Reza Widianto Sudjud 1 , Jenifer kiem 2 , Ruli Herman Sitanggang 3 , Ike Sri Redjeki 4 , Erwin Pradian 5 , Suwarman 6 , Nurita Dian Kestriani 7
Authors affiliations:
Methodology: The study compared breathing rate (BR), tidal volume (VT), and peak inspiratory pressure (PIP) delivered by AirgencyTM and 50 medical professionals during a controlled 30-minute resuscitation session. Variability in performance was assessed using the coefficient of variation, while fatigue in medical professionals was measured using the Visual Analog Scale for Fatigue (VAS-F).
Results: AirgencyTM demonstrated significantly lower variability in all parameters compared to medical professionals (P < 0.0001). While medical professionals exhibited significant variability in BR (27.6%), VT (26.4%), and PIP (25.2%), AirgencyTM demonstrated minimal fluctuations, with coefficients of variation under 3% for all parameters. Fatigue among medical professionals increased significantly over the resuscitation period, with median VAS-F scores rising from 1 to 5.
Conclusion: AirgencyTM consistently outperformed medical professionals in maintaining precise ventilation parameters with minimal variability. These results suggest that automated devices like AirgencyTM may enhance the reliability of resuscitation efforts, particularly in mitigating the impact of operator fatigue. However, further studies in real-world settings are necessary to confirm these findings.
Abbreviations: BR: breathing rate, PIP: peak inspiratory pressure, VAS-F: Visual Analog Scale for Fatigue,
Keywords: bag-valve manual resuscitation machine; breathing rate; tidal volume; peak inspiratory pressure; fatigue.
Citation: Sudjud RW, Aviani JK, Sitanggang RH, Redjeki IS, Pradian E, Suwarman, Kestriani ND. Simulation-based assessment of AirgencyTM: a novel automatic resuscitator for emergency respiratory support Anaesth. pain intensive care 2025;29(9):1196-1203. DOI: 10.35975/apic.v29i9.3060
Received: August 17, 2025; Revised: September 05, 2025; Accepted: September 06, 2025
Respiratory failure is a critical disruption of the respiratory system, particularly in the regulation of gas exchange. It is a leading cause of morbidity and mortality among patients in intensive care units. This condition can lead to various complications, including lung failure, hypoxemia, pump failure, alveolar hypoventilation, and hypercapnia.1
During pandemics, the demand for ventilators rises significantly. Reflecting on the recent COVID-19 pandemic, there was a notable disparity between the high admission rates to critical care units and the limited availability of ventilators. Most hospitals had minimal or no surplus ventilators to address the surge in demand caused by disasters or pandemics. However, the high cost of ventilators makes it impractical for healthcare facilities to maintain large reserves. This highlights the pressing need for a simple, cost-effective, yet efficient respiratory support system to address such crises effectively.2
Among the available modalities for respiratory support, the Ambu bag (manual resuscitator) plays a critical role in emergency scenarios. Unlike high-flow nasal cannulas (HFNC), which provide non-invasive oxygen delivery for patients with intact respiratory drive, or mechanical ventilators, which offer precise, long-term support for critically ill patients, the Ambu bag is uniquely suited for immediate and temporary respiratory assistance. Its portability, ease of use, and independence from external power sources make it indispensable in acute settings, especially during resuscitation or transportation of patients. While nasal cannulas and ventilators require specific conditions and setups, the Ambu bag serves as a rapid-response tool that bridges the gap between initial intervention and advanced respiratory management.3
Despite of its simplicity, Ambu bag have been liked to injuries such as gastric insufflation, aspiration, and pneumothorax from hyperventilation. Its effectiveness depends heavily on skilled operators and consistent manual effort, which can be challenging to sustain in prolonged or high-demand situations, such as mass casualties or pandemics. Studies have shown that even the highly skilled operators with high level of experience are prone to hyperventilate patients due to fatigue.4
The development of Airgency, an automatic Ambu-bag resuscitator machine, manufactured by Institut
Teknologi Bandung and Padjadjaran University, Indonesia, offers a transformative solution by automating the manual ventilation process. AirgencyTM ensure consistent, controlled ventilation while reducing the risk of human error and operator fatigue. Moreover, they are cost-effective and portable, making them particularly valuable in resource-limited settings or during large-scale emergencies when advanced mechanical ventilators are unavailable or in short supply. By combining simplicity, reliability, and efficiency, AirgencyTM have the potential to bridge the gap between manual resuscitation and sophisticated ventilators, improving outcomes for patients with respiratory failure in diverse clinical and disaster scenarios. Current study aims to evaluate the performance of AirgencyTM in comparison to manual human resuscitation using an adult Manikin-based simulation model.
2.1. Product Details
Figure 1 illustrates the design and components of the Airgency device. Airgency is a compact and lightweight unit, measuring 21 x 24 x 31 cm and weighing 3 kg. To operate the device, the casing is opened by moving the left and right case handles outward. The Ambu-bag is then placed securely on the Ambu-bag stand, positioned between the presser arms, and fastened into place. All resuscitator components are subsequently attached to the Ambu-bag, and the airflow sensor tube is connected to the Airgency module. The casing is then moved inward to lock the Ambu-bag securely in position. Next, the adaptor cable is connected to the Airgency power supply port and a 200-400 VAC, 50/60 Hz power source. The device is then powered on using the switch. The breathing parameters can then be adjusted with the following configurable settings:
The Assisted Mode supports patients in achieving the set respiratory parameters. In this mode, the patient’s inspiratory effort serves as the trigger to initiate the machine’s cycle, making it appropriate for patients with limited or insufficient spontaneous breathing. System failure is detected if the patient does not initiate an inspiratory effort within 10 seconds. The indicator LED displays the operational status of the device: it illuminates green during Normal Mode and yellow during Assisted Mode. In the event of a system failure, the LED will turn red to signal the error.
During patient transfers, the device can operate independently of an external power source, as it is equipped with a built-in 5200mAh battery, providing up to 2 hours of continuous operation. The indicator LED illuminates green when the device is connected to an external power source and red when operating on battery power.
