Zahraa Ismail Abbas 1*, Haider Salih Jaffat 2
Author affiliations:
Background & objective: Atherosclerosis affects the large and medium arteries and is a chronic inflammatory condition. It is intimately linked to dyslipidemia and entails the accumulation of lipid-rich plaques.
Its progression is impacted by lipid abnormalities and immune-inflammatory responses. This study focuses on significant lipid indicators, including triglycerides, cholesterol, VLDL, HDL, and Lp-PLA₂. It also looks at different hematological parameters and inflammatory markers like CD40. This study aims to investigate the biochemical relationships between these markers in patients with atherosclerosis and find viable multi-marker panels for better risk prediction.
Methodology: In a case-control study, 90 people between the ages of 45 and 65 were split into three groups: 30 atherosclerosis patients with diabetes and hypertension, 30 pathological controls who had both conditions but no atherosclerosis, and 30 healthy controls. Hematological characteristics, inflammatory markers (Lp-PLA₂, CD40), and lipid profiles were examined in fasting blood samples. Spectrophotometric and ELISA methods were used. Statistical analysis was carried out with SPSS v26.
Results: Lp-PLA₂ and CD40 levels were significantly greater in atherosclerosis patients, suggesting increased vascular inflammation and immunological activation. The patient group had considerably reduced HDL and significantly greater triglycerides, cholesterol, and VLDL. According to hematological data, patients had higher WBC and Hb, while pathological controls had higher lymphocyte counts. Correlation analysis revealed a strong positive association between triglycerides (TG) and total cholesterol (R = 0.722, P < 0.001). In contrast, Lp-PLA₂ showed no significant correlation with lipid parameters, suggesting that it may play an independent role in vascular inflammation. A weak correlation was observed between CD40 and lymphocyte percentage.
Conclusions: The results highlight how crucial it is to combine inflammatory and lipid markers, such as CD40 and Lp-PLA₂, to comprehend the pathophysiology of atherosclerosis. These biomarkers could be helpful in risk assessment and early diagnosis. Lp-PLA₂'s function as a unique inflammatory marker in atherosclerosis is highlighted by the lack of connection it exhibits with conventional lipid markers.
Abbreviations: Lp-PLA₂: Lipoprotein-associated phospholipase A2, HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very-low-density lipoprotein, TG: Triglycerides, CD40: Tumor Necrosis Factor Receptor Superfamily Member 5 (TNFRSF5), Hb: Hemoglobin, WBC: White blood cell, PLT: Platelet, LYM: Lymphocytes
Keywords: Atherosclerosis; Lp-PLA₂; CD40; Lipid profile; Inflammatory biomarkers; Hematological indices
Citation: Abbas ZI, Jaffat HS. Interplay of inflammatory and lipid biomarkers in atherosclerosis: role of Lp-PLA₂, CD40, and hematological indices; a case control study. Anaesth. pain intensive care 2025;29(6):770-778. DOI: 10.35975/apic.v29i7.2960
Received: June 25, 2025; Revised: July 10, 2025; Accepted: July 20, 2025
Atherosclerosis is a chronic inflammatory disease of large and medium-sized arteries that is distinguished by the accumulation of plaques that contain lipids inside the artery walls. Peripheral arterial disease, ischemic stroke, and coronary artery disease are some of its manifestations. Atherosclerosis risk is causally linked to dyslipidemia, which is characterized by decreases in high-density lipoprotein (HDL) and increases in plasma levels of low-density lipoprotein (LDL) and triglycerides.1,2
Recent developments highlight the role that lipid-related and inflammatory indicators play in the development and progression of atherosclerosis. Several lipid types, including small dense LDL (sdLDL), oxidized LDL (oxLDL), and low-density lipoprotein (LDL) cholesterol, have been studied in relation to the development and course of atherosclerosis. The formation and fragility of plaques are influenced by the malfunction and inflammatory processes that these lipoproteins support. Furthermore, atherosclerosis has been connected to specific lipid-related proteins and enzymes, underscoring the intricate relationship between inflammation and lipid metabolism in this condition. The functions of lipids, enzymes, and regulatory proteins in the mechanisms producing atherosclerosis are examined in this article. Additionally, it will discuss new and existing treatments that target these molecular pathways in an attempt to understand atherosclerosis and guide future treatment strategies. 3,4
The enzyme Lp-PLA2, which is primarily produced by leukocytes, plays a crucial role in vascular inflammation. Its participation in atherosclerosis is highlighted by the fact that it is present in the necrotic core of atherosclerotic plaques. Lp-PLA2 levels are elevated in patients with intracranial atherosclerotic disease (ICAD) and are linked to more complex and irregular plaques. According to certain research, Lp-PLA2 activity (Lp-PLA2-A) can be a more accurate indicator of vascular events than its mass. However, due to the lack of pathology data from ICAD cases, there is currently insufficient evidence to establish the role of inflammation in ICAD-related stroke 5,6
CD40 and CD40 ligand (CD40L, CD154) are important co-stimulatory and immunological checkpoints that are essential to the adaptive immune response. Members of the tumor necrosis factor receptor and its ligand superfamily, CD40 and CD40L, can interact to trigger an immunological response. Inflammatory or autoimmune disorders, particularly atherosclerosis, are significantly influenced by the CD40-CD40L system, according to research conducted over the past 30 years. The interaction between CD40 and CD40L, which are present on the surface of immune cells, is essential for immunological signaling. Many immunological activities are compromised in the absence of this interaction, even though T and B cell responses can still occur. For instance, it is necessary for the formation of follicular helper T cells (TFH) in germinal centers, B cell differentiation, proliferation, and antibody class switching. The CD40-CD40L pathway affects hematopoietic and non-hematopoietic stem cells in addition to B cells. 7,8
Hematological indicators, including hemoglobin levels, platelet counts, lymphocyte counts, and white blood cell (WBC) counts, also provide information on the inflammatory state of the vascular system. These metrics are readily available and reasonably priced indicators that might represent long-term, low-grade inflammation linked to atherogenesis.
Hemoglobin (Hb), WBC, PLT, and lymphocytes (LYM) are hematological indicators that have been linked to cardiovascular and metabolic disorders. WBC and PLT levels are frequently high in people with metabolic syndrome (MetS), which exacerbates vascular inflammation and atherosclerosis. Atherogenic processes are further promoted by increased platelet-leukocyte contacts. Furthermore, anomalies in lymphocyte profiles and hemoglobin levels could be signs of increased cardiovascular risk. 9, 10
In this study, we will investigate how lipid indicators (Lp-PLA₂, VLDL, HDL, cholesterol, and TG) and inflammatory markers (CD40, hematological indices) interact in individuals with atherosclerosis. The goal of the study is to understand the biochemical interactions that underlie the disease and to find viable multi-marker panels for risk assessment by looking at their correlations and relevance.
This case-control study included ninety participants, divided into three groups:
Participants ranged in age from 45 to 65. The diagnosis of vascular disease and atherosclerosis was confirmed by diagnostic catheterization and ultrasound imaging. All participants had their fasting blood samples taken in the morning at the Open-Heart Center of Al-Sadr Medical City, situated in Al-Najaf Al-Ashraf, Iraq. All participants underwent a comprehensive medical evaluation to screen for additional underlying diseases, including kidney illness, chronic inflammation, or thyroid issues that could affect the study's findings.
2.1. Blood sample collection
Sample collection was conducted over the course of four months. After a 10-hour fast, five milliliters
of venous blood were extracted in the morning from both patients and control subjects (without a tourniquet) using disposable needles and plastic syringes. After that, the materials were put into gel tubes and centrifuged for 15 minutes at 3000 rpm to separate their constituent parts.
2.2. Serum level of cytokine
Lipoprotein-associated Phospholipase A2 (Lp-PLA₂) and CD40 blood levels were assessed using the Enzyme-Linked Immunosorbent Assay (ELISA) technique. Both assays were carried out using ELISA kits provided by BT LAB (China) in compliance with the manufacturer's instructions.
