Muhammad Winardi Setia Lesmana 1 , Sri Rahardjo 2 , Iwan Faudi 3 , Iwan Abdul Rahman 4
Authors affiliations:
Introduction: Traumatic cervical spinal cord injury (SCI) is often complicated by neurogenic hypotension, which exacerbates secondary injury. This case is unique due to a 10-hour delayed presentation without prehospital care, successful use of dual vasopressors (norepinephrine + dopamine) in a resource-limited setting, and neurological stabilization despite initial MAP of 54 mmHg. Guidelines recommend maintaining MAP >85 mmHg for 7 days.
Case Description: This report describes a 57-year-old male presented 10 hours after a collapsing structure injury with ASIA Impairment Scale C tetraparesis, complete lower limb paralysis, absent sacral sparing, and MAP 54 mmHg. Haemodynamic support with norepinephrine (0.02 mcg/kg/min) and dopamine (1 mcg/kg/min) elevated MAP to >85 mmHg. Diagnostic magnetic resonance imaging (MRI) revealed disc protrusions at C3-6 with spinal cord edema. The patient underwent elective Anterior Cervical Discectomy and Fusion (ACDF) under neuroanesthesia, with induction using fentanyl, propofol, and rocuronium. Intraoperative stability was maintained (MAP 87–90 mmHg), and postoperative care included vasopressor tapering by day 3, with a stable ASIA scale C and no further neurological worsening.
Conclusion: This case emphasizes the critical role of early aggressive hypotension management in SCI to preserve neurological functions. Targeting MAP >85 mmHg using vasoactive agents and surgical intervention prevents secondary injury, highlighting a multidisciplinary approach for optimal outcomes in traumatic cervical SCI.
Keywords: Hypotension, traumatic spinal cord injury, tetraplegia, perioperative management, neurogenic shock
Citation: Lesmana MWS, Rahardjo S, Faudi I, Rahman IA. Perioperative management of hypotension in traumatic cervical spinal cord injury: a case study and clinical insights. Anaesth. pain intensive care 2025;30(1):114-119. DOI: 10.35975/apic.v30i1.3089
Received: November 10, 2025; Revised: December 10, 2024; Accepted: December 16, 2025
Traumatic spinal cord injury (SCI) is a devastating condition with significant morbidity and mortality, often resulting from high-impact incidents such as motor vehicle accidents, falls, or acts of violence. The global prevalence of SCI varies, with an estimated incidence of 4.3% for cervical injuries, 6.3% for thoracolumbar injuries, and 1.3% for injuries directly affecting the spinal cord itself.1 Owing to their high mobility, cervical spine injuries are particularly prone to severe neurological deficits, including motor and sensory impairments, and can lead to life-threatening complications.2 According to the National Spinal Cord Injury Statistical Center, approximately 296,000 individuals in the United States live with SCI, with 17,900 new cases reported annually, predominantly affecting males aged 29–43 years.3 Cervical injuries account for 55% of SCI cases, with incomplete tetraplegia being the most common (46%).3
The pathophysiology of traumatic SCI involves both the primary and secondary mechanisms. Primary injury results from initial mechanical trauma, while secondary injuries, including ischemia, edema, and inflammation, exacerbate neurological damage.4 One critical complication of acute cervical SCI is neurogenic hypotension caused by sympathetic denervation, which leads to bradycardia, peripheral vasodilation, and reduced systemic vascular resistance.5 If not managed promptly, this condition can precipitate neurogenic shock and worsen spinal cord perfusion, significantly contributing to secondary injury.6 The mortality rate in the acute phase of SCI can reach 50%, with only a 10% likelihood of full neurological recovery.2,7
Effective perioperative management is crucial to stabilize hemodynamics, prevent secondary neurological injuries, and optimize patient outcomes. Hypotension, in particular, requires aggressive intervention with vasoactive agents to maintain adequate spinal cord perfusion, typically targeting a mean arterial pressure (MAP) above 85 mmHg.8 Additionally, surgical interventions such as Anterior Cervical Discectomy and Fusion (ACDF) are often employed to decompress neural structures and correct spinal deformities.9 This case study discusses the perioperative management of a 57-year-old male with traumatic cervical SCI presenting with neurogenic hypotension, highlighting the importance of early and aggressive hemodynamic stabilization to prevent further neurological deterioration.
This case is scientifically notable for three reasons: (1) delayed presentation (10 hours post-injury) without prehospital cervical immobilization or medical support, uncommon in high-resource settings; (2) Successful use of combined norepinephrine and dopamine to achieve rapid MAP correction when phenylephrine was unavailable, challenging guideline preference for norepinephrine monotherapy; (3) Perioperative neuroanesthetic management in a conscious (GCS 15), hemodynamically labile patient in a resource-limited hospital, highlighting real-world clinical challenges.
