Poppy Novita Rini 1 , Muhammad Syifa Irvandy 2 , Tifani Antonia Pradhea 3
Authors affiliations;
Background. Congenital Insensitivity to Pain and Anhidrosis (CIPA) is a rare hereditary sensory and autonomic neuropathy type IV (HSAN IV) caused by NTRK1 gene mutations. It disrupts pain and temperature regulation, leading to anhidrosis, recurrent fever, self-injury, and, in severe cases, intellectual disability. The absence of pain perception increases the risk of unnoticed injuries and long-term complications. Understanding these complications is essential to improving patient care and quality of life.
Methodology: A systematic search on PubMed, ScienceDirect, and ProQuest was conducted on October 30, 2024, using keywords related to CIPA and HSAN IV. This review included English-language clinical studies and case reports (2014–2024) reporting complications of CIPA. Reviews, books, inaccessible articles, and duplicates were excluded. A total of 29 case reports were analyzed, with quality assessed using JBI Critical Appraisal Tools.
Result. A total of 29 articles met the inclusion criteria, reporting complications among patients with CIPA. The most frequently observed complications were fever (87%), self-mutilation (73%), and recurrent fractures (68%), while developmental delay (63%) represented a major neurodevelopmental manifestation. The mean age of patients was 10.9 years, ranging from 1 to 38 years. Most reported cases originated from China (41%).
Conclusion. This review emphasizes the importance of early diagnosis in CIPA patients to prevent complications. However, current studies often lack comprehensive follow-up, which hinders our understanding of long-term outcomes. Further research is needed to fill these gaps and improve the quality of life for patients with this rare condition.
Abbreviations: CIPA: Congenital Insensitivity to Pain and Anhidrosis, HSAN IV: hereditary sensory and autonomic neuropathy type IV, NTRKI: neurotrophic tyrosine kinase 1,
Keywords: Congenital insensitivity to pain and anhidrosis, hereditary sensory and autonomic neuropathy type IV
Citation: Rini PN, Irvandy MS, Pradhea TA. Complications in patients with congenital insensitivity to pain and anhidrosis: a systematic review. Anaesth. pain intensive care 2025;29(6):1290-1301. DOI: 10.35975/apic.v29i6.3067
Received: February 16, 2025; Revised: November 02, 2025; Accepted: November 16, 2025
Congenital Insensitivity to Pain and Anhidrosis (CIPA) is a rare form of hereditary sensory and autonomic neuropathy (HSAN) type IV, caused by a genetic mutation in the neurotrophic tyrosine kinase 1 (NTRK1) gene.1,2 This autosomal recessive condition disrupts the regulation of pain and temperature sensation, affecting multiple aspects of physical and neurodevelopmental functioning CIPA affects approximately 1 in 125 million people, with common symptoms such as recurrent fever, absence of sweating, insensitivity to pain, and a tendency to self-harm. In severe cases, patients may experience developmental delays or mental retardation.3 Chromosomal abnormalities in CIPA patients are reported to be mutations in neurotrophic tyrosine kinase 1 (NTRK1).2 The inability to sense pain impedes normal responses to injuries, making patients particularly vulnerable to infections and other complications.
The lack of connection between pain-sensing nerves and the brain’s pain-processing centers complicates early intervention and treatment in CIPA patients.4 Repeated complications can lead to the development of new, debilitating conditions, significantly reducing quality of life.5 Despite increased awareness of the disease's impact, research on its long-term complications remains limited. This study seeks to explore these complications to inform strategies aimed at improving the quality of life for CIPA patients.
This systematic review was conducted based on the PRISMA 2020 Guideline.6 The search for the relevant studies was carried out on October 30, 2024, across international databases such as PubMed, ScienceDirect, and ProQuest. The protocol for this review has been registered with the International Prospective Register for Systematic Reviews (PROSPERO) under the registration number CRD42025606656.
The keywords for this study were selected based on the relevance to the research topics, using terms such as "Congenital Insensitivity to Pain and Anhidrosis" and "Hereditary Sensory and Autonomic Neuropathy Type IV," combined with the Boolean method (Table 1). This approach ensured that all relevant studies related to the topic were captured effectively.
Clinical studies and case reports involving patients diagnosed with congenital insensitivity to pain and anhidrosis, articles published in English, free full-text availability, and publications from the last 10 years (2014–2024) were included. Exclusion criteria included studies that did not report complications, research using review methods (narrative reviews, systematic reviews, or meta-analyses), books or documents, articles in languages other than English, inaccessible articles, and duplicate studies, where only one version was considered.
Three reviewers (PNR, MSI, TAP) independently assessed titles and abstracts to identify potentially relevant studies. Subsequently, full-text articles were retrieved and evaluated for eligibility based on the inclusion and exclusion criteria. The JBI tool was utilized to assess the quality of the included case reports, categorizing criteria as “Yes,” “No,” or “Unclear” to increase credibility and facilitate collaboration between authors, while also extracting key information such as country of origin, patient demographics (e.g., sex, age, familial and parental marital history), genetic variants, and other clinical markers.7
Based on the critical appraisal using the JBI assessment, six of the eight appraisal questions were adequately addressed by more than 80% of the 29 reviewed articles, while the remaining two were met by over 58% of studies. However, several articles did not provide data presented according to a timeline, which limited the ability to evaluate disease progression. Nevertheless, most studies were able to supply sufficient data to support and strengthen the findings of this review. In contrast, studies providing detailed clinical, familial, and genetic data enhanced validity and introduced novel findings such as specific NTRK1 mutations and rare complications.
