Shamim Kausar 1 , Rohan Advani 2 , Zeeshan Ali 3 , Wajeeha Batool 4
Authors affiliations:
Background & Objective: Sepsis is a major global health threat, and it is especially true for low- and middle-income countries. Sepsis may be a result of deteriorated acid-base balance, or it may lead to such an imbalance in its own right. Both conditions pose a major challenge in the intensive care unit (ICU) patients. This study investigates the impact of acid-base disorder on the severity of sepsis and its associated mortality in critically ill patients.
Methodology: A retrospective cohort study was conducted covering the period from December 2022 to December 2023 at Jinnah Post Graduate Medical Centre, Karachi, Pakistan. We included 144 patients admitted to the medical Intensive care unit (ICU)/High dependency unit (HDU) with suspected sepsis, based upon laboratory investigations and physical signs. Acid-base disorders were investigated using arterial blood gas analyses. Outcomes were determined as mortalities and the length of ICU/HDU stay. Appropriate statistical tests such as chi-square or Fisher exact tests for categorical variables and t-test for continuous variables, were used. P < 0.05 was considered to be statistically significant.
Results: Out of 144 patients, 71 (49.3%) participants had metabolic acidosis categorized as mild (29.8%), moderate (16.6%) and severe (2.8%). In contrast, 39 patients (27.1%) had metabolic alkalosis, categorized as mild (20.8%) and moderate (6.3%). Additionally, 34 (23.6%) patients had a normal acid-base status. The pH differed significantly between acid-base groups (P = 0.000). Overall mortality was 31.3% (n = 45). Notably, patients with severe metabolic acidosis exhibited a 100% mortality rate compared to only 20.59% among those with normal acid-base status. Serum lactate was the only significant prognostic marker in this study (P < 0.05).
Conclusion: This study shows that acid-base imbalance in sepsis is significantly linked to mortality, with severe metabolic acidosis yielding 100% mortality. It also demonstrates serum lactate as a crucial prognostic marker.
Abbreviations: HDU: High dependency unit, ICU: Intensive care unit, SIRS: Systemic Inflammatory Response Syndrome, SOFA: Sequential Organ Failure Assessment
Keywords: Acid-base disorder; Base excess; Intensive Care Unit; Lactic acidosis; Length of stay; Metabolic Acidosis; Metabolic Alkalosis; Mortality; pH; Sepsis
Citation: Kausar S, Advani R, Ali Z, Batool W. Prevalence of acid-base disorders and impact on outcome in sepsis in critically ill patients: A retrospective cohort study. Anaesth. pain intensive care 2025;29(7):764-769. DOI: 10.35975/apic.v29i7.2952
Received: September 26, 2024; Revised: May 29, 2025; Accepted: September 02, 2025
Sepsis is a significant global health burden that affects millions of people worldwide each year, with a disproportionate impact on low- and middle-income countries.1 The management of sepsis, particularly in critically ill patients, is complex and multifaceted, requiring accurate assessment of illness severity and prediction of patient outcomes.2
Acid-base imbalances are common in hospitalized patients and must not be overlooked while treating the primary cause to avoid adverse outcomes, with acidemia being the most common finding.3, 4 A study found that the presence of metabolic acidosis in critically ill patients was associated with 20% increase in mortality risk (45% vs. 25%.5 High mortality (80%) is observed in patients with metabolic alkalosis when the pH is >7.65, which can cause complications such as hypercapnia, hypoxemia, cardiac arrhythmias, altered consciousness, and neuromuscular hyper-excitability.6
The arterial blood gas analysis is a point-of-care test in the setting of acute emergency, pending other Labs. Correlation of acid-base disorder with the prognosis of a patient during sepsis can change the management strategies and extent of treatment by the physician.
The Sequential Organ Failure Assessment (SOFA) score is a commonly used tool for predicting mortality in patients with sepsis and multi-organ involvement.7 However, SOFA does not account for metabolic disturbances such as pH, which are considered important predictors of mortality in some scoring systems like APACHE II.8
The exclusion of metabolic disturbances from the scoring system has not been well studied, and the impact of this exclusion on outcome prediction is unclear.9 Only limited studies have been performed on determining the prevalence, types, and impact on outcome of acid-base disturbances in patients with sepsis, and the type of disorder that may potentially predict the outcome in sepsis.
The objectives of the study were to determine the prevalence and different types of acid-base disorders and evaluate their impact on clinical outcomes in patients with sepsis admitted to the intensive care unit (ICU), and to explore potential associations between acid-base disorders and other prognostic factors, such as lactate levels, blood sugar, base excess, and serum creatinine levels.
