Dhay Ihab AL-jdooa 1 , Ahmed Ghdhban Al-Ziaydi 2*
Authors affiliations:
Background & objective: Breast cancer is one of the leading and most aggressive cancers in women worldwide. Pancreatic dysfunction is common among cancer patients and is associated with chronic inflammation and metastatic breast cancer. The inflammation markers, Metabolic Alkaline Phosphate (ALP), Interleukin-6 (IL-6), and C-reactive Protein (CRP) are often associated with metabolic disruptions. Some genetic polymorphisms, like the SNP of the TCF7L2 gene, have been associated with metabolic disorders and pancreatic insufficiency. We assessed the diagnostic correlates of biomarkers ALP, IL-6, and CRP and pancreatic dysfunction in breast cancer patients and evaluated the relationship of polymorphisms of the TCF7L2 gene with pancreatic dysfunction.
Methods: The biomarkers were detected using ELISA, and the levels of ALP, IL-6, and CRP were compared between breast cancer patients and healthy individuals. The TCF7L2 Gene polymorphism (rs12255372) was performed by T-ARMS PCR and agarose gel electrophoresis. Diagnostic assessment was conducted by ROC curve and chi-square statistical analysis of the polymorphisms TCF7L2 and markers of pancreatic dysfunction.
Results: The results suggest that ALP as a single marker lacks sufficient sensitivity for diagnosing pancreatic dysfunction in breast cancer patients (AUROC=0.55). CRP showed moderate diagnostic potential with an AUC of 0.60, but breast cancer patients paradoxically had lower CRP compared to healthy controls. IL-6 performed poorly as well, since no differences were found between patients and controls. The analysis of the TCF7L2 gene polymorphism showed that there was an increased prevalence of the GG genotype among breast cancer patients, which may indicate pancreatic dysfunction.
Conclusion: ALP, IL-6, and CRP, as individual biomarkers, did not prove useful for the diagnosis of pancreatic dysfunction in breast cancer patients, but an enhancement in diagnostic accuracy may be achievable with the use of other adjunct markers. The particular polymorphism of the TCF7L2 gene, with focus on the GG genotype, may be another factor contributing to pancreatic dysfunction in breast cancer patients. More research is necessary to understand the relations between these markers and other genetic factors to formulate better and targeted interventions for pancreatic dysfunction arising from breast cancer.
Abbreviations: ALP: Metabolic Alkaline Phosphate, IL-6: Interleukin-6, CRP: C-reactive Protein
Keywords: Inflammatory Biomarkers; Metabolic Disorders; Type 2 Diabetes Mellitus; Metabolic Alterations; Cancer
Citation: AL-jdooa DI, Al-Ziaydi AG. The influence of gene polymorphisms and biomarkers (ALP, IL-6 and CRP) on pancreatic dysfunction in breast cancer patients. Anaesth. pain intensive care 2025;29(7):702-711. DOI: 10.35975/apic.v29i7.2954
Received: April 25, 2025; Revised: May 27, 2025; Accepted: June 10, 2025
Breast cancer is one of the most widespread types of cancer among women and is still one of the leading causes of death from cancer. While the prognosis has improved with the advent of new diagnostic and therapeutic techniques, such as treatments targeting HER2 and other molecular pathways, challenges remain due to the multifactorial nature of genetics, inflammation, and metabolic processes involved.1 Trastuzumab-based therapy leads to lower serum levels of HER-2 in breast cancer patients. Additionally, although there has been significant progress in diagnostic and therapeutic modalities, the complex interplay of genetics, inflammation, and metabolic processes underlying breast cancer is still only partially understood.2 The dysfunction of the pancreas commonly encountered among cancer patients is thought to be due to the presence of a systemic inflammatory process with altered metabolism, which complicates the clinical management of breast cancer significantly.3
The quest for accurate biomarkers and genetic polymorphisms indicative of pancreatic insufficiency in breast cancer patients may be critical in elucidating important determinants of disease progression and therapeutic measures. Alkaline phosphatase (ALP), interleukin-6 (IL-6), and C-reactive protein (CRP) are well-established inflammatory and metabolic markers, and are even more distinguished by their use and versatility in medicine. Research has shown that the enzyme ALP, which is present in the liver, bone, and intestines, is connected to several disease processes, including cancer.4 The pro-inflammatory cytokine IL-6 is a key immune responder and is known to play a role in cancer development and metastasis.5 CRP, an acute-phase reactant, is a well-known sensitive marker of systemic inflammation and is linked to several forms of cancer, including breast cancer.6 However, with respect to markers, diagnostics, and prognostics for breast cancer with pancreatic insufficiency, the pediatric population has not been exhaustively explored.
Cancer risk and progression are multifactorial, including genetic polymorphisms that impact metabolic and inflammatory processes. The TCF7L2 gene, associated with diabetes and pancreatic abnormalities, encodes a transcription factor of the Wnt Pathway.7 Certain polymorphisms, like rs12255372 TCF7L2, are known to be associated with increased expression and increased risk for metabolic disorders, which may explain some pancreatic deficiency in cancer patients. Understanding breast cancer-associated pancreatic abnormalities may serve as a new frontier for TCF7L2 polymorphisms and precision medicine. This study deals with the effect of gene polymorphisms and the ALP, IL-6, and CRP biomarkers on pancreatic disorders in women suffering from breast cancer. As reported by Abed et al. (2023), CRP serves as a sensitive inflammatory marker that correlates with disease severity and can reflect systemic complications such as liver or renal failure.9 The aim of this study is to analyze how the combination of the ALP and IL-6 cytokine biomarkers, along with CRP levels, might aid in identifying the pancreatic dysfunction alongside TCF7L2 gene polymorphisms in patients with breast cancer. We aim to illuminate the contested pathways of inflammation and metabolism that underpin both phenomena while exploring how genetic risk factors interact with cancer-systemic processes. Such an approach might enable the creation of more precise diagnostic processes and targeted treatment strategies. This knowledge can add to the current literature on the subject and facilitate, to a great extent, the formulation of effective diagnostic and therapeutic measures for pancreatic lesions linked to breast cancer.
ELISA was used to measure ALP (Catalog Number: E5528Hu), IL-6 (Catalog No.: E0090Hu), and CRP (Catalog No.: BPE193) Biomarkers: As instructed in the manufacturer’s protocols (BT LAB Bioassay Technology Laboratory), all commercially procured kits were used for each relevant assay. Standard procedures included preparing all samples and reagents at room temperature, incubating with biotinylated antibodies and streptavidin-HRP, extensive washing, development with substrate solutions, and reading absorbance at 450 nm on a microplate reader. All measured concentrations were derived from generated standard curves based on four-parameter logistic regression. Each kit’s specific protocol was followed, including incubation times and volumes of reagents added to the reactions. All kits were used per manufacturer protocols and quality control guidelines.
