Theresia Chandra Tania Novy 1 , Hemant Kalia 2 , Yu Chuan (Grace) Tsai 3
Authors affiliations:
Complex Regional Pain Syndrome (CRPS) is a chronic neuropathic condition marked by pain disproportionate to the initial trauma, often accompanied by hyperalgesia, allodynia, and autonomic dysfunction. It commonly follows surgery, trauma, or nerve injury. This case report highlights the use of ultrasound-guided hydrodissection with dextrose prolotherapy as a minimally invasive approach to managing CRPS secondary to nerve injury.
A 27-year-old male presented with persistent pain, paresthesia, hypersensitivity, and intermittent shock-like sensations from the left index finger radiating to the upper back, occurring after surgical wire removal for a finger fracture. Clinical and ultrasound findings supported the diagnosis of CRPS type II (causalgia) due to nerve injury. The patient was treated with ultrasound-guided perineural hydrodissection using 5% dextrose to reduce nerve adhesion and irritation. Pain was assessed using the Numeric Rating Scale (NRS) at baseline, one week post-procedure, monthly for 12 months, and at a 21-month follow-up. The patient demonstrated sustained improvement in pain and sensory function without complications.
This case illustrates the potential of ultrasound-guided dextrose hydrodissection as a safe and effective treatment for CRPS caused by nerve injury. Larger studies are warranted to validate its efficacy and elucidate underlying mechanisms.
Abbreviations: CRPS: Complex Regional Pain Syndrome, IPM: Interventional Pain Medicine, NRS: Numeric Rating Scale, ORIF: Open Reduction and Internal Fixation, NSAIDs: Nonsteroidal Anti-Inflammatory Drugs
Keywords: Complex Regional Pain Syndrome; dextrose prolotherapy; hydrodissection; interventional pain management; ultrasound-guided injection
Citation: Novy TCT, Kalia H, Tsai YCG.Novel treatment of complex regional pain syndrome using hydrodissection with dextrose prolotherapy. Anaesth. pain intensive care 2025;29(7):808-813. DOI: 10.35975/apic.v29i7.2973
Received: Jul 12, 2025; Revised; August 27, 2025; Accepted: August 27, 2025
Complex Regional Pain Syndrome (CRPS) is a chronic neurological condition that causes debilitating pain, and a common indicator is allodynia and hyperalgesia in the extremities. It may also involve dystrophic changes, such as pale, cold skin. In the past, this syndrome has been referred to as "reflex sympathetic dystrophy", "causalgia", "algoneurodystrophy", and "Sudeck atrophy". CRPS is classified into two types: CRPS-I and CRPS-II. Their differences lie in the presence of definite nerve damage. CRPS type I develops in the absence of definite damage to the nerve, whereas CRPS type II occurs only when there is confirmed neuropathy.1,2
The prevalence of CRPS ranges from 6.28 to 26.2 per 100,000 person-years. Its common indicators include chronic pain, pain hypersensitivity, and/or allodynia accompanied by edema or changes in sudomotor activity, typically affecting the distal extremities.1,3 A set of signs and symptoms referred to as the Budapest criteria has been developed; however, accurate diagnosis of CRPS remains a challenge due to various knowledge gaps regarding the pathophysiology of CRPS. Neuropathic inflammation, particularly the activation of peripheral C-fiber nociceptors and the autonomic nervous system, has been shown to be pivotal in the development of CRPS.1 However, the exact etiology of the condition likely lies in different interactions between several mechanisms, such as central sensitization and neuroplastic alterations.3
Injuries occurring in the extremities, such as fractures, dislocations, past surgical interventions, and carpal tunnel syndrome, are the most common triggers for CRPS. In a 2018 study cited by Taylor et al., it was found that of 1043 patients diagnosed with CRPS, 441 (42%) were caused by fractures, 214 (21%) by blunt traumatic injuries excluding fractures, 124 (12%) by prior surgical history, 69 (7%) by carpal tunnel syndrome, 47 (5%) by sharp traumas, and 77 (7%) cases had no clear triggering event.1 CRPS symptoms show varying progression over time, making early initiation of therapy crucial for patient prognosis. The goals are to reduce pain, restore limb functionality, and improve quality of life. This will involve a multifaceted plan incorporating patient-centered education, therapy (physical and occupational), psychiatry, pain medicine specialists, as well as surgical and pharmacological solutions.4,5
The most used treatment for CRPS is sympathetic blockade, mainly due to its minimally invasive nature. Despite its popularity, there is limited evidence regarding its short-term and long-term analgesic effects.1 In a 2019 study of 255 out of 318 patients diagnosed with CRPS (80%), 155 experienced over 50% pain reduction. Most of the patients (71%) reported pain reduction for 1–4 weeks, while 14% experienced pain reduction for more than a month. Data from this study showed clinical significance and acted as pioneering evidence for the use of sympathetic blockade in the treatment of CRPS.4,5
This case report presents a novel management approach using ultrasound-guided interventional pain medicine (IPM) with hydrodissection and dextrose prolotherapy, which yielded satisfactory outcomes in a 27-year-old male patient with CRPS due to a nerve injury in the left index finger.