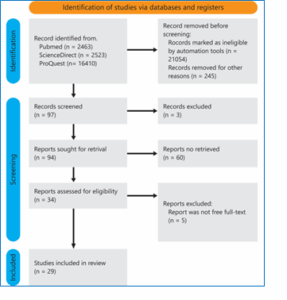
During the search for articles in the different databases (PubMed, Science Direct, and ProQuest), 97 articles were considered, which, upon a preliminary reading of titles and abstracts, were further reduced to 34 because did not fit in with the line of research pursued by this systematic review (e.g. the articles did not include any complication, the articles were review article or books, and duplicates). These 34 articles were selected for free full-text evaluation, and ultimately, this review includes 29 articles that were matched with inclusion criteria. Below is the flow diagram of the current systematic review. (Figure 1)
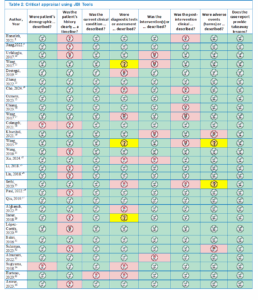
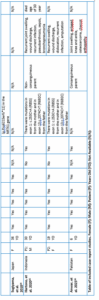
The critical appraisal of the included studies was conducted using JBI tools, as presented in Table 2, with a summary of the appraisal results provided in Figure 2. The detailed characteristics of all included studies are presented in Table 3, while Figure 3 provides a summarized overview of demographic distribution (sex, age, country) and complication percentages.




Study Outcomes
This study examined CIPA cases across multiple countries. A total of 29 articles analyzed 41 cases, with a gender distribution of 17 females (41%), 23 males (56%), and 1 unspecified. Most cases were reported from China (41%), Turkey (9%), Saudi Arabia (7%), Japan (7%), Korea (7%), India (4%), Pakistan (4%), and Indonesia (4%); while single cases (2% each) were identified from Palestine, Taiwan, Italy, America, and Jordan.8–36 Genetic mutations were identified in several cases, often from carriers without phenotypic expression.13,14,20–22,24 The mutations were homozygous (10 cases) or heterozygous (12 cases).8,13,14,17,21–24,30–33
The CIPA phenotype appeared in both familial and non-familial cases, including consanguineous marriages.8,12,14,17,19–23,25,26,29–31,33,35,36 Mortality data was limited, with only two patients reported deceased at 30 years of age.31,35
Among 41 cases, 34 had complications, including unexplained fever (87 %)9–17,19–27,30–36, self-injurious behavior (73 %) 8–36, recurrent fractures (68%)8,10–14,16,17,19–22,24,28–31,34–36, developmental delay (63%)8–16,19–26,30,32,33,36. Some patients were diagnosed with Riga-Fede, Lesch-Nyhan, Renal Amyloidosis, Nora Lesion, or ASD (12%).9,13,18,28–31,36 Other complications also included swelling, dislocation, ulceration, hyperkeratosis, infection, and Charcot arthropathy (9%).28,29,36
Clinically, all patients exhibited insensitivity to pain, with many presenting early self-mutilation behaviors, recurrent unexplained fevers due to anhidrosis, and frequent bone fractures and joint dislocations. Some cases also reported developmental delays, ASD, or neurological complications such as paraplegia. Genetic analysis revealed various NTRK1 mutations, including homozygous, heterozygous, and compound heterozygous forms, with some cases linked to consanguinity. Additional complications included recurrent infections, palmo-plantar hyperkeratosis, poor wound healing, and susceptibility to osteomyelitis. Several patients experienced hair loss, and antipyretics were often ineffective in managing fever. While most patients were alive at reporting, severe complications such as coma, respiratory failure, and paraplegia were observed.
The clinical manifestations commonly reported in CIPA patients across multiple studies include insensitivity to pain stimuli and anhidrosis.3 Based on the results of data collection, China has the highest number of reported CIPA cases, with 17 cases documented in the reviewed articles. However, there is limited research investigating the relationship between CIPA incidence and specific ethnic groups.
Among the 41 cases analyzed, 23 documented the marital history of the patients' parents. Six cases involved patients with parents who were consanguineous, while 17 cases had parents without inbreeding. The inheritance pattern in CIPA is autosomal recessive, meaning that cases may or may not affect other family members. For instance, Hartono et al. (2020) reported a case in which a consanguineous couple had two children, both diagnosed with CIPA, due to both parents carrying mutations in the NTRK1 gene.35 In contrast, Wang et al. (2017) described a case where the patient’s siblings did not exhibit CIPA phenotypes, as the mutation occurred in the father, and the affected child acquired an additional de novo mutation independent of parental inheritance.20
The mean age of CIPA patients in the reviewed cases was 10.9 years, with the oldest patient being 38 years and the youngest 1 year old.9,29 However, these ages reflect the last recorded visits to healthcare facilities rather than actual life expectancy. Ghorpade et al. (2023) suggested that CIPA patients rarely live beyond 25 years.37 Contrary to our literature review, surprisingly there were cases of CIPA patients living up to the age of 38 years and cases who died at the age of 30 years.29,31,35 The lack of long-term follow-up in many cases makes it difficult to fully understand the disease trajectory and lifespan of CIPA patients.