A 57-year-old male, weighing 60 kg, no known past medical illness, chronic medications, smoking, alcohol use, prior spinal surgery, or family history of neurological or spinal disease, presented to the emergency department with weakness in all four limbs following a traumatic incident. Approximately 10 h prior to admission, the patient sustained a neck injury when a collapsing structure struck his head, causing him to fall and impact the ground with his head and neck. He reported immediate weakness in all extremities, neck pain, and numbness radiating from the forearm to both feet. Additionally, he experienced difficulty in controlling bowel and bladder function. There had no history of loss of consciousness, vomiting, seizures, or bleeding from the ears, nose, or mouth. The patient arrived at the hospital via a private vehicle without medical assistance and was diagnosed with a suspected traumatic cervical SCI.
2.1. Clinical Assessment
The respiratory rate was 22 breaths per minute, with thoracoabdominal breathing, vesicular breath sounds, and no adventitious sounds. Oxygen saturation was 97% on room air, which improved to 99% with nasal cannula oxygen at 3 L/min. Peripheral pulses were palpable, with warm, dry extremities, and a capillary refill time of less than 2 s. The initial blood pressure was 72/46 mmHg (mean arterial pressure [MAP], 54 mmHg) with a heart rate of 65 beats per minute (regular). Intravenous access was established with a 0.9% NaCl bolus of 1000 mL, followed by a maintenance infusion at 100 mL/h, resulting in a blood pressure of 85/67 mmHg (MAP 73 mmHg). Due to persistent hypotension, norepinephrine (0.02 mcg/kg/min) and dopamine (1 mcg/kg/min) were initiated, achieving a blood pressure of 113/68 mmHg (MAP 84 mmHg). The patient was fully conscious with a Glasgow Coma Scale (GCS) score of 15 (E4M6V5), bilateral pupils of 3 mm with intact light reflexes, and no cranial nerve deficits. A 4 × 2 x 0.5 cm laceration above the right supraorbital region was noted and dressed with gauze. Log-roll examination revealed no additional injuries to the posterior body.
A secondary survey confirmed stable respiratory and hemodynamic parameters. Neurological examination revealed a motor strength of 2-3/5 in the upper extremities (right/left: 22333/32222) and 0/5 in the lower extremities (00000/00000). Sensory examination revealed hypoesthesia below the C5 level, absence of perianal sensation, absence of voluntary anal contraction, and absence of toe flexion. The proprioceptive sensation was impaired, and physiological reflexes were absent. The American Spinal Injury Association (ASIA) Impairment Scale was graded as C.10]. The patient reported an inability to sense urination, and a urinary catheter was inserted, which yielded 200 mL of clear yellow urine. The abdomen was soft with normal peristalsis; however, the patient experienced fecal incontinence.
2.2. Imaging / Laboratory Findings
Cervical spine X-ray showed no fracture or malalignment. Magnetic resonance imaging (MRI) revealed multilevel disc protrusions at C3–4, C4–5, and C5–6 with associated spinal cord edema and T2 hyperintensity at C4–6 (Figure 1). Preoperative laboratory results were within normal limits, including hemoglobin 13.8 g/dL, sodium 138 mmol/L, and creatinine 0.9 mg/dL, ruling out anemia or electrolyte imbalance as contributors to hypotension.
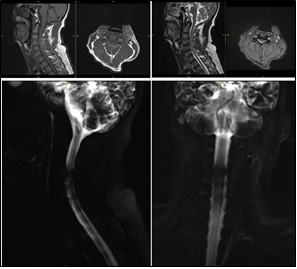
Figure 1: Sagittal T2-weighted MRI showing disc protrusions at C3-4, C4-5, and C5-6 with spinal cord edema.
2.3. Differential Diagnosis of Hypotension
Hemorrhagic shock was excluded due to warm extremities, capillary refill <2 seconds, and absence of external bleeding. Cardiogenic shock was unlikely given normal heart rate and no cardiac risk factors. Sepsis was ruled out by the absence of fever and normal white cell count. Neurogenic shock was confirmed by the combination of bradycardia, vasodilation, and cervical spinal cord injury level.
The 10-hour delay in presentation, self-transport without cervical immobilization, and limited access to computed tomography posed significant challenges; MRI was performed despite movement risk. The patient was classified as ASIA Impairment Scale C with absent sacral sparing, indicating incomplete injury but a poorer prognosis for ambulation (estimated 40–60% chance) and high risk of permanent bladder/bowel dysfunction.