A 27-year-old male patient reported nine months of hypersensitivity in his left index finger, triggered by touch and causing electric shock-like pain radiating to his shoulder. Additional symptoms included nighttime numbness, tingling, dizziness, and cold, pale skin. He had undergone open reduction and internal fixation (ORIF) with wire placement for a work-related finger fracture 1.5 years prior, followed by wire removal surgery nine months ago—after which his symptoms began immediately. Activities such as push-ups and sensory exercises exacerbated the pain. During fieldwork, he experienced intense pain when holding tools, often resulting in tools falling out of his grasp. These occurrences posed safety risks, resulting in his reassignment from field duties to an office role. Despite treatment with amitriptyline and gabapentin prescribed by his occupational physician, his symptoms persisted, interfering with sleep and daily activities. He also reported dizziness as a side effect of gabapentin.
The patient was in a generally good condition, fully conscious, with normal vital signs and body mass index. Physical examination showed normal wrist movement and no neurological deficits, except for increased pain sensitivity (hyperalgesia) at the tip of the left index finger. Sensory and motor tests are summarized in Table 1.
Ultrasound examination of the finger revealed fibrotic tissue without neovascularization, consistent with a nerve injury (Figure 1).
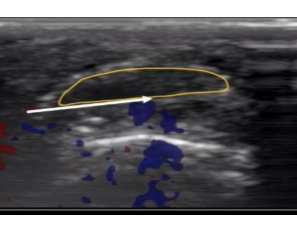
Figure 1: Ultrasound examination of the left index finger showing fibrotic tissue without neovascularization, consistent with nerve injury.
This patient fulfilled all the Budapest criteria for CRPS type II caused by nerve injury. He had persistent, excessive pain for nine months following wire removal after ORIF, described as electric shock-like pain radiating to the shoulder. Furthermore, the patient exhibited symptoms across all categories: sensory (touch hypersensitivity, hyperalgesia, and allodynia), vasomotor (cold, pale skin), and motor/trophic (functional impairment affecting daily activities and work duties). Alternative diagnoses did not adequately account for his symptoms. The case was classified as CRPS type II due to a documented nerve injury related to the wire removal surgery, with symptoms emerging after a known insult.
We proceeded with a left median nerve block followed by hydrodissection. Pain was reassessed using the Numeric Rating Scale (NRS). The patient underwent ultrasound-guided interventional pain management (IPM), starting with a left median nerve block using 2 cc of 1% lidocaine, followed by hydrodissection with 2 cc of 5% dextrose. After the procedure, his pain score dropped to 0/10, and the affected finger was no longer pale or cold. The patient was then prescribed acetaminophen-tramadol every 12 hours and amitriptyline for one week. Additionally, gabapentin was tapered from 300 mg to 100 mg every 8 hours. He was advised to maintain a pain diary and to return for a follow-up in one week.
At the one-week follow-up, the tingling had decreased by 75% and was limited to the wrist. Furthermore, the finger appeared warm with improved vascularity. Dizziness had resolved, object handling had improved, and sleep quality had improved. The patient was given a new prescription of acetaminophen-tramadol every 24 hours for one week, while amitriptyline was discontinued, and gabapentin was further tapered to 100 mg once daily. He remained in an office-based work role.
By one month, all symptoms had resolved. The patient resumed fieldwork and continued mecobalamin 500 mcg twice daily for six months. Gabapentin was discontinued, and dizziness did not recur. At the 12- and 21-month follow-ups, he remained symptom-free and was able to perform work, daily activities, and sports without disruptions. The clinical progress of the patient is summarized in Figure 2 and Table 2.
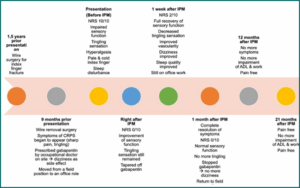
Figure 2: Clinical progression of the patient following ultrasound-guided hydrodissection with 5% dextrose. Pain intensity, sensory symptoms, and functional improvement were monitored at baseline, 1 week, 1 month, 12 months, and 21 months post-procedure, showing sustained resolution of symptoms
CRPS is a neurological condition that causes debilitating pain and often involves pain hypersensitivity (hyperalgesia) and allodynia in the extremities. Injuries in the extremities, such as fractures, sprains, surgical history, and carpal tunnel syndrome, are the most common triggers for CRPS.3 CRPS type II can be associated with identifiable nerve injuries. These injuries disrupt normal nerve conduction due to trauma, inadequate surgical repair, or chronic fibro-inflammatory processes. Such disruption can hinder the reinnervation process, especially when scar tissue obstructs nerve regeneration. Rather than representing a malignant neoplasm, this condition reflects a non-neoplastic, localized proliferation and dysregulation of injured nerve fibers.4,5 In this study, we outline the treatment of a 27-year-old male who presented to the Bandung Pain Rehab Center with complaints of hypersensitivity in the left index finger. The symptoms worsened with touch, leading to a sensation of electric shock extending to the left shoulder and numbness (paresthesia).
