCLUSION
This study considerably supports the application of ultrasound-guided suprainguinal fascia iliaca block as an effective and opioid-sparing alternative to multimodal intravenous analgesia after hip hemiarthroplasty. Our results showed that SIFI block significantly decreased total opioid consumption, prolonged the time to first rescue analgesia, and reduced postoperative pain scores in the first 24 hours after surgery.7. Data availability
Numerical data generated during this study is available on request.
8. Ethical considerations
Approved by Ain Shams University Ethics Committee (FMASU MD 12/2023, FWA 000017585) and registered in PACTR (PACTR202305920421968). Written consent was obtained.
9. Competing interests
None
10. Funding
This study was completed by using institutional resources, and no external of industry funding was received.No funding received.11. Authors' contributions
All authors contributed to the study and approved the final manuscript. The corresponding author, Nouran Mohsen Ahmed Fahmy, will handle all communications with the journal at every stage of the refereeing and publication process, including post-publication responsibilities.
12. REFERENCES
- Zhou J, Shi L, Tian C, Gao Y, Wang J, Mao J, et al. Effects of an emergency-based FASE strategy on treating geriatric patients with femoral neck fracture: a retrospective propensity score-matched study. Clin Interv Aging. 2024;19:1867-80. [PubMed] DOI: 2147/CIA.S485809
- Aprisunadi N, Nursalam N, Mustikasari M, Ifadah E, Hapsari ED. Effect of Early Mobilization on Hip and Lower Extremity Postoperative: A Literature Review. SAGE Open Nurs. 2023;9:23779608231167825. [PubMed] DOI: 1177/23779608231167825
- Handoll HH, Cameron ID, Mak JC, Panagoda CE, Finnegan TP. Multidisciplinary rehabilitation for older people with hip fractures. Cochrane Database Syst Rev. 2021;11(11):CD007125. [PubMed] DOI: 1002/14651858.CD007125.pub3
- Luo X, Rao PG, Lei XH, Yang WW, Liao BZ, Guo R. Opioid-free strategies for patient-controlled intravenous postoperative analgesia: a review of recent studies. Front Pharmacol. 2024;15:1454112. [PubMed] DOI: 3389/fphar.2024.1454112
- Chunduri A, Aggarwal AK. Multimodal Pain Management in Orthopedic Surgery. J Clin Med. 2022;11(21):6386. [PubMed] DOI: 3390/jcm11216386
- Fillingham YA, Hannon CP, Buvanendran A, Hamilton WG, Della Valle CJ. Multimodal Analgesia for Hip and Knee Arthroplasty: Eliminating Opioids as the Cornerstone of Postoperative Pain Management. J Arthroplasty. 2020;35(10):2695-6. [PubMed] DOI: 1016/j.arth.2020.05.036
- Kianian S, Bansal J, Lee C, Zhang K, Bergese SD. Perioperative multimodal analgesia: a review of efficacy and safety of the treatment options. Anesthesiol Perioper Sci. 2024;2(1):9. [PubMed] DOI: 1007/s44254-023-00043-1
- Schwenk ES, Mariano ER. Designing the ideal perioperative pain management plan starts with multimodal analgesia. Korean J Anesthesiol. 2018;71(5):345-52. [PubMed] DOI: 4097/kja.d.18.00217
- Chitnis SS, Tang R, Mariano ER. The role of regional analgesia in personalized postoperative pain management. Korean J Anesthesiol. 2020;73(5):363-71. [PubMed] DOI: 4097/kja.20323
- Lim JY, Chan CH. The Suprainguinal Fascia Iliaca Block Prolonging Spinal Anesthesia Duration. Cureus. 2024;16(7):e65732. [PubMed] DOI: 7759/cureus.65732