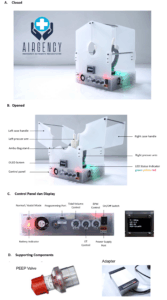
Figure 1: Picture of Airgency (A) closed, (B) opened (C) control panel and (D) supporting components
2.2. Experiment Setting
2.2.1. Manikin Simulation Setting
A respiratory adult Manikin was connected to an automated test lung to monitor ventilation parameters. An Ambu-bag mask was positioned over the Manikin's nose and mouth. Respiratory resuscitation was then performed for 30 minutes, either using the Airgency device or manually by medical professionals.
2.2.2. AirgencyTM Settings
The Airgency device was configured to operate in normal mode, with a tidal volume of 400 mL (selected based on lung-protective ventilation guidelines of 6–8 mL/kg for an average 60–70 kg adult, corresponding to approximately 6 mL/kg), I/E Ratio 1:1, and a breathing rate of 15 breaths per minute (reflecting the normal adult physiologic rate and consistent with BLS/resuscitation guidelines) . The resuscitation procedure was repeated 50 times.
2.2.3. Medical Professionals Control Group
Fifty medical professionals were recruited for the study based on the following inclusion criteria: (1) enrollment in an anesthesiology residency program (PGY-3 to PGY-4), (2) a body mass index (BMI) between 18.5 and 24.99, (3) possession of a valid Basic Life Support (BLS) certification, and (4) being in good physical health at the time of participation.
Each participant was instructed to perform respiratory resuscitation for 30 minutes, maintaining a breathing rate of 15 breaths per minute (bpm). While grip strength was not measured, all participants held valid BLS certification and had prior exposure to manual ventilation as part of training. We have acknowledged this as a limitation regarding variability.
2.3. Outcome Measure
Breathing rate, tidal volume (VT), and peak inspiratory pressure (PIP) were measured every minute using pressure and flow transducers connected to the test lung. The coefficient of variation for each minute's measurements was calculated to assess stability within each group. Operator fatigue was assessed using the Visual Analog Scale for Fatigue (VAS-F), a 10-point scale where 1 indicates no fatigue and 10 indicates extreme fatigue. The mean values of the collected data are presented as a line plot for visualization.
2.4. Statistical Analysis
Statistical analysis was conducted using GraphPad Prism version 10.1.2. An Independent T-Test was used to evaluate differences between groups. Additionally, Multiple Independent T-Tests with the Benjamini, Krieger, and Yekutieli method for controlling the false discovery rate (FDR) at a 5% threshold were performed to assess differences between the two groups at each time point. A P < 0.05 was considered statistically significant.
Here, we offer an outline of the various features,
3.1. Breathing Rate
There were no significant differences in the breathing rate per time frame during resuscitation performed by Airgency and medical professionals. However, over the entire 30-minute period, the mean breathing rate showed a significant difference (P = 0.0170), with Airgency achieving a rate of 14.77 ± 0.07 bpm compared to 14.52 ± 4.00 bpm for medical professionals (Figure 2A).
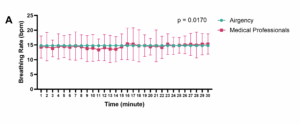
Figure 2 (A): AirgencyTM achieved a rate of 14.77 ± 0.07 bpm compared to 14.52 ± 4.00 bpm for medical professionals
The breathing rate delivered by medical professionals exhibited considerable variability within each time frame, ranging from 18.0% to 36.1% (mean = 27.6%). In contrast, AirgencyTM demonstrated minimal variability across 50 repetitions, with fluctuations between 0.4% and 1.1% (mean = 0.7%). The coefficient of variation between the two groups was significantly different (P < 0.0001) (Figure 2B).
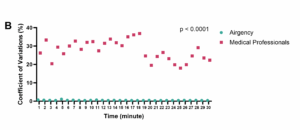
Figure 2 (B): Shows the coefficient of variation between the two groups
3.2. Tidal Volume (VT)
Significant differences were observed in the tidal volume (VT) achieved during resuscitation performed by AirgencyTM compared to medical professionals across each time frame. Over the entire 30-minute period, the mean VT delivered by AirgencyTM was 397.36 ± 3.52 mL, whereas the VT delivered by medical professionals was 353.6 ± 111.75 mL (P = 0.0006) (Figure 3A).
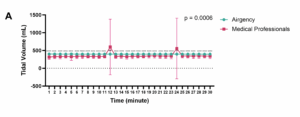
Figure 3 (A): Mean VT delivered by AirgencyTM was more than the VT delivered by medical professionals (P = 0.0006)
The VT delivered by 50 medical professionals showed considerable variability within each time frame, ranging from 13.5% to 153.2% (mean = 26.4%). In contrast, the VT delivered by AirgencyTM exhibited minimal fluctuation across 50 repetitions, ranging from 0.5% to 3.3% (mean = 0.9%) (P < 0.0001) (Figure 3B).
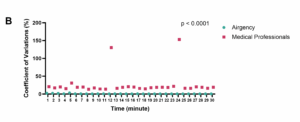
Figure 3 (B) VT delivered by AirgencyTM exhibited minimal fluctuation across 50 repetitions
3.3. Peak Inspiratory Pressure (PIP)
Significant differences in peak inspiratory pressure (PIP) were observed over the entire 30-minute observation period (Figure 4A). The mean PIP generated by AirgencyTM was 29.78 ± 0.84 cm H₂O, whereas the PIP achieved through manual resuscitation by medical professionals was 24.07 ± 6.33 cm H₂O (P < 0.0001).
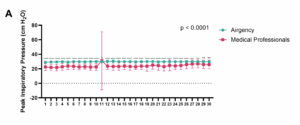
Figure 4 (A): The mean PIP generated by AirgencyTM was higher than achieved through manual resuscitation by medical professionals (P < 0.0001).