2.1. Statistical Analysis
Standard curve fitting for ELISA data utilizing four-parameter logistic regression and the computation of optical density (OD) values were executed using GraphPad Prism (version 8.0.2). Supplementary statistical analyses, including ROC curve analysis, chi-square testing, and odds ratio calculations, were performed using GraphPad Prism. All tests were bilateral with significance established at P < 0.05.
3.1. Assessment of ALP Levels
The examination of ALP as a potential biomarker did not help differentiate breast cancer patients from healthy individuals. The Receiver Operating Characteristic (ROC) curve is a graphical representation commonly used in diagnostic medicine to evaluate the performance of a diagnostic test or model.10 The analysis of the ROC curve yielded an AUC value of 0.55, suggesting insufficient distinguishing capability, meaning that ALP alone is not adequate for the diagnosis of pancreatic pathology in breast cancer patients. The analysis of the lognormal QQ plot gave insight that Enhanced ALP production could be attributed to the presence of underlying liver disease due to its values falling within the recesses of the lognormal distribution, thus allowing for subsequent logarithmic computation. On the other hand, the deviation from the diagonal line could indicate a possibility of having outliers or having greater variation than expected amongst the subjects, making the findings rather harder to interpret. The bar chart analysis comparing patients and controls showed that there was no significant difference in ALP concentration, and casts further doubts on its relevance as an isolated biomarker for pancreatic disorder. As these results indicate, ALP alone does not appear to be a reliable diagnostic marker; however, its use in combination with other biomarkers shows promise. Further studies are needed to determine which inflammatory, genetic, or metabolic markers could be used alongside ALP to enhance its diagnostic utility. Furthermore, examining the influence of breast cancer on ALP in relation to the stages of the disease, the response to treatment, or other clinical factors can shed some light on its potent role in evaluating pancreatic health among breast cancer patients (Figure 1).
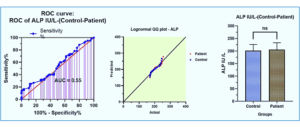
Figure 1: Comparative serum alkaline phosphatase levels in breast cancer patients with healthy controls. Barchart indicates no statistically significant difference in ALP concentration between the patient and control groups. ROC curve analysis (AUC = 0.55) demonstrates limited diagnostic accuracy of ALP for pancreatic dysfunction in breast cancer.
3.2. Assessment of CRP Levels
Evaluating C-Reactive Protein (CRP) concentration with respect to its use as a biomarker differentiating breast cancer patients from healthy subjects shows moderate diagnostic potential. The calculated area under the ROC curve was 0.60, which implies fair accuracy in differentiating between the two groups. This suggests that CRP may have value in detecting inflammatory processes associated with breast cancer; however, this diagnostic implication requires further verification. Examination of the lognormal QQ plot confirms that the average CRP level logarithmically follows a normal distribution; hence, the data is fit for parametric statistical method analysis. In a case-control study assessing the concentration of CRP in breast cancer patients and healthy controls, it was found that the breast cancer patients had significantly lower CRP concentrations than healthy individuals. This finding is unexpected, as most literature reports elevated CRP levels in cancer patients. The unexpected reduction in CRP is likely due to the stage of the disease, treatment effects, or alterations of metabolism that support the energy needs of the breast tumor cells. A better understanding of the mechanisms regulating CRP expression in cancer-associated inflammation will provide insight into some of these enigmatic observations. Even though CRP on its own is not sufficient to be considered a diagnostic marker, it has clinical utility when included in a panel of inflammatory biomarkers that can help monitor disease progression and treatment response. The relationship of CRP to other cytokines or inflammatory mediators is of interest and should be further investigated in the context of its potential role in breast cancer pathology and assessment of inflammatory markers in oncology more generally (Figure 2).
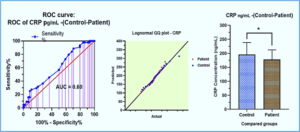
Figure 2: Comparative serum CRP levels in breast cancer patients with healthy controls. Barchart indicates a statistically significant difference in CRP concentration between the patient and control groups. ROC curve analysis (AUC = 0.60) demonstrates the unexpectedly lower diagnostic accuracy of CRP for pancreatic dysfunction in breast cancer.
3.3. Assessment of IL-6 Levels
There appears to be limited utility in using Serum Interleukin-6 (IL-6) results for distinguishing between breast cancer patients and healthy controls, as seen with the ROC curve analysis, which yielded a low AUC. This means that there is not enough sensitivity and specificity for the determination of breast cancer with possible pancreatic impairment. The lognormal QQ plot for the IL-6 concentrations indicated that the values of IL-6 levels reasonably clustered along the diagonal line, supporting the claim of lognormal distribution. This indicates that IL-6 could be subjected to parametric statistical analysis; however, the lack of significant differences in the concentrations of IL-6 between patients and controls makes it less useful in diagnosis. The comparative study of the concentration of IL-6 between the two groups did not show a statistically significant difference, indicating that IL-6 does not have a distinct role in the inflammatory processes associated with breast cancer in the selected population. Given those considerations, these findings suggest that IL-6 used independently has a limited potential as a diagnostic marker for breast cancer or dysfunction of the pancreas. Nonetheless, the involvement of IL-6 in systemic inflammation and regulation of the tumor microenvironment warrants study for some populations or subtypes of patients with breast cancer or with different stages of the disease. It is recommended that future studies investigate the potential of IL-6 as part of a multi-marker panel for comprehensive disease evaluation by exploring its interactions with other inflammatory cytokines and biomarkers. Furthermore, assessing changes in IL-6 levels following treatment or monitoring them in longitudinal studies may provide valuable insight into its prognostic utility, rather than limiting its application to diagnostic purposes alone. (Figure 3).
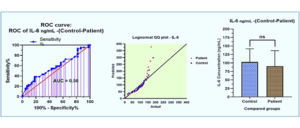
Figure 3: Comparative serum IL-6 levels in breast cancer patients with healthy controls. Barchart indicates no statistically significant difference in IL-6 concentration between the patient and control groups. ROC curve analysis (AUC = 0.58) demonstrates limited diagnostic accuracy of IL-6 for pancreatic dysfunction in breast cancer.
3.4. Analysis of Gene Polymorphism
The objective of the analysis was to examine the polymorphism of the TCF7L2 gene (rs12255372), noting particular variances in genotype distribution of breast cancer patients and healthy controls as presented in Figure 4 and Table 1.
Noteworthy was the increased prevalence of the GG genotype among patients, with 27 cases compared to 13 in the control group. (Tables 2,3,4).
This can mean that breast cancer patients with pancreatic dysfunction may have a higher tendency for the GG genotype. Further statistical analysis, including chi-square tests, found differences across other genotypes, which provided stronger evidence (p-value < 0.05) for the assumption that the TCF7L2 polymorphism had an association with breast cancer-related pancreatic dysfunction. It was noted that G allele frequency was significantly higher in patients as compared to controls, while the G allele was the least common among the patients, suggesting a possible protective role. Also, Odds Ratio values were suggestive of concern about having the GG genotype for developing pancreatic dysfunction in breast cancer. On the other hand, the T allele appeared to be reducing the risk (Table 5, Figures 5, 6). In summary, the data suggest that the role of the TCF7L2 gene in pancreatic dysfunction and breast cancer does not mask the TCF7L2 gene polymorphism.