The research was undertaken at Jinnah Postgraduate and Medical Centre (JPMC), a public sector hospital in Karachi, Pakistan, using a retrospective cohort design.
All patients between the ages of 18 to 70 diagnosed with sepsis and admitted to the medical ICU, HDU from December 2022 to December 2023 were included in the study. Sepsis was diagnosed when there was evidence of infection (positive culture of blood, urine, tracheal aspirate) or with clinical signs of infection along with at least 2 out of 4 of Systemic Inflammatory Response Syndrome (SIRS) criteria. These included: (i) Tachycardia - Heart rate > 90 beats/min, (ii) Tachypnea -Respiratory rate >20 breaths/min, (iii) Leukocytosis (WBC >12000/mm3) or Leucopenia (WBC < 4000/mm3), (iv) fever or Hypothermia (Temp >38 or <36 °C).
Patients with fulminant hepatic failure, acute poisoning, chronic kidney disease stage 5, advanced chronic obstructive pulmonary disease on long-term oxygen therapy, pregnant females, patients whose mortality status could not be assessed from the hospital files record, and patients without any data on acid-base status were excluded from the study population.
Acid-base disorders were defined as a deviation in blood pH (Power of hydrogen) from the normal range of 7.35 – 7.45. This deviation was subdivided as follows: mild acidosis (7.25-7.35), moderate acidosis (7.0-7.25), severe acidosis (<7.0), mild alkalosis (7.45-7.55), moderate alkalosis (7.55-7.65), severe alkalosis (7.65-7.75). Prevalence was considered as a percentage of different acid-base disorders amongst the participants of the study.
Outcomes were determined as mortalities and the length of ICU/HDU stay. Patients who expired during the hospital stay were considered as mortality. Length of ICU/HDU stay in days was considered as the mean of days spent in MICU/HDU was taken as another outcome of the study.
After IRB approval (No. F.2-81/2024-GENL/53/JPMC), records of the patients were retrieved who were admitted to JPMC's medical ICU and HDU of Medical Unit 4, with diagnosed cases of sepsis as per the operational definition, were included as per the inclusion and exclusion criteria. Non-probability sampling was used to ensure inclusion of all patients fulfilling the criteria. The data about patients’ demographics were recorded. Further record of Power of Hydrogen (pH), Serum creatinine level, Blood Sugar Random (BSR), lactic acid levels, and Base excess levels at the time of admission, along with mortality and length of ICU/HDU stay, were recorded.
Data were analyzed using the Statistical Package for Social Sciences (SPSS, version 24.0). Continuous variables were presented as either the mean and standard deviation or the median, while categorical variables were presented as numbers and percentages. To compare the characteristics of patients who died or who survived, appropriate statistical tests such as chi-square or Fisher exact tests for categorical variables and t-test for continuous variables were used. A P < 0.05 was considered to be statistically significant.
The study included a sample size of 144 participants, of which 52.8% were male (n = 76) and 47.2% were female (n = 68). Participants had an age range between 12 and 75 y (mean 30.95 ± 13.39 years). The mean pH level was 7.36 ± 0.13, and the mean base excess (BE) was -3.96 ± 26.58. The blood sugar level (mg/dL) had a mean of 169.31 ± 100.96. Creatinine levels (mg/dL) averaged 1.76 ± 1.81, and lactic acid levels averaged 3.36 ± 2.51. The length of ICU stay ranged from 1 to 27 days, with a mean of 3.95 ± 3.39. Out of the 144 participants, Amongst the participants of our study, the prevalence of different categories of acid-base disorder as per the operational definition was analyzed. It was revealed that 43 (29.9%) had mild acidosis, 24 (16.7%) had moderate acidosis, and 4 (2.8%) had severe acidosis. 30 participants (20.8%) had mild alkalosis, 9 had moderate alkalosis (6.3%), while 34 (23.6%) participants had a normal range of acid-base levels. The difference in the pH of the acid-base group was statistically significant with a P-value of 0.000.
Overall mortality was observed in 31.3% (n = 45) of the participants, and 68.8% (n = 99) participants survived during their ICU/HDU stay. The percentage contributed by each acid-base disorder group in the overall mortality of the study is shown in Figure 1.
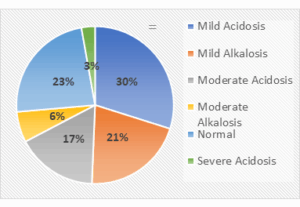
Figure 1: Percentages contributed by each study group in gross mortality.
