Safya E. Esmaeel 1 , Haba Mofareh Alhumaidi Alanazi 2 , Hajar Hamed Mosharek Alruwaili 3 , Wahj Radi M. Alenezi 4 , Dala Naif M Alenzi 5 , Eslam K.Fahmy 6 , Baraah Abu Alsel 7 , Manal S. Fawzy 8*
Authors affiliations:
Background & objective: This study aimed to systematically assess the prevalence of ventilator-associated pneumonia (VAP) among intensive care unit (ICU) patients in Saudi Arabia and to evaluate the impact of preventive interventions.
Methodology: A systematic search of PubMed, Scopus, Web of Science, and regional databases identified 364 studies (2000–2023). After duplicate removal and screening, four studies (n = 4247 patients; 64.7% male) met the inclusion criteria. Data extraction and quality assessment were performed using Rayyan QCRI and PRISMA guidelines.
Results: VAP prevalence in Saudi ICUs varied widely, ranging from 2.2% to 35.4%, with a pooled prevalence of 12%. Implementation of structured preventive measures, particularly ventilator care bundles, was consistently associated with reduced VAP incidence, shorter durations of mechanical ventilation, decreased hospital stays, and improved patient outcomes. Despite these improvements, differences in study design and reporting continue to limit direct comparisons across centers.
Conclusion: VAP remains a significant concern in Saudi Arabian ICUs, with prevalence rates higher than some international benchmarks. Preventive strategies, especially care bundles, are effective but require ongoing adaptation to local contexts. Further research should focus on standardizing surveillance, evaluating long-term intervention effectiveness, and identifying region-specific risk factors to optimize patient care and resource utilization.
Abbreviations: ICU: intensive care unit, VAP: ventilator-associated pneumonia,
Keywords: Ventilator-associated pneumonia; Intensive care unit; Critically ill patients; Saudi Arabia; Systematic review.
Citation: Esmaeel SE, Alanazi HM, Alruwaili HH, Alenezi WR, Alenzi DN, Fahmy EK, Abu Alsel BT, Fawzy MS. Prevalence of ventilator-associated pneumonia (VAP) in patients admitted to intensive care units in Saudi Arabia: a systematic review. Anaesth. pain intensive care 2025;29(8):1014-1021. DOI: 10.35975/apic.v29i8.3032.
Received: May 09, 2025; Revised: October 06, 2025; Accepted: October 06, 2025
Ventilator-associated pneumonia (VAP), also known as intubation-associated pneumonia, is defined as pneumonia occurring more than 48-72 hours after endotracheal intubation, provided it was not incubating at the time of admission.1,2 Clinically, VAP is characterized by new or progressive pulmonary infiltrates, systemic signs of infection, and alterations in the characteristics of sputum.3 It represents one of the most frequent and severe nosocomial infections among patients admitted to intensive care units (ICUs), significantly contributing to patient morbidity and mortality.1-4 VAP-related mortality rates range widely from 24% to 76% across various international settings.5,6
The Institute of Medicine has identified the prevention of hospital-acquired infections, including VAP, as a national healthcare priority due to their substantial impact on patient outcomes and healthcare resources.7,8 Patients diagnosed with VAP experience prolonged hospital stays and increased healthcare costs, placing additional burdens on healthcare systems.9,10 Globally, the reported incidence of VAP among ICU populations varies considerably, ranging from 8.0% to 28.8%, reflecting differences in healthcare practices, infection control measures, patient populations, and microbial environments.11-13
Future research should prioritize standardizing surveillance, assessing the long-term effectiveness of interventions, and identifying region-specific risk factors to optimize patient care and resource allocation.14,15 Although several individual studies have examined VAP incidence in various Saudi Arabian hospitals or regions, a systematic synthesis of these data at the national level remains limited.16 Previous multi-hospital surveillance reports from Saudi Arabia have been published; however, these reports lack sufficient representativeness and methodological rigor to estimate national prevalence rates accurately.17,18 Consequently, there is a critical knowledge gap regarding the true burden of VAP across Saudi Arabian ICUs.
Addressing this gap through a comprehensive systematic review is essential for accurately quantifying the VAP prevalence in Saudi Arabia. Such an approach will facilitate an improved understanding of regional variations in risk factors and microbial profiles associated with VAP. Furthermore, synthesizing existing data can inform targeted preventive strategies aimed at reducing the incidence of VAP, optimizing resource allocation within ICUs, and ultimately improving patient outcomes nationwide.19,20 In this sense, the principal objective of this systematic review is to critically evaluate and consolidate available evidence regarding the prevalence of ventilator-associated pneumonia among ICU patients throughout Saudi Arabia.
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines21 and the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).22 The protocol was registered with the International Platform of Registered Systematic Review and Meta-Analysis (INPLASY), with the registration number: NPLASY202530042. A thorough search strategy was developed to identify relevant studies investigating the VAP prevalence among ICU patients in Saudi Arabia. From the start to the date of this review, four electronic databases, PubMed, Scopus, Web of Science, and Cochrane Library, were methodically searched. The search terms included combinations of keywords and medical subject headings (MeSH), such as ventilator-associated pneumonia (VAP), mechanical ventilation, intensive care unit (ICU), prevalence, incidence, and Saudi Arabia. No language/publication date restrictions were applied.
After removing duplicates, all retrieved titles and abstracts were imported into Rayyan QCR, a software tool for initial screening. Two independent coauthors screened the titles and abstracts to identify potentially eligible studies. The full texts of these studies were then retrieved and independently assessed by the same coauthors against predefined inclusion criteria. Any discrepancies or disagreements regarding study eligibility were resolved through consensus discussions or, when necessary, consultation with a third reviewer.