3.5 Agarose gel electrophoresis Assay
Agarose gel electrophoresis confirmed the amplification of the TCF7L2 (rs12255372) polymorphism by T-ARMS PCR. Gradient PCR optimization showed clear banding at 58 °C, with distinct bands for GG, TT, and GT genotypes along with the 587 bp control band. The assay reliably differentiated patient and control genotypes, as shown in Figures 4–6.
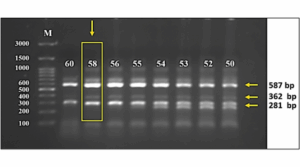
Figure 4: The image obtained from agarose gel electrophoresis (the gel concentration is 1.5 percent) shows how the TCF7L2 gene (rs12255372) was amplified by T-ARMS PCR using a gradient protocol. In this case, the same PCR conditions were used apart from the temperature at which the primers were annealed, which was set at 50 °C to 60 °C. From the results, it was concluded that the most effective temperature for amplification is 58 °C. The gel contains the “M” label, which is a molecular marker (3000-100 bp) from the company GeneDirex Korea, South Korea, which verifies the size of the amplified fragments.
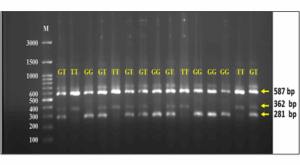
Figure 5: Control: The agarose gel electrophoresis image (1.5% agarose) illustrates the amplification of the TCF7L2 gene (rs12255372) using T-ARMS PCR. This indicates the presence of genotypes (GT, TT, GG) in the control group. The marker M is a molecular weight marker (3000-100 bp) obtained from GeneDirex, South Korea.
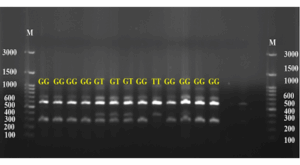
Figure 6: Patients: The image of agarose gel electrophoresis (1.5% agarose) displays the amplification of the TCF7L2 gene (rs12255372) using T-ARMS PCR. This reveals the presence of genotypes (GT, TT, GG) in the patients. The marker M is a molecular weight marker (3000-100 bp) sourced from GeneDirex, South Korea
The results of the study “Inabilities in Using Distinct Biomarkers to Diagnose Pancreatic Dysfunction in Breast Cancer Patients” show how the inflammatory markers and polymorphisms of genes contribute to the growing research of breast cancer and pancreatic dysfunction. The results of this study show some agreement and disagreement with previous works, underlying the nuances in the application of biomarkers and genetic modifications in cancer diagnosis and treatment.
4.1. ALP as a Biomarker
This study shows that ALP by itself is not an adequate biomarker for indicating pancreatic abnormalities in breast cancer patients, owing to its low AUC of 0.55.
This corroborates with other studies that have previously raised concerns regarding the lack of specificity of ALP as a biomarker when used independently. Sharma et al. point out that ALP is raised in liver and bone diseases, which may pose a problem to its diagnostic use in many cancer patients.1 On the contrary, some literature advocates for more attention to be placed towards metabolic disturbances that are state-specific to cancer when using ALP as a complement to other markers. We partake in the view that ALP does not provide much diagnostic information when used alone, but that view will change when ALP is part of a multi-marker panel.
4.2. CRP as a Biomarker
The diagnostic accuracy of CRP corresponds to an AUC of 0.60, which is, to some extent, above average. However, the lower levels of CRP in breast cancer patients in reference to healthy controls are quite surprising and unlike most studies that, in fact, document heightened levels in cancer patients because of inflammation.2 This difference can result from the disease's stage, treatment received, or some particular changes in the metabolism related to the tumor microenvironment. More work is required to clarify and understand the mechanisms and determination of whether limiting factors such as CRP concentrations make specific breast cancer subtype variance or treatment regime change modification acceptable.
Undoubtedly, contrary to expectations, CRP values were notably lower in patients with breast cancer in comparison with their healthy counterparts. This surprising figure may indicate the inflammatory response heterogeneity among patients suffering from cancer, perhaps due to the tumor’s stage, the tumor microenvironment’s immunosuppressive function, or even some treatments like chemotherapy or immunotherapy, which modify the expression of CRP. More recent cancer research indicated some subtypes of breast cancer—primarily those that are hormone receptor positive and HER2-enriched—are less likely to induce significant systemic elevations of CRP, particularly in immune checkpoint blockade or anti-inflammatory treatment responsive situations. A different plausible rationale is cancer-induced cachexia, or altered metabolism, which may blunt usual acute phase reactant responses. More longitudinal and mechanistic research is needed to clarify the influence of CRP changes over time in relation to the advancement of breast cancer and its treatment.
4.3. IL-6 as a Biomarker
The diagnostic limitations of IL-6 are unexpected, especially considering its significance in inflammation and tumor progression. Undoubtedly, IL-6 did not show any notable difference among breast cancer patients in comparison to healthy counterparts.3 Previous literature has suggested that IL-6 is involved in the microenvironment of a tumor and serves as a prognostic marker for specific cancers. Nonetheless, our data demonstrates that IL-6 is not likely to be a useful pancreatic dysfunction marker in breast cancer patients, at least in the studied cohort. This change may be due to the distinct study populations, differing cancer stages, or even diversity in methods. More research is required to determine the role of IL-6 in a multi-marker panel as well as the specific subtypes of breast cancer.