To explore the relationship between specific metabolic disorders and their associated mortality, a stratified analysis was performed (Table 2). The results revealed significant findings. Among the patients with severe acidosis (n = 4) no one survived (mortality rate = 100%) with a P value of 0.003. The group with moderate alkalosis (n = 9) also exhibited a very high mortality rate of 66.67% with P = 0.018, while the patients with moderate acidosis (n = 24) showed a mortality rate of 37.5%. Patients with mild acidosis (n = 43) or alkalosis (n = 30) had mortality rates of 25.58% and 26.67%, respectively, reflecting an increased survival rate compared to other groups. Normal acid-base status (n = 34) had the lowest mortality rate of 20.59% amongst all groups. Table 1 highlights the mortality and survival rates among different acid-base groups.
Further analysis showed no significant difference in mean age among different acid-base groups, with severe acidosis having the lowest mean age (23.00 ± 8.12) and mild acidosis having the highest mean age (34.13 ± 14.20).
Base excess showed the lowest mean value in the severe acidosis group (-20.40 ± 7.40) and the highest mean value in the moderate alkalosis group (0.33 ± 6.05). Our study showed a significant difference (P = 0.017) in mean lactic acid levels, with the lowest value in the mild alkalosis group (2.73 ± 1.53) and the highest value in the severe acidosis group (6.63 ± 8.68). It was also found that mean blood sugar levels were highest in the severe acidosis group (228.25 ± 53.13) and lowest in the mild alkalosis group (134.8 ± 56.97), with an insignificant difference (P = 0.182). Likewise, mean serum creatinine levels were highest in the moderate acidosis group (2.27 ± 2.49) and lowest in the moderate alkalosis group (0.85 ± 0.43), with an insignificant difference (P = 0.426). The mean length of ICU stay was shortest in the severe acidosis group (3.23 ± 2.06) and longest in the normal acid-base status group (3.94 ± 3.04), with an insignificant difference (P = 0.932). Table 2 highlights a comparison of different parameters amongst acid-base subgroups.
Sepsis is a potentially fatal condition that leads to impaired function of one or more vital organs as a result of the dysregulated body’s response to infection.
It shares the major burden on the healthcare system in resource-constrained countries. It is estimated that more than 19 million sepsis cases and 5 million sepsis-related deaths occur annually, with the majority of these cases and deaths happening in low and middle-income countries (LMICs).10 Hence, early prognostication of illness is important to determine the extent of treatment and outcomes of the disease.
In our study, we tried to establish the role of pH as an independent mortality predictor of patients with sepsis. The literature reports metabolic acidosis associated with lactic acidosis as the most common metabolic disturbance among septic patients.11 Our results corroborate this finding, with metabolic acidosis being the most common acid-base disorder observed in our study (n = 71). It was also seen in our study that the lactate levels were highest in patients with severe acidosis compared to the lowest in the mild alkalosis group. These levels had a significant correlation with mortality (P = 0.017). The etiology of hyper-lactatemia is multifactorial that involving overproduction due to anaerobic glycolysis as well as reduced clearance in patients with sepsis.12
Several studies have explored the utility of elevated lactate and associated metabolic acidosis in the prognostication of septic patients. Puskarich et al. (2013) studied resuscitation in sepsis during first 6 hours of management and found that reduced clearance of lactate is associated with increased mortality.13 This necessitates early goal-directed management of shock to reduce serum lactate levels and subsequent acidemia, thereby improving overall mortality.
In our study, metabolic alkalosis was found in only 39 patients out of 144, and among them, the patients with moderate metabolic alkalosis exhibited significantly greater mortality (66%; P value 0.018). This finding was contradictory to a previous study by Kreü S et al. whose research found no deleterious effect of metabolic alkalosis in septic patients, except for prolonged ICU stay.13 The association between metabolic alkalosis and increased mortality is attributed to several underlying factors, such as over-correcting hypotension and shock through aggressive fluid resuscitation, specifically Ringer’s lactate administration and transfusion of citrated blood. These interventions result in alkalinization of the blood, which causes hypoventilation as a physiological response before the kidneys start to excrete excess bicarbonate. Alkalosis is also associated with hypokalemia, which can result in life-threatening arrhythmias.14
We also investigated the association of acid-base disorders with other prognostic markers of sepsis, including base excess, random blood sugars, serum creatinine, and length of stay in the ICU.