2.4. Management
The patient was admitted to the high care unit (HCU) with stable respiratory parameters (respiratory rate 18 breaths/min, SpO2 99% on nasal cannula) and hemodynamics (blood pressure 123/63 mmHg, MAP 83 mmHg, supported by norepinephrine 0.02 mcg/kg/min and dopamine 1 mcg/kg/min; heart rate 85 beats/min). Treatment included a soft diet, paracetamol 1 g every 6 hours, omeprazole 20 mg twice daily, ceftriaxone 1 g twice daily, methylprednisolone 125 mg every 8 hours, and inline positioning.The patient underwent elective Anterior Cervical Discectomy and Fusion (ACDF) after preoperative fasting for 6–8 hours. In the operating room, the patient was positioned supine, with a neutral neck. Induction was performed with 125 mcg, propofol 100 mg (titrated), and rocuronium 50 mg intravenously. Video laryngoscopy facilitated intubation using a non-kinking endotracheal tube (size, 7.5; depth, 20 cm). An arterial line and central venous catheter (subclavian vein) were placed. Ventilation was set to volume-controlled mode (tidal volume 450 mL, respiratory rate 12 breaths/min, PEEP 5 cmH2O, FiO2 50%). Anesthesia was maintained with sevoflurane (1–2%), dexmedetomidine (0.3–0.5 mcg/kg/hour), and intermittent rocuronium. The procedure lasted 3 hours with stable hemodynamics (systolic blood pressure, 97–124 mmHg; diastolic blood pressure, 58–91 mmHg; heart rate, 61–73 beats/min, SpO2 98–99%). The intraoperative blood loss was approximately 50 mL, urine output was 200 mL, and fluid input included 1500 mL of Ringer’s lactate. Dopamine was titrated to 2–5 mcg/kg/min intraoperatively.
The patient was extubated after the procedure and transferred to the intensive care unit (ICU) with inline positioning. Spontaneous respiration was maintained (respiratory rate 16 breaths/min, SpO2 98% on a nasal cannula, 3 L/min). Blood pressure was 127/72 mmHg (MAP 90.3 mmHg) with norepinephrine (0.01 mcg/kg/min) and dopamine (1 mcg/kg/hour), and heart rate was 62 beats/min. The patient remained fully conscious (GCS E4MxV5). Postoperative therapy included fentanyl (25 µg/h), paracetamol (1 g every 6 h), Ringer’s lactate (75 mL/h), and omeprazole (40 mg every 12 h). On postoperative day 3, neurological assessment confirmed ASIA scale C, vasopressors were tapered, and the patient was transferred to the semi-intensive care unit.
Traumatic cervical spinal cord injury (SCI) is a complex clinical entity that is associated with significant neurological and systemic complications. This case highlights the critical interplay between neurogenic hypotension and perioperative management in a 57-year-old male with ASIA Impairment Scale C injury secondary to a suspected C7 burst fracture. The primary goals of managing acute traumatic SCI include preventing secondary neurological injury, optimizing existing neurological deficits, achieving neural decompression, and correcting spinal deformities through surgical intervention.1,11 This case underscores the importance of early and aggressive hemodynamic stabilization to mitigate secondary spinal cord injury, particularly neurogenic hypotension.
Neurogenic hypotension, a hallmark of acute cervical SCI, results from sympathetic denervation, leading to bradycardia, peripheral vasodilation, and reduced systemic vascular resistance.5 These physiological changes can precipitate neurogenic shock, characterized by inadequate spinal cord perfusion, which exacerbates secondary injury mechanisms such as ischemia and edema.6,12 In the present case, the patient’s initial blood pressure of 72/46 mmHg (MAP, 54 mmHg) indicated significant hemodynamic instability, necessitating immediate fluid resuscitation and vasoactive support with norepinephrine and dopamine to achieve a target MAP above 85 mmHg. This aligns with the current guidelines recommending maintenance of MAP between 85 and 90 mmHg in the acute phase of SCI to ensure adequate spinal cord perfusion and minimize secondary injury.8,13 The successful stabilization of the patient’s hemodynamics, both pre- and intraoperatively, likely contributed to the prevention of further neurological deterioration, as evidenced by the stable postoperative ASIA scale C status.
Surgical intervention and Anterior Cervical Discectomy and Fusion (ACDF) were performed to address disc protrusions at C3-4, C4-5, and C5-6, as well as spinal cord edema identified on MRI. ACDF is a well-established procedure for decompressing neural structures and stabilizing the cervical spine in traumatic SCI.9 In this case, the procedure was conducted under careful neuroanesthetic management to avoid exacerbating hypotension during induction and intubation, which could further compromise spinal cord perfusion.14 The use of video laryngoscopy and inline stabilization during intubation minimized the risk of additional cervical spine injury, whereas intraoperative monitoring ensured stable hemodynamics (systolic blood pressure, 97–124 mmHg; MAP, 87–90.3 mmHg). These measures reflect the importance of a multidisciplinary approach involving neurosurgery and anesthesiology to optimize outcomes in traumatic SCI.15
The postoperative management in this case focused on continued hemodynamic support and neurological monitoring. The tapering of vasopressors by postoperative day 3 and the patient’s transfer to a semi-intensive care unit suggested a favorable early response to treatment. However, the persistent ASIA scale C status indicates that significant neurological recovery remains challenging, consistent with the literature reporting only a 10% likelihood of full neurological recovery in acute SCI.7 The absence of perianal sensation, voluntary anal contraction, and lower extremity motor function underscores the severity of the injury and the importance of early intervention to prevent further deterioration.10 The use of methylprednisolone in this case, although controversial, was likely aimed at reducing spinal cord edema, although its efficacy in improving neurological outcomes remains debated.16
Promising neuroprotective strategies include riluzole (sodium-glutamate blocker, shown to improve ASIA scores in phase III trials), therapeutic hypothermia (33–35°C for 48 hours to reduce inflammation), and granulocyte colony-stimulating factor (G-CSF) for anti-apoptotic effects. Refining vasopressor protocols — such as norepinephrine vs. phenylephrine vs. vasopressin — in randomized trials could further optimize spinal cord perfusion while minimizing cardiac side effects.