4.4. Polymorphism of the TCF7L2 Gene
The examination of the TCF7L2 gene polymorphism suggests a possible link with pancreatic disorder due to the increased frequency of breast cancer patients with the GG genotype. This is in accordance with prior studies that have associated TCF7L2 polymorphisms with metabolic problems such as type 2 diabetes and, within the context, pancreatic disorder.4 This phenomenon may be the result of numerous breast cancer patients who previously had the GG genotype demonstrating a higher rate of pancreatic dysfunction, indicating a greater genetic impact toward metabolic changes in the presence of malignancy. These assertions need to be substantiated with additional research for validation, especially to understand the functional ramifications of TCF7L2 polymorphisms on breast cancer and pancreatic health. The conclusion that ALP, IL-6, and CRP are not useful as single biomarkers is consistent with some studies but contrasts with others that have reported significant correlations between these biomarkers and cancer outcomes. One example regarding this, Mantovani et al., highlighted the significance of CRP in cancer-related inflammation; however, our study reported lower levels of CRP in breast cancer patients, which indicates the association of CRP and cancer may be more complex than what was understood.2 Likewise, Knüpfer and Preiss illustrated the significance of IL-6 in the progression of breast cancer, but we did not find a significant difference in IL-6 levels in the patient and control participants, suggesting that the diagnostic value of IL-6 is population and context-dependent.3
This study underscores, and to an extent contradicts, other work done concerning the use of ALP, IL-6, and CRP as singular diagnostic markers for pancreatic dysfunction in breast cancer patients. The low ALP diagnostic accuracy observed here, AUC = 0.55, resonates with Patel et al.,12 who pointed out that ALP sensitivity for pancreatic complications in colorectal cancer patients is nonspecific due to its elevation in many other pathologies. However, Zhang et al.13 provided evidence to the contrary, suggesting that some ALP isoforms, notably intestinal ALP, are associated with metabolic dysregulation and advanced malignancy. These contrasting claims reveal the need for a multi-marker approach that could potentially provide a solution to the issue outlined. The unexpected finding of lower CRP levels in breast cancer patients, alongside the work of Lee et al.14 highlights the necessity for longitudinal studies that aim to clarify CRP’s role in cancer-associated inflammation. Lee’s study determined that CRP levels decrease in metastatic breast cancer patients treated with immunotherapy, further substantiating the growing need for multidisciplinary studies. Lastly, there is a significant deviation from prior work undertaken by Chen et al. in their analysis of IL-6.16 Raised IL-6 levels serve as a marker of pancreatic metastatic spread in triple-negative breast cancer, which is a clear example of this cytokine’s context-dependent variability.
The correlation of the TCF7L2 GG genotype with pancreatic dysfunction is also consistent with new studies that have proposed the TCF7L2 variants as being associated with Wnt signaling insulin resistance in cancer.16 These results bolster the case for using genetic profiling to identify patients with an increased risk and tailor treatment accordingly. Indeed, the shortcomings of the single biomarkers as pointed out by Torres et al.17 demonstrate the need for new approaches to cancer diagnosis that combine correlational evidence.
4.5. Association Between TCF7L2 Genotype and Biomarker Levels
In order to examine further aspects of genetic susceptibility and systemic inflammation, we analyzed biomarker data concerning the TCF7L2 genotype. TCF7L2 breast cancer patients with the GG genotype appeared to have slightly elevated ALP levels and lower CRP levels compared to those with the TT and GT genotypes; however, these differences were not statistically significant (p > 0.05). IL-6 did not show any consistent pattern in this regard either. In any case, these data are too simplistic, but do imply that some variation at TCF7L2 might modulate the inflammation or the metabolism involving pancreatic cancerous processes in breast cancer patients. Although this much is evident, the present results need to be confirmed in studies involving larger cohorts.
4.6. Integration of Genotype and Biomarker Data
To assess how genetic variation of TCF7L2 may impact inflammation or metabolic activity, we analyzed the ALP, CRP, and IL-6 levels by genotype. It was noted that patients carrying the GG genotype had higher ALP and lower CRP compared to the TT or GT genotypes, but these differences were not significant (P > 0.05, Table 6). No persistent differences were noted regarding IL-6 levels either. While such results are premature, they point towards the possibility of some genetic factors in systemic inflammatory and metabolic changes in women with breast cancer and pancreatic insufficiency.
This case study demonstrates the complexities in using distinct biomarkers to diagnose pancreatic dysfunction in patients suffering from breast cancer. While ALP, IL-6, and CRP did not display much promise as individual results, the output can be improved through the incorporation of other genetic markers. The interplay between the TCF7L2 gene polymorphism and pancreatic dysfunction in breast cancer patients is yet to be fully understood. A new direction to the existing body of literature could provide further understanding of the genetic components of metabolic imbalance associated with cancer. Targeting the interactions between the biomarkers and genetic factors is a promising area in need of research to aid in the diagnosis and treatment of breast cancer and pancreatic malignancies.
6. Data availability
The numerical data generated during this research are available from the authors.
7. Acknowledgments
The University of Al-Qadisiyah College of Medicine deserves recognition for its beneficent assistance. Sincere gratitude is extended to all the female breast cancer patients who participated in this study and greatly contributed to its completion. Special thanks are also due to the staff of the Oncology Department at Al-Diwaniyah Teaching Hospital in Al-Diwaniyah for their proactive support.
8. Financial support and sponsorship
This was a self‑funded study.
9. Ethical considerations
Written informed consent was obtained from all patients and, where applicable, from their parents or guardians for sample collection. The principles of the Declaration of Helsinki (1964) concerning medical research on human subjects were followed. Furthermore, the research was approved by the Research and Ethics Committee of the university.
10. Conflicts of interest
The authors declare that they have no competing interests and no conflicts of interest in the current study.
11. Authors’ contribution
DIJ: Laboratory Work, Data Curation, Resources, Formal Analysis, Writing, and Original Draft Preparation.
AGZ: Conceptualization, Methodology Design, Project Supervision, Statistical Analysis, Interpretation of Results, Review & Editing, and Corresponding Author Responsibilities.
Authors affiliations:
- Dhay Ihab AL-jdooa, Department of Medical Chemistry, College of Medicine, University of Al-Qadisiyah, Al-Qadisiyah, Iraq; Email: med.post24.62@qu.edu.iq
- Ahmed Ghdhban Al-Ziaydi, Department of Medical Chemistry, College of Medicine, University of Al-Qadisiyah, Iraq; Email: ahmed.alziaydi@qu.edu.iq
ABSTRACT
Background & objective: Breast cancer is one of the leading and most aggressive cancers in women worldwide. Pancreatic dysfunction is common among cancer patients and is associated with chronic inflammation and metastatic breast cancer. The inflammation markers, Metabolic Alkaline Phosphate (ALP), Interleukin-6 (IL-6), and C-reactive Protein (CRP) are often associated with metabolic disruptions. Some genetic polymorphisms, like the SNP of the TCF7L2 gene, have been associated with metabolic disorders and pancreatic insufficiency. We assessed the diagnostic correlates of biomarkers ALP, IL-6, and CRP and pancreatic dysfunction in breast cancer patients and evaluated the relationship of polymorphisms of the TCF7L2 gene with pancreatic dysfunction.
Methods: The biomarkers were detected using ELISA, and the levels of ALP, IL-6, and CRP were compared between breast cancer patients and healthy individuals. The TCF7L2 Gene polymorphism (rs12255372) was performed by T-ARMS PCR and agarose gel electrophoresis. Diagnostic assessment was conducted by ROC curve and chi-square statistical analysis of the polymorphisms TCF7L2 and markers of pancreatic dysfunction.
Results: The results suggest that ALP as a single marker lacks sufficient sensitivity for diagnosing pancreatic dysfunction in breast cancer patients (AUROC=0.55). CRP showed moderate diagnostic potential with an AUC of 0.60, but breast cancer patients paradoxically had lower CRP compared to healthy controls. IL-6 performed poorly as well, since no differences were found between patients and controls. The analysis of the TCF7L2 gene polymorphism showed that there was an increased prevalence of the GG genotype among breast cancer patients, which may indicate pancreatic dysfunction.