Notably, the base excess (BE) - the amount of base/acid needed to restore normal blood pH- serves as a sensitive indicator of acid-base disorder. Unlike pH, which is affected by both respiratory and metabolic factors, BE exclusively reflects acid-base balance.15 Our study found that the patients with severe metabolic acidosis had the lowest base excess among all the groups, although this difference did not reach statistical significance (P > 0.05). This finding contrasts with a previous study conducted by Junfang Qi et al., which reported a significant correlation between BE and pH in poly-trauma patients (P < 0.05). This discrepancy can be largely attributed to the difference in sample size as our study included a small number of patients with metabolic acidosis (n = 71) compared to 495 patients with metabolic acidosis in Junfanq Qi’s research.16
Our study also examined the relationship between blood sugar levels and acid-base imbalance. Notably, the group with severe metabolic acidosis (all non-survivors) exhibited significantly elevated blood sugar levels compared to other participants (228.25 ± 53.13 mg/dL). This finding may be attributed to enhanced metabolism in sepsis, leading to insulin resistance.17 Despite the non-significant result (P > 0.05), our findings underscore the need for further investigation. To the best of our knowledge, there is limited literature exploring the relationship between hyperglycemia and acid-base disequilibrium, and further studies are warranted to establish a potential correlation.
We also observed a trend of shorter ICU stay in patients with severe metabolic acidosis, suggesting early mortality associated with academia. This finding is consistent with a study conducted in India by Sujay Samanta et al.18 which also reported an association between low pH and shorter ICU stay in non-survivors. Although our findings lacked statistical significance, unlike Samanta’s study, it nonetheless supports the notion that severe metabolic acidosis leads to rapid clinical deterioration.
Contrary to our expectations, the mean serum creatinine was unexpectedly lower in all non-survivor groups i.e. severe metabolic acidosis, compared to other groups (except for mild metabolic alkalosis), which exhibited higher mean serum creatinine values. This result implies that deranged renal function did not predict mortality in our study. This observation was not statistically significant (P > 0.05)
This study had several limitations. Complete biochemical and metabolic data were not available for the patients included in the study. As a result, the analysis conducted was restricted to acid-base disturbances without additional information regarding anion gap or respiratory acidosis or alkalosis. Furthermore, our patient cohort was followed only for a period of hospital admission, with no follow-up data available after discharge. As a result, we were unable to assess readmission rates and long-term mortality.
Despite these limitations, our study underscores the need for future research to focus on formulating scoring system that integrates pH levels with clinical parameters as an important prognostic indicator in septic patients.
Acid-base imbalance is quite prevalent in septic patients and has a significant impact on the mortality rate. Severe metabolic acidosis carries 100% mortality in our study compared to only a 20.59% death rate in patients with normal acid-base status.
Serum lactate levels are substantially elevated in patients with severe metabolic acidosis, serving as a critical prognostic marker. Its monitoring should be prioritized in sepsis management.
Acid-base imbalance affects patients of all ages. While base excess, serum creatinine, blood sugar, and length of ICU stay differ among acid-base disorder groups, these variations lack statistical significance. Further studies are warranted to illustrate potential correlations.
Prompt diagnosis and management of acid-base disorders greatly improve outcomes in sepsis patients. Targeted interventions should be developed for early correction of acid-base disequilibrium.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflicts of interest
Authors declare no conflict of interest.
9. Author's contribution
SK: Concept and design of the study, acquisition of data, and analysis
RA: Drafting the paper and result writing
ZA: Revising and approving the article and providing the intellectual concept.
WB: Contributed to writing the manuscript, critically revised the article
Authors affiliations:
- Shamim Kausar, Critical Care Consultant and Physician, Jinnah Postgraduate Medical Centre, Karachi, Pakistan; Email: drshamimahsan@gmail.com; {ORCID:0000-0001-8291-492X}
- Rohan Advani, Intern, Jinnah Postgraduate Medical Centre, Karachi, Pakistan; Email: rohan_advani@ymail.com
- Zeeshan Ali, Associate Professor Medicine, Jinnah Postgraduate Medical Centre, Karachi, Pakistan; Email: Dr.zeeshan.j@gmail.com; {ORCID:0000-0001-8291-492X}
- Wajeeha Batool, Resident Internal Medicine, Jinnah Postgraduate Medical Centre, Karachi, Pakistan; Email: batool.syedawajeeha@yahoo.com; {ORCID:0009-0008-4012-7993}
ABSTRACT
Background & Objective: Sepsis is a major global health threat, and it is especially true for low- and middle-income countries. Sepsis may be a result of deteriorated acid-base balance, or it may lead to such an imbalance in its own right. Both conditions pose a major challenge in the intensive care unit (ICU) patients. This study investigates the impact of acid-base disorder on the severity of sepsis and its associated mortality in critically ill patients.