Studies were selected based on clearly defined Population-Exposure-Outcome (PEO) criteria: (i) Population: adult patients (≥18 years old) admitted to intensive care units (ICUs) in hospitals across Saudi Arabia, (ii) Exposure: patients receiving mechanical ventilation during their ICU admission, and (iii) Outcome: studies reporting data on the occurrence, or prevalence /incidence of VAP among mechanically ventilated ICU patients. Studies were excluded if they involved pediatric populations, did not explicitly report VAP prevalence/incidence, or were conducted outside Saudi Arabia. Additionally, case reports, letters, editorials, reviews without original data, conference abstracts without full-text availability, and studies lacking sufficient data for extraction were excluded.
Two independent coauthors extracted data from publications that matched the inclusion criteria using a predetermined/consistent methodology and a standardized data extraction form designed specifically for this review. The extracted data included: (i) Name of the first author; (ii) Publication year; (iii) Study design; (iv) Sample size (number of participants); (v) Participant demographics (age range or mean age; gender distribution); (vi) Prevalence/incidence rates of VAP (%); and (viii) Key findings related to risk factors and preventive interventions. Discrepancies in extracted data between coauthors were resolved through discussion until a consensus was reached.
The methodological quality and risk of bias in included studies were evaluated using the Risk Of Bias In Non-randomized Studies–of Interventions (ROBINS-I) assessment tool. This tool provides a structured framework for assessing bias across seven domains: confounding factors, selection bias, classification bias regarding interventions/exposures, deviations from intended interventions/exposures, missing data bias, measurement bias in outcomes assessment, and selective reporting bias. Two independent coauthors assessed each study independently using these criteria. Disagreements regarding risk-of-bias ratings were resolved through discussion or consultation with a third coauthor.23
Extracted data were synthesized narratively due to anticipated heterogeneity in study designs and outcome measurements among included studies Prevalence estimates were summarized descriptively. Key findings related to preventive interventions and associated outcomes (e.g., morbidity, mortality) are presented narratively to provide comprehensive insights into VAP prevalence and management practices within Saudi Arabian ICUs.
The targeted search approach produced 364 publications (Figure 1). Then, the removal of duplicates (n = 160) and 204 trials were assessed using the abstract and title. One hundred sixty-eight of these did not meet the qualifying requirements; therefore, only 50 full-text publications remained for thorough evaluation. Four in all met the eligibility standards for analysis using evidence synthesis.
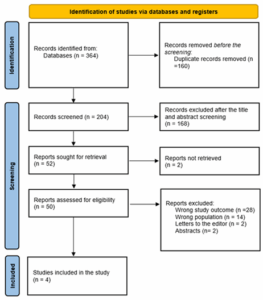
Figure 1: PRISMA flowchart
Four studies involving a total of 4,247 ICU patients met the inclusion criteria for qualitative synthesis. Among these patients, 2,749 (64.7%) were males. Regarding study designs, three studies utilized prospective cohort methodologies,24-26 while one study employed a case-control design.27 All four studies were conducted in Riyadh City hospitals between 2004 and 2017.24-27
The reported prevalence of ventilator-associated pneumonia (VAP) among critically ill patients in Saudi Arabia ranged widely from 2.2% to 35.4%,24-27 with an overall pooled prevalence of 12% (510 cases). Key findings from the included studies provided important insights into the prevalence trends of VAP and associated clinical outcomes. One study observed a declining trend in VAP rates over time, suggesting the effectiveness of targeted preventive interventions and improved healthcare practices in reducing infection incidence.24
Another study underscored the benefits of implementing structured care protocols, particularly ventilator care bundles, in reducing VAP incidence and optimizing ventilator utilization. These protocol-driven approaches demonstrated the potential to decrease hospital-acquired infections and improve resource management within ICU settings.25
Further analysis indicated that VAP was consistently associated with prolonged durations of mechanical ventilation, increased length of hospital stays, and elevated morbidity and mortality rates among affected patients. These findings underscore the substantial clinical burden imposed by VAP on both patient outcomes and healthcare resources, emphasizing the critical need for effective preventive strategies to mitigate these adverse impacts.27
Lastly, extended ICU stays attributed to VAP were strongly correlated with significantly higher morbidity rates and hospital mortality. This association highlights severe complications arising from prolonged critical care exposure due to VAP, further reinforcing the importance of early detection, timely intervention, and comprehensive infection prevention measures within ICU settings.26
This systematic review aimed to critically evaluate and synthesize existing evidence regarding the prevalence of VAP among ICU patients in Saudi Arabia. Our findings indicate substantial variability in VAP prevalence across studies, highlighting a significant healthcare challenge within Saudi ICUs. The reviewed studies collectively underscore the clinical burden imposed by VAP, including prolonged durations of mechanical ventilation, increased ICU/hospital stays, and elevated morbidity and mortality rates. Importantly, structured preventive interventions, particularly ventilator care bundles, appear effective in reducing VAP incidence and optimizing resource utilization. Despite these promising results, the variability observed emphasizes the necessity of tailoring preventive strategies to local contexts. To our knowledge, this is the first systematic review consolidating national data on VAP prevalence in Saudi Arabia, providing critical insights that could inform future healthcare policies, clinical practices, and targeted preventive strategies.