Conclusion: ALP, IL-6, and CRP, as individual biomarkers, did not prove useful for the diagnosis of pancreatic dysfunction in breast cancer patients, but an enhancement in diagnostic accuracy may be achievable with the use of other adjunct markers. The particular polymorphism of the TCF7L2 gene, with focus on the GG genotype, may be another factor contributing to pancreatic dysfunction in breast cancer patients. More research is necessary to understand the relations between these markers and other genetic factors to formulate better and targeted interventions for pancreatic dysfunction arising from breast cancer.
Abbreviations: ALP: Metabolic Alkaline Phosphate, IL-6: Interleukin-6, CRP: C-reactive Protein
Keywords: Inflammatory Biomarkers; Metabolic Disorders; Type 2 Diabetes Mellitus; Metabolic Alterations; Cancer
Citation: AL-jdooa DI, Al-Ziaydi AG. The influence of gene polymorphisms and biomarkers (ALP, IL-6 and CRP) on pancreatic dysfunction in breast cancer patients. Anaesth. pain intensive care 2025;29(7):702-711. DOI: 10.35975/apic.v29i7.2954
Received: April 25, 2025; Revised: May 27, 2025; Accepted: June 10, 2025
1. INTRODUCTION
Breast cancer is one of the most widespread types of cancer among women and is still one of the leading causes of death from cancer. While the prognosis has improved with the advent of new diagnostic and therapeutic techniques, such as treatments targeting HER2 and other molecular pathways, challenges remain due to the multifactorial nature of genetics, inflammation, and metabolic processes involved.1 Trastuzumab-based therapy leads to lower serum levels of HER-2 in breast cancer patients. Additionally, although there has been significant progress in diagnostic and therapeutic modalities, the complex interplay of genetics, inflammation, and metabolic processes underlying breast cancer is still only partially understood.2 The dysfunction of the pancreas commonly encountered among cancer patients is thought to be due to the presence of a systemic inflammatory process with altered metabolism, which complicates the clinical management of breast cancer significantly.3
The quest for accurate biomarkers and genetic polymorphisms indicative of pancreatic insufficiency in breast cancer patients may be critical in elucidating important determinants of disease progression and therapeutic measures. Alkaline phosphatase (ALP), interleukin-6 (IL-6), and C-reactive protein (CRP) are well-established inflammatory and metabolic markers, and are even more distinguished by their use and versatility in medicine. Research has shown that the enzyme ALP, which is present in the liver, bone, and intestines, is connected to several disease processes, including cancer.4 The pro-inflammatory cytokine IL-6 is a key immune responder and is known to play a role in cancer development and metastasis.5 CRP, an acute-phase reactant, is a well-known sensitive marker of systemic inflammation and is linked to several forms of cancer, including breast cancer.6 However, with respect to markers, diagnostics, and prognostics for breast cancer with pancreatic insufficiency, the pediatric population has not been exhaustively explored.
Cancer risk and progression are multifactorial, including genetic polymorphisms that impact metabolic and inflammatory processes. The TCF7L2 gene, associated with diabetes and pancreatic abnormalities, encodes a transcription factor of the Wnt Pathway.7 Certain polymorphisms, like rs12255372 TCF7L2, are known to be associated with increased expression and increased risk for metabolic disorders, which may explain some pancreatic deficiency in cancer patients. Understanding breast cancer-associated pancreatic abnormalities may serve as a new frontier for TCF7L2 polymorphisms and precision medicine. This study deals with the effect of gene polymorphisms and the ALP, IL-6, and CRP biomarkers on pancreatic disorders in women suffering from breast cancer. As reported by Abed et al. (2023), CRP serves as a sensitive inflammatory marker that correlates with disease severity and can reflect systemic complications such as liver or renal failure.9 The aim of this study is to analyze how the combination of the ALP and IL-6 cytokine biomarkers, along with CRP levels, might aid in identifying the pancreatic dysfunction alongside TCF7L2 gene polymorphisms in patients with breast cancer. We aim to illuminate the contested pathways of inflammation and metabolism that underpin both phenomena while exploring how genetic risk factors interact with cancer-systemic processes. Such an approach might enable the creation of more precise diagnostic processes and targeted treatment strategies. This knowledge can add to the current literature on the subject and facilitate, to a great extent, the formulation of effective diagnostic and therapeutic measures for pancreatic lesions linked to breast cancer.
2. METHODOLOGY
ELISA was used to measure ALP (Catalog Number: E5528Hu), IL-6 (Catalog No.: E0090Hu), and CRP (Catalog No.: BPE193) Biomarkers: As instructed in the manufacturer’s protocols (BT LAB Bioassay Technology Laboratory), all commercially procured kits were used for each relevant assay. Standard procedures included preparing all samples and reagents at room temperature, incubating with biotinylated antibodies and streptavidin-HRP, extensive washing, development with substrate solutions, and reading absorbance at 450 nm on a microplate reader. All measured concentrations were derived from generated standard curves based on four-parameter logistic regression. Each kit’s specific protocol was followed, including incubation times and volumes of reagents added to the reactions. All kits were used per manufacturer protocols and quality control guidelines.
2.1. Statistical Analysis
Standard curve fitting for ELISA data utilizing four-parameter logistic regression and the computation of optical density (OD) values were executed using GraphPad Prism (version 8.0.2). Supplementary statistical analyses, including ROC curve analysis, chi-square testing, and odds ratio calculations, were performed using GraphPad Prism. All tests were bilateral with significance established at P < 0.05.
3. RESULTS
3.1. Assessment of ALP Levels
The examination of ALP as a potential biomarker did not help differentiate breast cancer patients from healthy individuals. The Receiver Operating Characteristic (ROC) curve is a graphical representation commonly used in diagnostic medicine to evaluate the performance of a diagnostic test or model.10 The analysis of the ROC curve yielded an AUC value of 0.55, suggesting insufficient distinguishing capability, meaning that ALP alone is not adequate for the diagnosis of pancreatic pathology in breast cancer patients. The analysis of the lognormal QQ plot gave insight that Enhanced ALP production could be attributed to the presence of underlying liver disease due to its values falling within the recesses of the lognormal distribution, thus allowing for subsequent logarithmic computation. On the other hand, the deviation from the diagonal line could indicate a possibility of having outliers or having greater variation than expected amongst the subjects, making the findings rather harder to interpret. The bar chart analysis comparing patients and controls showed that there was no significant difference in ALP concentration, and casts further doubts on its relevance as an isolated biomarker for pancreatic disorder. As these results indicate, ALP alone does not appear to be a reliable diagnostic marker; however, its use in combination with other biomarkers shows promise. Further studies are needed to determine which inflammatory, genetic, or metabolic markers could be used alongside ALP to enhance its diagnostic utility. Furthermore, examining the influence of breast cancer on ALP in relation to the stages of the disease, the response to treatment, or other clinical factors can shed some light on its potent role in evaluating pancreatic health among breast cancer patients (Figure 1).