2.3. Serum level of lipid profile and glycemic markers
The spectrophotometric method was used to evaluate the amount of cholesterol, triglycerides (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) in the serum. Spinreact (Spain) provided specific test kits for each parameter. Glycated hemoglobin (HbA1c) and fasting blood glucose (FBG) levels were also measured. Using Spinreact kits (Spain), the manufacturer's protocol was followed to detect FBG using the glucose oxidase-peroxidase technique and quantify HbA1c using a turbidimetric inhibition immunoassay.
2.4. Hematological Parameters
Total white blood cells (WBC), lymphocytes (LYM), hemoglobin (Hb), and platelet count (PLT) were measured using an automated hematology analyzer (such as the Sysmex XN-Series) for the complete blood count (CBC). These metrics were used to evaluate the research groups' overall hematological health and any alterations linked to inflammation.
2.5. Statistical Analysis
Statistical software (SPSS 26) was used to do statistical calculations on the data gathered from the study of biochemical data. The F-distribution analysis's mean, standard deviation, and findings were acquired.
3.1. Demographic Characteristics
Table 1 shows the study population's demographic details. The mean age of patients with atherosclerosis was (55.83 ± 9.23), (55.03 ± 10.89) for pathological controls, and (55.76 ± 10.07) for healthy controls, with no significant difference. But there was a significant difference in weight between the groups (P = 0.001). The mean weight was highest among patients (85.48 ± 7.51 kg), lowest among pathological controls (66.77 ± 8.62 kg), and highest among healthy controls (76.00 ± 12.80 kg).
3.2. Inflammatory biomarkers: Lp-PLA₂ and CD40
Table 2 presents the serum levels of Lipoprotein-associated Phospholipase A2 (Lp-PLA₂) and CD40 in atherosclerosis patients in contrast to both healthy and pathological control groups. The findings show that the patient group's levels of CD40 and Lp-PLA₂ have significantly increased. Patients had significantly higher amounts of Lp-PLA₂ than both diseased and healthy controls, which may indicate increased vascular inflammation. Similarly, the patient group's CD40 levels were noticeably higher, indicating immunological activation linked to the advancement of atherosclerosis.
3.3. Lipid profile and arterial stiffness index
Table 3 showed that triglyceride, total cholesterol, and VLDL levels were considerably greater in atherosclerosis patients than in both pathological and healthy controls (P < 0.01), even if the patients' HDL was lower and their LDL was higher.
3.4. Hematological Parameters
Table 4 showed significant differences between the groups in hemoglobin, platelets, WBC, and lymphocyte percentage (P = 0.001). Compared to healthy controls, atherosclerosis patients had greater WBC and Hb levels, pathological controls had the highest lymphocytes, and both patient and pathological groups had more platelets.
3.5. Correlation between all variables in atherosclerosis patients
All parameters in patients and controls were examined for potential associations using the Spearman correlation test. The results of this study showed a substantial and significant positive connection between triglycerides (TG) and total cholesterol (CHO) (R = 0.722, P < 0.001), suggesting that these two lipid components are closely related in patients.
On the other hand, despite weak positive and negative tendencies, Lp-PLA₂ did not exhibit any statistically significant association with HDL, LDL, VLDL, TG, or total cholesterol. The lack of a significant association raises the possibility that Lp-PLA₂ functions independently of conventional lipid indicators and represents vascular inflammation as opposed to dyslipidemia. While CD40 did not exhibit significant associations with either lipid parameters or Lp-PLA₂, it did show a somewhat favorable correlation with lymphocyte percentage (LYM), suggesting that it may be linked to immunological activation in individuals with atherosclerosis. Additionally, LYM's involvement in lipid-associated immune responses was demonstrated by its negative correlation with LDL and positive correlation with HDL. Hemoglobin (Hb) and WBC had a negative correlation, which could be an indication of oxidative stress or systemic inflammation. VLDL and platelet count (PLT) had a significant negative correlation, which may indicate that thrombocyte activity and VLDL are inversely related.
3.6. Diagnostic value of Lp-PLA₂ and CD40
The receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of Lp-PLA₂ and CD40 in discriminating patients with atherosclerosis from pathological controls and healthy individuals.
With a 95% CI of 0.886–0.985 and P = 0.0001, the area under the curve (AUC) for Lp-PLA₂ was 0.936. The test's sensitivity was 91.3% and its specificity was 84.4% at a cut-off value of 33.63.
An AUC of 0.880, 95% CI = 0.808–0.953, and P = 0.0001 was found for CD40. As indicated in Table 5, Figure 1, the test obtained a sensitivity of 87.0% and a specificity of 80.0% at the cut-off value of 17.95.
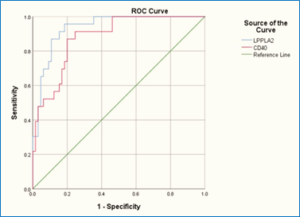
Figure 1: ROC curve demonstrating the diagnostic performance of CD40 and Lp-PLA2 in patients with atherosclerosis
Table 3 presents data demonstrating a statistically significant increase (P < 0.01). In atherosclerosis patients, serum levels of triglycerides (TG), total cholesterol (CHO), and very-low-density lipoprotein (VLDL) were higher than in both diseased and healthy controls. This increase reflects the well-known function of dyslipidemia in the development of atherosclerosis. The results of this study are consistent with those of Zachariah, who reported that high TG and LDL levels, along with low HDL, contribute to the development of atherosclerosis. Elevated TG affects HDL function via lipid exchange processes, resulting in a detrimental lipid profile with increased VLDL and LDL and decreased HDL, as found in high-risk individuals.11
The observed lipid changes are most likely due to increased insulin resistance and metabolic imbalance, which are typically seen in people with diabetes and vascular dysfunction. This imbalance increases hepatic synthesis of triglycerides and cholesterol, which are then released into the bloodstream, causing endothelial damage and plaque development. Furthermore, atherosclerosis is regarded as a chronic inflammatory disorder, and inflammation has been shown to promote lipid oxidation, resulting in hazardous chemicals such as oxidized LDL (ox-LDL), which exacerbate arterial wall damage and plaque instability. These pathways contribute to the typical profile of high LDL and low HDL levels found in such patients. 12, 13
Although the patient group had higher LDL levels and lower HDL levels, the differences were not statistically significant (P = 0.092 and P = 0.161, respectively). Nonetheless, the observed tendency matches the recognized pathophysiological concept in which oxidized LDL infiltrates arterial walls and triggers immunological responses, whereas low HDL inhibits reverse cholesterol transport. Together, these factors contribute to plaque progression and instability.14
This runs counter to the findings of Higashi (2023), who contends that triglycerides, VLDL, and LDL do not always cause atherosclerosis since their effects differ based on genetics, oxidative stress, and vascular resistance. The fact that some people with severe dyslipidemia yet have good endothelial function suggests that atherogenesis is not always caused by lipid abnormalities alone. The study suggests that dyslipidemia may occasionally function more as a modulator than as the main cause of the complicated illness known as atherosclerosis. 15
Table 4 reveals a significant alteration in hematological parameters in patients with atherosclerosis compared to both pathological and healthy control groups.