One of the hallmark clinical features of CIPA is anhidrosis, which results from mutations in the NTRK1 gene.2 This gene is essential for the development, differentiation, and maintenance of sensory and sympathetic neurons.21 Consequently, CIPA patients not only lose the ability to perceive pain but also experience impaired sweat gland function.33 Although histological analysis shows that their sweat glands appear structurally normal, their physiological function is disrupted, leading to an inability to regulate body temperature. As a result, recurrent febrile episodes commonly occur during the first two years of life.3,22 In some cases, antipyretics prove ineffective due to the absence of NTRK1-mediated neural regulation in the thermoregulatory system.19,21 Instead, conventional cooling methods, such as bathing, are often used to manage hyperthermia.20
The absence of pain perception in CIPA patients makes them highly susceptible to undetected injuries. Pain serves as a crucial warning signal triggered by nociceptive pathways, alerting individuals to potential harm.38 In CIPA patients, the inability to recognize trauma often leads to repeated injuries, which may go unnoticed unless accompanied by inflammation. Consequently, recurrent fractures, joint dislocations, and chronic wounds are common complications in these patients.
Self-mutilation is another significant characteristic of CIPA. This behavior is closely linked to the patient’s inability to perceive pain, with many cases reporting the onset of self-injurious behaviors during the teething process. However, not all CIPA patients exhibit self-mutilation.13,19,20,31 Among the 41 cases reviewed, three patients did not engage in self-harming behaviors, likely due to parental interventions and strict supervision.14,23 This finding highlights the role of behavioral and environmental factors in modulating self-mutilation tendencies.39,40 Additional complications, including swelling, ulceration, recurrent infections, joint dislocations, slow wound healing, hyperkeratosis, and Charcot arthropathy, were also frequently reported. These complications often result from repeated trauma and self-mutilation, underscoring the importance of parental education and close monitoring of affected children
Beyond physical injuries, neurological and developmental impairments are frequently observed in CIPA patients. Of the 41 cases analyzed, 26 reported delayed mental development. Zhang et al. (2022) noted that many CIPA patients exhibit intellectual disabilities, emotional instability, and hyperactivity.13 In addition, Bakri et al. (2016) reported that CIPA patients may develop inflammatory bowel disease due to immune system dysregulation.31 Furthermore, some patients have been diagnosed with coexisting conditions such as autism spectrum disorder (ASD) or Nora’s lesion. However, Zhang et al. found no direct correlation between NTRK1 mutations and the genetic mutations associated with ASD.13 Similarly, Colangeli et al. (2021) described a case of Nora’s lesion in a child with CIPA, though its etiopathogenesis remains unclear. These findings suggest that while CIPA primarily affects the nervous system, it may also contribute to broader systemic complications.18
Complications in CIPA patients show marked variability influenced by geography, sex, and age. Reports from China highlighted the broadest spectrum of complications—including autism spectrum disorder, recurrent dislocations, impaired healing, and severe infections—while Turkey, Korea, and Palestine described septic arthritis, palmar thickening, and poor weight gain, and cases from Pakistan, India, Japan, and Saudi Arabia more often reported Charcot arthropathy, musculoskeletal deformities, and life-threatening infections.8–10,12–15,22,24,27 Rare manifestations such as CNS perfusion abnormalities, Riga-Fede disease, and renal amyloidosis were also documented in select regions.16,30,31 Sex-based patterns were noted, with females more frequently showing alopecia, scoliosis, and osteomyelitis with amputation, while males often developed severe complications such as renal amyloidosis, respiratory failure, and sepsis.21,31,35 Age distribution further revealed that complications were most often identified in toddlers, followed by school-age children, underscoring age as a determinant of clinical presentation.8–16,18–21,25–27,30,32,36 Collectively, these findings emphasize that demographic and geographic factors substantially shape complication patterns and warrant further study to clarify underlying genetic, environmental, and healthcare-related influences.
Early diagnosis of CIPA is essential to reduce complications and improve patient outcomes. In this review, 87% of patients experienced recurrent fever, 73% self-mutilation, 68% fractures, and 63% developmental delay, indicating a substantial clinical burden. Most reported cases originated from China, likely reflecting a higher number of publications rather than true geographic prevalence. However, limited long-term follow-up—most patients were reported during childhood—hinders a full understanding of disease progression. Further longitudinal studies are needed to clarify genotype–phenotype correlations and improve the quality of life of affected individuals.