The PIP delivered by medical professionals exhibited substantial variability within each time frame, ranging from 15.4% to 128.9% (mean = 25.2%). In contrast, the PIP delivered by AirgencyTM demonstrated minimal fluctuations, ranging from 1.0% to 6.6% (mean = 2.8%) (P < 0.0001) (Figure 4B).
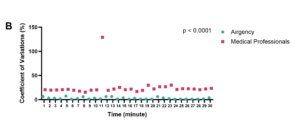
Figure 4 (B) AirgencyTM demonstrated minimal fluctuations (P < 0.0001)
3.4. Fatigue Level
Medical professionals exhibited increasing fatigue over the course of the 30-minute resuscitation procedure, as illustrated in Figure 5. During the initial 9 minutes, the median VAS-F score remained at 1, indicating minimal fatigue. However, by the end of the procedure, the median score had risen to 5, reflecting significant fatigue.
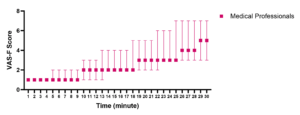
Figure 5: Comparative fatigue onset in the two groups
The findings of this study highlight the superior performance and consistency of AirgencyTM compared to manual resuscitation performed by medical professionals, particularly in critical metrics such as breathing rate, tidal volume (VT), and peak inspiratory pressure (PIP).
Respiratory rate is a critical parameter in ventilation, as excessively high rates can lead to hyperventilation, respiratory alkalosis, and insufficient expiratory time. Conversely, rates that are too low risk inadequate ventilation and respiratory acidosis.5 Both AirgencyTM and medical professionals achieved an appropriate respiratory rate, targeted at 15 breaths per minute, which aligns with the normal physiological and comfortable breathing rate.6 However, deviations were observed among medical professionals, with rates dropping to 8 breaths per minute at the 11th minute and increasing to 21 breaths per minute at the 16th minute. Despite these fluctuations, the rates remained within the range of normal breathing.7
Tidal volume (VT) is a vital parameter during resuscitation, as it must be sufficient to overcome anatomical dead space and ensure effective ventilation. Insufficient tidal volumes can lead to atelectasis, while excessively high volumes may result in hyperventilation and increase the risk of lung injury.7 AirgencyTM demonstrated superior performance in achieving the targeted tidal volume of 400 mL, with an average of 397 ± 3.52 mL over a 30-minute resuscitation period and a low variability of 0.9%. In contrast, human resuscitation achieved only 88.4% of the desired VT, delivering an average of 314.96 ± 65.25 mL (78.7%) during the first minute of resuscitation. Instances of hyperventilation were observed during human resuscitation at the 12th and 24th minutes, with tidal volumes exceeding 1300 mL. A low tidal volume of 6–8 mL/kg of ideal body weight is generally recommended during initial resuscitation, as evidence suggests it is associated with reduced pulmonary complications in patients without acute respiratory distress syndrome (ARDS).7,9,10 For this study, a target tidal volume of 400 mL was chosen, assuming an average adult body weight of 60–70 kg and a tidal volume of 6 mL/kg.
Peak inspiratory pressure (PIP) refers to the maximum pressure exerted on the lungs during inhalation. It is influenced by airway resistance, and elevated PIP levels can indicate underlying issues such as excessive secretions, bronchospasm, occlusion from biting down on ventilation tubing, or reduced lung compliance. Prolonged PIP levels exceeding 40 cm H₂O should generally be avoided, except in cases of acute respiratory distress syndrome (ARDS), where higher pressures may be required to maintain adequate ventilation.10 Both Airgency and manual resuscitation resulted in peak inspiratory pressure (PIP) levels that remained below 30 cm H₂O for most of the 30-minute observation period. However, a transient spike in PIP up to 70 cm H₂O was observed during manual resuscitation at the 11th minute, lasting for one minute. Despite this brief elevation, the PIP levels achieved during both human and Airgency resuscitation were generally within the safe range. Nevertheless, the significant inter variability in PIP during manual resuscitation is a critical point of concern, as it may lead to either insufficient ventilation or hyperventilation, potentially compromising patient safety and outcomes.
Manual hyperventilation can elevate intrathoracic pressure, leading to adverse hemodynamic effects, including reduced venous return (VR), cardiac output (CO), and coronary perfusion pressure (CPP). Furthermore, elevated inspiratory pressures may compromise the lower esophageal sphincter, resulting in gastric insufflation, regurgitation, and aspiration. Excessive manual ventilation can also cause acute barotrauma, manifesting as pneumothorax, pneumomediastinum, pneumoperitoneum, or subcutaneous emphysema. Additionally, sub-barotraumatic lung injuries driven by inflammation may occur due to aggressive ventilation.8
The primary challenge in human resuscitation lies in the significant variability in performance across individuals and over time. Scott et al. (2020) demonstrated that male operators delivered higher tidal volumes compared to female operators. Additionally, operators wearing medium-sized gloves delivered lower tidal volumes compared to those wearing small or large gloves.11 Li et al. (2018) reported that experienced clinicians provided smaller tidal volumes (VT) and higher breathing rates (BR).12 Culbreth and Gardenhire (2021) found a correlation between delivered tidal volumes, peak pressures, years of experience, and the operator's confidence level.13 Khoury et al. observed that excessive ventilation was influenced by rapid bag refilling, which could trigger a reflexive squeeze and ventilation response as soon as the bag reinflates. They also noted that hyperventilation was associated with high grip strength, where excessive insufflation volumes were mitigated by significant air leaks.15 Moreover, the technique used for bag ventilation, such as employing one-hand versus two-hand methods, can significantly affect tidal volume delivery.15 To enhance control over delivered tidal volume (VT), breathing rate (BR), and peak inspiratory pressure (PIP), some groups have developed feedback monitoring systems. These systems have been shown to significantly improve the accuracy of these parameters.8
Muscle fatigue is a significant issue during manual resuscitation, as it can lead to ventilation inconsistencies, as highlighted in several studies.16-19 Our study observed an increase in fatigue levels over time; however, the median fatigue level during a 30-minute resuscitation session was still categorized as mild. Bergrath et al. reported a median fatigue score of 6 out of 10 during 3 hours of bag-valve-mask (BVM) resuscitation.16 Similarly, Halpern et al. documented an increase in Borg's Perceived Exertion and Pain Scale from 6.4 (very light effort) to 10.2 (fairly light effort) over 6 hours of manual resuscitation. This rise in perceived exertion may be attributed more to boredom than to physical fatigue during prolonged resuscitation periods.19
This study has several limitations. First, the variability in manual resuscitation performance by medical professionals may be influenced by factors such as experience level, physical fitness, and training background, which were not detailed in this study. Second, Airgency’s performance was evaluated in a manikin-based simulation under controlled conditions, which may not fully replicate the challenges encountered in clinical or emergency settings, such as patient movement, distractions, or device malfunctions. Third, fatigue levels in medical professionals were assessed using a subjective scale (VAS-F), potentially introducing bias or inconsistency in reporting. Fourth, the study focused on a 30-minute duration, which, while appropriate for an acute resuscitation scenario, does not address the long-term reliability and consistency of Airgency under extended use. Lastly, only three parameters were evaluated in this study, which may not adequately reflect the broader impact on patient physiology. In practical application, Airgency™ requires an oxygen source or power supply, which may limit use in field emergencies where AMBU bags remain indispensable. A manual AMBU bag should always be available as a backup in case of malfunction or power failure. Furthermore, user training and familiarization are essential; structured teaching should be incorporated into BLS/ALS curricula.