The white blood cell (WBC) count was observed to be considerably higher (P = 0.001) in atherosclerosis patients. This increase reflects an active systemic inflammatory response, which is a known feature of atherosclerotic disease. Elevated leukocyte counts are frequently associated with immune cell migration to vascular locations, which contributes to endothelial activation and damage. WBC, PLT, and lymphocyte counts were found to be highly predictive of acute coronary events and had prognostic significance.16, 17
latelet (PLT) count was also significantly higher (P = 0.001), indicating increased platelet activation and aggregation. This hyperactivity is frequent in atherothrombosis and plays an important role in plaque rupture and thrombus development. The increased platelet response exacerbates the pro-thrombotic condition seen in many cardiovascular diseases. It has been demonstrated that the PLT/WBC ratio and lymphocyte count can be used as early predictors of cardiovascular disease development and inflammation. 18,19
Hemoglobin (HB) levels in the atherosclerotic group were substantially higher than in the pathological controls. This could indicate a compensatory erythropoietic mechanism or a change in oxygen demand in tissues affected by vascular injury. It could also indicate a reaction to prolonged low-grade hypoxia in the inflamed vasculature. It has been reported that complete blood count measures such as WBC, lymphocytes, hemoglobin, and platelet indices are independently related to cardiovascular outcomes.2 Lymphocyte (LYM) percentages varied significantly among groups, indicating underlying immunological dysregulation. Lymphocytes are implicated in both innate and adaptive immunity pathways; therefore, their imbalance contributes to the inflammatory and immunological-mediated character of atherosclerosis. It has been demonstrated that the PLT/WBC ratio and lymphocyte count can be used as early predictors of cardiovascular disease development and inflammation. 21
hese hematological alterations provide credence to the notion that atherosclerosis is a long-term, immuno-inflammatory disease. Circulating blood components, particularly leukocytes and platelets, play essential roles in endothelial dysfunction, vascular inflammation, and plaque instability, resulting in disease development and consequences.
In contrast, research by Abate et al. (2023) found no significant differences in hemoglobin (Hb), platelet (PLT), or white blood cell (WBC) levels between individuals with atherosclerotic cardiovascular disease and those who were only at risk. Although a slight increase was observed in their comparison study, these changes were not statistically significant and did not consistently correlate with the severity of atherosclerosis. The study discovered that common ratios like platelet-to-lymphocyte (PLR) and neutrophil-to-lymphocyte (NLR) had limited predictive value, casting doubt on the validity of complete blood count (CBC) parameters as stand-alone indicators of vascular damage or systemic inflammation in atherosclerosis. These findings imply that hematologic indicators' specificity and diagnostic value in cardiovascular pathology may be limited by non-atherosclerotic variables, including infection, stress, or metabolic problems.22
Table 5 presents several important correlations among lipid parameters, inflammatory markers, and hematological indicators in atherosclerosis patients. Total cholesterol and triglycerides (TG) showed a substantial positive connection (R = 0.722, P < 0.01), confirming the metabolic relationship between hepatic lipogenesis and circulating lipid levels. This association implies that an increase in endogenous triglyceride synthesis is frequently associated with higher cholesterol, both of which lead to atherogenic dyslipidemia. 23
While Lp-PLA₂ did not exhibit significant relationships with specific lipid markers, its slight negative correlation with cholesterol and TG may indicate its involvement as an inflammatory mediator rather than a direct lipid transporter. Lp-PLA₂ releases pro-inflammatory chemicals when it hydrolyzes the oxidized phospholipids in LDL particles. Its higher presence in atherosclerotic plaques suggests a relationship to oxidative stress, rather than classical lipid storage.24
Interestingly, CD40 revealed a strong positive connection with lymphocyte percentage (LYM) (R = 0.421, P = 0.046), indicating a function in immune cell activation. CD40 is a co-stimulatory protein that regulates T-cell and B-cell interactions. It has been shown to aggravate inflammation within the vascular wall by activating cytokine cascades and encouraging foam cell production. The link between CD40 and lymphocytes supports its immunomodulatory involvement in atherosclerotic pathogenesis. 25
In addition, LYM had a significant positive association with HDL (R = 0.466, P = 0.025) and a negative correlation with LDL (R = -0.441, P = 0.035), indicating that lymphocytes may have a protective function in lipid control. The inverse association between platelets (PLT) and VLDL (R = -0.483, P = 0.02) may reflect a thrombo-inflammatory interaction in which lipid-rich particles regulate platelet activity and contribute to vascular remodeling.25
A significant link was also found between WBC and hemoglobin (Hb), with a significant negative relationship (R = -0.439, P = 0.036), suggesting that systemic inflammation affects erythropoiesis or red blood cell turnover. Inflammatory conditions, such as atherosclerosis, are frequently accompanied by chronic illness, anemia, or stress erythropoiesis, which may explain this link. 26, 27
The relationships above demonstrate how intricately lipid metabolism, inflammation, and the immune system interact to cause atherosclerosis. Markers like Lp-PLA₂ and CD40, along with hematological data, offer insight into the disease's complex character and can be used for risk classification and monitoring disease activity.
Table 6 presents the receiver operating characteristic (ROC) analysis of CD40 and Lp-PLA₂, highlighting their potential as diagnostic biomarkers for atherosclerosis. The results show that both markers had a good discriminatory capacity between atherosclerosis patients and controls, with high sensitivity, specificity, and area under the curve (AUC).
Lp-PLA₂ achieved an AUC of 0.936 (95% CI: 0.886-0.985; P = 0.0001), showing high diagnostic accuracy. Lp-PLA₂ demonstrated 91.3% sensitivity and 84.4% specificity at a cut-off value of 33.63, suggesting that it may reliably distinguish between individuals with vascular inflammation and atherogenic risk and those who are not afflicted. This enzyme, produced by activated macrophages within plaques, reflects active oxidative stress and inflammation, making it a therapeutically useful diagnostic for vascular injury and development.28
Similarly, CD40 had an AUC of 0.880 (95% CI: 0.808-0.953; P = 0.0001), demonstrating superior diagnostic ability. At a threshold of 17.95, CD40 had 87% sensitivity and 80% specificity. CD40's increase is consistent with its role in increasing cytokine release, endothelial activation, and immune cell recruitment—all hallmarks of atherosclerosis progression.29
Several investigations have questioned the diagnostic reliability of Lp-PLA₂ and CD40 in the setting of atherosclerosis, which runs counter to the current findings. According to Adam et al. (2022), Lp-PLA₂'s utility as an early biomarker for vascular inflammation is limited because it is absent from early atherosclerotic lesions. Similarly, Abera et al. (2024) discovered that in patients with stable coronary artery disease, darapladib-induced Lp-PLA₂ inhibition did not significantly alter inflammatory or platelet indicators like CD40 ligand, indicating limited prognostic usefulness.30,31
The strong AUC values for both markers not only validate their individual diagnostic power but also highlight their combined efficacy in detecting the inflammatory and immune-mediated aspects of atherosclerosis, which standard lipid assays may not fully capture.
Including Lp-PLA₂ and CD40 in routine testing may improve the early detection of subclinical atherosclerosis, particularly in high-risk populations such as those with diabetes, hypertension, and metabolic syndrome. Their combined measurements may help stratify cardiovascular risk and guide preventive actions before irreparable vascular damage occurs.
This study has a number of issues. First, the results may not be as broadly applicable to the general population due to the small sample size of serum samples taken from atherosclerosis patients. Second, because the trial only lasted four months, it may not have captured long-term changes in biomarker levels. Third, the study's cross-sectional design makes it impossible to determine a direct link between blood indicators and the advancement of the illness. Additionally, the biochemical results might have been impacted by possible pre-analytical differences in sample handling and storage.
This study emphasizes how important lipid metabolism and inflammation are in atherosclerosis. Vascular inflammation is indicated by elevated levels of CD40 and Lp-PLA₂, which go beyond conventional lipid indicators. Triglycerides, cholesterol, and VLDL are still significant, but inflammatory markers offer a more comprehensive understanding of disease activity. Systemic inflammation can also be seen in hematological indices, including WBC, Hb, and lymphocytes. A multi-marker approach for more precise diagnosis and monitoring is supported by these findings. Risk stratification is improved by using lipid and inflammatory indicators. Early detection and more individualized treatment regimens could result from this approach.
7. Ethical Considerations
The Institutional Review Board (IRB) at the Najaf Health Directorate, Training and Human Development Center granted ethical approval for the study. According to the formal facilitation letter issued on December 24, 2023, approval was given under document number 7676 on December 17, 2023.
8. Acknowledgments
The authors would like to express their sincere gratitude to the staff of the Open Heart Center for their valuable support and cooperation. We also thank all the patients who participated in this study for their willingness and commitment.