Methodology: A retrospective cohort study was conducted covering the period from December 2022 to December 2023 at Jinnah Post Graduate Medical Centre, Karachi, Pakistan. We included 144 patients admitted to the medical Intensive care unit (ICU)/High dependency unit (HDU) with suspected sepsis, based upon laboratory investigations and physical signs. Acid-base disorders were investigated using arterial blood gas analyses. Outcomes were determined as mortalities and the length of ICU/HDU stay. Appropriate statistical tests such as chi-square or Fisher exact tests for categorical variables and t-test for continuous variables, were used. P < 0.05 was considered to be statistically significant.
Results: Out of 144 patients, 71 (49.3%) participants had metabolic acidosis categorized as mild (29.8%), moderate (16.6%) and severe (2.8%). In contrast, 39 patients (27.1%) had metabolic alkalosis, categorized as mild (20.8%) and moderate (6.3%). Additionally, 34 (23.6%) patients had a normal acid-base status. The pH differed significantly between acid-base groups (P = 0.000). Overall mortality was 31.3% (n = 45). Notably, patients with severe metabolic acidosis exhibited a 100% mortality rate compared to only 20.59% among those with normal acid-base status. Serum lactate was the only significant prognostic marker in this study (P < 0.05).
Conclusion: This study shows that acid-base imbalance in sepsis is significantly linked to mortality, with severe metabolic acidosis yielding 100% mortality. It also demonstrates serum lactate as a crucial prognostic marker.
Abbreviations: HDU: High dependency unit, ICU: Intensive care unit, SIRS: Systemic Inflammatory Response Syndrome, SOFA: Sequential Organ Failure Assessment
Keywords: Acid-base disorder; Base excess; Intensive Care Unit; Lactic acidosis; Length of stay; Metabolic Acidosis; Metabolic Alkalosis; Mortality; pH; Sepsis
Citation: Kausar S, Advani R, Ali Z, Batool W. Prevalence of acid-base disorders and impact on outcome in sepsis in critically ill patients: A retrospective cohort study. Anaesth. pain intensive care 2025;29(7):764-769. DOI: 10.35975/apic.v29i7.2952
Received: September 26, 2024; Revised: May 29, 2025; Accepted: September 02, 2025
1. NTRODUCTION
Sepsis is a significant global health burden that affects millions of people worldwide each year, with a disproportionate impact on low- and middle-income countries.1 The management of sepsis, particularly in critically ill patients, is complex and multifaceted, requiring accurate assessment of illness severity and prediction of patient outcomes.2
Acid-base imbalances are common in hospitalized patients and must not be overlooked while treating the primary cause to avoid adverse outcomes, with acidemia being the most common finding.3, 4 A study found that the presence of metabolic acidosis in critically ill patients was associated with 20% increase in mortality risk (45% vs. 25%.5 High mortality (80%) is observed in patients with metabolic alkalosis when the pH is >7.65, which can cause complications such as hypercapnia, hypoxemia, cardiac arrhythmias, altered consciousness, and neuromuscular hyper-excitability.6
The arterial blood gas analysis is a point-of-care test in the setting of acute emergency, pending other Labs. Correlation of acid-base disorder with the prognosis of a patient during sepsis can change the management strategies and extent of treatment by the physician.
The Sequential Organ Failure Assessment (SOFA) score is a commonly used tool for predicting mortality in patients with sepsis and multi-organ involvement.7 However, SOFA does not account for metabolic disturbances such as pH, which are considered important predictors of mortality in some scoring systems like APACHE II.8
The exclusion of metabolic disturbances from the scoring system has not been well studied, and the impact of this exclusion on outcome prediction is unclear.9 Only limited studies have been performed on determining the prevalence, types, and impact on outcome of acid-base disturbances in patients with sepsis, and the type of disorder that may potentially predict the outcome in sepsis.
The objectives of the study were to determine the prevalence and different types of acid-base disorders and evaluate their impact on clinical outcomes in patients with sepsis admitted to the intensive care unit (ICU), and to explore potential associations between acid-base disorders and other prognostic factors, such as lactate levels, blood sugar, base excess, and serum creatinine levels.
2. METHODOLOGY
The research was undertaken at Jinnah Postgraduate and Medical Centre (JPMC), a public sector hospital in Karachi, Pakistan, using a retrospective cohort design.
All patients between the ages of 18 to 70 diagnosed with sepsis and admitted to the medical ICU, HDU from December 2022 to December 2023 were included in the study. Sepsis was diagnosed when there was evidence of infection (positive culture of blood, urine, tracheal aspirate) or with clinical signs of infection along with at least 2 out of 4 of Systemic Inflammatory Response Syndrome (SIRS) criteria. These included: (i) Tachycardia - Heart rate > 90 beats/min, (ii) Tachypnea -Respiratory rate >20 breaths/min, (iii) Leukocytosis (WBC >12000/mm3) or Leucopenia (WBC < 4000/mm3), (iv) fever or Hypothermia (Temp >38 or <36 °C).