The study highlights significant differences between Airgency and medical professionals in delivering consistent resuscitation parameters. Airgency demonstrated superior consistency with minimal variability in breathing rate (BR), tidal volume (VT), and peak inspiratory pressure (PIP) compared to medical professionals, whose performance exhibited considerable fluctuations. Over the 30-minute resuscitation period, Airgency achieved more stable and precise delivery of ventilation parameters, as evidenced by lower coefficients of variation. Additionally, medical professionals experienced increasing fatigue over time, which may have contributed to their variability in performance. These findings suggest that automated systems like Airgency could enhance the reliability of manual resuscitation by reducing variability and mitigating the effects of operator fatigue.
However, the study's limitations underscore the need for further research in real-world settings and over extended durations to fully evaluate the clinical impact of Airgency's performance.
7. Data availability
The datasets generated and/or analysed during current study are not publicly available
8. Conflict of Interest
The authors declared no conflict of interests.
9. Funding
This work did not receive any funding from governmental or institutional sources.
10. Acknowledgement
The authors express their sincere gratitude to Ruli Herman Sitanggang, MD(Anest.), M.PH, Ike Sri Redjeki, MD(Anest.), M.PH, Ph.D., Erwin Pradian, MD(Anest.), M.PH, Ph.D., Suwarman, MD(Anest.), M.PH, Ph.D., Nurita Dian Kestriani, MD(Anest.) from Department of Anesthesiology and Intensive Care Therapy, and Gilang Yubiliana, DMD, M.PH, Ph.D. from Department of Dentistry, Padjadjaran University, Bandung, Indonesia for their valuable contribution during data acquisition process.
11. Authors contribution
Reza Widianto Sudjud: Conceptualisation, Resources, Methodology, Data Curation, Writing – Review & Editing; Jenifer Kiem Aviani: Writing – original draft, Writing – Review & Editing, Visualisation, Formal Analysis;
Authors affiliations:
- Reza Widianto Sudjud, MD, M.PH, Ph.D. Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia. Email: widianto.sudjud@unpad.ac.id; {ORCID:0000-0001-5966-4846}
- Jenifer Kiem Aviani, B.Sc., M.Sc. Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University. Email: jenifer_kiem@yahoo.co.id
- Ruli Herman Sitanggang, MD, M.PH, Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia; Email: herman.sitanggang@unpad.ac.id
- Ike Sri Redjeki, MD, M.PH, Ph.D. (†), Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia; Email: tpauncen2022@gmail.com
- Erwin Pradian, MD, M.PH, Ph.D., Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia; Email: pradian@unpad.ac.id
- Suwarman, MD, M.PH, Ph.D., Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia; Email: suwarman@unpad.ac.id
- Nurita Dian Kestriani, MD, Department of Anesthesiology & Intensive Care, Faculty of Medicine, Padjadjaran University / Dr. Hasan Sadikin Central General Hospital, Bandung, Indonesia; Email: dian@unpad.ac.id
ABSTRACT
Background & Objectives: This study evaluates the performance of AirgencyTM, an automated Ambu-bag resuscitator manufactured by Institut Teknologi Bandung and Padjadjaran University, Indonesia, against manual resuscitation using a simulation model to address these limitations.Methodology: The study compared breathing rate (BR), tidal volume (VT), and peak inspiratory pressure (PIP) delivered by AirgencyTM and 50 medical professionals during a controlled 30-minute resuscitation session. Variability in performance was assessed using the coefficient of variation, while fatigue in medical professionals was measured using the Visual Analog Scale for Fatigue (VAS-F).
Results: AirgencyTM demonstrated significantly lower variability in all parameters compared to medical professionals (P < 0.0001). While medical professionals exhibited significant variability in BR (27.6%), VT (26.4%), and PIP (25.2%), AirgencyTM demonstrated minimal fluctuations, with coefficients of variation under 3% for all parameters. Fatigue among medical professionals increased significantly over the resuscitation period, with median VAS-F scores rising from 1 to 5.
Conclusion: AirgencyTM consistently outperformed medical professionals in maintaining precise ventilation parameters with minimal variability. These results suggest that automated devices like AirgencyTM may enhance the reliability of resuscitation efforts, particularly in mitigating the impact of operator fatigue. However, further studies in real-world settings are necessary to confirm these findings.
Abbreviations: BR: breathing rate, PIP: peak inspiratory pressure, VAS-F: Visual Analog Scale for Fatigue,
Keywords: bag-valve manual resuscitation machine; breathing rate; tidal volume; peak inspiratory pressure; fatigue.