Authors affiliations;
- Poppy Novita Rini, Ji Prof. Dr. H. Hadari Nawawi, Pontianak, 78124, West Kalimantan, Indonesia; Email; poppynovitarini@medical.untan.ac.id; {ORCID:0009-0007-2314-0881}
- Muhammad Syifa Irvandy, Ji Prof. Dr. H. Hadari Nawawi, Pontianak, 78124, West Kalimantan, Indonesia; Email; muhammadsyifairvandy130773@gmail.com; {ORCID:0009-0002-3510-1226}
- Tifani Antonia Pradhea, Ji Prof. Dr. H. Hadari Nawawi, Pontianak, 78124, West Kalimantan, Indonesia; Email; tifaniantonia@gmail.com; {ORCID:0009-0009-0223-826X}
ABSTRACT
Background. Congenital Insensitivity to Pain and Anhidrosis (CIPA) is a rare hereditary sensory and autonomic neuropathy type IV (HSAN IV) caused by NTRK1 gene mutations. It disrupts pain and temperature regulation, leading to anhidrosis, recurrent fever, self-injury, and, in severe cases, intellectual disability. The absence of pain perception increases the risk of unnoticed injuries and long-term complications. Understanding these complications is essential to improving patient care and quality of life.
Methodology: A systematic search on PubMed, ScienceDirect, and ProQuest was conducted on October 30, 2024, using keywords related to CIPA and HSAN IV. This review included English-language clinical studies and case reports (2014–2024) reporting complications of CIPA. Reviews, books, inaccessible articles, and duplicates were excluded. A total of 29 case reports were analyzed, with quality assessed using JBI Critical Appraisal Tools.
Result. A total of 29 articles met the inclusion criteria, reporting complications among patients with CIPA. The most frequently observed complications were fever (87%), self-mutilation (73%), and recurrent fractures (68%), while developmental delay (63%) represented a major neurodevelopmental manifestation. The mean age of patients was 10.9 years, ranging from 1 to 38 years. Most reported cases originated from China (41%).
Conclusion. This review emphasizes the importance of early diagnosis in CIPA patients to prevent complications. However, current studies often lack comprehensive follow-up, which hinders our understanding of long-term outcomes. Further research is needed to fill these gaps and improve the quality of life for patients with this rare condition.
Abbreviations: CIPA: Congenital Insensitivity to Pain and Anhidrosis, HSAN IV: hereditary sensory and autonomic neuropathy type IV, NTRKI: neurotrophic tyrosine kinase 1,
Keywords: Congenital insensitivity to pain and anhidrosis, hereditary sensory and autonomic neuropathy type IV
Citation: Rini PN, Irvandy MS, Pradhea TA. Complications in patients with congenital insensitivity to pain and anhidrosis: a systematic review. Anaesth. pain intensive care 2025;29(6):1290-1301. DOI: 10.35975/apic.v29i6.3067
Received: February 16, 2025; Revised: November 02, 2025; Accepted: November 16, 2025
1. INTRODUCTION
Congenital Insensitivity to Pain and Anhidrosis (CIPA) is a rare form of hereditary sensory and autonomic neuropathy (HSAN) type IV, caused by a genetic mutation in the neurotrophic tyrosine kinase 1 (NTRK1) gene.1,2 This autosomal recessive condition disrupts the regulation of pain and temperature sensation, affecting multiple aspects of physical and neurodevelopmental functioning CIPA affects approximately 1 in 125 million people, with common symptoms such as recurrent fever, absence of sweating, insensitivity to pain, and a tendency to self-harm. In severe cases, patients may experience developmental delays or mental retardation.3 Chromosomal abnormalities in CIPA patients are reported to be mutations in neurotrophic tyrosine kinase 1 (NTRK1).2 The inability to sense pain impedes normal responses to injuries, making patients particularly vulnerable to infections and other complications.
The lack of connection between pain-sensing nerves and the brain’s pain-processing centers complicates early intervention and treatment in CIPA patients.4 Repeated complications can lead to the development of new, debilitating conditions, significantly reducing quality of life.5 Despite increased awareness of the disease's impact, research on its long-term complications remains limited. This study seeks to explore these complications to inform strategies aimed at improving the quality of life for CIPA patients.
2. METHODOLOGY
This systematic review was conducted based on the PRISMA 2020 Guideline.6 The search for the relevant studies was carried out on October 30, 2024, across international databases such as PubMed, ScienceDirect, and ProQuest. The protocol for this review has been registered with the International Prospective Register for Systematic Reviews (PROSPERO) under the registration number CRD42025606656.
The keywords for this study were selected based on the relevance to the research topics, using terms such as "Congenital Insensitivity to Pain and Anhidrosis" and "Hereditary Sensory and Autonomic Neuropathy Type IV," combined with the Boolean method (Table 1). This approach ensured that all relevant studies related to the topic were captured effectively.
| Table 1: Boolean Operator | ||
| No | Database | Keyword dan boolean operator |
| 1. | PubMed | (Congenital insensitivity to Pain and Anhidrosis) OR (Hereditary Sensory and Autonomic Neuropathy Type IV) |
| 2. | Science Direct | congenital insensitivity to pain and anhidrosis OR hereditary sensory and autonomic neuropathy Type IV |
| 3. | ProQuest | (congenital insensitivity to pain with anhidrosis) OR (hereditary sensory and autonomic neuropathy Type IV) |
Clinical studies and case reports involving patients diagnosed with congenital insensitivity to pain and anhidrosis, articles published in English, free full-text availability, and publications from the last 10 years (2014–2024) were included. Exclusion criteria included studies that did not report complications, research using review methods (narrative reviews, systematic reviews, or meta-analyses), books or documents, articles in languages other than English, inaccessible articles, and duplicate studies, where only one version was considered.