Patients with fulminant hepatic failure, acute poisoning, chronic kidney disease stage 5, advanced chronic obstructive pulmonary disease on long-term oxygen therapy, pregnant females, patients whose mortality status could not be assessed from the hospital files record, and patients without any data on acid-base status were excluded from the study population.
Acid-base disorders were defined as a deviation in blood pH (Power of hydrogen) from the normal range of 7.35 – 7.45. This deviation was subdivided as follows: mild acidosis (7.25-7.35), moderate acidosis (7.0-7.25), severe acidosis (<7.0), mild alkalosis (7.45-7.55), moderate alkalosis (7.55-7.65), severe alkalosis (7.65-7.75). Prevalence was considered as a percentage of different acid-base disorders amongst the participants of the study.
Outcomes were determined as mortalities and the length of ICU/HDU stay. Patients who expired during the hospital stay were considered as mortality. Length of ICU/HDU stay in days was considered as the mean of days spent in MICU/HDU was taken as another outcome of the study.
After IRB approval (No. F.2-81/2024-GENL/53/JPMC), records of the patients were retrieved who were admitted to JPMC's medical ICU and HDU of Medical Unit 4, with diagnosed cases of sepsis as per the operational definition, were included as per the inclusion and exclusion criteria. Non-probability sampling was used to ensure inclusion of all patients fulfilling the criteria. The data about patients’ demographics were recorded. Further record of Power of Hydrogen (pH), Serum creatinine level, Blood Sugar Random (BSR), lactic acid levels, and Base excess levels at the time of admission, along with mortality and length of ICU/HDU stay, were recorded.
Data were analyzed using the Statistical Package for Social Sciences (SPSS, version 24.0). Continuous variables were presented as either the mean and standard deviation or the median, while categorical variables were presented as numbers and percentages. To compare the characteristics of patients who died or who survived, appropriate statistical tests such as chi-square or Fisher exact tests for categorical variables and t-test for continuous variables were used. A P < 0.05 was considered to be statistically significant.
3. RESULTS
The study included a sample size of 144 participants, of which 52.8% were male (n = 76) and 47.2% were female (n = 68). Participants had an age range between 12 and 75 y (mean 30.95 ± 13.39 years). The mean pH level was 7.36 ± 0.13, and the mean base excess (BE) was -3.96 ± 26.58. The blood sugar level (mg/dL) had a mean of 169.31 ± 100.96. Creatinine levels (mg/dL) averaged 1.76 ± 1.81, and lactic acid levels averaged 3.36 ± 2.51. The length of ICU stay ranged from 1 to 27 days, with a mean of 3.95 ± 3.39. Out of the 144 participants, Amongst the participants of our study, the prevalence of different categories of acid-base disorder as per the operational definition was analyzed. It was revealed that 43 (29.9%) had mild acidosis, 24 (16.7%) had moderate acidosis, and 4 (2.8%) had severe acidosis. 30 participants (20.8%) had mild alkalosis, 9 had moderate alkalosis (6.3%), while 34 (23.6%) participants had a normal range of acid-base levels. The difference in the pH of the acid-base group was statistically significant with a P-value of 0.000.
| Table 1: Acid-base disorders and mortality rate. | ||||
| Metabolic Disorder | (n = 144) | Died | Survived | P-value |
| Normal | 34 | 7 (20.59) | 27 (79.41) | 0.125 |
| Mild Acidosis | 43 | 11 (25.58) | 32 (74.42) | 0.332 |
| Mild Alkalosis | 30 | 8 (26.67) | 22 (73.33) | 0.543 |
| Moderate Acidosis | 24 | 9 (37.50) | 15 (62.50) | 0.469 |
| Moderate Alkalosis | 9 | 6 (66.67) | 3 (33.33) | 0.018* |
| Severe Acidosis | 4 | 4 (100.00) | 0 (0.00) | 0.003* |
| Data presented as n (%)’ P < 0.05 is considered significant. | ||||
Overall mortality was observed in 31.3% (n = 45) of the participants, and 68.8% (n = 99) participants survived during their ICU/HDU stay. The percentage contributed by each acid-base disorder group in the overall mortality of the study is shown in Figure 1.
Figure 1: Percentages contributed by each study group in gross mortality.