Citation: Sudjud RW, Aviani JK, Sitanggang RH, Redjeki IS, Pradian E, Suwarman, Kestriani ND. Simulation-based assessment of AirgencyTM: a novel automatic resuscitator for emergency respiratory support Anaesth. pain intensive care 2025;29(9):1196-1203. DOI: 10.35975/apic.v29i9.3060
Received: August 17, 2025; Revised: September 05, 2025; Accepted: September 06, 2025
1. INTRODUCTION
Respiratory failure is a critical disruption of the respiratory system, particularly in the regulation of gas exchange. It is a leading cause of morbidity and mortality among patients in intensive care units. This condition can lead to various complications, including lung failure, hypoxemia, pump failure, alveolar hypoventilation, and hypercapnia.1
During pandemics, the demand for ventilators rises significantly. Reflecting on the recent COVID-19 pandemic, there was a notable disparity between the high admission rates to critical care units and the limited availability of ventilators. Most hospitals had minimal or no surplus ventilators to address the surge in demand caused by disasters or pandemics. However, the high cost of ventilators makes it impractical for healthcare facilities to maintain large reserves. This highlights the pressing need for a simple, cost-effective, yet efficient respiratory support system to address such crises effectively.2
Among the available modalities for respiratory support, the Ambu bag (manual resuscitator) plays a critical role in emergency scenarios. Unlike high-flow nasal cannulas (HFNC), which provide non-invasive oxygen delivery for patients with intact respiratory drive, or mechanical ventilators, which offer precise, long-term support for critically ill patients, the Ambu bag is uniquely suited for immediate and temporary respiratory assistance. Its portability, ease of use, and independence from external power sources make it indispensable in acute settings, especially during resuscitation or transportation of patients. While nasal cannulas and ventilators require specific conditions and setups, the Ambu bag serves as a rapid-response tool that bridges the gap between initial intervention and advanced respiratory management.3
Despite of its simplicity, Ambu bag have been liked to injuries such as gastric insufflation, aspiration, and pneumothorax from hyperventilation. Its effectiveness depends heavily on skilled operators and consistent manual effort, which can be challenging to sustain in prolonged or high-demand situations, such as mass casualties or pandemics. Studies have shown that even the highly skilled operators with high level of experience are prone to hyperventilate patients due to fatigue.4
The development of Airgency, an automatic Ambu-bag resuscitator machine, manufactured by Institut
Teknologi Bandung and Padjadjaran University, Indonesia, offers a transformative solution by automating the manual ventilation process. AirgencyTM ensure consistent, controlled ventilation while reducing the risk of human error and operator fatigue. Moreover, they are cost-effective and portable, making them particularly valuable in resource-limited settings or during large-scale emergencies when advanced mechanical ventilators are unavailable or in short supply. By combining simplicity, reliability, and efficiency, AirgencyTM have the potential to bridge the gap between manual resuscitation and sophisticated ventilators, improving outcomes for patients with respiratory failure in diverse clinical and disaster scenarios. Current study aims to evaluate the performance of AirgencyTM in comparison to manual human resuscitation using an adult Manikin-based simulation model.
2. METHODOLOGY
2.1. Product Details
Figure 1 illustrates the design and components of the Airgency device. Airgency is a compact and lightweight unit, measuring 21 x 24 x 31 cm and weighing 3 kg. To operate the device, the casing is opened by moving the left and right case handles outward. The Ambu-bag is then placed securely on the Ambu-bag stand, positioned between the presser arms, and fastened into place. All resuscitator components are subsequently attached to the Ambu-bag, and the airflow sensor tube is connected to the Airgency module. The casing is then moved inward to lock the Ambu-bag securely in position. Next, the adaptor cable is connected to the Airgency power supply port and a 200-400 VAC, 50/60 Hz power source. The device is then powered on using the switch. The breathing parameters can then be adjusted with the following configurable settings:
- Tidal volume: 200 – 500 mL
- Inspiration / Expiration (I/E) Ratio: 1:1, 1:2, 1:3
- Breathing Rate: 10 – 20 breathe per minute
- Operating Mode: Normal & Assisted mode
The Assisted Mode supports patients in achieving the set respiratory parameters. In this mode, the patient’s inspiratory effort serves as the trigger to initiate the machine’s cycle, making it appropriate for patients with limited or insufficient spontaneous breathing. System failure is detected if the patient does not initiate an inspiratory effort within 10 seconds. The indicator LED displays the operational status of the device: it illuminates green during Normal Mode and yellow during Assisted Mode. In the event of a system failure, the LED will turn red to signal the error.
During patient transfers, the device can operate independently of an external power source, as it is equipped with a built-in 5200mAh battery, providing up to 2 hours of continuous operation. The indicator LED illuminates green when the device is connected to an external power source and red when operating on battery power.
Figure 1: Picture of Airgency (A) closed, (B) opened (C) control panel and (D) supporting components
2.2. Experiment Setting
2.2.1. Manikin Simulation Setting
A respiratory adult Manikin was connected to an automated test lung to monitor ventilation parameters. An Ambu-bag mask was positioned over the Manikin's nose and mouth. Respiratory resuscitation was then performed for 30 minutes, either using the Airgency device or manually by medical professionals.
2.2.2. AirgencyTM Settings
The Airgency device was configured to operate in normal mode, with a tidal volume of 400 mL (selected based on lung-protective ventilation guidelines of 6–8 mL/kg for an average 60–70 kg adult, corresponding to approximately 6 mL/kg), I/E Ratio 1:1, and a breathing rate of 15 breaths per minute (reflecting the normal adult physiologic rate and consistent with BLS/resuscitation guidelines) . The resuscitation procedure was repeated 50 times.
2.2.3. Medical Professionals Control Group
Fifty medical professionals were recruited for the study based on the following inclusion criteria: (1) enrollment in an anesthesiology residency program (PGY-3 to PGY-4), (2) a body mass index (BMI) between 18.5 and 24.99, (3) possession of a valid Basic Life Support (BLS) certification, and (4) being in good physical health at the time of participation.