Three reviewers (PNR, MSI, TAP) independently assessed titles and abstracts to identify potentially relevant studies. Subsequently, full-text articles were retrieved and evaluated for eligibility based on the inclusion and exclusion criteria. The JBI tool was utilized to assess the quality of the included case reports, categorizing criteria as “Yes,” “No,” or “Unclear” to increase credibility and facilitate collaboration between authors, while also extracting key information such as country of origin, patient demographics (e.g., sex, age, familial and parental marital history), genetic variants, and other clinical markers.7
Based on the critical appraisal using the JBI assessment, six of the eight appraisal questions were adequately addressed by more than 80% of the 29 reviewed articles, while the remaining two were met by over 58% of studies. However, several articles did not provide data presented according to a timeline, which limited the ability to evaluate disease progression. Nevertheless, most studies were able to supply sufficient data to support and strengthen the findings of this review. In contrast, studies providing detailed clinical, familial, and genetic data enhanced validity and introduced novel findings such as specific NTRK1 mutations and rare complications.
3. RESULTS
During the search for articles in the different databases (PubMed, Science Direct, and ProQuest), 97 articles were considered, which, upon a preliminary reading of titles and abstracts, were further reduced to 34 because did not fit in with the line of research pursued by this systematic review (e.g. the articles did not include any complication, the articles were review article or books, and duplicates). These 34 articles were selected for free full-text evaluation, and ultimately, this review includes 29 articles that were matched with inclusion criteria. Below is the flow diagram of the current systematic review. (Figure 1)
The critical appraisal of the included studies was conducted using JBI tools, as presented in Table 2, with a summary of the appraisal results provided in Figure 2. The detailed characteristics of all included studies are presented in Table 3, while Figure 3 provides a summarized overview of demographic distribution (sex, age, country) and complication percentages.
Study Outcomes
This study examined CIPA cases across multiple countries. A total of 29 articles analyzed 41 cases, with a gender distribution of 17 females (41%), 23 males (56%), and 1 unspecified. Most cases were reported from China (41%), Turkey (9%), Saudi Arabia (7%), Japan (7%), Korea (7%), India (4%), Pakistan (4%), and Indonesia (4%); while single cases (2% each) were identified from Palestine, Taiwan, Italy, America, and Jordan.8–36 Genetic mutations were identified in several cases, often from carriers without phenotypic expression.13,14,20–22,24 The mutations were homozygous (10 cases) or heterozygous (12 cases).8,13,14,17,21–24,30–33
The CIPA phenotype appeared in both familial and non-familial cases, including consanguineous marriages.8,12,14,17,19–23,25,26,29–31,33,35,36 Mortality data was limited, with only two patients reported deceased at 30 years of age.31,35
Among 41 cases, 34 had complications, including unexplained fever (87 %)9–17,19–27,30–36, self-injurious behavior (73 %) 8–36, recurrent fractures (68%)8,10–14,16,17,19–22,24,28–31,34–36, developmental delay (63%)8–16,19–26,30,32,33,36. Some patients were diagnosed with Riga-Fede, Lesch-Nyhan, Renal Amyloidosis, Nora Lesion, or ASD (12%).9,13,18,28–31,36 Other complications also included swelling, dislocation, ulceration, hyperkeratosis, infection, and Charcot arthropathy (9%).28,29,36
Clinically, all patients exhibited insensitivity to pain, with many presenting early self-mutilation behaviors, recurrent unexplained fevers due to anhidrosis, and frequent bone fractures and joint dislocations. Some cases also reported developmental delays, ASD, or neurological complications such as paraplegia. Genetic analysis revealed various NTRK1 mutations, including homozygous, heterozygous, and compound heterozygous forms, with some cases linked to consanguinity. Additional complications included recurrent infections, palmo-plantar hyperkeratosis, poor wound healing, and susceptibility to osteomyelitis. Several patients experienced hair loss, and antipyretics were often ineffective in managing fever. While most patients were alive at reporting, severe complications such as coma, respiratory failure, and paraplegia were observed.
4. DISCUSSION
The clinical manifestations commonly reported in CIPA patients across multiple studies include insensitivity to pain stimuli and anhidrosis.3 Based on the results of data collection, China has the highest number of reported CIPA cases, with 17 cases documented in the reviewed articles. However, there is limited research investigating the relationship between CIPA incidence and specific ethnic groups.