Recent evidence underscores the persistent challenge of VAP in modern intensive care settings.28 Alnimr's comprehensive review highlighted that despite advances in critical care medicine, VAP remains a significant concern with far-reaching consequences for patient outcomes.29 Of particular concern is the growing association between VAP and antibiotic-resistant pathogens, which substantially increases patient morbidity, mortality, and healthcare expenditures.29-31
This alarming trend emphasizes why VAP prevention must remain a clinical priority.32 When VAP does occur, early and appropriate antibiotic therapy becomes crucial, not only to improve patient outcomes but also to minimize the emergence of resistant microorganisms that further complicate treatment.29,33 Hassan and colleagues reinforced these concerns, noting that VAP significantly extends ICU stays and elevates mortality rates, creating additional strain on healthcare systems, particularly in resource-limited settings.5
Our systematic review revealed considerable variability in VAP prevalence among critically ill patients in Saudi Arabia, with rates ranging from as low as 2.2%34 to as high as 35.4%35, yielding an overall prevalence of 12% (510 cases). These findings gain perspective when compared with international data. North American hospitals typically report remarkably low VAP incidence, between 1 and 2.5 cases per 1000 ventilator days.1,7,36 European healthcare facilities, however, demonstrate substantially higher rates, exemplified by the EU-VAP/CAP study, which documented an incidence density of 18.3 episodes per 1000 ventilator days.1,7,37,38 The disparity becomes even more pronounced when comparing high-income countries with lower-middle-income nations, where rates of 9.0 versus 18.5 per 1000 ventilator days, respectively (P = 0.035), reveal significant healthcare inequities.1,2,39
These striking variations in reported VAP prevalence likely stem from several factors, including inconsistent diagnostic criteria, differences in how these criteria are applied in clinical practice, inherent limitations in the definitions themselves, and variations in microbiological sampling techniques across healthcare settings.1,39,40 The temporal pattern of VAP risk also warrants attention—patients face the highest daily risk between days 5 and 9 of mechanical ventilation, while the cumulative incidence correlates strongly with the overall duration of ventilator support.41,42 These findings emphasize the importance of implementing preventive measures early in the course of mechanical ventilation, particularly for patients anticipated to require prolonged respiratory support.
The reviewed evidence strongly supports implementing structured preventive interventions such as the Institute for Healthcare Improvement ventilator bundle as standard practice within ICUs. Emphasis should be placed on continuous staff training and adherence monitoring to ensure sustained effectiveness of these protocols. Additionally, addressing antibiotic-resistant pathogens through early diagnosis and appropriate antibiotic stewardship remains critical for improving patient outcomes and reducing healthcare-associated costs.29-31
Key strengths of this study include prospective designs allowing accurate temporal assessment of intervention effectiveness and outcomes. Moreover, relatively large sample sizes enhance the generalizability of findings. However, notable limitations exist. All studies were conducted within a single city (Riyadh), limiting geographic representativeness. Methodological variations existed regarding diagnostic criteria for VAP, and differences in compliance with preventive bundles were not consistently reported or analyzed.
Structured interventions such as ventilator care bundles effectively reduce VAP incidence among ICU patients in Saudi Arabia, improving patient outcomes and optimizing healthcare resource utilization. Nonetheless, further research addressing existing methodological limitations, including broader geographic representation within Saudi Arabia, is required. Future studies should investigate long-term intervention sustainability, regional differences in risk factors, compliance variations across hospitals, and impacts on antibiotic resistance patterns to enhance preventive strategies tailored specifically to local contexts.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
This research was funded by the Deanship of Scientific Research at Northern Border University, Arar, KSA, through project number NBU-FFR-2025-3172-04.
10. Author Contributions
HMAA, HHMA, WRMA, DNMA: contributed to data collection and preparation, initial processing and verification of the material, resource management, and drafting of the initial manuscript.
SEE, EKF, BTAA. MSF: responsible for conceptualization, study design, validation, resource provision, critical review, and overall oversight of the study.
All authors have reviewed and approved the final version of the manuscript.
Authors affiliations:
- Safya E. Esmaeel, Department of Physiology, College of Medicine, Northern Border University, 91431, Arar, Saudi Arabia; Email: ebraheem@nbu.edu.sa
- Haba Mofareh Alhumaidi Alanazi, College of Medicine, Northern Border University, Arar 91431, Saudi Arabia; Email: Hemofreh14@gmail.com
- Hajar Hamed Mosharek Alruwaili, College of Medicine, Northern Border University, Arar 91431, Saudi Arabia; Email: Im3hajar@gmail.com
- Wahj Radi M. Alenezi, College of Medicine, Northern Border University, Arar 91431, Saudi Arabia; Email: Wahajalenzi13@gmail.com
- Dala Naif M Alenzi, College of Medicine, Northern Border University, Arar 91431, Saudi Arabia; Email: dalaalanze@gmail.com
- Eslam K. Fahmy, Department of Physiology, College of Medicine, Northern Border University, 91431, Arar, Saudi Arabia; Email: kamal@nbu.edu.sa
- Baraah Abu Alsel, Medical Sciences & Preparatory Year Department, North Private College of Nursing, Arar, Saudi Arabia; Email: Baraahsel@nec.edu.sa
- Manal S. Fawzy, Center for Health Research, Northern Border University, Arar 73213, Saudi Arabia; Email: darwish@nbu.edu.sa
ABSTRACT
Background & objective: This study aimed to systematically assess the prevalence of ventilator-associated pneumonia (VAP) among intensive care unit (ICU) patients in Saudi Arabia and to evaluate the impact of preventive interventions.
Methodology: A systematic search of PubMed, Scopus, Web of Science, and regional databases identified 364 studies (2000–2023). After duplicate removal and screening, four studies (n = 4247 patients; 64.7% male) met the inclusion criteria. Data extraction and quality assessment were performed using Rayyan QCRI and PRISMA guidelines.
Results: VAP prevalence in Saudi ICUs varied widely, ranging from 2.2% to 35.4%, with a pooled prevalence of 12%. Implementation of structured preventive measures, particularly ventilator care bundles, was consistently associated with reduced VAP incidence, shorter durations of mechanical ventilation, decreased hospital stays, and improved patient outcomes. Despite these improvements, differences in study design and reporting continue to limit direct comparisons across centers.