Figure 1: Comparative serum alkaline phosphatase levels in breast cancer patients with healthy controls. Barchart indicates no statistically significant difference in ALP concentration between the patient and control groups. ROC curve analysis (AUC = 0.55) demonstrates limited diagnostic accuracy of ALP for pancreatic dysfunction in breast cancer.
3.2. Assessment of CRP Levels
Evaluating C-Reactive Protein (CRP) concentration with respect to its use as a biomarker differentiating breast cancer patients from healthy subjects shows moderate diagnostic potential. The calculated area under the ROC curve was 0.60, which implies fair accuracy in differentiating between the two groups. This suggests that CRP may have value in detecting inflammatory processes associated with breast cancer; however, this diagnostic implication requires further verification. Examination of the lognormal QQ plot confirms that the average CRP level logarithmically follows a normal distribution; hence, the data is fit for parametric statistical method analysis. In a case-control study assessing the concentration of CRP in breast cancer patients and healthy controls, it was found that the breast cancer patients had significantly lower CRP concentrations than healthy individuals. This finding is unexpected, as most literature reports elevated CRP levels in cancer patients. The unexpected reduction in CRP is likely due to the stage of the disease, treatment effects, or alterations of metabolism that support the energy needs of the breast tumor cells. A better understanding of the mechanisms regulating CRP expression in cancer-associated inflammation will provide insight into some of these enigmatic observations. Even though CRP on its own is not sufficient to be considered a diagnostic marker, it has clinical utility when included in a panel of inflammatory biomarkers that can help monitor disease progression and treatment response. The relationship of CRP to other cytokines or inflammatory mediators is of interest and should be further investigated in the context of its potential role in breast cancer pathology and assessment of inflammatory markers in oncology more generally (Figure 2).
Figure 2: Comparative serum CRP levels in breast cancer patients with healthy controls. Barchart indicates a statistically significant difference in CRP concentration between the patient and control groups. ROC curve analysis (AUC = 0.60) demonstrates the unexpectedly lower diagnostic accuracy of CRP for pancreatic dysfunction in breast cancer.
3.3. Assessment of IL-6 Levels
There appears to be limited utility in using Serum Interleukin-6 (IL-6) results for distinguishing between breast cancer patients and healthy controls, as seen with the ROC curve analysis, which yielded a low AUC. This means that there is not enough sensitivity and specificity for the determination of breast cancer with possible pancreatic impairment. The lognormal QQ plot for the IL-6 concentrations indicated that the values of IL-6 levels reasonably clustered along the diagonal line, supporting the claim of lognormal distribution. This indicates that IL-6 could be subjected to parametric statistical analysis; however, the lack of significant differences in the concentrations of IL-6 between patients and controls makes it less useful in diagnosis. The comparative study of the concentration of IL-6 between the two groups did not show a statistically significant difference, indicating that IL-6 does not have a distinct role in the inflammatory processes associated with breast cancer in the selected population. Given those considerations, these findings suggest that IL-6 used independently has a limited potential as a diagnostic marker for breast cancer or dysfunction of the pancreas. Nonetheless, the involvement of IL-6 in systemic inflammation and regulation of the tumor microenvironment warrants study for some populations or subtypes of patients with breast cancer or with different stages of the disease. It is recommended that future studies investigate the potential of IL-6 as part of a multi-marker panel for comprehensive disease evaluation by exploring its interactions with other inflammatory cytokines and biomarkers. Furthermore, assessing changes in IL-6 levels following treatment or monitoring them in longitudinal studies may provide valuable insight into its prognostic utility, rather than limiting its application to diagnostic purposes alone. (Figure 3).
Figure 3: Comparative serum IL-6 levels in breast cancer patients with healthy controls. Barchart indicates no statistically significant difference in IL-6 concentration between the patient and control groups. ROC curve analysis (AUC = 0.58) demonstrates limited diagnostic accuracy of IL-6 for pancreatic dysfunction in breast cancer.
3.4. Analysis of Gene Polymorphism
The objective of the analysis was to examine the polymorphism of the TCF7L2 gene (rs12255372), noting particular variances in genotype distribution of breast cancer patients and healthy controls as presented in Figure 4 and Table 1.
| Table 1: Primers Sequence Association of TCF7L2 Gene Polymorphisms with T2DM in the Population of Juana Koslay, San Luis Province, Argentina. Primer sequences used for TCF7L2 (rs12255372) T-ARMS PCR. | |||
| Primer name | Sequence | Product size | |
| Forward outer | GGCTGTATGAAGTCATTTGATGATTGTTT | 587 bp outer band |
|
| Reverse outer | ACGCTTTGAAGGTAGAGAGGACACACT | ||
| Forward inner | CTGCCCAGGAATATCCAGGCAAGAGTT | 362 bp | T allele |
| Reverse inner | GAGGCCTGAGTAATTATCAGAATATGATC | 281 bp | G allele |
Noteworthy was the increased prevalence of the GG genotype among patients, with 27 cases compared to 13 in the control group. (Tables 2,3,4).
| Table 2: Genotype distribution of TCF7L2 (rs12255372) in breast cancer patients and controls. Shows counts for GG, TT, and TG genotypes in each group. | ||
| Genotype | Control | Patients |
| GG | 13 | 27 |
| TT | 8 | 4 |
| TG | 24 | 14 |
| Table 3: Statistical comparison of TCF7L2 polymorphisms in breast cancer patients vs. controls. Includes allele frequencies, odds ratios, and p-values for genotype group comparisons. | ||||||
| Polymorphisms
TCL (G/T) |
G1
Control N=45(%) |
G2
Patients N=45(%) |
χ2 | P value | OR (95% CI) | P value |
| GG
TT GT |
13(28.9) 8(17.8) 24(53.3) |
27 (60.0) 4(8.9) 14(31.1) |
8.865 | 0.012* | 1.0ref (1.0ref) 0.241(0.061-0.948) 0.281(0.110-0.715) |
0.034* 0.007* |
| G allele
T allele |
50(55.6) 40(44.4) |
68(75.6) 22(24.4) |
7.972 | 0.005* | 1.0ref (1.0ref) 0.404(0.214-0.764) |
|
| GG
TT & GT |
13(28.9) 32(71.1) |
27(60.0) 18(40.0) |
8.820 | 0.003* | 1.0ref (1.0ref) 0.271(0.113-0.652) |
|
| TT
GG & GT |
8(17.8) 37(82.2) |
4(8.9) 41(91.1) |
1.538 | 0.215 | 1.0ref (1.0ref) 2.216(0.616-7.970) |
|
This can mean that breast cancer patients with pancreatic dysfunction may have a higher tendency for the GG genotype. Further statistical analysis, including chi-square tests, found differences across other genotypes, which provided stronger evidence (p-value < 0.05) for the assumption that the TCF7L2 polymorphism had an association with breast cancer-related pancreatic dysfunction. It was noted that G allele frequency was significantly higher in patients as compared to controls, while the G allele was the least common among the patients, suggesting a possible protective role. Also, Odds Ratio values were suggestive of concern about having the GG genotype for developing pancreatic dysfunction in breast cancer. On the other hand, the T allele appeared to be reducing the risk (Table 5, Figures 5, 6). In summary, the data suggest that the role of the TCF7L2 gene in pancreatic dysfunction and breast cancer does not mask the TCF7L2 gene polymorphism.