Among the 41 cases analyzed, 23 documented the marital history of the patients' parents. Six cases involved patients with parents who were consanguineous, while 17 cases had parents without inbreeding. The inheritance pattern in CIPA is autosomal recessive, meaning that cases may or may not affect other family members. For instance, Hartono et al. (2020) reported a case in which a consanguineous couple had two children, both diagnosed with CIPA, due to both parents carrying mutations in the NTRK1 gene.35 In contrast, Wang et al. (2017) described a case where the patient’s siblings did not exhibit CIPA phenotypes, as the mutation occurred in the father, and the affected child acquired an additional de novo mutation independent of parental inheritance.20
The mean age of CIPA patients in the reviewed cases was 10.9 years, with the oldest patient being 38 years and the youngest 1 year old.9,29 However, these ages reflect the last recorded visits to healthcare facilities rather than actual life expectancy. Ghorpade et al. (2023) suggested that CIPA patients rarely live beyond 25 years.37 Contrary to our literature review, surprisingly there were cases of CIPA patients living up to the age of 38 years and cases who died at the age of 30 years.29,31,35 The lack of long-term follow-up in many cases makes it difficult to fully understand the disease trajectory and lifespan of CIPA patients.
One of the hallmark clinical features of CIPA is anhidrosis, which results from mutations in the NTRK1 gene.2 This gene is essential for the development, differentiation, and maintenance of sensory and sympathetic neurons.21 Consequently, CIPA patients not only lose the ability to perceive pain but also experience impaired sweat gland function.33 Although histological analysis shows that their sweat glands appear structurally normal, their physiological function is disrupted, leading to an inability to regulate body temperature. As a result, recurrent febrile episodes commonly occur during the first two years of life.3,22 In some cases, antipyretics prove ineffective due to the absence of NTRK1-mediated neural regulation in the thermoregulatory system.19,21 Instead, conventional cooling methods, such as bathing, are often used to manage hyperthermia.20
The absence of pain perception in CIPA patients makes them highly susceptible to undetected injuries. Pain serves as a crucial warning signal triggered by nociceptive pathways, alerting individuals to potential harm.38 In CIPA patients, the inability to recognize trauma often leads to repeated injuries, which may go unnoticed unless accompanied by inflammation. Consequently, recurrent fractures, joint dislocations, and chronic wounds are common complications in these patients.
Self-mutilation is another significant characteristic of CIPA. This behavior is closely linked to the patient’s inability to perceive pain, with many cases reporting the onset of self-injurious behaviors during the teething process. However, not all CIPA patients exhibit self-mutilation.13,19,20,31 Among the 41 cases reviewed, three patients did not engage in self-harming behaviors, likely due to parental interventions and strict supervision.14,23 This finding highlights the role of behavioral and environmental factors in modulating self-mutilation tendencies.39,40 Additional complications, including swelling, ulceration, recurrent infections, joint dislocations, slow wound healing, hyperkeratosis, and Charcot arthropathy, were also frequently reported. These complications often result from repeated trauma and self-mutilation, underscoring the importance of parental education and close monitoring of affected children
Beyond physical injuries, neurological and developmental impairments are frequently observed in CIPA patients. Of the 41 cases analyzed, 26 reported delayed mental development. Zhang et al. (2022) noted that many CIPA patients exhibit intellectual disabilities, emotional instability, and hyperactivity.13 In addition, Bakri et al. (2016) reported that CIPA patients may develop inflammatory bowel disease due to immune system dysregulation.31 Furthermore, some patients have been diagnosed with coexisting conditions such as autism spectrum disorder (ASD) or Nora’s lesion. However, Zhang et al. found no direct correlation between NTRK1 mutations and the genetic mutations associated with ASD.13 Similarly, Colangeli et al. (2021) described a case of Nora’s lesion in a child with CIPA, though its etiopathogenesis remains unclear. These findings suggest that while CIPA primarily affects the nervous system, it may also contribute to broader systemic complications.18
Complications in CIPA patients show marked variability influenced by geography, sex, and age. Reports from China highlighted the broadest spectrum of complications—including autism spectrum disorder, recurrent dislocations, impaired healing, and severe infections—while Turkey, Korea, and Palestine described septic arthritis, palmar thickening, and poor weight gain, and cases from Pakistan, India, Japan, and Saudi Arabia more often reported Charcot arthropathy, musculoskeletal deformities, and life-threatening infections.8–10,12–15,22,24,27 Rare manifestations such as CNS perfusion abnormalities, Riga-Fede disease, and renal amyloidosis were also documented in select regions.16,30,31 Sex-based patterns were noted, with females more frequently showing alopecia, scoliosis, and osteomyelitis with amputation, while males often developed severe complications such as renal amyloidosis, respiratory failure, and sepsis.21,31,35 Age distribution further revealed that complications were most often identified in toddlers, followed by school-age children, underscoring age as a determinant of clinical presentation.8–16,18–21,25–27,30,32,36 Collectively, these findings emphasize that demographic and geographic factors substantially shape complication patterns and warrant further study to clarify underlying genetic, environmental, and healthcare-related influences.