This case report provides several clinical insights. First, prompt recognition and management of neurogenic hypotension is critical for preventing secondary spinal cord injury. Second, meticulous perioperative care, including targeted MAP goals and careful anesthetic techniques, is essential for optimizing the surgical outcomes. Third, the integration of imaging (e.g., MRI) and clinical assessment (e.g., the ASIA scale) is vital for guiding treatment decisions in traumatic SCI. Future research should focus on refining vasopressor protocols and exploring neuroprotective strategies to enhance neurological recovery in similar cases.6,17
For ASIA C cervical SCI without sacral sparing, long-term prognosis includes 40–60% chance of independent ambulation with intensive rehabilitation. Most patients require lifelong intermittent catheterization and bowel management programs. Expected rehabilitation pathway: acute inpatient rehab (3–6 months), followed by outpatient physical/occupational therapy. Psychological support is critical due to high risk of depression. The limitations of this case report include its single-patient focus, which precludes generalizability, and lack of long-term follow-up data to assess functional outcomes.
4. CONCLUSION
Perioperative management of neurogenic hypotension in traumatic cervical spinal cord injury, as illustrated in the case of a 57-year-old male undergoing ACDF, underscores the critical need for early and aggressive hemodynamic stabilization to prevent secondary neurological deterioration. Maintaining a target mean arterial pressure above 85 mmHg through fluid resuscitation and vasoactive agents, such as norepinephrine and dopamine, effectively preserved spinal cord perfusion, resulting in stable postoperative neurological status (ASIA scale C) and avoidance of further complications. This case highlights the importance of a multidisciplinary approach, integrating prompt vasopressor therapy, careful neuroanesthetic techniques, and surgical decompression to optimize outcomes, emphasizing that timely intervention can significantly mitigate the risk of irreversible deficits and improve the quality of life in patients with SCI.
5. Conflict of interest
All authors declare that there was no conflict of interest.
6. Ethical considerations
Written permission od the patient was obtained from the patient to use the data for academic purposes.The study utilized the hospital resources only, and no external or industry funding was involved.
7. Authors’ contribution
MWSL: Conception and design. provision of study materials or patients.
SR, IF, IAR: Conception and design, administrative support.
Authors affiliations:
- Muhammad Winardi Setia Lesmana, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia; Email: mwinardisl@gmail.com
- Sri Rahardjo, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia; Email: m84972998@gmail.com
- Iwan Faudi, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia; Email: jhonclark.prima@gmail.com
- Iwan Abdul Rahman, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin Hospital, Bandung, Indonesia; Email: : paulawhiteanes@gmail.com
ABSTRACT
Introduction: Traumatic cervical spinal cord injury (SCI) is often complicated by neurogenic hypotension, which exacerbates secondary injury. This case is unique due to a 10-hour delayed presentation without prehospital care, successful use of dual vasopressors (norepinephrine + dopamine) in a resource-limited setting, and neurological stabilization despite initial MAP of 54 mmHg. Guidelines recommend maintaining MAP >85 mmHg for 7 days.
Case Description: This report describes a 57-year-old male presented 10 hours after a collapsing structure injury with ASIA Impairment Scale C tetraparesis, complete lower limb paralysis, absent sacral sparing, and MAP 54 mmHg. Haemodynamic support with norepinephrine (0.02 mcg/kg/min) and dopamine (1 mcg/kg/min) elevated MAP to >85 mmHg. Diagnostic magnetic resonance imaging (MRI) revealed disc protrusions at C3-6 with spinal cord edema. The patient underwent elective Anterior Cervical Discectomy and Fusion (ACDF) under neuroanesthesia, with induction using fentanyl, propofol, and rocuronium. Intraoperative stability was maintained (MAP 87–90 mmHg), and postoperative care included vasopressor tapering by day 3, with a stable ASIA scale C and no further neurological worsening.
Conclusion: This case emphasizes the critical role of early aggressive hypotension management in SCI to preserve neurological functions. Targeting MAP >85 mmHg using vasoactive agents and surgical intervention prevents secondary injury, highlighting a multidisciplinary approach for optimal outcomes in traumatic cervical SCI.