3.5 Agarose gel electrophoresis Assay
Agarose gel electrophoresis confirmed the amplification of the TCF7L2 (rs12255372) polymorphism by T-ARMS PCR. Gradient PCR optimization showed clear banding at 58 °C, with distinct bands for GG, TT, and GT genotypes along with the 587 bp control band. The assay reliably differentiated patient and control genotypes, as shown in Figures 4–6.
Figure 4: The image obtained from agarose gel electrophoresis (the gel concentration is 1.5 percent) shows how the TCF7L2 gene (rs12255372) was amplified by T-ARMS PCR using a gradient protocol. In this case, the same PCR conditions were used apart from the temperature at which the primers were annealed, which was set at 50 °C to 60 °C. From the results, it was concluded that the most effective temperature for amplification is 58 °C. The gel contains the “M” label, which is a molecular marker (3000-100 bp) from the company GeneDirex Korea, South Korea, which verifies the size of the amplified fragments.
Figure 5: Control: The agarose gel electrophoresis image (1.5% agarose) illustrates the amplification of the TCF7L2 gene (rs12255372) using T-ARMS PCR. This indicates the presence of genotypes (GT, TT, GG) in the control group. The marker M is a molecular weight marker (3000-100 bp) obtained from GeneDirex, South Korea.
Figure 6: Patients: The image of agarose gel electrophoresis (1.5% agarose) displays the amplification of the TCF7L2 gene (rs12255372) using T-ARMS PCR. This reveals the presence of genotypes (GT, TT, GG) in the patients. The marker M is a molecular weight marker (3000-100 bp) sourced from GeneDirex, South Korea
4. DISCUSSION
The results of the study “Inabilities in Using Distinct Biomarkers to Diagnose Pancreatic Dysfunction in Breast Cancer Patients” show how the inflammatory markers and polymorphisms of genes contribute to the growing research of breast cancer and pancreatic dysfunction. The results of this study show some agreement and disagreement with previous works, underlying the nuances in the application of biomarkers and genetic modifications in cancer diagnosis and treatment.
4.1. ALP as a Biomarker
This study shows that ALP by itself is not an adequate biomarker for indicating pancreatic abnormalities in breast cancer patients, owing to its low AUC of 0.55.
This corroborates with other studies that have previously raised concerns regarding the lack of specificity of ALP as a biomarker when used independently. Sharma et al. point out that ALP is raised in liver and bone diseases, which may pose a problem to its diagnostic use in many cancer patients.1 On the contrary, some literature advocates for more attention to be placed towards metabolic disturbances that are state-specific to cancer when using ALP as a complement to other markers. We partake in the view that ALP does not provide much diagnostic information when used alone, but that view will change when ALP is part of a multi-marker panel.
4.2. CRP as a Biomarker
The diagnostic accuracy of CRP corresponds to an AUC of 0.60, which is, to some extent, above average. However, the lower levels of CRP in breast cancer patients in reference to healthy controls are quite surprising and unlike most studies that, in fact, document heightened levels in cancer patients because of inflammation.2 This difference can result from the disease's stage, treatment received, or some particular changes in the metabolism related to the tumor microenvironment. More work is required to clarify and understand the mechanisms and determination of whether limiting factors such as CRP concentrations make specific breast cancer subtype variance or treatment regime change modification acceptable.
Undoubtedly, contrary to expectations, CRP values were notably lower in patients with breast cancer in comparison with their healthy counterparts. This surprising figure may indicate the inflammatory response heterogeneity among patients suffering from cancer, perhaps due to the tumor’s stage, the tumor microenvironment’s immunosuppressive function, or even some treatments like chemotherapy or immunotherapy, which modify the expression of CRP. More recent cancer research indicated some subtypes of breast cancer—primarily those that are hormone receptor positive and HER2-enriched—are less likely to induce significant systemic elevations of CRP, particularly in immune checkpoint blockade or anti-inflammatory treatment responsive situations. A different plausible rationale is cancer-induced cachexia, or altered metabolism, which may blunt usual acute phase reactant responses. More longitudinal and mechanistic research is needed to clarify the influence of CRP changes over time in relation to the advancement of breast cancer and its treatment.
4.3. IL-6 as a Biomarker
The diagnostic limitations of IL-6 are unexpected, especially considering its significance in inflammation and tumor progression. Undoubtedly, IL-6 did not show any notable difference among breast cancer patients in comparison to healthy counterparts.3 Previous literature has suggested that IL-6 is involved in the microenvironment of a tumor and serves as a prognostic marker for specific cancers. Nonetheless, our data demonstrates that IL-6 is not likely to be a useful pancreatic dysfunction marker in breast cancer patients, at least in the studied cohort. This change may be due to the distinct study populations, differing cancer stages, or even diversity in methods. More research is required to determine the role of IL-6 in a multi-marker panel as well as the specific subtypes of breast cancer.
4.4. Polymorphism of the TCF7L2 Gene
The examination of the TCF7L2 gene polymorphism suggests a possible link with pancreatic disorder due to the increased frequency of breast cancer patients with the GG genotype. This is in accordance with prior studies that have associated TCF7L2 polymorphisms with metabolic problems such as type 2 diabetes and, within the context, pancreatic disorder.4 This phenomenon may be the result of numerous breast cancer patients who previously had the GG genotype demonstrating a higher rate of pancreatic dysfunction, indicating a greater genetic impact toward metabolic changes in the presence of malignancy. These assertions need to be substantiated with additional research for validation, especially to understand the functional ramifications of TCF7L2 polymorphisms on breast cancer and pancreatic health. The conclusion that ALP, IL-6, and CRP are not useful as single biomarkers is consistent with some studies but contrasts with others that have reported significant correlations between these biomarkers and cancer outcomes. One example regarding this, Mantovani et al., highlighted the significance of CRP in cancer-related inflammation; however, our study reported lower levels of CRP in breast cancer patients, which indicates the association of CRP and cancer may be more complex than what was understood.2 Likewise, Knüpfer and Preiss illustrated the significance of IL-6 in the progression of breast cancer, but we did not find a significant difference in IL-6 levels in the patient and control participants, suggesting that the diagnostic value of IL-6 is population and context-dependent.3
This study underscores, and to an extent contradicts, other work done concerning the use of ALP, IL-6, and CRP as singular diagnostic markers for pancreatic dysfunction in breast cancer patients. The low ALP diagnostic accuracy observed here, AUC = 0.55, resonates with Patel et al.,12 who pointed out that ALP sensitivity for pancreatic complications in colorectal cancer patients is nonspecific due to its elevation in many other pathologies. However, Zhang et al.13 provided evidence to the contrary, suggesting that some ALP isoforms, notably intestinal ALP, are associated with metabolic dysregulation and advanced malignancy. These contrasting claims reveal the need for a multi-marker approach that could potentially provide a solution to the issue outlined. The unexpected finding of lower CRP levels in breast cancer patients, alongside the work of Lee et al.14 highlights the necessity for longitudinal studies that aim to clarify CRP’s role in cancer-associated inflammation. Lee’s study determined that CRP levels decrease in metastatic breast cancer patients treated with immunotherapy, further substantiating the growing need for multidisciplinary studies. Lastly, there is a significant deviation from prior work undertaken by Chen et al. in their analysis of IL-6.16 Raised IL-6 levels serve as a marker of pancreatic metastatic spread in triple-negative breast cancer, which is a clear example of this cytokine’s context-dependent variability.