- Hebbard P, Ivanusic J, Sha S. Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric evaluation of a novel approach. Anaesthesia. 2011;66(4):300-5. [PubMed] DOI: 1111/j.1365-2044.2011.06628.x
- Muse IO, Deiling B, Grinman L, Hadeed MM, Elkassabany N. Peripheral Nerve Blocks for Hip Fractures. J Clin Med. 2024;13(12):3457. [PubMed] DOI: 3390/jcm13123457
- Grinman L, Elmore B, Ardon AE, Hussain A, Malik MF, Hernandez N, et al. Use of Peripheral Nerve Blocks for Total hip Arthroplasty. Curr Pain Headache Rep. 2024;28(11):1113-21. [PubMed] DOI: 1007/s11916-024-01287-7
- Vermeylen K, Desmet M, Leunen I, Soetens F, Neyrinck A, Carens D, et al. Supra-inguinal injection for fascia iliaca compartment block results in more consistent spread towards the lumbar plexus than an infra-inguinal injection: a volunteer study. Reg Anesth Pain Med. 2019;44(5):483-91. [PubMed] DOI: 1136/rapm-2018-100092
- Sucher JF, Barletta JF, Shirah GR, Prokuski LJ, Montanarella PD, Dzandu JK, et al. The safety of continuous fascia iliaca block in patients with hip fracture taking pre-injury anticoagulant and/or antiplatelet medications. Am J Surg. 2022;224(6):1473-7. [PubMed] DOI: 1016/j.amjsurg.2022.08.019
- Wan HY, Li SY, Ji W, Yu B, Jiang N. Fascia Iliaca Compartment Block for Perioperative Pain Management of Geriatric Patients with Hip Fractures: A Systematic Review of Randomized Controlled Trials. Pain Res Manag. 2020;2020:8503963. [PubMed] DOI: 1155/2020/8503963
- Amin SR, Ahmed F. Comparison between pericapsular nerve group block and fascia iliaca compartment block for perioperative pain control in hip surgeries: A meta-analysis from randomized controlled trials. Egypt J Anaesth. 2023;39(1):185-96.DOI: 1080/11101849.2023.2180540
- Hyland SJ, Brockhaus KK, Vincent WR, Spence NZ, Lucki MM, Howkins MJ, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare (Basel). 2021;9(3):333. [PubMed] DOI: 3390/healthcare9030333
- Desmet M, Vermeylen K, Van Herreweghe I, et al. A Longitudinal Supra-Inguinal Fascia Iliaca Compartment Block Reduces Morphine Consumption After Total Hip Arthroplasty. Reg Anesth Pain Med. 2017;42(3):327-33. [PubMed] DOI: 1097/AAP.0000000000000543
- Richter J. Unlearn Pain: The Successful Techniques and Exercises of Psychological Pain Management. Springer Nature; 2023.
- Wyld LN, Rayment C, Bennett MI. Definition and assessment of chronic pain in advanced disease. In: Cherny NI, Fallon MT, Kaasa S, Portenoy RK, Currow DC, editors. Oxford Textbook of Palliative Medicine. 6th ed. Oxford University Press; 2021. p. 313-20.
- Niyonkuru E, Iqbal MA, Zeng R, Zhang X, Ma P. Nerve blocks for postsurgical pain management: a narrative review of current research. J Pain Res. 2024;17:3217-39. [PubMed] DOI: 2147/JPR.S476563
- Memtsoudis SG, Cozowicz C, Bekeris J, Bekere D, Liu J, Soffin EM, et al. Peripheral nerve block anesthesia/analgesia for patients undergoing primary hip and knee arthroplasty: recommendations from the International Consensus on Anesthesia-Related Outcomes after Surgery (ICAROS) group based on a systematic review and meta-analysis of current literature. Reg Anesth Pain Med. 2021;46(11):971-85. [PubMed] DOI: 1136/rapm-2021-102750
- Krosch CFH. Opioid free anesthesia–benefits and risks [dissertation]. Vilnius University; 2024. [FreeText]
- Winoker JS, Koo K, Alam R, Matlaga BR. Opioid-sparing analgesic effects of peripheral nerve blocks in percutaneous nephrolithotomy: A systematic review. J Endourol. 2022;36(1):38-46. [PubMed] DOI: 1089/end.2021.0402
- Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287-98. [PubMed] DOI: 2147/JPR.S144066
- Ma YK, Qu L, Chen N, Chen Z, Li Y, Jiang ALM, et al. Effect of multimodal opioid-sparing anesthesia on intestinal function and prognosis of elderly patients with hypertension after colorectal cancer surgery. BMC Surg. 2024;24(1):341. [PubMed] DOI: 1186/s12893-024-02604-y
- Sullivan D, Lyons M, Montgomery R, Quinlan-Colwell A. Exploring Opioid-Sparing Multimodal Analgesia Options in Trauma: A Nursing Perspective. J Trauma Nurs. 2016;23(6):361-75. [PubMed] DOI: 1097/JTN.0000000000000250
- Neuman MD, Bateman BT, Wunsch H. Inappropriate opioid prescription after surgery. Lancet. 2019;393(10180):1547-57. [PubMed] DOI: 1016/S0140-6736(19)30428-3
- Howard R, Brown CS, Lai YL, Gunaseelan V, Brummett CM, Englesbe M, et al. Postoperative opioid prescribing and new persistent opioid use: the risk of excessive prescribing. Ann Surg. 2023;277(6):e1225-e1231. [PubMed] DOI: 1097/SLA.0000000000005392
- Rømer H, Gazerani P. Perioperative pain-management of patients undergoing amputation: What is the recent evidence in clinical practice? 4th International Conference for Perianaesthesia Nurses, ICPAN, Sydney, Australia. 2017. Available from: https://vbn.aau.dk/en/publications/perioperative-pain-management-of-patients-undergoing-amputation-w/
- Simpson JC, Bao X, Agarwala A. Pain Management in Enhanced Recovery after Surgery (ERAS) Protocols. Clin Colon Rectal Surg. 2019;32(2):121-8. [PubMed] DOI: 1055/s-0038-1676477
- Irani JL, Hedrick TL, Miller TE, Lee L, Steinhagen E, Shogan BD, et al. Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American Society of Colon and Rectal Surgeons and the Society of American Gastrointestinal and Endoscopic Surgeons. Surg Endosc. 2023;37(1):5-30. [PubMed] DOI: 1007/s00464-022-09758-x
- Hedrick TL, McEvoy MD, Mythen MMG, Bergamaschi R, Gupta R, Holubar SD, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. Anesth Analg. 2018;126(6):1896-907. [PubMed] DOI: 1213/ANE.0000000000002742
- Okusaga O, Mowat R, Cook C. Effectiveness of early mobilisation versus laxative use in reducing opioid induced constipation in post-operative orthopaedic patients: an integrative review. Aust J Adv Nurs. 2022;39(2):23-35. [FreeText]
- McEvoy MD, Raymond BL, Krige A. Opioid-sparing perioperative analgesia within enhanced recovery programs. Anesthesiol Clin. 2022;40(1):35-58. [PubMed] DOI: 1016/j.anclin.2021.11.001
- Jogie J, Jogie JA. A Comprehensive Review on the Efficacy of Nerve Blocks in Reducing Postoperative Anesthetic and Analgesic Requirements. Cureus. 2023;15(5):e38552. [PubMed] DOI: 7759/cureus.38552
- Hyland SJ, Brockhaus KK, Vincent WR, Spence NZ, Lucki MM, Howkins MJ, et al. Perioperative Pain Management and Opioid Stewardship: A Practical Guide. Healthcare (Basel). 2021;9(3):333. [PubMed] DOI: 3390/healthcare9030333
- Gray CF, Smith C, Zasimovich Y, Tighe PJ. Economic Considerations of Acute Pain Medicine Programs. Tech Orthop. 2017;32(4):217-25. [PubMed] DOI: 1097/BTO.0000000000000241
- Kefyalew M, Deyassa N, Gidey U, Temesgen M, Mehari M. Improving the time to pain relief in the emergency department through triage nurse-initiated analgesia - a quasi-experimental study from Ethiopia. Afr J Emerg Med. 2024;14(3):161-6. [PubMed] DOI: 1016/j.afjem.2024.06.004