Keywords: Hypotension, traumatic spinal cord injury, tetraplegia, perioperative management, neurogenic shock
Citation: Lesmana MWS, Rahardjo S, Faudi I, Rahman IA. Perioperative management of hypotension in traumatic cervical spinal cord injury: a case study and clinical insights. Anaesth. pain intensive care 2025;30(1):114-119. DOI: 10.35975/apic.v30i1.3089
Received: November 10, 2025; Revised: December 10, 2024; Accepted: December 16, 2025
1. INTRODUCTION
Traumatic spinal cord injury (SCI) is a devastating condition with significant morbidity and mortality, often resulting from high-impact incidents such as motor vehicle accidents, falls, or acts of violence. The global prevalence of SCI varies, with an estimated incidence of 4.3% for cervical injuries, 6.3% for thoracolumbar injuries, and 1.3% for injuries directly affecting the spinal cord itself.1 Owing to their high mobility, cervical spine injuries are particularly prone to severe neurological deficits, including motor and sensory impairments, and can lead to life-threatening complications.2 According to the National Spinal Cord Injury Statistical Center, approximately 296,000 individuals in the United States live with SCI, with 17,900 new cases reported annually, predominantly affecting males aged 29–43 years.3 Cervical injuries account for 55% of SCI cases, with incomplete tetraplegia being the most common (46%).3
The pathophysiology of traumatic SCI involves both the primary and secondary mechanisms. Primary injury results from initial mechanical trauma, while secondary injuries, including ischemia, edema, and inflammation, exacerbate neurological damage.4 One critical complication of acute cervical SCI is neurogenic hypotension caused by sympathetic denervation, which leads to bradycardia, peripheral vasodilation, and reduced systemic vascular resistance.5 If not managed promptly, this condition can precipitate neurogenic shock and worsen spinal cord perfusion, significantly contributing to secondary injury.6 The mortality rate in the acute phase of SCI can reach 50%, with only a 10% likelihood of full neurological recovery.2,7
Effective perioperative management is crucial to stabilize hemodynamics, prevent secondary neurological injuries, and optimize patient outcomes. Hypotension, in particular, requires aggressive intervention with vasoactive agents to maintain adequate spinal cord perfusion, typically targeting a mean arterial pressure (MAP) above 85 mmHg.8 Additionally, surgical interventions such as Anterior Cervical Discectomy and Fusion (ACDF) are often employed to decompress neural structures and correct spinal deformities.9 This case study discusses the perioperative management of a 57-year-old male with traumatic cervical SCI presenting with neurogenic hypotension, highlighting the importance of early and aggressive hemodynamic stabilization to prevent further neurological deterioration.
This case is scientifically notable for three reasons: (1) delayed presentation (10 hours post-injury) without prehospital cervical immobilization or medical support, uncommon in high-resource settings; (2) Successful use of combined norepinephrine and dopamine to achieve rapid MAP correction when phenylephrine was unavailable, challenging guideline preference for norepinephrine monotherapy; (3) Perioperative neuroanesthetic management in a conscious (GCS 15), hemodynamically labile patient in a resource-limited hospital, highlighting real-world clinical challenges.
2. CASE REPORT
A 57-year-old male, weighing 60 kg, no known past medical illness, chronic medications, smoking, alcohol use, prior spinal surgery, or family history of neurological or spinal disease, presented to the emergency department with weakness in all four limbs following a traumatic incident. Approximately 10 h prior to admission, the patient sustained a neck injury when a collapsing structure struck his head, causing him to fall and impact the ground with his head and neck. He reported immediate weakness in all extremities, neck pain, and numbness radiating from the forearm to both feet. Additionally, he experienced difficulty in controlling bowel and bladder function. There had no history of loss of consciousness, vomiting, seizures, or bleeding from the ears, nose, or mouth. The patient arrived at the hospital via a private vehicle without medical assistance and was diagnosed with a suspected traumatic cervical SCI.
2.1. Clinical Assessment
The respiratory rate was 22 breaths per minute, with thoracoabdominal breathing, vesicular breath sounds, and no adventitious sounds. Oxygen saturation was 97% on room air, which improved to 99% with nasal cannula oxygen at 3 L/min. Peripheral pulses were palpable, with warm, dry extremities, and a capillary refill time of less than 2 s. The initial blood pressure was 72/46 mmHg (mean arterial pressure [MAP], 54 mmHg) with a heart rate of 65 beats per minute (regular). Intravenous access was established with a 0.9% NaCl bolus of 1000 mL, followed by a maintenance infusion at 100 mL/h, resulting in a blood pressure of 85/67 mmHg (MAP 73 mmHg). Due to persistent hypotension, norepinephrine (0.02 mcg/kg/min) and dopamine (1 mcg/kg/min) were initiated, achieving a blood pressure of 113/68 mmHg (MAP 84 mmHg). The patient was fully conscious with a Glasgow Coma Scale (GCS) score of 15 (E4M6V5), bilateral pupils of 3 mm with intact light reflexes, and no cranial nerve deficits. A 4 × 2 x 0.5 cm laceration above the right supraorbital region was noted and dressed with gauze. Log-roll examination revealed no additional injuries to the posterior body.