In a study of over 33 million patients (2007–2011), 22,533 (0.07%) were diagnosed with CRPS. A 2018 study by Ott and Maihöfner in Germany showed similar trends, with CRPS being more common in women (71%) than men (29%). The condition mostly affects the upper limbs (70% of cases), and CRPS type I is more common than type II (88% vs. 12%). Distal injuries, such as forearm fractures, are more likely to lead to CRPS than proximal fractures. Additionally, musculoskeletal conditions like rheumatoid arthritis, high-energy trauma, and severe fractures increase the risk of developing CRPS.6 Our case presents a male patient with CRPS type II, contrasting epidemiological studies where CRPS type I is typically more common, with a higher prevalence in women. On the other hand, this case report aligns with the literature, indicating that injury or trauma is the most common cause of CRPS.
No precise test has been developed for CRPS, which makes diagnosis difficult. The Budapest Criteria were developed and have now become the standard for diagnosing CRPS. These criteria maintain high sensitivity for CRPS (0.99), but significantly improve the specificity of the IASP diagnostic criteria (0.41-0.68). This patient met all the Budapest criteria, with continuing excessive pain to any triggering event. The patient reported and displayed symptoms in three of four categories: hyperesthesia, temperature asymmetry, skin color changes, and motor dysfunction (tremor and dystonia). To further quantify disease severity, the CRPS Severity Score (CSS) was introduced in 2010. This score includes 17 distinct symptoms, with each symptom being assigned 1 point.6–8
Her et al., outline several treatments for CRPS, such as “sympathetic plexus blocks, spinal cord stimulation (SCS), dorsal root ganglion stimulation (DRG-S), peripheral nerve stimulation (PNS), and intrathecal drug delivery system (IDDS).”4 CRPS management is symptomatic and involves physical/occupational therapy, psychological therapy, neuropathic pain medications, anti-inflammatory drugs, and interventional procedures. Physical and occupational therapy are crucial in helping patients cope with pain-related fears. Therapeutic modalities include massage, electrotherapy, acupuncture, contrast baths, biofeedback, and isometric strengthening exercises. CRPS treatment plans are often a multilayered approach, integrating a combination of physical rehabilitation with occupational and psychological therapy.9-11
Pharmacological therapy with nonsteroidal anti-inflammatory drugs (NSAIDs) can provide anti-inflammatory effects and reduce pain in CRPS, particularly in the initial months. Gabapentin shows evidence from randomized controlled trials (RCTs) in reducing pain in CRPS patients. An RCT conducted in 2016 examined the effectiveness of amitriptyline and gabapentin for CRPS I treatment and found that both drugs were equally effective for lowering pain levels and resulted in higher sleep quality.9-12
In our case, the patient with CRPS type II experienced difficult-to-manage symptoms in the left index finger, despite having undergone treatment with NSAIDs, gabapentin, and amitriptyline. Aside from the injury and a history of orthopedic surgery, the patient did not have other risk factors for disease onset and persistence. The patient was treated with an ultrasound-guided left median nerve block with 2 mL of lidocaine 1%, followed by hydrodissection with dextrose 5% 2 mL. Pharmacological therapy involved mecobalamin every 12 hours. The patient showed positive outcomes, being pain-free and recovering fully in terms of general symptoms, sensory, motor, and reflex functions. Additionally, the patient experienced improved sleep quality and successfully returned to work without experiencing any pain.