To explore the relationship between specific metabolic disorders and their associated mortality, a stratified analysis was performed (Table 2). The results revealed significant findings. Among the patients with severe acidosis (n = 4) no one survived (mortality rate = 100%) with a P value of 0.003. The group with moderate alkalosis (n = 9) also exhibited a very high mortality rate of 66.67% with P = 0.018, while the patients with moderate acidosis (n = 24) showed a mortality rate of 37.5%. Patients with mild acidosis (n = 43) or alkalosis (n = 30) had mortality rates of 25.58% and 26.67%, respectively, reflecting an increased survival rate compared to other groups. Normal acid-base status (n = 34) had the lowest mortality rate of 20.59% amongst all groups. Table 1 highlights the mortality and survival rates among different acid-base groups.
| Table 2: Comparison of different parameters of acid-base groups. | |||||||
| Parameters | Normal | Mild Acidosis | Mild Alkalosis | Moderate Acidosis | Moderate Alkalosis | Severe Acidosis | P value |
| Age (y) | 29.94 ± 13.27 | 34.13 ± 14.20 | 29.62 ± 15.73 | 30.33 ± 10.17 | 29.00 ± 10.29 | 23.00 ± 8.12 | 0.476 |
| pH | 7.40 ± 0.03 | 7.31 ± 0.02 | 7.48 ± 0.022 | 7.19 ± .0.04 | 7.57 ± 0.023 | 6.94 ± 0.06 | 0.000 |
| Base excess | -0.12 ± 3.06 | -9.80 ± 9.86 | -0.93 ± 4.88 | -5.32 ± 6.50 | 0.33 ± 6.05 | -20.40 ± 7.40 |
0.240 |
| Blood sugar (mg/dL) | 166 ± 92.95 | 171 ± 103.80 | 134.8 ± 56.97 | 204.09 ± 150.65 | 173.11 ± 72.68 | 228.25 ± 53.13 | 0.182 |
| Serum Creatinine (mg/dL) | 1.83 ± 1.67 | 1.65 ± 1.58 | 1.79 ± 1.93 | 2.27 ± 2.49 | 0.85 ± 0.43 | 1.08 ± 0.66 | 0.426 |
| Lactic acid (mmol/L) | 2.75 ± 2.06 | 3.25 ± 2.64 | 2.73 ± 1.53 | 4.09 ± 2.75 | 5.67 ± 2.23 | 6.63 ± 8.68 | 0.017 |
| ICU/HDU stay (days) | 3.94 ± 3.04 | 3.83 ± 2.76 | 4.53 ± 4.78 | 3.62 ± 2.88 | 3.77 ± 4.02 | 3.23 ± 2.06 | 0.932 |
| Data presented as mean ± SD’ P < 0.05 is considered significant. | |||||||
Further analysis showed no significant difference in mean age among different acid-base groups, with severe acidosis having the lowest mean age (23.00 ± 8.12) and mild acidosis having the highest mean age (34.13 ± 14.20).
Base excess showed the lowest mean value in the severe acidosis group (-20.40 ± 7.40) and the highest mean value in the moderate alkalosis group (0.33 ± 6.05). Our study showed a significant difference (P = 0.017) in mean lactic acid levels, with the lowest value in the mild alkalosis group (2.73 ± 1.53) and the highest value in the severe acidosis group (6.63 ± 8.68). It was also found that mean blood sugar levels were highest in the severe acidosis group (228.25 ± 53.13) and lowest in the mild alkalosis group (134.8 ± 56.97), with an insignificant difference (P = 0.182). Likewise, mean serum creatinine levels were highest in the moderate acidosis group (2.27 ± 2.49) and lowest in the moderate alkalosis group (0.85 ± 0.43), with an insignificant difference (P = 0.426). The mean length of ICU stay was shortest in the severe acidosis group (3.23 ± 2.06) and longest in the normal acid-base status group (3.94 ± 3.04), with an insignificant difference (P = 0.932). Table 2 highlights a comparison of different parameters amongst acid-base subgroups.
4. DISCUSSION
Sepsis is a potentially fatal condition that leads to impaired function of one or more vital organs as a result of the dysregulated body’s response to infection.
It shares the major burden on the healthcare system in resource-constrained countries. It is estimated that more than 19 million sepsis cases and 5 million sepsis-related deaths occur annually, with the majority of these cases and deaths happening in low and middle-income countries (LMICs).10 Hence, early prognostication of illness is important to determine the extent of treatment and outcomes of the disease.