Conclusion: VAP remains a significant concern in Saudi Arabian ICUs, with prevalence rates higher than some international benchmarks. Preventive strategies, especially care bundles, are effective but require ongoing adaptation to local contexts. Further research should focus on standardizing surveillance, evaluating long-term intervention effectiveness, and identifying region-specific risk factors to optimize patient care and resource utilization.
Abbreviations: ICU: intensive care unit, VAP: ventilator-associated pneumonia,
Keywords: Ventilator-associated pneumonia; Intensive care unit; Critically ill patients; Saudi Arabia; Systematic review.
Citation: Esmaeel SE, Alanazi HM, Alruwaili HH, Alenezi WR, Alenzi DN, Fahmy EK, Abu Alsel BT, Fawzy MS. Prevalence of ventilator-associated pneumonia (VAP) in patients admitted to intensive care units in Saudi Arabia: a systematic review. Anaesth. pain intensive care 2025;29(8):1014-1021. DOI: 10.35975/apic.v29i8.3032.
Received: May 09, 2025; Revised: October 06, 2025; Accepted: October 06, 2025
1. INTRODUCTION
Ventilator-associated pneumonia (VAP), also known as intubation-associated pneumonia, is defined as pneumonia occurring more than 48-72 hours after endotracheal intubation, provided it was not incubating at the time of admission.1,2 Clinically, VAP is characterized by new or progressive pulmonary infiltrates, systemic signs of infection, and alterations in the characteristics of sputum.3 It represents one of the most frequent and severe nosocomial infections among patients admitted to intensive care units (ICUs), significantly contributing to patient morbidity and mortality.1-4 VAP-related mortality rates range widely from 24% to 76% across various international settings.5,6
The Institute of Medicine has identified the prevention of hospital-acquired infections, including VAP, as a national healthcare priority due to their substantial impact on patient outcomes and healthcare resources.7,8 Patients diagnosed with VAP experience prolonged hospital stays and increased healthcare costs, placing additional burdens on healthcare systems.9,10 Globally, the reported incidence of VAP among ICU populations varies considerably, ranging from 8.0% to 28.8%, reflecting differences in healthcare practices, infection control measures, patient populations, and microbial environments.11-13
Future research should prioritize standardizing surveillance, assessing the long-term effectiveness of interventions, and identifying region-specific risk factors to optimize patient care and resource allocation.14,15 Although several individual studies have examined VAP incidence in various Saudi Arabian hospitals or regions, a systematic synthesis of these data at the national level remains limited.16 Previous multi-hospital surveillance reports from Saudi Arabia have been published; however, these reports lack sufficient representativeness and methodological rigor to estimate national prevalence rates accurately.17,18 Consequently, there is a critical knowledge gap regarding the true burden of VAP across Saudi Arabian ICUs.
Addressing this gap through a comprehensive systematic review is essential for accurately quantifying the VAP prevalence in Saudi Arabia. Such an approach will facilitate an improved understanding of regional variations in risk factors and microbial profiles associated with VAP. Furthermore, synthesizing existing data can inform targeted preventive strategies aimed at reducing the incidence of VAP, optimizing resource allocation within ICUs, and ultimately improving patient outcomes nationwide.19,20 In this sense, the principal objective of this systematic review is to critically evaluate and consolidate available evidence regarding the prevalence of ventilator-associated pneumonia among ICU patients throughout Saudi Arabia.
2. METHODOLOGY
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines21 and the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).22 The protocol was registered with the International Platform of Registered Systematic Review and Meta-Analysis (INPLASY), with the registration number: NPLASY202530042. A thorough search strategy was developed to identify relevant studies investigating the VAP prevalence among ICU patients in Saudi Arabia. From the start to the date of this review, four electronic databases, PubMed, Scopus, Web of Science, and Cochrane Library, were methodically searched. The search terms included combinations of keywords and medical subject headings (MeSH), such as ventilator-associated pneumonia (VAP), mechanical ventilation, intensive care unit (ICU), prevalence, incidence, and Saudi Arabia. No language/publication date restrictions were applied.
After removing duplicates, all retrieved titles and abstracts were imported into Rayyan QCR, a software tool for initial screening. Two independent coauthors screened the titles and abstracts to identify potentially eligible studies. The full texts of these studies were then retrieved and independently assessed by the same coauthors against predefined inclusion criteria. Any discrepancies or disagreements regarding study eligibility were resolved through consensus discussions or, when necessary, consultation with a third reviewer.
Studies were selected based on clearly defined Population-Exposure-Outcome (PEO) criteria: (i) Population: adult patients (≥18 years old) admitted to intensive care units (ICUs) in hospitals across Saudi Arabia, (ii) Exposure: patients receiving mechanical ventilation during their ICU admission, and (iii) Outcome: studies reporting data on the occurrence, or prevalence /incidence of VAP among mechanically ventilated ICU patients. Studies were excluded if they involved pediatric populations, did not explicitly report VAP prevalence/incidence, or were conducted outside Saudi Arabia. Additionally, case reports, letters, editorials, reviews without original data, conference abstracts without full-text availability, and studies lacking sufficient data for extraction were excluded.
Two independent coauthors extracted data from publications that matched the inclusion criteria using a predetermined/consistent methodology and a standardized data extraction form designed specifically for this review. The extracted data included: (i) Name of the first author; (ii) Publication year; (iii) Study design; (iv) Sample size (number of participants); (v) Participant demographics (age range or mean age; gender distribution); (vi) Prevalence/incidence rates of VAP (%); and (viii) Key findings related to risk factors and preventive interventions. Discrepancies in extracted data between coauthors were resolved through discussion until a consensus was reached.