The correlation of the TCF7L2 GG genotype with pancreatic dysfunction is also consistent with new studies that have proposed the TCF7L2 variants as being associated with Wnt signaling insulin resistance in cancer.16 These results bolster the case for using genetic profiling to identify patients with an increased risk and tailor treatment accordingly. Indeed, the shortcomings of the single biomarkers as pointed out by Torres et al.17 demonstrate the need for new approaches to cancer diagnosis that combine correlational evidence.
4.5. Association Between TCF7L2 Genotype and Biomarker Levels
In order to examine further aspects of genetic susceptibility and systemic inflammation, we analyzed biomarker data concerning the TCF7L2 genotype. TCF7L2 breast cancer patients with the GG genotype appeared to have slightly elevated ALP levels and lower CRP levels compared to those with the TT and GT genotypes; however, these differences were not statistically significant (p > 0.05). IL-6 did not show any consistent pattern in this regard either. In any case, these data are too simplistic, but do imply that some variation at TCF7L2 might modulate the inflammation or the metabolism involving pancreatic cancerous processes in breast cancer patients. Although this much is evident, the present results need to be confirmed in studies involving larger cohorts.
4.6. Integration of Genotype and Biomarker Data
To assess how genetic variation of TCF7L2 may impact inflammation or metabolic activity, we analyzed the ALP, CRP, and IL-6 levels by genotype. It was noted that patients carrying the GG genotype had higher ALP and lower CRP compared to the TT or GT genotypes, but these differences were not significant (P > 0.05, Table 6). No persistent differences were noted regarding IL-6 levels either. While such results are premature, they point towards the possibility of some genetic factors in systemic inflammatory and metabolic changes in women with breast cancer and pancreatic insufficiency.
5. CONCLUSION
This case study demonstrates the complexities in using distinct biomarkers to diagnose pancreatic dysfunction in patients suffering from breast cancer. While ALP, IL-6, and CRP did not display much promise as individual results, the output can be improved through the incorporation of other genetic markers. The interplay between the TCF7L2 gene polymorphism and pancreatic dysfunction in breast cancer patients is yet to be fully understood. A new direction to the existing body of literature could provide further understanding of the genetic components of metabolic imbalance associated with cancer. Targeting the interactions between the biomarkers and genetic factors is a promising area in need of research to aid in the diagnosis and treatment of breast cancer and pancreatic malignancies.
6. Data availability
The numerical data generated during this research are available from the authors.
7. Acknowledgments
The University of Al-Qadisiyah College of Medicine deserves recognition for its beneficent assistance. Sincere gratitude is extended to all the female breast cancer patients who participated in this study and greatly contributed to its completion. Special thanks are also due to the staff of the Oncology Department at Al-Diwaniyah Teaching Hospital in Al-Diwaniyah for their proactive support.
8. Financial support and sponsorship
This was a self‑funded study.
9. Ethical considerations
Written informed consent was obtained from all patients and, where applicable, from their parents or guardians for sample collection. The principles of the Declaration of Helsinki (1964) concerning medical research on human subjects were followed. Furthermore, the research was approved by the Research and Ethics Committee of the university.
10. Conflicts of interest
The authors declare that they have no competing interests and no conflicts of interest in the current study.
11. Authors’ contribution
DIJ: Laboratory Work, Data Curation, Resources, Formal Analysis, Writing, and Original Draft Preparation.
AGZ: Conceptualization, Methodology Design, Project Supervision, Statistical Analysis, Interpretation of Results, Review & Editing, and Corresponding Author Responsibilities.
12. REFERENCES
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. 694-701 DOI: 3322/caac.21492
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–74. [PubMed] DOI: 1016/j.cell.2011.02.013
- Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–99. [PubMed] DOI: 1016/j.cell.2010.01.025
- Sharma U, Pal D, Prasad R. Alkaline phosphatase: an overview. Indian J Clin Biochem. 2014;29(3):269–78. [PubMed] DOI: 1007/s12291-013-0408-y
- Knüpfer H, Preiss R. Significance of interleukin-6 (IL-6) in breast cancer. Breast Cancer Res Treat. 2007;102(2):129–35. [PubMed] DOI: 1007/s10549-006-9328-3
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–44. [PubMed] DOI: 1038/nature07205
- Grant SF, Thorleifsson G, Reynisdottir I, Benediktsson R, Manolescu A, Sainz J, et al. Variant of transcription factor 7-like 2 (TCF7L2) gene confers risk of type 2 diabetes. Nat Genet. 2006;38(3):320–3. [PubMed] DOI: 1038/ng1732
- Abed HH, Ali AM, Al-Ziaydi AG. Evaluation level of serum vitamin B12 in Iraqi patients with diabetes mellitus type 2, who used the metformin drug as a hypoglycemic agent. Pak J Pharm Sci. 2023;36(2):425-9. [PubMed]
- Abed HH, Al-Ziaydi AG, Taher IA, Al Dulaimi AK. Comparison of some hematological parameters between male and female patients infected with COVID-19. Hum Antibodies. 2022;30(3):151-5. [PubMed] DOI: 3233/HAB-220006
- Al-Ziaydi AG. Evaluation of D-Mannoheptulose and Doxorubicin as Potential Therapeutic Agents for Breast Cancer by Targeting Glycolysis and Inducing Apoptosis. Indian J Clin Biochem. 2025;40(3):412-421.[PubMed] DOI: 1007/s12291-024-01266-0
- Kadooh QA, Al-Ziaydi AG, Hamza AJ. Evaluation of the influence of trastuzumab therapy on serum levels of HER-2 protein and breast cancer cell lines. Prz Menopauzalny. 2024;23(1):28-35. [PubMed] DOI: 5114/pm.2024.139607