9. Funding
No specific grant from a public, private, or nonprofit organization was obtained for this study.
10. Conflict of Interest
No conflicts of interest have been declared by the author.
11. Author's contribution
ZA: Concept, data collection, manuscript preparation.
Ha: Data analysis, manuscript editing, literature search, conduct of the study, manuscript preparation, and editing.
Author affiliations:
- Zahraa Ismail Abbas, Biology Department, Faculty of Science, University of Kufa, Al Najaf, Iraq; Email: Zah9898hra@gmail.com
- Haider Salih Jaffat, Biology Department, Faculty of Science, University of Kufa, Al Najaf, Iraq; Email: alshafie@uokufa.edu.iq
ABSTRACT
Background & objective: Atherosclerosis affects the large and medium arteries and is a chronic inflammatory condition. It is intimately linked to dyslipidemia and entails the accumulation of lipid-rich plaques.
Its progression is impacted by lipid abnormalities and immune-inflammatory responses. This study focuses on significant lipid indicators, including triglycerides, cholesterol, VLDL, HDL, and Lp-PLA₂. It also looks at different hematological parameters and inflammatory markers like CD40. This study aims to investigate the biochemical relationships between these markers in patients with atherosclerosis and find viable multi-marker panels for better risk prediction.
Methodology: In a case-control study, 90 people between the ages of 45 and 65 were split into three groups: 30 atherosclerosis patients with diabetes and hypertension, 30 pathological controls who had both conditions but no atherosclerosis, and 30 healthy controls. Hematological characteristics, inflammatory markers (Lp-PLA₂, CD40), and lipid profiles were examined in fasting blood samples. Spectrophotometric and ELISA methods were used. Statistical analysis was carried out with SPSS v26.
Results: Lp-PLA₂ and CD40 levels were significantly greater in atherosclerosis patients, suggesting increased vascular inflammation and immunological activation. The patient group had considerably reduced HDL and significantly greater triglycerides, cholesterol, and VLDL. According to hematological data, patients had higher WBC and Hb, while pathological controls had higher lymphocyte counts. Correlation analysis revealed a strong positive association between triglycerides (TG) and total cholesterol (R = 0.722, P < 0.001). In contrast, Lp-PLA₂ showed no significant correlation with lipid parameters, suggesting that it may play an independent role in vascular inflammation. A weak correlation was observed between CD40 and lymphocyte percentage.
Conclusions: The results highlight how crucial it is to combine inflammatory and lipid markers, such as CD40 and Lp-PLA₂, to comprehend the pathophysiology of atherosclerosis. These biomarkers could be helpful in risk assessment and early diagnosis. Lp-PLA₂'s function as a unique inflammatory marker in atherosclerosis is highlighted by the lack of connection it exhibits with conventional lipid markers.
Abbreviations: Lp-PLA₂: Lipoprotein-associated phospholipase A2, HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very-low-density lipoprotein, TG: Triglycerides, CD40: Tumor Necrosis Factor Receptor Superfamily Member 5 (TNFRSF5), Hb: Hemoglobin, WBC: White blood cell, PLT: Platelet, LYM: Lymphocytes
Keywords: Atherosclerosis; Lp-PLA₂; CD40; Lipid profile; Inflammatory biomarkers; Hematological indices
Citation: Abbas ZI, Jaffat HS. Interplay of inflammatory and lipid biomarkers in atherosclerosis: role of Lp-PLA₂, CD40, and hematological indices; a case control study. Anaesth. pain intensive care 2025;29(6):770-778. DOI: 10.35975/apic.v29i7.2960
Received: June 25, 2025; Revised: July 10, 2025; Accepted: July 20, 2025
1. INTRODUCTION
Atherosclerosis is a chronic inflammatory disease of large and medium-sized arteries that is distinguished by the accumulation of plaques that contain lipids inside the artery walls. Peripheral arterial disease, ischemic stroke, and coronary artery disease are some of its manifestations. Atherosclerosis risk is causally linked to dyslipidemia, which is characterized by decreases in high-density lipoprotein (HDL) and increases in plasma levels of low-density lipoprotein (LDL) and triglycerides.1,2
Recent developments highlight the role that lipid-related and inflammatory indicators play in the development and progression of atherosclerosis. Several lipid types, including small dense LDL (sdLDL), oxidized LDL (oxLDL), and low-density lipoprotein (LDL) cholesterol, have been studied in relation to the development and course of atherosclerosis. The formation and fragility of plaques are influenced by the malfunction and inflammatory processes that these lipoproteins support. Furthermore, atherosclerosis has been connected to specific lipid-related proteins and enzymes, underscoring the intricate relationship between inflammation and lipid metabolism in this condition. The functions of lipids, enzymes, and regulatory proteins in the mechanisms producing atherosclerosis are examined in this article. Additionally, it will discuss new and existing treatments that target these molecular pathways in an attempt to understand atherosclerosis and guide future treatment strategies. 3,4
The enzyme Lp-PLA2, which is primarily produced by leukocytes, plays a crucial role in vascular inflammation. Its participation in atherosclerosis is highlighted by the fact that it is present in the necrotic core of atherosclerotic plaques. Lp-PLA2 levels are elevated in patients with intracranial atherosclerotic disease (ICAD) and are linked to more complex and irregular plaques. According to certain research, Lp-PLA2 activity (Lp-PLA2-A) can be a more accurate indicator of vascular events than its mass. However, due to the lack of pathology data from ICAD cases, there is currently insufficient evidence to establish the role of inflammation in ICAD-related stroke 5,6
CD40 and CD40 ligand (CD40L, CD154) are important co-stimulatory and immunological checkpoints that are essential to the adaptive immune response. Members of the tumor necrosis factor receptor and its ligand superfamily, CD40 and CD40L, can interact to trigger an immunological response. Inflammatory or autoimmune disorders, particularly atherosclerosis, are significantly influenced by the CD40-CD40L system, according to research conducted over the past 30 years. The interaction between CD40 and CD40L, which are present on the surface of immune cells, is essential for immunological signaling. Many immunological activities are compromised in the absence of this interaction, even though T and B cell responses can still occur. For instance, it is necessary for the formation of follicular helper T cells (TFH) in germinal centers, B cell differentiation, proliferation, and antibody class switching. The CD40-CD40L pathway affects hematopoietic and non-hematopoietic stem cells in addition to B cells. 7,8
Hematological indicators, including hemoglobin levels, platelet counts, lymphocyte counts, and white blood cell (WBC) counts, also provide information on the inflammatory state of the vascular system. These metrics are readily available and reasonably priced indicators that might represent long-term, low-grade inflammation linked to atherogenesis.
Hemoglobin (Hb), WBC, PLT, and lymphocytes (LYM) are hematological indicators that have been linked to cardiovascular and metabolic disorders. WBC and PLT levels are frequently high in people with metabolic syndrome (MetS), which exacerbates vascular inflammation and atherosclerosis. Atherogenic processes are further promoted by increased platelet-leukocyte contacts. Furthermore, anomalies in lymphocyte profiles and hemoglobin levels could be signs of increased cardiovascular risk. 9, 10
In this study, we will investigate how lipid indicators (Lp-PLA₂, VLDL, HDL, cholesterol, and TG) and inflammatory markers (CD40, hematological indices) interact in individuals with atherosclerosis. The goal of the study is to understand the biochemical interactions that underlie the disease and to find viable multi-marker panels for risk assessment by looking at their correlations and relevance.
2. METHODOLOGY
This case-control study included ninety participants, divided into three groups:
- Group 1 (n = 30): Patients diagnosed with atherosclerosis in addition to diabetes mellitus and hypertension.
- Group 2 (n = 30): Patients diagnosed with diabetes mellitus and hypertension only, without atherosclerosis.
- Group 3 (n = 30): Healthy individuals who served as the control group, with no history of atherosclerosis, diabetes, or hypertension.