The methodological quality and risk of bias in included studies were evaluated using the Risk Of Bias In Non-randomized Studies–of Interventions (ROBINS-I) assessment tool. This tool provides a structured framework for assessing bias across seven domains: confounding factors, selection bias, classification bias regarding interventions/exposures, deviations from intended interventions/exposures, missing data bias, measurement bias in outcomes assessment, and selective reporting bias. Two independent coauthors assessed each study independently using these criteria. Disagreements regarding risk-of-bias ratings were resolved through discussion or consultation with a third coauthor.23
Extracted data were synthesized narratively due to anticipated heterogeneity in study designs and outcome measurements among included studies Prevalence estimates were summarized descriptively. Key findings related to preventive interventions and associated outcomes (e.g., morbidity, mortality) are presented narratively to provide comprehensive insights into VAP prevalence and management practices within Saudi Arabian ICUs.
3. RESULTS
The targeted search approach produced 364 publications (Figure 1). Then, the removal of duplicates (n = 160) and 204 trials were assessed using the abstract and title. One hundred sixty-eight of these did not meet the qualifying requirements; therefore, only 50 full-text publications remained for thorough evaluation. Four in all met the eligibility standards for analysis using evidence synthesis.
Figure 1: PRISMA flowchart
Four studies involving a total of 4,247 ICU patients met the inclusion criteria for qualitative synthesis. Among these patients, 2,749 (64.7%) were males. Regarding study designs, three studies utilized prospective cohort methodologies,24-26 while one study employed a case-control design.27 All four studies were conducted in Riyadh City hospitals between 2004 and 2017.24-27
The reported prevalence of ventilator-associated pneumonia (VAP) among critically ill patients in Saudi Arabia ranged widely from 2.2% to 35.4%,24-27 with an overall pooled prevalence of 12% (510 cases). Key findings from the included studies provided important insights into the prevalence trends of VAP and associated clinical outcomes. One study observed a declining trend in VAP rates over time, suggesting the effectiveness of targeted preventive interventions and improved healthcare practices in reducing infection incidence.24
Another study underscored the benefits of implementing structured care protocols, particularly ventilator care bundles, in reducing VAP incidence and optimizing ventilator utilization. These protocol-driven approaches demonstrated the potential to decrease hospital-acquired infections and improve resource management within ICU settings.25
Further analysis indicated that VAP was consistently associated with prolonged durations of mechanical ventilation, increased length of hospital stays, and elevated morbidity and mortality rates among affected patients. These findings underscore the substantial clinical burden imposed by VAP on both patient outcomes and healthcare resources, emphasizing the critical need for effective preventive strategies to mitigate these adverse impacts.27
Lastly, extended ICU stays attributed to VAP were strongly correlated with significantly higher morbidity rates and hospital mortality. This association highlights severe complications arising from prolonged critical care exposure due to VAP, further reinforcing the importance of early detection, timely intervention, and comprehensive infection prevention measures within ICU settings.26
| Table 1: Outcomes of the included studies | |||||||
| First author/ Ref. | City | Study design | Socio-demographics | VAP (%) | Key findings | ||
| Participants | Mean age | Males
n (%) |
|||||
| Al-Dorzi et al.,24 | Riyadh | Prospective cohort | 2812 | 55 | 1873 (66.6%) | 433 (15.4%) | VAP is still a frequent side effect of serious disease. It shows that the VAP rate is trending downward, most likely as a result of diverse efforts. |
| Al-Thaqafy et al., 25 | Riyadh | Prospective cohort | 1026 | 56.6 | 618 (60.2%) | 23 (2.2%) |
When the ventilator bundle was implemented for adult critical patients, there was a more than 70% improvement in VAP rates and a 20% improvement in ventilator usage. |
| Almuneef et al.,26 | Riyadh | Prospective cohort | 361 | 28.5 | 230 (63.7%) | 37 (10 .2%) |
An extended period of ventilation, an ICU or hospital stay, and an increase in in-hospital morbidity and mortality are all linked to VAP, a common and dangerous ICU consequence that can result in greater treatment expenses. |
| Othman & Abdelazim, 27 | Riyadh | Case-control | 48 | 58.1 | 28 (58.3%) | 17 (35.4%) |
A frequent and dangerous intensive care unit consequence, VAP is linked to longer ventilation times, longer hospital stays, and greater rates of in-hospital morbidity and mortality, all of which can raise treatment expenses. |
| VAP: ventilator-associated pneumonia; Data presented as n or n (%); Mean age given as years. | |||||||
4. DISCUSSION
This systematic review aimed to critically evaluate and synthesize existing evidence regarding the prevalence of VAP among ICU patients in Saudi Arabia. Our findings indicate substantial variability in VAP prevalence across studies, highlighting a significant healthcare challenge within Saudi ICUs. The reviewed studies collectively underscore the clinical burden imposed by VAP, including prolonged durations of mechanical ventilation, increased ICU/hospital stays, and elevated morbidity and mortality rates. Importantly, structured preventive interventions, particularly ventilator care bundles, appear effective in reducing VAP incidence and optimizing resource utilization. Despite these promising results, the variability observed emphasizes the necessity of tailoring preventive strategies to local contexts. To our knowledge, this is the first systematic review consolidating national data on VAP prevalence in Saudi Arabia, providing critical insights that could inform future healthcare policies, clinical practices, and targeted preventive strategies.