Ultrasound-guided hydrodissection is an emerging interventional option in the management of CRPS type II associated with post-traumatic nerve injury. Unlike prolotherapy, which primarily targets chronic soft tissue injuries through regenerative pathways, hydrodissection focuses on mechanically separating the nerve from surrounding adhesions or fibrotic tissue to relieve entrapment and reduce neuropathic pain. In a novel case report, Smith et al. successfully treated a 64-year-old woman with CRPS type II due to median and ulnar nerve injuries using ultrasound-guided hydrodissection.13 The injectate consisted of 1% lidocaine, methylprednisolone, and normal saline. The procedure resulted in complete symptom relief lasting 3 to 12 weeks and was safely repeated multiple times over three years. This is the first reported use of ultrasound-guided hydrodissection as a treatment for CRPS type II due to compressive neuropathies using steroids, demonstrating promising results where conventional pharmacologic and interventional therapies had failed.13
In our study, we employed the hydrodissection technique to manage CRPS caused by nerve injury, but unlike previous studies, an injectate containing 5% dextrose was used. Dextrose 5% can have both mechanical and pharmacological effects. Mechanically, hydrodissection creates fluid pressure that helps separate the nerve from surrounding tissues, progressively reducing adhesions, improving vascular supply, and restoring nerve mobility. The pharmacological effects of dextrose are less clearly defined, but may involve neural membrane stabilization, modulation of glucose metabolism, and reduction of neurogenic inflammation—factors that can contribute to the alleviation of neuropathic pain.15 During the final follow-up, 21 months after the interventional procedure, the patient demonstrated full recovery: normal sensory function, absence of tingling or allodynia, no limitations in activities of daily living or work, and complete resolution of pain.
4. CONCLUSION
CRPS is an intricate condition due to various mechanisms coming into play. Despite advances in therapeutic strategies, no single intervention has proven universally effective. This case report introduces a novel, minimally invasive management approach using ultrasound-guided interventional pain management (IPM) with dextrose prolotherapy via hydrodissection for a 27-year-old male with CRPS caused by nerve injury affecting the left index finger. This innovative technique led to a favorable outcome, including a complete pain-free state, resolution of sensory, motor, and reflex abnormalities, improved sleep quality, and a full return to work without limitations. To our knowledge, this is the first report demonstrating long-term remission of CRPS symptoms using dextrose-based ultrasound-guided nerve hydrodissection.
Authors affiliations:
- Theresia Chandra Tania Novy, Bandung Pain Rehab Center, Jl. Supratman No. 57, Cihapit, Bandung, West Java, Indonesia, 40114; Email: theresianovymd@gmail.com
- Hemant Kalia, Center for Research & Innovation in Spine & Pain, Supratman Street No. 57, United States of America; ORCID: 0000-0001-9033-9080; Email: drhemantkalia@gmail.com
- Yu Chuan (Grace) Tsai, Center of Pain Management, E-Da Cancer Hospital, Kaohsiung, Taiwan; Email: t3589476@gmail.com
ABSTRACT
Complex Regional Pain Syndrome (CRPS) is a chronic neuropathic condition marked by pain disproportionate to the initial trauma, often accompanied by hyperalgesia, allodynia, and autonomic dysfunction. It commonly follows surgery, trauma, or nerve injury. This case report highlights the use of ultrasound-guided hydrodissection with dextrose prolotherapy as a minimally invasive approach to managing CRPS secondary to nerve injury.
A 27-year-old male presented with persistent pain, paresthesia, hypersensitivity, and intermittent shock-like sensations from the left index finger radiating to the upper back, occurring after surgical wire removal for a finger fracture. Clinical and ultrasound findings supported the diagnosis of CRPS type II (causalgia) due to nerve injury. The patient was treated with ultrasound-guided perineural hydrodissection using 5% dextrose to reduce nerve adhesion and irritation. Pain was assessed using the Numeric Rating Scale (NRS) at baseline, one week post-procedure, monthly for 12 months, and at a 21-month follow-up. The patient demonstrated sustained improvement in pain and sensory function without complications.
This case illustrates the potential of ultrasound-guided dextrose hydrodissection as a safe and effective treatment for CRPS caused by nerve injury. Larger studies are warranted to validate its efficacy and elucidate underlying mechanisms.