Participants ranged in age from 45 to 65. The diagnosis of vascular disease and atherosclerosis was confirmed by diagnostic catheterization and ultrasound imaging. All participants had their fasting blood samples taken in the morning at the Open-Heart Center of Al-Sadr Medical City, situated in Al-Najaf Al-Ashraf, Iraq. All participants underwent a comprehensive medical evaluation to screen for additional underlying diseases, including kidney illness, chronic inflammation, or thyroid issues that could affect the study's findings.
2.1. Blood sample collection
Sample collection was conducted over the course of four months. After a 10-hour fast, five milliliters
of venous blood were extracted in the morning from both patients and control subjects (without a tourniquet) using disposable needles and plastic syringes. After that, the materials were put into gel tubes and centrifuged for 15 minutes at 3000 rpm to separate their constituent parts.
2.2. Serum level of cytokine
Lipoprotein-associated Phospholipase A2 (Lp-PLA₂) and CD40 blood levels were assessed using the Enzyme-Linked Immunosorbent Assay (ELISA) technique. Both assays were carried out using ELISA kits provided by BT LAB (China) in compliance with the manufacturer's instructions.
2.3. Serum level of lipid profile and glycemic markers
The spectrophotometric method was used to evaluate the amount of cholesterol, triglycerides (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) in the serum. Spinreact (Spain) provided specific test kits for each parameter. Glycated hemoglobin (HbA1c) and fasting blood glucose (FBG) levels were also measured. Using Spinreact kits (Spain), the manufacturer's protocol was followed to detect FBG using the glucose oxidase-peroxidase technique and quantify HbA1c using a turbidimetric inhibition immunoassay.
2.4. Hematological Parameters
Total white blood cells (WBC), lymphocytes (LYM), hemoglobin (Hb), and platelet count (PLT) were measured using an automated hematology analyzer (such as the Sysmex XN-Series) for the complete blood count (CBC). These metrics were used to evaluate the research groups' overall hematological health and any alterations linked to inflammation.
2.5. Statistical Analysis
Statistical software (SPSS 26) was used to do statistical calculations on the data gathered from the study of biochemical data. The F-distribution analysis's mean, standard deviation, and findings were acquired.
3. RESULTS
3.1. Demographic Characteristics
Table 1 shows the study population's demographic details. The mean age of patients with atherosclerosis was (55.83 ± 9.23), (55.03 ± 10.89) for pathological controls, and (55.76 ± 10.07) for healthy controls, with no significant difference. But there was a significant difference in weight between the groups (P = 0.001). The mean weight was highest among patients (85.48 ± 7.51 kg), lowest among pathological controls (66.77 ± 8.62 kg), and highest among healthy controls (76.00 ± 12.80 kg).
| Table 1: Comparative demographic data of the study population | ||||
| Parameters | Patients
(n = 30) |
Pathological Control
(n = 30) |
Control
(n = 30) |
P Value |
| Age (years) | 55.83 ± 9.23 | 55.03 ± 10.89 | 55.76 ± 10.07 | 0.948 |
| Weight (kg) | 85.48 ± 7.51 | 66.77 ± 8.62 | 76.00 ± 12.80 | 0.001 |
| Data presented as Mean ± SD; P < 0.05 considered as significant
Statistical analysis was performed using SPSS v26 and Microsoft Excel 2019. |
||||
3.2. Inflammatory biomarkers: Lp-PLA₂ and CD40
Table 2 presents the serum levels of Lipoprotein-associated Phospholipase A2 (Lp-PLA₂) and CD40 in atherosclerosis patients in contrast to both healthy and pathological control groups. The findings show that the patient group's levels of CD40 and Lp-PLA₂ have significantly increased. Patients had significantly higher amounts of Lp-PLA₂ than both diseased and healthy controls, which may indicate increased vascular inflammation. Similarly, the patient group's CD40 levels were noticeably higher, indicating immunological activation linked to the advancement of atherosclerosis.
| Table 2: Enzymatic biomarker profile in atherosclerosis patients and controls | ||||
| Parameters | Patients
(n = 30) |
Pathological Control
(n = 30) |
Control
(n = 30) |
P Value |
| LPPLA2 | 46.71 ± 10.50 | 27.76 ± 10.87 | 18.52 ± 12.97 | 0.001 |
| CD40 | 25.71 ± 10.68 | 11.62 ± 9.42 | 7.86 ± 7.32 | 0.001 |
| Data presented as Mean ± SD; P < 0.05 considered as significant | ||||
3.3. Lipid profile and arterial stiffness index
Table 3 showed that triglyceride, total cholesterol, and VLDL levels were considerably greater in atherosclerosis patients than in both pathological and healthy controls (P < 0.01), even if the patients' HDL was lower and their LDL was higher.
| Table 3: Comparative lipid profile in the groups | |||||
| Parameters | Patients
(n = 30) |
Pathological Control
(n = 30) |
Control
(n = 30) |
Total
(n = 90) |
P Value |
| HDL | 36.60 ± 12.99 | 58.37 ± 73.23 | 56.15 ± 7.42 | 51.69 ± 44.49 | 0.161 |
| LDL | 111.01 ± 40.94 | 92.30 ± 102.50 | 70.48 ± 36.58 | 88.93 ± 69.21 | 0.092 |
| VLDL | 41.76 ± 24.52 | 41.80 ± 15.07 | 24.70 ± 8.82 | 35.23 ± 18.22 | 0.000 |
| Cholesterol | 183.26 ± 57.70 | 192.47 ± 64.78 | 151.33 ± 36.04 | 174.22 ± 55.90 | 0.008 |
| T.G | 189.98 ± 97.94 | 209.00 ± 75.33 | 123.52 ± 44.10 | 171.11 ± 81.45 | 0.001 |
3.4. Hematological Parameters
Table 4 showed significant differences between the groups in hemoglobin, platelets, WBC, and lymphocyte percentage (P = 0.001). Compared to healthy controls, atherosclerosis patients had greater WBC and Hb levels, pathological controls had the highest lymphocytes, and both patient and pathological groups had more platelets.
| Table 4: Hematological Parameters in patients, Pathological controls, and Controls | ||||
| Parameters | Patients
(n = 30) |
Pathological Control
(n = 30) |
Control
(n = 30) |
P Value |
| WBC | 8.03 ± 1.54 | 5598.16 ± 3975.22 | 7.35± 2.31 | 0.001 |
| PLT | 230.96 ± 54.22 | 267.73 ± 108.21 | 159.12 ± 43.43 | 0.001 |
| HB | 14.14 ± 2.26 | 12.10 ± 1.51 | 13.65 ±2.08 | 0.001 |
| LYM. | 28.92 ± 10.89 | 37.20± 12.34 | 16.60 ± 18.56 | 0.001 |
3.5. Correlation between all variables in atherosclerosis patients
All parameters in patients and controls were examined for potential associations using the Spearman correlation test. The results of this study showed a substantial and significant positive connection between triglycerides (TG) and total cholesterol (CHO) (R = 0.722, P < 0.001), suggesting that these two lipid components are closely related in patients.
On the other hand, despite weak positive and negative tendencies, Lp-PLA₂ did not exhibit any statistically significant association with HDL, LDL, VLDL, TG, or total cholesterol. The lack of a significant association raises the possibility that Lp-PLA₂ functions independently of conventional lipid indicators and represents vascular inflammation as opposed to dyslipidemia. While CD40 did not exhibit significant associations with either lipid parameters or Lp-PLA₂, it did show a somewhat favorable correlation with lymphocyte percentage (LYM), suggesting that it may be linked to immunological activation in individuals with atherosclerosis. Additionally, LYM's involvement in lipid-associated immune responses was demonstrated by its negative correlation with LDL and positive correlation with HDL. Hemoglobin (Hb) and WBC had a negative correlation, which could be an indication of oxidative stress or systemic inflammation. VLDL and platelet count (PLT) had a significant negative correlation, which may indicate that thrombocyte activity and VLDL are inversely related.