Each participant was instructed to perform respiratory resuscitation for 30 minutes, maintaining a breathing rate of 15 breaths per minute (bpm). While grip strength was not measured, all participants held valid BLS certification and had prior exposure to manual ventilation as part of training. We have acknowledged this as a limitation regarding variability.
2.3. Outcome Measure
Breathing rate, tidal volume (VT), and peak inspiratory pressure (PIP) were measured every minute using pressure and flow transducers connected to the test lung. The coefficient of variation for each minute's measurements was calculated to assess stability within each group. Operator fatigue was assessed using the Visual Analog Scale for Fatigue (VAS-F), a 10-point scale where 1 indicates no fatigue and 10 indicates extreme fatigue. The mean values of the collected data are presented as a line plot for visualization.
2.4. Statistical Analysis
Statistical analysis was conducted using GraphPad Prism version 10.1.2. An Independent T-Test was used to evaluate differences between groups. Additionally, Multiple Independent T-Tests with the Benjamini, Krieger, and Yekutieli method for controlling the false discovery rate (FDR) at a 5% threshold were performed to assess differences between the two groups at each time point. A P < 0.05 was considered statistically significant.
3. RESULTS
Here, we offer an outline of the various features,
3.1. Breathing Rate
There were no significant differences in the breathing rate per time frame during resuscitation performed by Airgency and medical professionals. However, over the entire 30-minute period, the mean breathing rate showed a significant difference (P = 0.0170), with Airgency achieving a rate of 14.77 ± 0.07 bpm compared to 14.52 ± 4.00 bpm for medical professionals (Figure 2A).
Figure 2 (A): AirgencyTM achieved a rate of 14.77 ± 0.07 bpm compared to 14.52 ± 4.00 bpm for medical professionals
The breathing rate delivered by medical professionals exhibited considerable variability within each time frame, ranging from 18.0% to 36.1% (mean = 27.6%). In contrast, AirgencyTM demonstrated minimal variability across 50 repetitions, with fluctuations between 0.4% and 1.1% (mean = 0.7%). The coefficient of variation between the two groups was significantly different (P < 0.0001) (Figure 2B).
Figure 2 (B): Shows the coefficient of variation between the two groups
3.2. Tidal Volume (VT)
Significant differences were observed in the tidal volume (VT) achieved during resuscitation performed by AirgencyTM compared to medical professionals across each time frame. Over the entire 30-minute period, the mean VT delivered by AirgencyTM was 397.36 ± 3.52 mL, whereas the VT delivered by medical professionals was 353.6 ± 111.75 mL (P = 0.0006) (Figure 3A).
Figure 3 (A): Mean VT delivered by AirgencyTM was more than the VT delivered by medical professionals (P = 0.0006)
The VT delivered by 50 medical professionals showed considerable variability within each time frame, ranging from 13.5% to 153.2% (mean = 26.4%). In contrast, the VT delivered by AirgencyTM exhibited minimal fluctuation across 50 repetitions, ranging from 0.5% to 3.3% (mean = 0.9%) (P < 0.0001) (Figure 3B).
Figure 3 (B) VT delivered by AirgencyTM exhibited minimal fluctuation across 50 repetitions
3.3. Peak Inspiratory Pressure (PIP)
Significant differences in peak inspiratory pressure (PIP) were observed over the entire 30-minute observation period (Figure 4A). The mean PIP generated by AirgencyTM was 29.78 ± 0.84 cm H₂O, whereas the PIP achieved through manual resuscitation by medical professionals was 24.07 ± 6.33 cm H₂O (P < 0.0001).
Figure 4 (A): The mean PIP generated by AirgencyTM was higher than achieved through manual resuscitation by medical professionals (P < 0.0001).
The PIP delivered by medical professionals exhibited substantial variability within each time frame, ranging from 15.4% to 128.9% (mean = 25.2%). In contrast, the PIP delivered by AirgencyTM demonstrated minimal fluctuations, ranging from 1.0% to 6.6% (mean = 2.8%) (P < 0.0001) (Figure 4B).
Figure 4 (B) AirgencyTM demonstrated minimal fluctuations (P < 0.0001)
3.4. Fatigue Level
Medical professionals exhibited increasing fatigue over the course of the 30-minute resuscitation procedure, as illustrated in Figure 5. During the initial 9 minutes, the median VAS-F score remained at 1, indicating minimal fatigue. However, by the end of the procedure, the median score had risen to 5, reflecting significant fatigue.
Figure 5: Comparative fatigue onset in the two groups
4. DISCUSSION
The findings of this study highlight the superior performance and consistency of AirgencyTM compared to manual resuscitation performed by medical professionals, particularly in critical metrics such as breathing rate, tidal volume (VT), and peak inspiratory pressure (PIP).
Respiratory rate is a critical parameter in ventilation, as excessively high rates can lead to hyperventilation, respiratory alkalosis, and insufficient expiratory time. Conversely, rates that are too low risk inadequate ventilation and respiratory acidosis.5 Both AirgencyTM and medical professionals achieved an appropriate respiratory rate, targeted at 15 breaths per minute, which aligns with the normal physiological and comfortable breathing rate.6 However, deviations were observed among medical professionals, with rates dropping to 8 breaths per minute at the 11th minute and increasing to 21 breaths per minute at the 16th minute. Despite these fluctuations, the rates remained within the range of normal breathing.7
Tidal volume (VT) is a vital parameter during resuscitation, as it must be sufficient to overcome anatomical dead space and ensure effective ventilation. Insufficient tidal volumes can lead to atelectasis, while excessively high volumes may result in hyperventilation and increase the risk of lung injury.7 AirgencyTM demonstrated superior performance in achieving the targeted tidal volume of 400 mL, with an average of 397 ± 3.52 mL over a 30-minute resuscitation period and a low variability of 0.9%. In contrast, human resuscitation achieved only 88.4% of the desired VT, delivering an average of 314.96 ± 65.25 mL (78.7%) during the first minute of resuscitation. Instances of hyperventilation were observed during human resuscitation at the 12th and 24th minutes, with tidal volumes exceeding 1300 mL. A low tidal volume of 6–8 mL/kg of ideal body weight is generally recommended during initial resuscitation, as evidence suggests it is associated with reduced pulmonary complications in patients without acute respiratory distress syndrome (ARDS).7,9,10 For this study, a target tidal volume of 400 mL was chosen, assuming an average adult body weight of 60–70 kg and a tidal volume of 6 mL/kg.