- Chapman CR, Vierck CJ. The transition of acute postoperative pain to chronic pain: an integrative overview of research on mechanisms. J Pain. 2017;18(4):359.e1-359.e38. [PubMed] DOI: 1016/j.jpain.2016.11.004
- Zwolinski NM, Patel KS, Vadivelu N, Kodumudi G, Kaye AD. ERAS protocol options for perioperative pain management of substance use disorder in the ambulatory surgical setting. Curr Pain Headache Rep. 2023;27(5):65-79. [PubMed] DOI: 1007/s11916-023-01108-3
- Prabhakar NK, Chadwick AL, Nwaneshiudu C, Aggarwal A, Salmasi V, Lii TR, et al. Management of postoperative pain in patients following spine surgery: a narrative review. Int J Gen Med. 2022;15:4535-49. [PubMed] DOI: 2147/IJGM.S292698
- Goel S, Deshpande SV, Jadawala VH, Suneja A, Singh R. A Comprehensive Review of Postoperative Analgesics Used in Orthopedic Practice. Cureus. 2023;15(11):e48750. [PubMed] DOI: 7759/cureus.48750
- Weinstein EJ, Levene JL, Cohen MS, Andreae DA, Chao JY, Johnson M, Hall CB, et al. Local anaesthetics and regional anaesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children. Cochrane Database Syst Rev. 2018;6(6):CD007105. [PubMed] DOI: 1002/14651858.CD007105.pub4
- Fu G, Xu L, Chen H, Lin J. State-of-the-art anesthesia practices: a comprehensive review on optimizing patient safety and recovery. BMC Surg. 2025;25(1):32. [PubMed] DOI: 1186/s12893-025-02763-6
- Reysner T, Wieczorowska-Tobis K, Kowalski G, Grochowicka M, Pyszczorska M, Mularski A, et al. The Influence of Regional Anesthesia on the Systemic Stress Response. Reports. 2024;7(4):89. [PubMed] DOI: 3390/reports7040089
- Rosenberger DC, Pogatzki-Zahn EM. Chronic postsurgical pain - update on incidence, risk factors and preventive treatment options. BJA Educ. 2022;22(5):190-6. [PubMed] DOI: 1016/j.bjae.2021.11.008
- Sun M, Wang X, Lu Z, Yang Y, Lv S, Miao M, et al. Chronic postsurgical pain increases postoperative depression risk. J Epidemiol Community Health. 2025;79(1):23-9. [PubMed] DOI: 1136/jech-2024-222761
- VanEenenaam DP Jr, Cardin S, Yang D, O'Brien E, Muhly WT, Sankar WN. Comparison of Suprainguinal Fascia Iliaca Nerve Block and Epidural Analgesia in Patients Undergoing Periacetabular Osteotomy. J Am Acad Orthop Surg. 2024;32(24):1123-9. [PubMed] DOI: 5435/JAAOS-D-24-00177
- Gao Y, Tan H, Sun R, Zhu J. Fascia iliaca compartment block reduces pain and opioid consumption after total hip arthroplasty: A systematic review and meta-analysis. Int J Surg. 2019;65:70-9. [PubMed] DOI: 1016/j.ijsu.2019.03.014
- Khan MH, Hussain S, Khan MG, Bahadar J, Kashif M, Uddin R. Efficacy of Ultrasound Guided Fascia Iliaca Block for Pain Management Compared to Conventional Pain Killers; A Comparative Study. Pak J Med Health Sci. 2021;15(8). DOI: 53350/pjmhs211582525
- Madabushi R, Rajappa GC, Thammanna PP, Iyer SS. Fascia iliaca block vs intravenous fentanyl as an analgesic technique before positioning for spinal anesthesia in patients undergoing surgery for femur fractures-a randomized trial. J Clin Anesth. 2016;35:398-403. [PubMed] DOI: 1016/j.jclinane.2016.09.014
- Gola W, Bialka S, Owczarek AJ, Misiolek H. Effectiveness of Fascia Iliaca Compartment Block after Elective Total Hip Replacement: A Prospective, Randomized, Controlled Study. Int J Environ Res Public Health. 2021;18(9):4891. [PubMed] DOI: 3390/ijerph18094891