A secondary survey confirmed stable respiratory and hemodynamic parameters. Neurological examination revealed a motor strength of 2-3/5 in the upper extremities (right/left: 22333/32222) and 0/5 in the lower extremities (00000/00000). Sensory examination revealed hypoesthesia below the C5 level, absence of perianal sensation, absence of voluntary anal contraction, and absence of toe flexion. The proprioceptive sensation was impaired, and physiological reflexes were absent. The American Spinal Injury Association (ASIA) Impairment Scale was graded as C.10]. The patient reported an inability to sense urination, and a urinary catheter was inserted, which yielded 200 mL of clear yellow urine. The abdomen was soft with normal peristalsis; however, the patient experienced fecal incontinence.
2.2. Imaging / Laboratory Findings
Cervical spine X-ray showed no fracture or malalignment. Magnetic resonance imaging (MRI) revealed multilevel disc protrusions at C3–4, C4–5, and C5–6 with associated spinal cord edema and T2 hyperintensity at C4–6 (Figure 1). Preoperative laboratory results were within normal limits, including hemoglobin 13.8 g/dL, sodium 138 mmol/L, and creatinine 0.9 mg/dL, ruling out anemia or electrolyte imbalance as contributors to hypotension.
Figure 1: Sagittal T2-weighted MRI showing disc protrusions at C3-4, C4-5, and C5-6 with spinal cord edema.
2.3. Differential Diagnosis of Hypotension
Hemorrhagic shock was excluded due to warm extremities, capillary refill <2 seconds, and absence of external bleeding. Cardiogenic shock was unlikely given normal heart rate and no cardiac risk factors. Sepsis was ruled out by the absence of fever and normal white cell count. Neurogenic shock was confirmed by the combination of bradycardia, vasodilation, and cervical spinal cord injury level.
The 10-hour delay in presentation, self-transport without cervical immobilization, and limited access to computed tomography posed significant challenges; MRI was performed despite movement risk. The patient was classified as ASIA Impairment Scale C with absent sacral sparing, indicating incomplete injury but a poorer prognosis for ambulation (estimated 40–60% chance) and high risk of permanent bladder/bowel dysfunction.
| Table 1: Preoperative laboratory results | |
| Parameter | Result |
| Hemoglobin, g/dL | 15.0 |
| Hematocrit, % | 42.5 |
| Leukocytes, /mm³ | 14,100 |
| Platelets, /mm³ | 202,000 |
| Sodium, mEq/L | 140 |
| Potassium, mEq/L | 3.3 |
| Chloride, mEq/L | 106 |
| Blood Glucose, mg/dL | 141 |
| Urea, mg/dL | 17 |
| Creatinine, mg/dL | 0.94 |
| Prothrombin Time, seconds | 13.3 |
| INR | 0.91 |
| APTT (Activated Partial Thromboplastin Time), seconds | 42.0 |
| SGOT (AST), U/L | 53 |
| SGPT (ALT), U/L | 40 |
2.4. Management
The patient was admitted to the high care unit (HCU) with stable respiratory parameters (respiratory rate 18 breaths/min, SpO2 99% on nasal cannula) and hemodynamics (blood pressure 123/63 mmHg, MAP 83 mmHg, supported by norepinephrine 0.02 mcg/kg/min and dopamine 1 mcg/kg/min; heart rate 85 beats/min). Treatment included a soft diet, paracetamol 1 g every 6 hours, omeprazole 20 mg twice daily, ceftriaxone 1 g twice daily, methylprednisolone 125 mg every 8 hours, and inline positioning.The patient underwent elective Anterior Cervical Discectomy and Fusion (ACDF) after preoperative fasting for 6–8 hours. In the operating room, the patient was positioned supine, with a neutral neck. Induction was performed with 125 mcg, propofol 100 mg (titrated), and rocuronium 50 mg intravenously. Video laryngoscopy facilitated intubation using a non-kinking endotracheal tube (size, 7.5; depth, 20 cm). An arterial line and central venous catheter (subclavian vein) were placed. Ventilation was set to volume-controlled mode (tidal volume 450 mL, respiratory rate 12 breaths/min, PEEP 5 cmH2O, FiO2 50%). Anesthesia was maintained with sevoflurane (1–2%), dexmedetomidine (0.3–0.5 mcg/kg/hour), and intermittent rocuronium. The procedure lasted 3 hours with stable hemodynamics (systolic blood pressure, 97–124 mmHg; diastolic blood pressure, 58–91 mmHg; heart rate, 61–73 beats/min, SpO2 98–99%). The intraoperative blood loss was approximately 50 mL, urine output was 200 mL, and fluid input included 1500 mL of Ringer’s lactate. Dopamine was titrated to 2–5 mcg/kg/min intraoperatively.