Peak inspiratory pressure (PIP) refers to the maximum pressure exerted on the lungs during inhalation. It is influenced by airway resistance, and elevated PIP levels can indicate underlying issues such as excessive secretions, bronchospasm, occlusion from biting down on ventilation tubing, or reduced lung compliance. Prolonged PIP levels exceeding 40 cm H₂O should generally be avoided, except in cases of acute respiratory distress syndrome (ARDS), where higher pressures may be required to maintain adequate ventilation.10 Both Airgency and manual resuscitation resulted in peak inspiratory pressure (PIP) levels that remained below 30 cm H₂O for most of the 30-minute observation period. However, a transient spike in PIP up to 70 cm H₂O was observed during manual resuscitation at the 11th minute, lasting for one minute. Despite this brief elevation, the PIP levels achieved during both human and Airgency resuscitation were generally within the safe range. Nevertheless, the significant inter variability in PIP during manual resuscitation is a critical point of concern, as it may lead to either insufficient ventilation or hyperventilation, potentially compromising patient safety and outcomes.
Manual hyperventilation can elevate intrathoracic pressure, leading to adverse hemodynamic effects, including reduced venous return (VR), cardiac output (CO), and coronary perfusion pressure (CPP). Furthermore, elevated inspiratory pressures may compromise the lower esophageal sphincter, resulting in gastric insufflation, regurgitation, and aspiration. Excessive manual ventilation can also cause acute barotrauma, manifesting as pneumothorax, pneumomediastinum, pneumoperitoneum, or subcutaneous emphysema. Additionally, sub-barotraumatic lung injuries driven by inflammation may occur due to aggressive ventilation.8
The primary challenge in human resuscitation lies in the significant variability in performance across individuals and over time. Scott et al. (2020) demonstrated that male operators delivered higher tidal volumes compared to female operators. Additionally, operators wearing medium-sized gloves delivered lower tidal volumes compared to those wearing small or large gloves.11 Li et al. (2018) reported that experienced clinicians provided smaller tidal volumes (VT) and higher breathing rates (BR).12 Culbreth and Gardenhire (2021) found a correlation between delivered tidal volumes, peak pressures, years of experience, and the operator's confidence level.13 Khoury et al. observed that excessive ventilation was influenced by rapid bag refilling, which could trigger a reflexive squeeze and ventilation response as soon as the bag reinflates. They also noted that hyperventilation was associated with high grip strength, where excessive insufflation volumes were mitigated by significant air leaks.15 Moreover, the technique used for bag ventilation, such as employing one-hand versus two-hand methods, can significantly affect tidal volume delivery.15 To enhance control over delivered tidal volume (VT), breathing rate (BR), and peak inspiratory pressure (PIP), some groups have developed feedback monitoring systems. These systems have been shown to significantly improve the accuracy of these parameters.8
Muscle fatigue is a significant issue during manual resuscitation, as it can lead to ventilation inconsistencies, as highlighted in several studies.16-19 Our study observed an increase in fatigue levels over time; however, the median fatigue level during a 30-minute resuscitation session was still categorized as mild. Bergrath et al. reported a median fatigue score of 6 out of 10 during 3 hours of bag-valve-mask (BVM) resuscitation.16 Similarly, Halpern et al. documented an increase in Borg's Perceived Exertion and Pain Scale from 6.4 (very light effort) to 10.2 (fairly light effort) over 6 hours of manual resuscitation. This rise in perceived exertion may be attributed more to boredom than to physical fatigue during prolonged resuscitation periods.19
This study has several limitations. First, the variability in manual resuscitation performance by medical professionals may be influenced by factors such as experience level, physical fitness, and training background, which were not detailed in this study. Second, Airgency’s performance was evaluated in a manikin-based simulation under controlled conditions, which may not fully replicate the challenges encountered in clinical or emergency settings, such as patient movement, distractions, or device malfunctions. Third, fatigue levels in medical professionals were assessed using a subjective scale (VAS-F), potentially introducing bias or inconsistency in reporting. Fourth, the study focused on a 30-minute duration, which, while appropriate for an acute resuscitation scenario, does not address the long-term reliability and consistency of Airgency under extended use. Lastly, only three parameters were evaluated in this study, which may not adequately reflect the broader impact on patient physiology. In practical application, Airgency™ requires an oxygen source or power supply, which may limit use in field emergencies where AMBU bags remain indispensable. A manual AMBU bag should always be available as a backup in case of malfunction or power failure. Furthermore, user training and familiarization are essential; structured teaching should be incorporated into BLS/ALS curricula.
5. CONCLUSION
The study highlights significant differences between Airgency and medical professionals in delivering consistent resuscitation parameters. Airgency demonstrated superior consistency with minimal variability in breathing rate (BR), tidal volume (VT), and peak inspiratory pressure (PIP) compared to medical professionals, whose performance exhibited considerable fluctuations. Over the 30-minute resuscitation period, Airgency achieved more stable and precise delivery of ventilation parameters, as evidenced by lower coefficients of variation. Additionally, medical professionals experienced increasing fatigue over time, which may have contributed to their variability in performance. These findings suggest that automated systems like Airgency could enhance the reliability of manual resuscitation by reducing variability and mitigating the effects of operator fatigue.
6. LIMITATIONS
However, the study's limitations underscore the need for further research in real-world settings and over extended durations to fully evaluate the clinical impact of Airgency's performance.
7. Data availability
The datasets generated and/or analysed during current study are not publicly available
8. Conflict of Interest
The authors declared no conflict of interests.
9. Funding
This work did not receive any funding from governmental or institutional sources.