3.6. Diagnostic value of Lp-PLA₂ and CD40
The receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of Lp-PLA₂ and CD40 in discriminating patients with atherosclerosis from pathological controls and healthy individuals.
With a 95% CI of 0.886–0.985 and P = 0.0001, the area under the curve (AUC) for Lp-PLA₂ was 0.936. The test's sensitivity was 91.3% and its specificity was 84.4% at a cut-off value of 33.63.
An AUC of 0.880, 95% CI = 0.808–0.953, and P = 0.0001 was found for CD40. As indicated in Table 5, Figure 1, the test obtained a sensitivity of 87.0% and a specificity of 80.0% at the cut-off value of 17.95.
| Table 5: Spearman’s correlation of variables in atherosclerosis patients | ||||||||||||
| Varables | HDL | LDL | VLDL | Cholesterol | TG | LPPLA2 | CD40 | WBC | LYM | PLT | HB | |
| HDL | R | 1 | -0.375 | 0.254 | -0.027 | -0.099 | 0.188 | 0.188 | -0.017 | .466* | -0.017 | 0.109 |
| P | 0.078 | 0.242 | 0.904 | 0.654 | 0.391 | 0.391 | 0.938 | 0.025 | 0.938 | 0.621 | ||
| LDL | R | -0.375 | 1 | -0.107 | 0.12 | 0.171 | 0.181 | 0.181 | 0.041 | -.441* | 0.041 | -0.174 |
| P | 0.078 | 0.627 | 0.587 | 0.435 | 0.408 | 0.408 | 0.851 | 0.035 | 0.851 | 0.427 | ||
| VLDL | R | 0.254 | -0.107 | 1 | 0.047 | 0.116 | 0.118 | 0.118 | 0.136 | 0.072 | 0.136 | 0.332 |
| P | 0.242 | 0.627 | 0.831 | 0.597 | 0.592 | 0.592 | 0.535 | 0.742 | 0.535 | 0.121 | ||
| CHO | R | -0.027 | 0.12 | 0.047 | 1 | .722** | -0.34 | -0.34 | -0.144 | 0.086 | -0.144 | 0.025 |
| P | 0.904 | 0.587 | 0.831 | 0 | 0.113 | 0.113 | 0.513 | 0.695 | 0.513 | 0.91 | ||
| TG | R | -0.099 | 0.171 | 0.116 | .722** | 1 | -0.177 | -0.177 | -0.166 | 0.007 | -0.166 | -0.072 |
| P | 0.654 | 0.435 | 0.597 | 0 | 0.419 | 0.419 | 0.448 | 0.976 | 0.448 | 0.744 | ||
| LPPLA2 | R | 0.188 | 0.181 | 0.118 | -0.34 | -0.177 | 1 | 0.202 | 0.092 | -0.012 | -0.074 | -0.227 |
| P | 0.391 | 0.408 | 0.592 | 0.113 | 0.419 | 0.356 | 0.675 | 0.957 | 0.739 | 0.297 | ||
| CD40 | R | 0.18 | -0.108 | -0.107 | 0.033 | -0.04 | 0.202 | 1 | -0.152 | .421* | -0.074 | -0.051 |
| P | 0.49 | 0.046 | 0.739 | 0.816 | ||||||||
| WBC | R | -0.017 | 0.041 | 0.136 | -0.144 | -0.166 | 0.092 | -0.152 | 1 | -0.072 | 0.191 | -.439* |
| P | 0.938 | 0.851 | 0.535 | 0.513 | 0.448 | 0.675 | 0.49 | 0.745 | 0.382 | 0.036 | ||
| LYM | R | .466* | -.441* | 0.072 | 0.086 | 0.007 | -0.012 | .421* | -0.138 | 1 | -0.138 | 0.001 |
| P | 0.025 | 0.035 | 0.742 | 0.695 | 0.976 | 0.957 | 0.046 | 0.531 | 0.531 | 0.995 | ||
| PLT | R | -0.069 | 0.037 | -.483* | 0.07 | 0.09 | -0.074 | -0.074 | 0.191 | -0.138 | 1 | -0.356 |
| P | 0.755 | 0.866 | 0.02 | 0.75 | 0.682 | 0.739 | 0.739 | 0.382 | 0.531 | 0.095 | ||
| HB | R | 0.109 | -0.174 | 0.332 | 0.025 | -0.072 | -0.227 | -0.051 | -0.356 | 0.001 | -0.356 | 1 |
| P | 0.621 | 0.427 | 0.121 | 0.91 | 0.744 | 0.297 | 0.816 | 0.095 | 0.995 | 0.095 | ||
| * Correlation is significant at the 0.05 level’ ** Correlation is significant at the 0.01 level | ||||||||||||
Figure 1: ROC curve demonstrating the diagnostic performance of CD40 and Lp-PLA2 in patients with atherosclerosis
4. DISCUSSION
Table 3 presents data demonstrating a statistically significant increase (P < 0.01). In atherosclerosis patients, serum levels of triglycerides (TG), total cholesterol (CHO), and very-low-density lipoprotein (VLDL) were higher than in both diseased and healthy controls. This increase reflects the well-known function of dyslipidemia in the development of atherosclerosis. The results of this study are consistent with those of Zachariah, who reported that high TG and LDL levels, along with low HDL, contribute to the development of atherosclerosis. Elevated TG affects HDL function via lipid exchange processes, resulting in a detrimental lipid profile with increased VLDL and LDL and decreased HDL, as found in high-risk individuals.11
The observed lipid changes are most likely due to increased insulin resistance and metabolic imbalance, which are typically seen in people with diabetes and vascular dysfunction. This imbalance increases hepatic synthesis of triglycerides and cholesterol, which are then released into the bloodstream, causing endothelial damage and plaque development. Furthermore, atherosclerosis is regarded as a chronic inflammatory disorder, and inflammation has been shown to promote lipid oxidation, resulting in hazardous chemicals such as oxidized LDL (ox-LDL), which exacerbate arterial wall damage and plaque instability. These pathways contribute to the typical profile of high LDL and low HDL levels found in such patients. 12, 13
Although the patient group had higher LDL levels and lower HDL levels, the differences were not statistically significant (P = 0.092 and P = 0.161, respectively). Nonetheless, the observed tendency matches the recognized pathophysiological concept in which oxidized LDL infiltrates arterial walls and triggers immunological responses, whereas low HDL inhibits reverse cholesterol transport. Together, these factors contribute to plaque progression and instability.14
This runs counter to the findings of Higashi (2023), who contends that triglycerides, VLDL, and LDL do not always cause atherosclerosis since their effects differ based on genetics, oxidative stress, and vascular resistance. The fact that some people with severe dyslipidemia yet have good endothelial function suggests that atherogenesis is not always caused by lipid abnormalities alone. The study suggests that dyslipidemia may occasionally function more as a modulator than as the main cause of the complicated illness known as atherosclerosis. 15
Table 4 reveals a significant alteration in hematological parameters in patients with atherosclerosis compared to both pathological and healthy control groups.