Recent evidence underscores the persistent challenge of VAP in modern intensive care settings.28 Alnimr's comprehensive review highlighted that despite advances in critical care medicine, VAP remains a significant concern with far-reaching consequences for patient outcomes.29 Of particular concern is the growing association between VAP and antibiotic-resistant pathogens, which substantially increases patient morbidity, mortality, and healthcare expenditures.29-31
This alarming trend emphasizes why VAP prevention must remain a clinical priority.32 When VAP does occur, early and appropriate antibiotic therapy becomes crucial, not only to improve patient outcomes but also to minimize the emergence of resistant microorganisms that further complicate treatment.29,33 Hassan and colleagues reinforced these concerns, noting that VAP significantly extends ICU stays and elevates mortality rates, creating additional strain on healthcare systems, particularly in resource-limited settings.5
Our systematic review revealed considerable variability in VAP prevalence among critically ill patients in Saudi Arabia, with rates ranging from as low as 2.2%34 to as high as 35.4%35, yielding an overall prevalence of 12% (510 cases). These findings gain perspective when compared with international data. North American hospitals typically report remarkably low VAP incidence, between 1 and 2.5 cases per 1000 ventilator days.1,7,36 European healthcare facilities, however, demonstrate substantially higher rates, exemplified by the EU-VAP/CAP study, which documented an incidence density of 18.3 episodes per 1000 ventilator days.1,7,37,38 The disparity becomes even more pronounced when comparing high-income countries with lower-middle-income nations, where rates of 9.0 versus 18.5 per 1000 ventilator days, respectively (P = 0.035), reveal significant healthcare inequities.1,2,39
These striking variations in reported VAP prevalence likely stem from several factors, including inconsistent diagnostic criteria, differences in how these criteria are applied in clinical practice, inherent limitations in the definitions themselves, and variations in microbiological sampling techniques across healthcare settings.1,39,40 The temporal pattern of VAP risk also warrants attention—patients face the highest daily risk between days 5 and 9 of mechanical ventilation, while the cumulative incidence correlates strongly with the overall duration of ventilator support.41,42 These findings emphasize the importance of implementing preventive measures early in the course of mechanical ventilation, particularly for patients anticipated to require prolonged respiratory support.
The reviewed evidence strongly supports implementing structured preventive interventions such as the Institute for Healthcare Improvement ventilator bundle as standard practice within ICUs. Emphasis should be placed on continuous staff training and adherence monitoring to ensure sustained effectiveness of these protocols. Additionally, addressing antibiotic-resistant pathogens through early diagnosis and appropriate antibiotic stewardship remains critical for improving patient outcomes and reducing healthcare-associated costs.29-31
| Table 2: Assessing bias risk with ROBINS-I | |||||||||
|
First author/Reference |
bias as a result of confusion | Bias in the participants' selection | Bias in characterizing interventions. | Bias caused by divergence from the scheduled time frame | The bias created by data shortages | Bias in measuring achievements | Bias in the selection of reported outcomes | Overall bias | |
| Al-Dorzi et al.,24 | Low | Low | Mod | Low | Low | Low | Mod | Low | |
| Al-Thaqafy et al.,25 | Mod | Low | Mod | Low | Low | Mod | Low | Moderate | |
| Almuneef et al.,26 | Mod | Low | Mod | Low | Low | Mod | Low | Moderate | |
| Othman & Abdelazim,27 | Mod | Mod | Low | Low | Low | Mod | Low | Moderate | |
5. Strengths and Limitations
Key strengths of this study include prospective designs allowing accurate temporal assessment of intervention effectiveness and outcomes. Moreover, relatively large sample sizes enhance the generalizability of findings. However, notable limitations exist. All studies were conducted within a single city (Riyadh), limiting geographic representativeness. Methodological variations existed regarding diagnostic criteria for VAP, and differences in compliance with preventive bundles were not consistently reported or analyzed.
6. CONCLUSION
Structured interventions such as ventilator care bundles effectively reduce VAP incidence among ICU patients in Saudi Arabia, improving patient outcomes and optimizing healthcare resource utilization. Nonetheless, further research addressing existing methodological limitations, including broader geographic representation within Saudi Arabia, is required. Future studies should investigate long-term intervention sustainability, regional differences in risk factors, compliance variations across hospitals, and impacts on antibiotic resistance patterns to enhance preventive strategies tailored specifically to local contexts.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
This research was funded by the Deanship of Scientific Research at Northern Border University, Arar, KSA, through project number NBU-FFR-2025-3172-04.
10. Author Contributions
HMAA, HHMA, WRMA, DNMA: contributed to data collection and preparation, initial processing and verification of the material, resource management, and drafting of the initial manuscript.
SEE, EKF, BTAA. MSF: responsible for conceptualization, study design, validation, resource provision, critical review, and overall oversight of the study.
All authors have reviewed and approved the final version of the manuscript.