The patient was extubated after the procedure and transferred to the intensive care unit (ICU) with inline positioning. Spontaneous respiration was maintained (respiratory rate 16 breaths/min, SpO2 98% on a nasal cannula, 3 L/min). Blood pressure was 127/72 mmHg (MAP 90.3 mmHg) with norepinephrine (0.01 mcg/kg/min) and dopamine (1 mcg/kg/hour), and heart rate was 62 beats/min. The patient remained fully conscious (GCS E4MxV5). Postoperative therapy included fentanyl (25 µg/h), paracetamol (1 g every 6 h), Ringer’s lactate (75 mL/h), and omeprazole (40 mg every 12 h). On postoperative day 3, neurological assessment confirmed ASIA scale C, vasopressors were tapered, and the patient was transferred to the semi-intensive care unit.
3. DISCUSSION
Traumatic cervical spinal cord injury (SCI) is a complex clinical entity that is associated with significant neurological and systemic complications. This case highlights the critical interplay between neurogenic hypotension and perioperative management in a 57-year-old male with ASIA Impairment Scale C injury secondary to a suspected C7 burst fracture. The primary goals of managing acute traumatic SCI include preventing secondary neurological injury, optimizing existing neurological deficits, achieving neural decompression, and correcting spinal deformities through surgical intervention.1,11 This case underscores the importance of early and aggressive hemodynamic stabilization to mitigate secondary spinal cord injury, particularly neurogenic hypotension.
Neurogenic hypotension, a hallmark of acute cervical SCI, results from sympathetic denervation, leading to bradycardia, peripheral vasodilation, and reduced systemic vascular resistance.5 These physiological changes can precipitate neurogenic shock, characterized by inadequate spinal cord perfusion, which exacerbates secondary injury mechanisms such as ischemia and edema.6,12 In the present case, the patient’s initial blood pressure of 72/46 mmHg (MAP, 54 mmHg) indicated significant hemodynamic instability, necessitating immediate fluid resuscitation and vasoactive support with norepinephrine and dopamine to achieve a target MAP above 85 mmHg. This aligns with the current guidelines recommending maintenance of MAP between 85 and 90 mmHg in the acute phase of SCI to ensure adequate spinal cord perfusion and minimize secondary injury.8,13 The successful stabilization of the patient’s hemodynamics, both pre- and intraoperatively, likely contributed to the prevention of further neurological deterioration, as evidenced by the stable postoperative ASIA scale C status.
Surgical intervention and Anterior Cervical Discectomy and Fusion (ACDF) were performed to address disc protrusions at C3-4, C4-5, and C5-6, as well as spinal cord edema identified on MRI. ACDF is a well-established procedure for decompressing neural structures and stabilizing the cervical spine in traumatic SCI.9 In this case, the procedure was conducted under careful neuroanesthetic management to avoid exacerbating hypotension during induction and intubation, which could further compromise spinal cord perfusion.14 The use of video laryngoscopy and inline stabilization during intubation minimized the risk of additional cervical spine injury, whereas intraoperative monitoring ensured stable hemodynamics (systolic blood pressure, 97–124 mmHg; MAP, 87–90.3 mmHg). These measures reflect the importance of a multidisciplinary approach involving neurosurgery and anesthesiology to optimize outcomes in traumatic SCI.15
The postoperative management in this case focused on continued hemodynamic support and neurological monitoring. The tapering of vasopressors by postoperative day 3 and the patient’s transfer to a semi-intensive care unit suggested a favorable early response to treatment. However, the persistent ASIA scale C status indicates that significant neurological recovery remains challenging, consistent with the literature reporting only a 10% likelihood of full neurological recovery in acute SCI.7 The absence of perianal sensation, voluntary anal contraction, and lower extremity motor function underscores the severity of the injury and the importance of early intervention to prevent further deterioration.10 The use of methylprednisolone in this case, although controversial, was likely aimed at reducing spinal cord edema, although its efficacy in improving neurological outcomes remains debated.16
Promising neuroprotective strategies include riluzole (sodium-glutamate blocker, shown to improve ASIA scores in phase III trials), therapeutic hypothermia (33–35°C for 48 hours to reduce inflammation), and granulocyte colony-stimulating factor (G-CSF) for anti-apoptotic effects. Refining vasopressor protocols — such as norepinephrine vs. phenylephrine vs. vasopressin — in randomized trials could further optimize spinal cord perfusion while minimizing cardiac side effects.
This case report provides several clinical insights. First, prompt recognition and management of neurogenic hypotension is critical for preventing secondary spinal cord injury. Second, meticulous perioperative care, including targeted MAP goals and careful anesthetic techniques, is essential for optimizing the surgical outcomes. Third, the integration of imaging (e.g., MRI) and clinical assessment (e.g., the ASIA scale) is vital for guiding treatment decisions in traumatic SCI. Future research should focus on refining vasopressor protocols and exploring neuroprotective strategies to enhance neurological recovery in similar cases.6,17
For ASIA C cervical SCI without sacral sparing, long-term prognosis includes 40–60% chance of independent ambulation with intensive rehabilitation. Most patients require lifelong intermittent catheterization and bowel management programs. Expected rehabilitation pathway: acute inpatient rehab (3–6 months), followed by outpatient physical/occupational therapy. Psychological support is critical due to high risk of depression. The limitations of this case report include its single-patient focus, which precludes generalizability, and lack of long-term follow-up data to assess functional outcomes.