The white blood cell (WBC) count was observed to be considerably higher (P = 0.001) in atherosclerosis patients. This increase reflects an active systemic inflammatory response, which is a known feature of atherosclerotic disease. Elevated leukocyte counts are frequently associated with immune cell migration to vascular locations, which contributes to endothelial activation and damage. WBC, PLT, and lymphocyte counts were found to be highly predictive of acute coronary events and had prognostic significance.16, 17
latelet (PLT) count was also significantly higher (P = 0.001), indicating increased platelet activation and aggregation. This hyperactivity is frequent in atherothrombosis and plays an important role in plaque rupture and thrombus development. The increased platelet response exacerbates the pro-thrombotic condition seen in many cardiovascular diseases. It has been demonstrated that the PLT/WBC ratio and lymphocyte count can be used as early predictors of cardiovascular disease development and inflammation. 18,19
Hemoglobin (HB) levels in the atherosclerotic group were substantially higher than in the pathological controls. This could indicate a compensatory erythropoietic mechanism or a change in oxygen demand in tissues affected by vascular injury. It could also indicate a reaction to prolonged low-grade hypoxia in the inflamed vasculature. It has been reported that complete blood count measures such as WBC, lymphocytes, hemoglobin, and platelet indices are independently related to cardiovascular outcomes.2 Lymphocyte (LYM) percentages varied significantly among groups, indicating underlying immunological dysregulation. Lymphocytes are implicated in both innate and adaptive immunity pathways; therefore, their imbalance contributes to the inflammatory and immunological-mediated character of atherosclerosis. It has been demonstrated that the PLT/WBC ratio and lymphocyte count can be used as early predictors of cardiovascular disease development and inflammation. 21
hese hematological alterations provide credence to the notion that atherosclerosis is a long-term, immuno-inflammatory disease. Circulating blood components, particularly leukocytes and platelets, play essential roles in endothelial dysfunction, vascular inflammation, and plaque instability, resulting in disease development and consequences.
In contrast, research by Abate et al. (2023) found no significant differences in hemoglobin (Hb), platelet (PLT), or white blood cell (WBC) levels between individuals with atherosclerotic cardiovascular disease and those who were only at risk. Although a slight increase was observed in their comparison study, these changes were not statistically significant and did not consistently correlate with the severity of atherosclerosis. The study discovered that common ratios like platelet-to-lymphocyte (PLR) and neutrophil-to-lymphocyte (NLR) had limited predictive value, casting doubt on the validity of complete blood count (CBC) parameters as stand-alone indicators of vascular damage or systemic inflammation in atherosclerosis. These findings imply that hematologic indicators' specificity and diagnostic value in cardiovascular pathology may be limited by non-atherosclerotic variables, including infection, stress, or metabolic problems.22
Table 5 presents several important correlations among lipid parameters, inflammatory markers, and hematological indicators in atherosclerosis patients. Total cholesterol and triglycerides (TG) showed a substantial positive connection (R = 0.722, P < 0.01), confirming the metabolic relationship between hepatic lipogenesis and circulating lipid levels. This association implies that an increase in endogenous triglyceride synthesis is frequently associated with higher cholesterol, both of which lead to atherogenic dyslipidemia. 23
While Lp-PLA₂ did not exhibit significant relationships with specific lipid markers, its slight negative correlation with cholesterol and TG may indicate its involvement as an inflammatory mediator rather than a direct lipid transporter. Lp-PLA₂ releases pro-inflammatory chemicals when it hydrolyzes the oxidized phospholipids in LDL particles. Its higher presence in atherosclerotic plaques suggests a relationship to oxidative stress, rather than classical lipid storage.24
Interestingly, CD40 revealed a strong positive connection with lymphocyte percentage (LYM) (R = 0.421, P = 0.046), indicating a function in immune cell activation. CD40 is a co-stimulatory protein that regulates T-cell and B-cell interactions. It has been shown to aggravate inflammation within the vascular wall by activating cytokine cascades and encouraging foam cell production. The link between CD40 and lymphocytes supports its immunomodulatory involvement in atherosclerotic pathogenesis. 25
In addition, LYM had a significant positive association with HDL (R = 0.466, P = 0.025) and a negative correlation with LDL (R = -0.441, P = 0.035), indicating that lymphocytes may have a protective function in lipid control. The inverse association between platelets (PLT) and VLDL (R = -0.483, P = 0.02) may reflect a thrombo-inflammatory interaction in which lipid-rich particles regulate platelet activity and contribute to vascular remodeling.25
A significant link was also found between WBC and hemoglobin (Hb), with a significant negative relationship (R = -0.439, P = 0.036), suggesting that systemic inflammation affects erythropoiesis or red blood cell turnover. Inflammatory conditions, such as atherosclerosis, are frequently accompanied by chronic illness, anemia, or stress erythropoiesis, which may explain this link. 26, 27
The relationships above demonstrate how intricately lipid metabolism, inflammation, and the immune system interact to cause atherosclerosis. Markers like Lp-PLA₂ and CD40, along with hematological data, offer insight into the disease's complex character and can be used for risk classification and monitoring disease activity.
Table 6 presents the receiver operating characteristic (ROC) analysis of CD40 and Lp-PLA₂, highlighting their potential as diagnostic biomarkers for atherosclerosis. The results show that both markers had a good discriminatory capacity between atherosclerosis patients and controls, with high sensitivity, specificity, and area under the curve (AUC).
Lp-PLA₂ achieved an AUC of 0.936 (95% CI: 0.886-0.985; P = 0.0001), showing high diagnostic accuracy. Lp-PLA₂ demonstrated 91.3% sensitivity and 84.4% specificity at a cut-off value of 33.63, suggesting that it may reliably distinguish between individuals with vascular inflammation and atherogenic risk and those who are not afflicted. This enzyme, produced by activated macrophages within plaques, reflects active oxidative stress and inflammation, making it a therapeutically useful diagnostic for vascular injury and development.28
Similarly, CD40 had an AUC of 0.880 (95% CI: 0.808-0.953; P = 0.0001), demonstrating superior diagnostic ability. At a threshold of 17.95, CD40 had 87% sensitivity and 80% specificity. CD40's increase is consistent with its role in increasing cytokine release, endothelial activation, and immune cell recruitment—all hallmarks of atherosclerosis progression.29
Several investigations have questioned the diagnostic reliability of Lp-PLA₂ and CD40 in the setting of atherosclerosis, which runs counter to the current findings. According to Adam et al. (2022), Lp-PLA₂'s utility as an early biomarker for vascular inflammation is limited because it is absent from early atherosclerotic lesions. Similarly, Abera et al. (2024) discovered that in patients with stable coronary artery disease, darapladib-induced Lp-PLA₂ inhibition did not significantly alter inflammatory or platelet indicators like CD40 ligand, indicating limited prognostic usefulness.30,31
The strong AUC values for both markers not only validate their individual diagnostic power but also highlight their combined efficacy in detecting the inflammatory and immune-mediated aspects of atherosclerosis, which standard lipid assays may not fully capture.
Including Lp-PLA₂ and CD40 in routine testing may improve the early detection of subclinical atherosclerosis, particularly in high-risk populations such as those with diabetes, hypertension, and metabolic syndrome. Their combined measurements may help stratify cardiovascular risk and guide preventive actions before irreparable vascular damage occurs.
5. LIMITATIONS
This study has a number of issues. First, the results may not be as broadly applicable to the general population due to the small sample size of serum samples taken from atherosclerosis patients. Second, because the trial only lasted four months, it may not have captured long-term changes in biomarker levels. Third, the study's cross-sectional design makes it impossible to determine a direct link between blood indicators and the advancement of the illness. Additionally, the biochemical results might have been impacted by possible pre-analytical differences in sample handling and storage.
6. CONCLUSION
This study emphasizes how important lipid metabolism and inflammation are in atherosclerosis. Vascular inflammation is indicated by elevated levels of CD40 and Lp-PLA₂, which go beyond conventional lipid indicators. Triglycerides, cholesterol, and VLDL are still significant, but inflammatory markers offer a more comprehensive understanding of disease activity. Systemic inflammation can also be seen in hematological indices, including WBC, Hb, and lymphocytes. A multi-marker approach for more precise diagnosis and monitoring is supported by these findings. Risk stratification is improved by using lipid and inflammatory indicators. Early detection and more individualized treatment regimens could result from this approach.
7. Ethical Considerations
The Institutional Review Board (IRB) at the Najaf Health Directorate, Training and Human Development Center granted ethical approval for the study. According to the formal facilitation letter issued on December 24, 2023, approval was given under document number 7676 on December 17, 2023.
8. Acknowledgments
The authors would like to express their sincere gratitude to the staff of the Open Heart Center for their valuable support and cooperation. We also thank all the patients who participated in this study for their willingness and commitment.
9. Funding
No specific grant from a public, private, or nonprofit organization was obtained for this study.