5. CONCLUSION
Early diagnosis of CIPA is essential to reduce complications and improve patient outcomes. In this review, 87% of patients experienced recurrent fever, 73% self-mutilation, 68% fractures, and 63% developmental delay, indicating a substantial clinical burden. Most reported cases originated from China, likely reflecting a higher number of publications rather than true geographic prevalence. However, limited long-term follow-up—most patients were reported during childhood—hinders a full understanding of disease progression. Further longitudinal studies are needed to clarify genotype–phenotype correlations and improve the quality of life of affected individuals.
- Study Limitation and Further Recommendation
- Data availability
- Conflict of interest
- Funding
- Authors’ contribution
11. REFERENCES
- Shin JY, Kim SW, Roh SG, Lee NH, Yang KM. Congenital Insensitivity to Pain and Anhidrosis. Arch Plast Surg. 2016 Jan;43(1):95–7.
- Indo Y, Tsuruta M, Hayashida Y, Karim MA, Ohta K, Kawano T, et al. Mutations in the TRKA/NGF receptor gene in patients with congenital insensitivity to pain with anhidrosis. Nat Genet. 1996 Aug;13(4):485–8.
- SWANSON AG. Congenital insensitivity to pain with anhydrosis. A unique syndrome in two male siblings. Arch Neurol. 1963 Mar;8:299–306.
- Daneshjou K, Jafarieh H, Raaeskarami SR. Congenital Insensitivity to Pain and Anhydrosis (CIPA) Syndrome; A Report of 4 Cases. Iran J Pediatr. 2012 Sep;22(3):412–6.
- Indo Y. Genetics of congenital insensitivity to pain with anhidrosis (CIPA) or hereditary sensory and autonomic neuropathy type IV. Clinical, biological and molecular aspects of mutations in TRKA(NTRK1) gene encoding the receptor tyrosine kinase for nerve growth factor. Clin Auton Res Off J Clin Auton Res Soc. 2002 May;12 Suppl 1:I20-32.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021 Mar 29;10(1):89.
- JBI Critical Appraisal Tools | JBI [Internet]. [cited 2025 Feb 16]. Available from: https://jbi.global/critical-appraisal-tools
- Hanatleh OM, Kofahi NK, Aburahma SK, Bintareef EM, Al-Bashtawy M, Alkhawaldeh A, et al. A 5-Year-Old Palestinian Bedouin Girl with Repeated Self-Induced Injuries to the Digits, a Diagnosis of Congenital Insensitivity to Pain, and Anhidrosis. Am J Case Rep. 2021 Nov 4;22:e933486.
- Jiang J, Wang X, Hu J, Wang S. A case report: Anesthetic management for open‐heart surgery in a child with congenital insensitivity to pain with anhidrosis. Pediatr Anesth. 2022;32(9):1070–2.
- Urfalioglu A, Arslan M, Duman Y, Gisi G, Oksuz G, Yildiz H, et al. Anesthesia procedure for congenital insensitivity to pain in a child with anhidrosis syndrome: A rare case. J Nippon Med Sch. 2017;84(5):237–40.
- Wang C, Zhang X, Guo S, Sun J, Li N. Anesthetic management during adenotonsillectomy for twins with congenital insensitivity to pain with anhidrosis: two case reports. J Med Case Reports. 2017;11:1–4.
- DESTEGÜL D, Kocaöz F, SARI AS. Anesthetic management of two siblings with congenital insensitivity to pain with anhidrosis syndrome. Agri Agri Algoloji Derneginin Yayin Organidir J Turk Soc Algol. 2019;31(4):202–5.
- Zhang M, Cao X, Li N, Duan G, Zhang X. Autism spectrum disorder in a boy with congenital insensitivity to pain with anhidrosis: a case report. BMC Pediatr. 2022;22(1):126.
- Cho JH, Hwang S, Kwak YH, Yum M, Seo GH, Koh J, et al. Clinical and genetic characteristics of three patients with congenital insensitivity to pain with anhidrosis: Case reports and a review of the literature. Mol Genet Genomic Med. 2024;12(4):e2430.
- Özmete Ö, Şener M, Bali Ç, Çalışkan E, Arıboğan A. Congenital insensitivity to pain: How should anesthesia be managed? Turk J Pediatr. 2017;59(1):87–9.
- Chiang CC, Wu YC, Lan CH, Wang KC, Tang HC, Chang ST. Exploring CNS Involvement in Pain Insensitivity in Hereditary Sensory and Autonomic Neuropathy Type 4: Insights from Tc− 99m ECD SPECT Imaging. Tomography. 2023;9(6):2261–9.
- Wang T, Li H, Xiang J, Wei B, Zhang Q, Zhu Q, et al. Identification of a novel nonsense mutation of the neurotrophic tyrosine kinase receptor type 1 gene in two siblings with congenital insensitivity to pain with anhidrosis. J Int Med Res. 2017;45(2):549–55.
- Colangeli M, Spinnato P, Zarantonello P, Bendandi B, Donati DM. Nora’s lesion in a child: a case of complete spontaneous regression. Balk Med J. 2021;38(1):57.
- Khurshid S, Khursheed T, Khan MS. Not Another Case Of Juvenile Idiopathic Arthritis: Congenital Insensitivity To Pain Presenting With Joint Problems. J Ayub Med Coll Abbottabad-Pak. 2021;33(3).