Abbreviations: CRPS: Complex Regional Pain Syndrome, IPM: Interventional Pain Medicine, NRS: Numeric Rating Scale, ORIF: Open Reduction and Internal Fixation, NSAIDs: Nonsteroidal Anti-Inflammatory Drugs
Keywords: Complex Regional Pain Syndrome; dextrose prolotherapy; hydrodissection; interventional pain management; ultrasound-guided injection
Citation: Novy TCT, Kalia H, Tsai YCG.Novel treatment of complex regional pain syndrome using hydrodissection with dextrose prolotherapy. Anaesth. pain intensive care 2025;29(7):808-813. DOI: 10.35975/apic.v29i7.2973
Received: Jul 12, 2025; Revised; August 27, 2025; Accepted: August 27, 2025
1. INTRODUCTION
Complex Regional Pain Syndrome (CRPS) is a chronic neurological condition that causes debilitating pain, and a common indicator is allodynia and hyperalgesia in the extremities. It may also involve dystrophic changes, such as pale, cold skin. In the past, this syndrome has been referred to as "reflex sympathetic dystrophy", "causalgia", "algoneurodystrophy", and "Sudeck atrophy". CRPS is classified into two types: CRPS-I and CRPS-II. Their differences lie in the presence of definite nerve damage. CRPS type I develops in the absence of definite damage to the nerve, whereas CRPS type II occurs only when there is confirmed neuropathy.1,2
The prevalence of CRPS ranges from 6.28 to 26.2 per 100,000 person-years. Its common indicators include chronic pain, pain hypersensitivity, and/or allodynia accompanied by edema or changes in sudomotor activity, typically affecting the distal extremities.1,3 A set of signs and symptoms referred to as the Budapest criteria has been developed; however, accurate diagnosis of CRPS remains a challenge due to various knowledge gaps regarding the pathophysiology of CRPS. Neuropathic inflammation, particularly the activation of peripheral C-fiber nociceptors and the autonomic nervous system, has been shown to be pivotal in the development of CRPS.1 However, the exact etiology of the condition likely lies in different interactions between several mechanisms, such as central sensitization and neuroplastic alterations.3
Injuries occurring in the extremities, such as fractures, dislocations, past surgical interventions, and carpal tunnel syndrome, are the most common triggers for CRPS. In a 2018 study cited by Taylor et al., it was found that of 1043 patients diagnosed with CRPS, 441 (42%) were caused by fractures, 214 (21%) by blunt traumatic injuries excluding fractures, 124 (12%) by prior surgical history, 69 (7%) by carpal tunnel syndrome, 47 (5%) by sharp traumas, and 77 (7%) cases had no clear triggering event.1 CRPS symptoms show varying progression over time, making early initiation of therapy crucial for patient prognosis. The goals are to reduce pain, restore limb functionality, and improve quality of life. This will involve a multifaceted plan incorporating patient-centered education, therapy (physical and occupational), psychiatry, pain medicine specialists, as well as surgical and pharmacological solutions.4,5
The most used treatment for CRPS is sympathetic blockade, mainly due to its minimally invasive nature. Despite its popularity, there is limited evidence regarding its short-term and long-term analgesic effects.1 In a 2019 study of 255 out of 318 patients diagnosed with CRPS (80%), 155 experienced over 50% pain reduction. Most of the patients (71%) reported pain reduction for 1–4 weeks, while 14% experienced pain reduction for more than a month. Data from this study showed clinical significance and acted as pioneering evidence for the use of sympathetic blockade in the treatment of CRPS.4,5
This case report presents a novel management approach using ultrasound-guided interventional pain medicine (IPM) with hydrodissection and dextrose prolotherapy, which yielded satisfactory outcomes in a 27-year-old male patient with CRPS due to a nerve injury in the left index finger.
2. CASE REPORT
A 27-year-old male patient reported nine months of hypersensitivity in his left index finger, triggered by touch and causing electric shock-like pain radiating to his shoulder. Additional symptoms included nighttime numbness, tingling, dizziness, and cold, pale skin. He had undergone open reduction and internal fixation (ORIF) with wire placement for a work-related finger fracture 1.5 years prior, followed by wire removal surgery nine months ago—after which his symptoms began immediately. Activities such as push-ups and sensory exercises exacerbated the pain. During fieldwork, he experienced intense pain when holding tools, often resulting in tools falling out of his grasp. These occurrences posed safety risks, resulting in his reassignment from field duties to an office role. Despite treatment with amitriptyline and gabapentin prescribed by his occupational physician, his symptoms persisted, interfering with sleep and daily activities. He also reported dizziness as a side effect of gabapentin.
The patient was in a generally good condition, fully conscious, with normal vital signs and body mass index. Physical examination showed normal wrist movement and no neurological deficits, except for increased pain sensitivity (hyperalgesia) at the tip of the left index finger. Sensory and motor tests are summarized in Table 1.
| Table 1: Sensory function was assessed using light touch and pinprick testing | ||
| Spinal Level | Sensory Function (R / L) | Motor Function (R / L) |
| C5 | 10 / 10 | 5 / 5 |
| C6 | 10 / 8 | 5 / 5 |
| C7 | 10 / 8 | 5 / 5 |
| C8 | 10 / 8 | 5 / 4 |
| T1 | 10 / 8 | 5 / 4 |
| Sensory function scored on a scale from 0 to 10 (normal = 10). Motor strength was graded on a scale from 0 to 5 (normal = 5). The examination revealed localized hyperalgesia at the tip of the left index finger, with otherwise normal motor function in most muscle groups. | ||
Ultrasound examination of the finger revealed fibrotic tissue without neovascularization, consistent with a nerve injury (Figure 1).
Figure 1: Ultrasound examination of the left index finger showing fibrotic tissue without neovascularization, consistent with nerve injury.