10. Conflict of Interest
No conflicts of interest have been declared by the author.
11. Author's contribution
ZA: Concept, data collection, manuscript preparation.
Ha: Data analysis, manuscript editing, literature search, conduct of the study, manuscript preparation, and editing.
12. REFERENCES
- Shi W. (2025). ApoE, Atherosclerosis, and Hypercholesterolemia. In Apolipoprotein E (pp. 1-21). Springer, Cham.
- Mohammed UJ, Ali BM. The association of atherosclerosis with cortisol and alpha-enolase levels and lipid profile. Anaesth. pain intensive care 2024;28(6):1097-1104; DOI: 35975/apic.v28i6.2609
- Akram MA, Khodja A, Dalibalta S, Majdalawieh AF. (2025). The Role of Lipids in Atherosclerosis: Focus on Molecular Biology Mechanisms and Therapeutic Approaches. Current Medicinal Chemistry.
- Ali B M, Alassadi P, Iqbal J, Zearah A P. (2020). Study the effect of antioxidants and oxidative products and their genetic effect on methionine synthase in people with autism spectrum disorder. Proff. Sameerah Ahmed, Study the Effect of Antioxidants and Oxidative Products and Their Genetic Effect on Methionine Synthase in People with Autism Spectrum Disorder (March 23, 2020).
- Mo J, Chen Z, Wang M, Cheng A, Li J, Pan Y, Li Z. (2024). Lipoprotein-associated phospholipase A2 activity levels is associated with artery to artery embolism in symptomatic intracranial atherosclerotic disease. Journal of Stroke and Cerebrovascular Diseases, 33(11), 108012.
- Ali B M, Moein F, Al-Andaleb M, Hussein Z, Abidali M K, Dhyaa S. (2021). Study of some factors affecting in myocardial infarction. Annals of the Romanian Society for Cell Biology, 25(6).
- Tian S, Wang Y, Wan J, Yang M, Fu Z. (2024). Co-stimulators CD40-CD40L, a potential immune-therapy target for atherosclerosis: a review. Medicine, 103(14), e37718.
- Askarizadeh F, Karav S, Jamialahmadi T, Sahebkar A. (2024). Impact of statin therapy on CD40: CD40L signaling: mechanistic insights and therapeutic opportunities. Pharmacological Reports, 1-29.
- Abate E, Degef M, Melkie A, Gnanasekeran N, Mehdi M, Tolcha Y, Chala D. (2023). Haematological Parameters in People with Atherosclerotic Cardiovascular Disease versus Those Who are Only at Risk for Cardiovascular Disease: A Comparative Cross-Sectional Study. Diabetes, Metabolic Syndrome and Obesity, 1869-1883.
- Mohammed UJ, Ali BM. The association of atherosclerosis with cortisol and alpha-enolase levels and lipid profile. Anaesth. pain intensive care 2024;28(6):1097-1104; DOI: 35975/apic.v28i6.2609
- Zachariah G. (2024). Management of triglycerides, non-high density lipoprotein cholesterol and high density lipoprotein cholesterol. Indian Heart Journal, 76, S58-S64.
- Auda F M, Ali B M, Al-Andaleb M, Abidali M K, Dhyaa S. (2021). Estimation of Hepcidin and Sexual Hormones Levels in Patients with Atherosclerosis in Al-Najaf City/Iraq. Indian Journal of Forensic Medicine Toxicology, 15(3), 5235-5239.
- Chandrasekaran P, Weiskirchen R. (2024). Cellular and molecular mechanisms of insulin resistance. Current Tissue Microenvironment Reports, 5(3), 79-90.
- Wang Z, Zhou S, Hao Y, Xu T, An P, Luo Y, Luo J. (2024). Nicotinamide mononucleotide protects against high-fat-diet-induced atherosclerosis in mice and dampens aortic inflammation and oxidative stress. Journal of Functional Foods, 112, 105985.
- Higashi Y. (2023). Endothelial function in dyslipidemia: roles of LDL-cholesterol, HDL-cholesterol and triglycerides. Cells, 12(9), 1293.
- Munno M, Mallia A, Greco A, Modafferi G, Banfi C, Eligini S. (2024). Radical oxygen species oxidized low-density lipoproteins, and lectin-like oxidized low-density lipoprotein receptor 1: a vicious circle in atherosclerotic process. Antioxidants, 13(5), 583.
- Karadeniz F. Ö., Karadeniz Y., Altuntaş E. (2024). Systemic immune–inflammation index, and neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios can predict clinical outcomes in patients with acute coronary syndrome. Cardiovascular journal of Africa, 35(2), 82-88.
- Pruc M, Kubica J, Szarpak L, Swieczkowski D, Niezgoda P. (2025). New platelet-derived ratios in acute coronary syndromes: a retrospective, single-center investigation. Disaster and Emergency Medicine Journal, 10(1), 9-17.
- Honey U, Saleh S A B, Salan M S A, Kabir M A, Ali A. (2024). Exploring the relationship between blood platelet and other components utilizing count regression: A cross‐sectional study in Bangladesh. Health Science Reports, 7(8), e70007.
- Pruc M, Kubica J, Szarpak L, Swieczkowski D, Niezgoda P. (2025). New platelet-derived ratios in acute coronary syndromes: a retrospective, single-center investigation. Disaster and Emergency Medicine Journal, 10(1), 9-17.
- Abate E, Degef M, Melkie A, Gnanasekeran N, Mehdi M, Tolcha Y, Chala D (2023). Haematological Parameters in People with Atherosclerotic Cardiovascular Disease versus Those Who are Only at Risk for Cardiovascular Disease: A Comparative Cross-Sectional Study. Diabetes, Metabolic Syndrome and Obesity, 1869-1883.
- Alcover S, Ramos-Regalado L, Girón G, Muñoz-García N, Vilahur G. (2025). HDL-Cholesterol and Triglycerides Dynamics: Essential Players in Metabolic Syndrome. Antioxidants, 14(4), 434.
- Soumya R S, Ayyappan P. (2023). Phospholipase activities in cardiovascular disease and its role as a potential biomarker in heart failure. In Phospholipases in Physiology and Pathology (pp. 225-236). Academic Press.
- Witkowski S. (2024). The role of co-stimulatory molecules CD40/CD40L during the immune response after acute myocardial infarction (Doctoral dissertation, Dissertation, Düsseldorf, Heinrich-Heine-Universität, 2024).
- Manke M C, Ahrends R, Borst O. (2022). Platelet lipid metabolism in vascular thrombo-inflammation. Pharmacology Therapeutics, 237, 108258.
- Wacka E, Nicikowski J, Jarmuzek P, Zembron-Lacny A (2024). Anemia and its connections to inflammation in older adults: a review. Journal of Clinical Medicine, 13(7), 2049.
- Bargieł W, Cierpiszewska K, Maruszczak K, Pakuła A, Szwankowska D, Wrzesińska A, et al. (2021). Recognized and potentially new biomarkers—their role in diagnosis and prognosis of cardiovascular disease. Medicina, 57(7), 701.
- Almohanna T, Auda F M, Ali B M (2025). Early Detection of Digestive System Cancers: Insights from Enzymatic and Non-Enzymatic Tumor Markers. Journal of Medical Biochemistry, 44(3), 631-636.
- Risan T Z, Ali B M (2024, March). Study the effect of amphetamine on neurotransmitter factors in abusers individuals. In AIP Conference Proceedings (Vol. 3092, No. 1). AIP Publishing
- Lacy M, Bürger C, Shami A, Ahmadsei M, Winkels H, Nitz K, et al. (2021). Cell-specific and divergent roles of the CD40L-CD40 axis in atherosclerotic vascular disease. Nature communications, 12(1), 3754.
- Abera A, Worede A, Hirigo A T, Alemayehu R, Ambachew S. (2024). Dyslipidemia and associated factors among adult cardiac patients: a hospital-based comparative cross-sectional study. European Journal of Medical Research, 29(1), 237