11. REFERENCES
- Papazian L, Klompas M, Luyt CE. Ventilator-associated pneumonia in adults: a narrative review. Intensive care medicine. 2020;46(5):888-906. [PubMed] DOI: 10.1007/s00134-020-05980-0
- Bonell A, Azarrafiy R, Huong VTL, Viet TL, Phu VD, Dat VQ, et al. A Systematic Review and Meta-analysis of Ventilator-associated Pneumonia in Adults in Asia: An Analysis of National Income Level on Incidence and Etiology. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2019;68(3):511-8. [PubMed] DOI: 10.1093/cid/ciy543
- Semet C. The ongoing challenge of ventilator-associated pneumonia: epidemiology, prevention, and risk factors for mortality in a secondary care hospital intensive care unit. Infection prevention in practice. 2023;5(4):100320. [PubMed] DOI: 10.1016/j.infpip.2023.100320
- Khan HA, Baig FK, Mehboob R. Nosocomial infections: Epidemiology, prevention, control and surveillance. Asian Pacific Journal of Tropical Biomedicine. 2017;7(5):478-82.[FullText] DOI: 10.1016/j.apjtb.2017.01.019
- Hasan MJ, Sumi CD, Huq SMR, Anam AM, Rabbani R. Aerosolized Plus Intravenous Polymyxin B Versus Colistin in the Treatment of Pandrug-Resistant Klebsiella Pneumonia-mediated Ventilator-Associated Pneumonia: A Retrospective Cohort Study in Bangladesh. Journal of critical care medicine. 2023;9(2):106-15.[PubMed] DOI: 10.2478/jccm-2023-0012
- Nunez SA, Roveda G, Zarate MS, Emmerich M, Veron MT. Ventilator-associated pneumonia in patients on prolonged mechanical ventilation: description, risk factors for mortality, and performance of the SOFA score. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2021;47(3):e20200569.[PubMed] DOI: 10.36416/1806-3756/e20200569
- Koulenti D, Tsigou E, Rello J. Nosocomial pneumonia in 27 ICUs in Europe: perspectives from the EU-VAP/CAP study. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2017;36(11):1999-2006.[PubMed] DOI: 10.1007/s10096-016-2703-z
- Magill SS, O'Leary E, Janelle SJ, Thompson DL, Dumyati G, Nadle J, et al. Changes in Prevalence of Health Care-Associated Infections in U.S. Hospitals. The New England journal of medicine. 2018;379(18):1732-44.
- Reignier J, Mercier E, Le Gouge A, Boulain T, Desachy A, Bellec F, et al. Effect of not monitoring residual gastric volume on risk of ventilator-associated pneumonia in adults receiving mechanical ventilation and early enteral feeding: a randomized controlled trial. Jama. 2013;309(3):249-56.[PubMed] DOI: 10.1001/jama.2012.196377
- Ahmadipour M, Lashkari M, Ahmadinejad M. Comparison of Morbidity, Mortality, and Costs of VAP Patients with Non-VAP Patients in the Tertiary Referral Hospital of Kerman, Iran. Tanaffos. 2023;22(1):61-9.[PubMed]
- Humayun T, Alshanbari N, Alanazi A, S. Aldecoa Y, H. Alanazi K, Bin Saleh G, et al. Rates of Ventilator Associated Pneumonia in Saudi Ministry of Health Hospitals; A Two-year Multi-Center Study. American Journal of Infectious Diseases and Microbiology. 2021;9(1):25-31. [FullText] DOI:10.12691/ajidm-9-1-6
- Alshamrani MM, El-Saed A, Alsaedi A, El Gammal A, Al Nasser W, Nazeer S, et al. Burden of healthcare-associated infections at six tertiary-care hospitals in Saudi Arabia: A point prevalence survey. Infection control and hospital epidemiology. 2019;40(3):355-7. [PubMed] DOI:10.1017/ice.2018.338
- Timsit JF, Esaied W, Neuville M, Bouadma L, Mourvllier B. Update on ventilator-associated pneumonia. F1000Research. 2017;6:2061. [PubMed] DOI:10.12688/f1000research.12222.1
- Kang L, Jing W, Liu J, Liu M. Trends of global and regional aetiologies, risk factors and mortality of lower respiratory infections from 1990 to 2019: An analysis for the Global Burden of Disease Study 2019. Respirology. 2023;28(2):166-75. [PubMed] DOI: 10.1111/resp.14389
- Mohamed HT, Farhan Alenezi WA, Sr., Alanzi MAA, Saleh Alsuqub FI, Salem Alhazmi SA, Mohammed Alhazmi OM. Prevalence of Ventilator-Associated Pneumonia in Children Admitted to Pediatric Intensive Care Units in the Middle East: A Systematic Review. Cureus. 2023;15(12):e51230. [PubMed] DOI: 10.7759/cureus.51230
- Gaid E, Assiri A, McNabb S, Banjar W. Device-associated nosocomial infection in general hospitals, Kingdom of Saudi Arabia, 2013-2016. Journal of epidemiology and global health. 2018;7 Suppl 1(Suppl 1):S35-S40. [PubMed] DOI: 10.1016/j.jegh.2017.10.008
- Banjar A, Felemban M, Dhafar K, Gazzaz Z, Al Harthi B, Baig M, et al. Surveillance of preventive measures for ventilator associated pneumonia (VAP) and its rate in Makkah Region hospitals, Saudi Arabia. Turkish journal of medical sciences. 2017;47(1):211-6. [PubMed] DOI:10.3906/sag-1510-105
- Hassan ME, Al-Khawaja SA, Saeed NK, Al-Khawaja SA, Al-Awainati M, Radhi SSY, et al. Causative bacteria of ventilator-associated pneumonia in intensive care unit in Bahrain: Prevalence and antibiotics susceptibility pattern. World journal of critical care medicine. 2023;12(3):165-75. [PubMed] DOI: 10.5492/wjccm.v12.i3.165
- Klompas M, Branson R, Cawcutt K, Crist M, Eichenwald EC, Greene LR, et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infection control and hospital epidemiology. 2022;43(6):687-713. [PubMed] DOI: 10.1017/ice.2022.88
- Boltey E, Yakusheva O, Costa DK. 5 Nursing strategies to prevent ventilator-associatedpneumonia. American nurse today. 2017;12(6):42-3. [PubMed] PMCID: PMC5706660
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. [PubMed] DOI:10.1186/2046-4053-4-1