- Wang Q, Guo S, Duan G, Xiang G, Ying Y, Zhang Y, et al. Novel and novel de novo mutations in NTRK1 associated with congenital insensitivity to pain with anhidrosis: a case report. Medicine (Baltimore). 2015;94(19):e871.
- Wang QL, Guo S, Duan G, Ying Y, Huang P, Liu JY, et al. Phenotypes and genotypes in five children with congenital insensitivity to pain with anhidrosis. Pediatr Neurol. 2016;61:63–9.
- Xu Q, Wang Y, Zhou Y, Zhang L, Xiang X, Xie Y, et al. Phenotypes of a toddler with hereditary sensory and autonomic neuropathy type IV: comparing with normal: A case report. Medicine (Baltimore). 2024;103(3):e36955.
- Li N, Sun J, Guo S, Liu Y, Wang C, Zhu C, et al. Phenotypic and genotypic features of a pair of Chinese identical twins with congenital insensitivity to pain and anhidrosis: A case report. Medicine (Baltimore). 2018;97(47):e13209.
- Liu Z, Liu J, Liu G, Cao W, Liu S, Chen Y, et al. Phenotypic heterogeneity of intellectual disability in patients with congenital insensitivity to pain with anhidrosis: a case report and literature review. J Int Med Res. 2018;46(6):2445–57.
- Sethi A, Ramasubramanian S, Swaminathan M. The painless eye: neurotrophic keratitis in a child suffering from hereditary sensory autonomic neuropathy type IV. Indian J Ophthalmol. 2020;68(10):2270–2.
- Paul M, Bamba C, Chugh V, Ravikumar N, Jayaram S. A boy who knows no pain: Anaesthetic management of congenital insensitivity to pain with anhidrosis. Cureus. 2022;14(10).
- Qiu Y, Zhao L, Yao D, Jia Y. Anesthetic management of children with congenital insensitivity to pain with anhidrosis. Pediatr Investig. 2020;4(04):296–8.
- s Alghamdi M, Reda B, Albukhari SN, Qoqandi MA. Arthroplasty of a Charcot knee in a patient with congenital insensitivity to pain. Cureus. 2022;14(4).
- Inoue D, Kabata T, Kajino Y, Taga T, Yamamoto T, Takagi T, et al. Clinical results of total hip arthroplasty in two patients with Charcot hip joints due to congenital insensivity to pain with anhydrosis. Case Rep Orthop. 2018;2018(1):1743068.
- López-Cortés A, Zambrano AK, Guevara-Ramírez P, Echeverría BA, Guerrero S, Cabascango E, et al. Clinical, genomics and networking analyses of a high-altitude native American Ecuadorian patient with congenital insensitivity to pain with anhidrosis: a case report. BMC Med Genomics. 2020;13:1–9.
- Bakri FG, Wahbeh A, Sneina AA, Al Khader A, Obeidat F, AlAwwa I, et al. Congenital insensitivity to pain and anhydrosis due to a rare mutation and that is complicated by inflammatory bowel disease and amyloidosis: a case report. Clin Case Rep. 2016;4(10):997.
- Sulaiman NM, Alyahya E. Congenital Insensitivity to Pain with Anhidrosis: A Case Report. Cureus. 2023;15(11).
- Almutairi MM, Tabassum S. Congenital insensitivity to pain with anhidrosis: A case report and review of the pertinent literature. Cureus. 2022;14(11).
- Sugiyama Y, Gotoh S, Urasawa M, Kawamata M, Nakajima K. Hemodynamic response to massive bleeding in a patient with congenital insensitivity to pain with anhidrosis. Case Rep Anesthesiol. 2018;2018(1):9593458.
- Hartono F, Tanjung C, Besinga KE, Marpaung D, Ananditya T, Budisantoso AB. Catastrophic results due to unrecognizing of congenital insensitivity to pain with anhidrosis in children with multiple long bones fractures: A case report of 27 years follow-up of two siblings. Int J Surg Case Rep. 2020;73:213–7.
- Anwar M, Malik MR, Bashir S, Hassan U, Sadaf A. Hyperplastic callus formation in congenital insensitivity to pain: A masquerader of osteosarcoma. Pediatr Hematol Oncol J. 2023;8(1):10–3.
- Ghorpade V, Zore M, Arjun P, Kore A, Kadam S. A Brief Review on Congenital Insensitivity to Pain and Anhydrosis (CIPA). Int J Pharm Pharm Res [Internet]. 2023;27. Available from: www.ijppr.humanjournals.com
- Chen J, Kandle PF, Murray I, Fitzgerald LA, Sehdev JS. Physiology, pain. 2019;
- Arafat SY, Akter H, Islam MA, Shah MMA, Kabir R. Parenting: Types, effects and cultural variation. Asian J Pediatr Res. 2020;3(3):32–6.
- Alizadeh S, Talib MBA, Abdullah R, Mansor M. Relationship between parenting style and children’s behavior problems. Asian Soc Sci. 2011;7(12):195–200.