This patient fulfilled all the Budapest criteria for CRPS type II caused by nerve injury. He had persistent, excessive pain for nine months following wire removal after ORIF, described as electric shock-like pain radiating to the shoulder. Furthermore, the patient exhibited symptoms across all categories: sensory (touch hypersensitivity, hyperalgesia, and allodynia), vasomotor (cold, pale skin), and motor/trophic (functional impairment affecting daily activities and work duties). Alternative diagnoses did not adequately account for his symptoms. The case was classified as CRPS type II due to a documented nerve injury related to the wire removal surgery, with symptoms emerging after a known insult.
We proceeded with a left median nerve block followed by hydrodissection. Pain was reassessed using the Numeric Rating Scale (NRS). The patient underwent ultrasound-guided interventional pain management (IPM), starting with a left median nerve block using 2 cc of 1% lidocaine, followed by hydrodissection with 2 cc of 5% dextrose. After the procedure, his pain score dropped to 0/10, and the affected finger was no longer pale or cold. The patient was then prescribed acetaminophen-tramadol every 12 hours and amitriptyline for one week. Additionally, gabapentin was tapered from 300 mg to 100 mg every 8 hours. He was advised to maintain a pain diary and to return for a follow-up in one week.
At the one-week follow-up, the tingling had decreased by 75% and was limited to the wrist. Furthermore, the finger appeared warm with improved vascularity. Dizziness had resolved, object handling had improved, and sleep quality had improved. The patient was given a new prescription of acetaminophen-tramadol every 24 hours for one week, while amitriptyline was discontinued, and gabapentin was further tapered to 100 mg once daily. He remained in an office-based work role.
By one month, all symptoms had resolved. The patient resumed fieldwork and continued mecobalamin 500 mcg twice daily for six months. Gabapentin was discontinued, and dizziness did not recur. At the 12- and 21-month follow-ups, he remained symptom-free and was able to perform work, daily activities, and sports without disruptions. The clinical progress of the patient is summarized in Figure 2 and Table 2.
Figure 2: Clinical progression of the patient following ultrasound-guided hydrodissection with 5% dextrose. Pain intensity, sensory symptoms, and functional improvement were monitored at baseline, 1 week, 1 month, 12 months, and 21 months post-procedure, showing sustained resolution of symptoms
| Table 2: Clinical progression of the patient | |||
| Time points | NRS Score | Sensory Function (C5, C6, C7, C8, T1) | Tingling Sensation |
| Before IPM | 10/10 | C5:10/10; C6: 0/8; C7: 0/8; C8: 10/8; T1: 10/8 | Yes |
| Right after IPM | 0/10 | C5: 0/10; C6: 10/9; C7: 0/9; C8: 10/9; T1: 10/9 | Yes |
| 1 week after IPM | 2/10 | C5: 10/10; C6: 0/10; C7: 0/10; C8: 10/10; T1: 10/10 | Yes |
| 1 month after IPM | 0/10 | C5: 10/10; C6: 10/10; C7: 10/10; C8: 10/10; T1: 10/10 | No |
| 12 months after IPM | 0/10 | C5: 10/10; C6: 10/10; C7: 10/10; C8: 10/10; T1: 10/10 | No |
3. DISCUSSION
CRPS is a neurological condition that causes debilitating pain and often involves pain hypersensitivity (hyperalgesia) and allodynia in the extremities. Injuries in the extremities, such as fractures, sprains, surgical history, and carpal tunnel syndrome, are the most common triggers for CRPS.3 CRPS type II can be associated with identifiable nerve injuries. These injuries disrupt normal nerve conduction due to trauma, inadequate surgical repair, or chronic fibro-inflammatory processes. Such disruption can hinder the reinnervation process, especially when scar tissue obstructs nerve regeneration. Rather than representing a malignant neoplasm, this condition reflects a non-neoplastic, localized proliferation and dysregulation of injured nerve fibers.4,5 In this study, we outline the treatment of a 27-year-old male who presented to the Bandung Pain Rehab Center with complaints of hypersensitivity in the left index finger. The symptoms worsened with touch, leading to a sensation of electric shock extending to the left shoulder and numbness (paresthesia).
In a study of over 33 million patients (2007–2011), 22,533 (0.07%) were diagnosed with CRPS. A 2018 study by Ott and Maihöfner in Germany showed similar trends, with CRPS being more common in women (71%) than men (29%). The condition mostly affects the upper limbs (70% of cases), and CRPS type I is more common than type II (88% vs. 12%). Distal injuries, such as forearm fractures, are more likely to lead to CRPS than proximal fractures. Additionally, musculoskeletal conditions like rheumatoid arthritis, high-energy trauma, and severe fractures increase the risk of developing CRPS.6 Our case presents a male patient with CRPS type II, contrasting epidemiological studies where CRPS type I is typically more common, with a higher prevalence in women. On the other hand, this case report aligns with the literature, indicating that injury or trauma is the most common cause of CRPS.