- Bang S, Chung J, Jeong J, Bak H, Kim D. Efficacy of ultrasound-guided fascia iliaca compartment block after hip hemiarthroplasty: A prospective, randomized trial. Medicine (Baltimore). 2016;95(39):e5018. [PubMed] DOI: 1097/MD.0000000000005018
- Wang YL, Liu YQ, Ni H, Zhang XL, Ding L, Tong F, et al. Ultrasound-guided, direct suprainguinal injection for fascia iliaca block for total hip arthroplasty: A retrospective study. World J Clin Cases. 2021;9(15):3567-75. [PubMed] DOI: 12998/wjcc.v9.i15.3567
- Ghimire A, Kalsotra S, Tobias JD, Veneziano G. Suprainguinal fascia iliaca compartment block in pediatric-aged patients: An educational focused review. Saudi J Anaesth. 2025;19(1):65-76. [PubMed] DOI: 4103/sja.sja_467_24
- Nelson E, Gan T, Urman R. Predicting Postoperative Pain: A Complex Interplay of Multiple Factors. Anesth Analg. 2021;132(3):652-5. [PubMed] DOI: 1213/ANE.0000000000005200
- Gillis C, Ljungqvist O, Carli F. Prehabilitation, enhanced recovery after surgery, or both? A narrative review. Br J Anaesth. 2022;128(3):434-48. [PubMed] DOI: 1016/j.bja.2021.12.007
- Finnerty CC, Mabvuure NT, Ali A, Kozar RA, Herndon DN. The surgically induced stress response. JPEN J Parenter Enteral Nutr. 2013;37(5 Suppl):21S-29S. [PubMed] DOI: 1177/0148607113496117
- Fenske JN, Berland DW, Chandran S, et al. Pain ManagementAnn Arbor (MI): Michigan Medicine University of Michigan; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572296/
- Tazreean R, Nelson G, Twomey R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J Comp Eff Res. 2022;11(2):121-9. [PubMed] DOI: 2217/cer-2021-0258
- Jain SN, Lamture Y, Krishna M. Enhanced Recovery After Surgery: Exploring the Advances and Strategies. Cureus. 2023;15(10):e47237. [PubMed] DOI: 7759/cureus.47237
- Brown J, Singh K, Dumitru R, Chan E, Kim MP. The Benefits of Enhanced Recovery After Surgery Programs and Their Application in Cardiothoracic Surgery. Methodist Debakey Cardiovasc J. 2018;14(2):77-88. [PubMed] DOI: 14797/mdcj-14-2-77
- Abdalla M. Pharmacology of non-opioid intravenous anesthetics. In: Farag E, Argalious M, Tetzlaff JE, Sharma D, editors. Basic Sciences in Anesthesia. Springer; 2025. p. 117-33.
- El Rabeey M, Shaboob I, Abo Gamaz A. Updates In Postopertive Nausea And Vomiting. Benha Med J. 2022;39(1):46-61. [PubMed] DOI:
- Cui X, Cheng Z, Zhang T, Xu H, Luan H, Feng J, et al. Effect of pericapsular nerve group block and suprainguinal fascia iliaca block on postoperative analgesia and stress response in elderly patients undergoing hip arthroplasty: a prospective randomized controlled double-blind trial. BMC Anesthesiol. 2024;24(1):220. [PubMed] DOI: 1186/s12871-024-02604-8
- Suzuki S, Gerner P, Lirk P. Local anesthetics. In: Hemmings HC, Egan TD, editors. Pharmacology and Physiology for Anesthesia. Elsevier; 2019. p. 390-411. DOI: 1016/B978-0-323-48110-6.00020-X
- Tomulić Brusich K, Valenčić L, Polonijo Ž. Physiology and pharmacology of epidurally administered drugs. In: Epidural Administration-New Perspectives and Uses. IntechOpen; 2023. Available from: https://www.intechopen.com/chapters/85295
- Zhou C, Huang X, Zhuo Z, Wu Q, Liu M, Li S. Effect of different anesthesia depths on perioperative heart rate variability and hemodynamics in middle-aged and elderly patients undergoing general anesthesia. BMC Anesthesiol. 2024;24(1):312. [PubMed] DOI: 1186/s12871-024-02700-9