4. CONCLUSION
Perioperative management of neurogenic hypotension in traumatic cervical spinal cord injury, as illustrated in the case of a 57-year-old male undergoing ACDF, underscores the critical need for early and aggressive hemodynamic stabilization to prevent secondary neurological deterioration. Maintaining a target mean arterial pressure above 85 mmHg through fluid resuscitation and vasoactive agents, such as norepinephrine and dopamine, effectively preserved spinal cord perfusion, resulting in stable postoperative neurological status (ASIA scale C) and avoidance of further complications. This case highlights the importance of a multidisciplinary approach, integrating prompt vasopressor therapy, careful neuroanesthetic techniques, and surgical decompression to optimize outcomes, emphasizing that timely intervention can significantly mitigate the risk of irreversible deficits and improve the quality of life in patients with SCI.
5. Conflict of interest
All authors declare that there was no conflict of interest.
6. Ethical considerations
Written permission od the patient was obtained from the patient to use the data for academic purposes.The study utilized the hospital resources only, and no external or industry funding was involved.
7. Authors’ contribution
MWSL: Conception and design. provision of study materials or patients.
SR, IF, IAR: Conception and design, administrative support.
8.REFERENCES
- Lindsay RW, Gugala Z, Pneumaticos SG. Injury to the vertebra and spinal cord. In: Moore EE, Feliciano DV, Mattox KL, eds. Trauma. 5th ed. New York: McGraw-Hill; 2014:459-492.
- Dutton RP, McCunn M, Grissom TE. Anesthesia for trauma. In: Miller RD, ed. Miller’s Anesthesia. 7th ed. Philadelphia: Churchill Livingstone; 2010:2277-2311.
- Cottrell JE, Patel P, eds. Cottrell and Patel’s Neuroanesthesia. 7th ed. Philadelphia: Elsevier Health Sciences; 2023.
- Dinata IGS, Yasa AAGWP. The overview of spinal cord injury. Ganesha Med. 2021;1(2):103-113.
- Hines RL, Jones SB, eds. Stoelting’s Anesthesia and Co-Existing Disease. 8th ed. Philadelphia: Elsevier Health Sciences; 2021.
- Bosmia AN, Hogan E, Loukas M, Tubbs RS, Cohen-Gadol AA. Blood supply to the human spinal cord: Part I. Anatomy and hemodynamics. Clin Anat. 2015;28(1):52-64. doi:10.1002/ca.22281.
- Amato ACM, Stolf NAG. Anatomia da circulação medular. J Vasc Bras. 2015;14(3):248-252.
- Hurlbert RJ, Hadley MN, Walters BC, Aarabi B, Dhall SS, Gelb DE, Rozzelle CJ, et al. Pharmacological therapy for acute spinal cord injury. Neurosurgery. 2013;72(Suppl 2):93-105.
- Bracken MB. Steroids for acute spinal cord injury. Cochrane Database Syst Rev. 2012;1:CD001046.
- Tee JW, Altaf F, Belanger L. Mean arterial blood pressure management of acute traumatic spinal cord injured patients during the pre-hospital and early admission period. J Neurotrauma. 2017;34(6):1271-1277.
- Saadoun S, Chen S, Papadopoulos MC. Intraspinal pressure and spinal cord perfusion pressure predict neurological outcome after traumatic spinal cord injury. J Neurol Neurosurg Psychiatry. 2017;88(5):452-453.
- Saadeh YS, Smith BW, Joseph JR. The impact of blood pressure management after spinal cord injury: a systematic review of the literature. Neurosurg Focus. 2017;43(5):E20.
- Wang TY, Park C, Zhang H. Management of acute traumatic spinal cord injury: a review of the literature. Front Surg. 2021; 8:698736. doi:10.3389/fsurg.2021.698736.
- Savic G, DeVivo MJ, Frankel HL, Jamous MA, Soni BM, Charlifue S. Causes of death after traumatic spinal cord injury: a 70-year British study. Spinal Cord. 2017;55(10):891-897.
- Schilero GJ, Bauman WA, Radulovic M. Traumatic spinal cord injury. Clin Chest Med. 2018;39(2):411-425.
- Evans LT, Lollis SS, Ball PA. Management of acute spinal cord injury in the neurocritical care unit. Neurosurg Clin N Am. 2013;24(3):339-347.
- Copuroglu C, Sahin SH, Ciftdemir M, Elif C. Anesthesia management in spinal cord injury patients. J Turk Spinal Surg. 2015;26(2):173-176.