No precise test has been developed for CRPS, which makes diagnosis difficult. The Budapest Criteria were developed and have now become the standard for diagnosing CRPS. These criteria maintain high sensitivity for CRPS (0.99), but significantly improve the specificity of the IASP diagnostic criteria (0.41-0.68). This patient met all the Budapest criteria, with continuing excessive pain to any triggering event. The patient reported and displayed symptoms in three of four categories: hyperesthesia, temperature asymmetry, skin color changes, and motor dysfunction (tremor and dystonia). To further quantify disease severity, the CRPS Severity Score (CSS) was introduced in 2010. This score includes 17 distinct symptoms, with each symptom being assigned 1 point.6–8
Her et al., outline several treatments for CRPS, such as “sympathetic plexus blocks, spinal cord stimulation (SCS), dorsal root ganglion stimulation (DRG-S), peripheral nerve stimulation (PNS), and intrathecal drug delivery system (IDDS).”4 CRPS management is symptomatic and involves physical/occupational therapy, psychological therapy, neuropathic pain medications, anti-inflammatory drugs, and interventional procedures. Physical and occupational therapy are crucial in helping patients cope with pain-related fears. Therapeutic modalities include massage, electrotherapy, acupuncture, contrast baths, biofeedback, and isometric strengthening exercises. CRPS treatment plans are often a multilayered approach, integrating a combination of physical rehabilitation with occupational and psychological therapy.9-11
Pharmacological therapy with nonsteroidal anti-inflammatory drugs (NSAIDs) can provide anti-inflammatory effects and reduce pain in CRPS, particularly in the initial months. Gabapentin shows evidence from randomized controlled trials (RCTs) in reducing pain in CRPS patients. An RCT conducted in 2016 examined the effectiveness of amitriptyline and gabapentin for CRPS I treatment and found that both drugs were equally effective for lowering pain levels and resulted in higher sleep quality.9-12
In our case, the patient with CRPS type II experienced difficult-to-manage symptoms in the left index finger, despite having undergone treatment with NSAIDs, gabapentin, and amitriptyline. Aside from the injury and a history of orthopedic surgery, the patient did not have other risk factors for disease onset and persistence. The patient was treated with an ultrasound-guided left median nerve block with 2 mL of lidocaine 1%, followed by hydrodissection with dextrose 5% 2 mL. Pharmacological therapy involved mecobalamin every 12 hours. The patient showed positive outcomes, being pain-free and recovering fully in terms of general symptoms, sensory, motor, and reflex functions. Additionally, the patient experienced improved sleep quality and successfully returned to work without experiencing any pain.
Ultrasound-guided hydrodissection is an emerging interventional option in the management of CRPS type II associated with post-traumatic nerve injury. Unlike prolotherapy, which primarily targets chronic soft tissue injuries through regenerative pathways, hydrodissection focuses on mechanically separating the nerve from surrounding adhesions or fibrotic tissue to relieve entrapment and reduce neuropathic pain. In a novel case report, Smith et al. successfully treated a 64-year-old woman with CRPS type II due to median and ulnar nerve injuries using ultrasound-guided hydrodissection.13 The injectate consisted of 1% lidocaine, methylprednisolone, and normal saline. The procedure resulted in complete symptom relief lasting 3 to 12 weeks and was safely repeated multiple times over three years. This is the first reported use of ultrasound-guided hydrodissection as a treatment for CRPS type II due to compressive neuropathies using steroids, demonstrating promising results where conventional pharmacologic and interventional therapies had failed.13
In our study, we employed the hydrodissection technique to manage CRPS caused by nerve injury, but unlike previous studies, an injectate containing 5% dextrose was used. Dextrose 5% can have both mechanical and pharmacological effects. Mechanically, hydrodissection creates fluid pressure that helps separate the nerve from surrounding tissues, progressively reducing adhesions, improving vascular supply, and restoring nerve mobility. The pharmacological effects of dextrose are less clearly defined, but may involve neural membrane stabilization, modulation of glucose metabolism, and reduction of neurogenic inflammation—factors that can contribute to the alleviation of neuropathic pain.15 During the final follow-up, 21 months after the interventional procedure, the patient demonstrated full recovery: normal sensory function, absence of tingling or allodynia, no limitations in activities of daily living or work, and complete resolution of pain.