10. Acknowledgement
The authors express their sincere gratitude to Ruli Herman Sitanggang, MD(Anest.), M.PH, Ike Sri Redjeki, MD(Anest.), M.PH, Ph.D., Erwin Pradian, MD(Anest.), M.PH, Ph.D., Suwarman, MD(Anest.), M.PH, Ph.D., Nurita Dian Kestriani, MD(Anest.) from Department of Anesthesiology and Intensive Care Therapy, and Gilang Yubiliana, DMD, M.PH, Ph.D. from Department of Dentistry, Padjadjaran University, Bandung, Indonesia for their valuable contribution during data acquisition process.
11. Authors contribution
Reza Widianto Sudjud: Conceptualisation, Resources, Methodology, Data Curation, Writing – Review & Editing; Jenifer Kiem Aviani: Writing – original draft, Writing – Review & Editing, Visualisation, Formal Analysis;
11. REFERENCES
- Lamba TS, Sharara RS, Singh AC, Balaan M. Pathophysiology and classification of respiratory failure. Crit Care Nurs Q. 2016;39(2):85-93. [PubMed] DOI: 1097/CNQ.0000000000000102
- L'Her E, Roy A. Bench tests of simple, handy ventilators for pandemics: performance, autonomy, and ergonomy. Respir Care. 2011;56(6):751-60. [PubMed] DOI: 4187/respcare.00841
- Jonkman AH, Katira BH, Schreiber A, et al. A Gas-Powered, Patient-Responsive Automatic Resuscitator for Use in Acute Respiratory Failure: A Bench and Experimental Study. Respir Care. 2021;66(3):366-77. [PubMed]DOI: 4187/respcare.08296
- Merrell JG, Scott AC, Stambro R, Boukai A, Cooper DD. Improved simulated ventilation with a novel tidal volume and peak inspiratory pressure controlling bag valve mask: A pilot study. Resusc Plus. 2023;13:100350. [PubMed] DOI: 1016/j.resplu.2022.100350
- Rittayamai N, Katsios CM, Beloncle F, Friedrich JO, Mancebo J, Brochard L. Pressure-Controlled vs Volume-Controlled Ventilation in Acute Respiratory Failure: A Physiology-Based Narrative and Systematic Review. Chest. 2015;148(2):340-55. [PubMed] DOI: 1378/chest.14-3169
- Taniguchi C, Eid RC, Saghabi C, Souza R, Silva E, Knobel E, et al. Automatic versus manual pressure support reduction in the weaning of post-operative patients: a randomised controlled trial. Crit Care. 2009;13(1):R6. [PubMed] DOI: 1186/cc7695
- Neto AS, Simonis FD, Barbas CS, et al. Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: A systematic review and individual patient data analysis. Crit Care Med. 2015;43(10):2155-63. [PubMed] DOI:1097/CCM.0000000000001189
- White LA, Conrad SA, Alexander JS. Pathophysiology and Prevention of Manual-Ventilation-Induced Lung Injury (MVILI). Pathophysiology. 2024;31(4):583-95. [PubMed] DOI: 3390/pathophysiology31040042
- Guay J, Ochroch EA, Kopp S. Intraoperative use of low volume ventilation to decrease postoperative mortality, mechanical ventilation, lengths of stay and lung injury in adults without acute lung injury. Cochrane Database Syst Rev. 2018;7(7):CD011151. [PubMed] DOI:1002/14651858.CD011151.pub3
- Rose L. Clinical application of ventilator modes: Ventilatory strategies for lung protection. Aust Crit Care. 2010;23(2):71-80. [PubMed] DOI: 1016/j.aucc.2010.03.003
- Scott JB, Schneider JM, Schneider K, Li J. An evaluation of manual tidal volume and respiratory rate delivery during simulated resuscitation. Am J Emerg Med. 2021;45:446-50. [PubMed] DOI: 1016/j.ajem.2020.09.091
- Li J, Mohn T, Schenider K, Scheinder J, Scott J. Tidal volume and respiratory rate assessment during manual ventilation. Crit Care Med. 2019;47(1):459. [PubMed]
- Culbreth RE, Gardenhire DS. Manual bag valve mask ventilation performance among respiratory therapists. Heart Lung. 2021;50(3):471-5. [PubMed] DOI: 1016/j.hrtlng.2020.10.012
- Khoury A, De Luca A, Sall FS, Pazart L, Capellier G. Ventilation feedback device for manual ventilation in simulated respiratory arrest: a crossover manikin study. Scand J Trauma Resusc Emerg Med. 2019;27(1):93. [PubMed] DOI: 1186/s13049-019-0674-7
- Hart D, Reardon R, Ward C, Miner J. Face mask ventilation: a comparison of three techniques. J Emerg Med. 2013;44(5):1028-1033. [PubMed] DOI:1016/j.jemermed.2012.11.005
- Bergrath S, Rossaint R, Biermann H, et al. Comparison of manually triggered ventilation and bag-valve-mask ventilation during cardiopulmonary resuscitation in a manikin model. Resuscitation. 2012;83(4):488-493. [PubMed] DOI: 1016/j.resuscitation.2011.09.010
- Bauman EB, Joffe AM, Lenz L, DeVries SA, Hetzel S, Seider SP. An evaluation of bag-valve-mask ventilation using an ergonomically designed facemask among novice users: a simulation-based pilot study. Resuscitation. 2010;81(9):1161-5. [PubMed] DOI:1016/j.resuscitation.2010.05.005
- Riggle JD, McCrory B, Wadman M, Miller E, Balogh B, Cao V, et al. Riggle JD, McCrory B, Wadman M, et al. Comparison of muscle exertion and fatigue between standard bag valve mask and NuMask. Proc Hum Factors Ergon Soc Annu Meet. 2012;56(1):892-896. DOI: 1177/1071181312561187
- Halpern P, Dang T, Epstein Y, Van Stijn-Bringas Dimitriades D, Koenig KL. Six Hours of Manual Ventilation With a Bag-Valve-Mask Device Is Feasible and Clinically Consistent. Crit Care Med. 2019;47(3):e222-e226. [PubMed] DOI: 1097/CCM.0000000000003632