- 22.Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, et al. Guidelines for Accurate and Transparent Health Estimates Reporting: the GATHER statement. Lancet (London, England). 2016;388(10062):e19-e23. [PubMed] DOI:10.1016/S0140-6736(16)30388-9
- Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Bmj. 2016;355:i4919. [PubMed] DOI: 10.1136/bmj.i4919
- 24.Al-Dorzi HM, El-Saed A, Rishu AH, Balkhy HH, Memish ZA, Arabi YM. The results of a 6-year epidemiologic surveillance for ventilator-associated pneumonia at a tertiary care intensive care unit in Saudi Arabia. American journal of infection control. 2012;40(9):794-9. [PubMed] DOI: 10.1016/j.ajic.2011.10.004
- Al-Thaqafy MS, El-Saed A, Arabi YM, Balkhy HH. Association of compliance of ventilator bundle with incidence of ventilator-associated pneumonia and ventilator utilization among critical patients over 4 years. Annals of thoracic medicine. 2014;9(4):221-6. [PubMed] DOI:10.4103/1817-1737.140132
- 26.Almuneef M, Memish ZA, Balkhy HH, Alalem H, Abutaleb A. Ventilator-associated pneumonia in a pediatric intensive care unit in Saudi Arabia: a 30-month prospective surveillance. Infection control and hospital epidemiology. 2004;25(9):753-8. [PubMed] DOI:10.1086/502472
- Abdelrazik Othman A, Salah Abdelazim M. Ventilator-associated pneumonia in adult intensive care unit prevalence and complications. The Egyptian Journal of Critical Care Medicine. 2017;5(2):61-3. [PubMed]
- Mergulhão P, Pereira JG, Fernandes AV, Krystopchuk A, Ribeiro JM, Miranda D, et al. Epidemiology and Burden of Ventilator-Associated Pneumonia among Adult Intensive Care Unit Patients: A Portuguese, Multicenter, Retrospective Study (eVAP-PT Study). Antibiotics (Basel, Switzerland). 2024;13(4). [PubMed] DOI: 10.3390/antibiotics13040290
- Alnimr A. Antimicrobial Resistance in Ventilator-Associated Pneumonia: Predictive Microbiology and Evidence-Based Therapy. Infectious diseases and therapy. 2023;12(6):1527-52. [PubMed] DOI:10.1007/s40121-023-00820-2
- Stoclin A, Rotolo F, Hicheri Y, Mons M, Chachaty E, Gachot B, et al. Ventilator-associated pneumonia and bloodstream infections in intensive care unit cancer patients: a retrospective 12-year study on 3388 prospectively monitored patients. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer. 2020;28(1):193-200. [PubMed] DOI: 10.1007/s00520-019-04800-6
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum beta-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2022;75(2):187-212. [PubMed]DOI:10.1093/cid/ciac268
- Hlinkova S, Moraucikova E, Strzelecka A, Mrazova M, Littva V. Ventilator-Associated Pneumonia in Intensive Care Units: A Comparison of Pre-Pandemic and COVID-19 Periods. J Clin Med. 2025;14(3). [PubMed] DOI: 10.3390/jcm14031000
- Howroyd F, Chacko C, MacDuff A, Gautam N, Pouchet B, Tunnicliffe B, et al. Ventilator-associated pneumonia: pathobiological heterogeneity and diagnostic challenges. Nature communications. 2024;15(1):6447. [PubMed] DOI: 10.1038/s41467-024-50805-z
- Dudeck MA, Horan TC, Peterson KD, Allen-Bridson K, Morrell G, Anttila A, et al. National Healthcare Safety Network report, data summary for 2011, device-associated module. American journal of infection control. 2013;41(4):286-300. [PubMed] DOI: 10.1016/j.ajic.2013.01.002
- Lanks CW, Musani AI, Hsia DW. Community-acquired Pneumonia and Hospital-acquired Pneumonia. The Medical clinics of North America. 2019;103(3):487-501. [PubMed] DOI: 10.1016/j.mcna.2018.12.008
- Blonz G, Kouatchet A, Chudeau N, Pontis E, Lorber J, Lemeur A, et al. Epidemiology and microbiology of ventilator-associated pneumonia in COVID-19 patients: a multicenter retrospective study in 188 patients in an un-inundated French region. Critical care. 2021;25(1):72. [PubMed] DOI:10.1186/s13054-021-03493-w
- Sleziak J, Pilarczyk K, Matysiak M, Duszynska W. Pneumonia Characteristics in an Intensive Care Unit Setting during and after the COVID-19 Pandemic-A Single-Center Prospective Study. J Clin Med. 2024;13(10). [PubMed] DOI: 10.3390/jcm13102824
- Baker D, Quinn B. Hospital Acquired Pneumonia Prevention Initiative-2: Incidence of nonventilator hospital-acquired pneumonia in the United States. American journal of infection control. 2018;46(1):2-7. [PubMed] DOI:10.1016/j.ajic.2017.08.036
- 39.Ego A, Preiser JC, Vincent JL. Impact of diagnostic criteria on the incidence of ventilator-associated pneumonia. Chest. 2015;147(2):347-55. [PubMed] DOI: 10.1378/chest.14-0610
- Magill SS, Klompas M, Balk R, Burns SM, Deutschman CS, Diekema D, et al. Developing a new, national approach to surveillance for ventilator-associated events: executive summary. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013;57(12):1742-6. [PubMed] DOI: 10.1093/cid/cit577
- Mumtaz H, Saqib M, Khan W, Ismail SM, Sohail H, Muneeb M, et al. Ventilator associated pneumonia in intensive care unit patients: a systematic review. Annals of medicine and surgery. 2023;85(6):2932-9. [PubMed] DOI: 10.1097/MS9.0000000000000836
- Mergulhao P, Pereira JG, Fernandes AV, Krystopchuk A, Ribeiro JM, Miranda D, et al. Epidemiology and Burden of Ventilator-Associated Pneumonia among Adult Intensive Care Unit Patients: A Portuguese, Multicenter, Retrospective Study (eVAP-PT Study). Antibiotics (Basel, Switzerland). 2024;13(4). [PubMed] DOI: 10.3390/antibiotics13040290