4. CONCLUSION
CRPS is an intricate condition due to various mechanisms coming into play. Despite advances in therapeutic strategies, no single intervention has proven universally effective. This case report introduces a novel, minimally invasive management approach using ultrasound-guided interventional pain management (IPM) with dextrose prolotherapy via hydrodissection for a 27-year-old male with CRPS caused by nerve injury affecting the left index finger. This innovative technique led to a favorable outcome, including a complete pain-free state, resolution of sensory, motor, and reflex abnormalities, improved sleep quality, and a full return to work without limitations. To our knowledge, this is the first report demonstrating long-term remission of CRPS symptoms using dextrose-based ultrasound-guided nerve hydrodissection.
5. Conflict of interest
All authors declare that there was no conflict of interest.6. Funding
This study received no funding regarding this study.7. Authors’ contribution
All authors took part in conceptualization, methodology, investigation, writing, review & editing this manuscript.8. REFERENCES
- Taylor SS, Noor N, Urits I, Paladini A, Sadhu MS, Gibb C, et al. Complex Regional Pain Syndrome: A Comprehensive Review. Pain Ther. 2021;10:875–92. [PubMed] DOI: 1007/s40122-021-00279-4
- Alshehri FS. The complex regional pain syndrome: Diagnosis and management strategies. Neurosciences (Riyadh). 2023;28(4):211–9. [PubMed] DOI: 17712/nsj.2023.4.20230034
- Abd-Elsayed A, Stark CW, Topoluk N, Isaamullah M, Uzodinma P, Viswanath O, et al. A brief review of complex regional pain syndrome and current management. Ann Med. 2024;56(1):2334398 [PubMed] DOI: 1080/07853890.2024.2334398
- Her YF, Kubrova E, Dombovy-Johnson M, ElSaban M, Mostert K, D’Souza RS. Complex Regional Pain Syndrome: Updates and Current Evidence. Curr Phys Med Rehabil Rep. 2024;12(2):50–70. DOI: 1007/s40141-023-00426-2
- Sobeeh MG, Hassan KA, da Silva AG, Youssef EF, Fayaz NA, Mohammed MM. Pain mechanisms in complex regional pain syndrome: a systematic review and meta-analysis of quantitative sensory testing outcomes. J Orthop Surg Res. 2023;18(1):2. [PubMed] DOI: 1186/s13018-022-03461-2
- Shim H, Rose J, Halle S, Shekane P. Complex regional pain syndrome: a narrative review for the practising clinician. Br J Anaesth. 2019;123(4):e424–33. [PubMed] DOI: 1016/j.bja.2019.03.030
- Michels T. Peripheral neuropathic pain and pain related to complex regional pain syndrome with and without fixed dystonia – efficient therapeutic approach with local anesthetics. Local Reg Anesth. 2020;13:11–6. [PubMed] DOI: 2147/LRA.S229315
- Sobeeh MG, Hassan KA, da Silva AG, Youssef EF, Fayaz NA, Mohammed MM. Pain mechanisms in complex regional pain syndrome: a systematic review and meta-analysis of quantitative sensory testing outcomes. J Orthop Surg Res. 2023;18(1): [Epub ahead of print] [PubMed] DOI: 1186/s13018-022-03461-2
- Kessler A, Yoo M, Calisoff R. Complex regional pain syndrome: An updated comprehensive review. NeuroRehabilitation. 2020;47(3):253–64. [PubMed] DOI: 3233/NRE-208001
- Ferraro MC, Cashin AG, Wand BM, Smart KM, Berryman C, Marston L, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome- an overview of systematic reviews. Cochrane Database Syst Rev. 2023;2023(6): [PubMed] DOI: 10.1002/14651858.CD009416.pub3
- Thor JA, Hanapi NHM, Halil H, Suhaimi A. Perineural injection therapy in the management of complex regional pain syndrome: A sweet solution to pain. Pain Med. 2017;18(10):2041–5. [PubMed] OI: 1093/pm/pnx063
- Jang KS, Kim HS. Treatment for acute stage complex regional pain syndrome type II with polydeoxyribonucleotide injection. J Korean Neurosurg Soc. 2016;59(5):529–32. [PubMed] DOI: 3340/jkns.2016.59.5.529
- Hauser RA, Brinker DK. The Theoretical Basis for and Treatment of Complex Regional Pain Syndrome with Prolotherapy. J Prolother. 2010;2(2):356-370. Full Text
- Smith MD, Schroeder AN, Helm E. A novel treatment for type 2 complex regional pain syndrome caused by median and ulnar compressive neuropathies: a case report. PM R. 2020;12(S1). Full Text
- Chao TC, Reeves KD, Stanley Lam KH, Li TY, Wu YT. The Effectiveness of Hydrodissection with 5% Dextrose for Persistent and Recurrent Carpal Tunnel Syndrome: A Retrospective Study. J Clin Med. 2022;11(13):3794. [PubMed] DOI: 3390/jcm11133705