In our study, we tried to establish the role of pH as an independent mortality predictor of patients with sepsis. The literature reports metabolic acidosis associated with lactic acidosis as the most common metabolic disturbance among septic patients.11 Our results corroborate this finding, with metabolic acidosis being the most common acid-base disorder observed in our study (n = 71). It was also seen in our study that the lactate levels were highest in patients with severe acidosis compared to the lowest in the mild alkalosis group. These levels had a significant correlation with mortality (P = 0.017). The etiology of hyper-lactatemia is multifactorial that involving overproduction due to anaerobic glycolysis as well as reduced clearance in patients with sepsis.12
Several studies have explored the utility of elevated lactate and associated metabolic acidosis in the prognostication of septic patients. Puskarich et al. (2013) studied resuscitation in sepsis during first 6 hours of management and found that reduced clearance of lactate is associated with increased mortality.13 This necessitates early goal-directed management of shock to reduce serum lactate levels and subsequent acidemia, thereby improving overall mortality.
In our study, metabolic alkalosis was found in only 39 patients out of 144, and among them, the patients with moderate metabolic alkalosis exhibited significantly greater mortality (66%; P value 0.018). This finding was contradictory to a previous study by Kreü S et al. whose research found no deleterious effect of metabolic alkalosis in septic patients, except for prolonged ICU stay.13 The association between metabolic alkalosis and increased mortality is attributed to several underlying factors, such as over-correcting hypotension and shock through aggressive fluid resuscitation, specifically Ringer’s lactate administration and transfusion of citrated blood. These interventions result in alkalinization of the blood, which causes hypoventilation as a physiological response before the kidneys start to excrete excess bicarbonate. Alkalosis is also associated with hypokalemia, which can result in life-threatening arrhythmias.14
We also investigated the association of acid-base disorders with other prognostic markers of sepsis, including base excess, random blood sugars, serum creatinine, and length of stay in the ICU.
Notably, the base excess (BE) - the amount of base/acid needed to restore normal blood pH- serves as a sensitive indicator of acid-base disorder. Unlike pH, which is affected by both respiratory and metabolic factors, BE exclusively reflects acid-base balance.15 Our study found that the patients with severe metabolic acidosis had the lowest base excess among all the groups, although this difference did not reach statistical significance (P > 0.05). This finding contrasts with a previous study conducted by Junfang Qi et al., which reported a significant correlation between BE and pH in poly-trauma patients (P < 0.05). This discrepancy can be largely attributed to the difference in sample size as our study included a small number of patients with metabolic acidosis (n = 71) compared to 495 patients with metabolic acidosis in Junfanq Qi’s research.16
Our study also examined the relationship between blood sugar levels and acid-base imbalance. Notably, the group with severe metabolic acidosis (all non-survivors) exhibited significantly elevated blood sugar levels compared to other participants (228.25 ± 53.13 mg/dL). This finding may be attributed to enhanced metabolism in sepsis, leading to insulin resistance.17 Despite the non-significant result (P > 0.05), our findings underscore the need for further investigation. To the best of our knowledge, there is limited literature exploring the relationship between hyperglycemia and acid-base disequilibrium, and further studies are warranted to establish a potential correlation.
We also observed a trend of shorter ICU stay in patients with severe metabolic acidosis, suggesting early mortality associated with academia. This finding is consistent with a study conducted in India by Sujay Samanta et al.18 which also reported an association between low pH and shorter ICU stay in non-survivors. Although our findings lacked statistical significance, unlike Samanta’s study, it nonetheless supports the notion that severe metabolic acidosis leads to rapid clinical deterioration.
Contrary to our expectations, the mean serum creatinine was unexpectedly lower in all non-survivor groups i.e. severe metabolic acidosis, compared to other groups (except for mild metabolic alkalosis), which exhibited higher mean serum creatinine values. This result implies that deranged renal function did not predict mortality in our study. This observation was not statistically significant (P > 0.05)
5. LIMITATIONS
This study had several limitations. Complete biochemical and metabolic data were not available for the patients included in the study. As a result, the analysis conducted was restricted to acid-base disturbances without additional information regarding anion gap or respiratory acidosis or alkalosis. Furthermore, our patient cohort was followed only for a period of hospital admission, with no follow-up data available after discharge. As a result, we were unable to assess readmission rates and long-term mortality.
Despite these limitations, our study underscores the need for future research to focus on formulating scoring system that integrates pH levels with clinical parameters as an important prognostic indicator in septic patients.
6. CONCLUSION
Acid-base imbalance is quite prevalent in septic patients and has a significant impact on the mortality rate. Severe metabolic acidosis carries 100% mortality in our study compared to only a 20.59% death rate in patients with normal acid-base status.
Serum lactate levels are substantially elevated in patients with severe metabolic acidosis, serving as a critical prognostic marker. Its monitoring should be prioritized in sepsis management.
Acid-base imbalance affects patients of all ages. While base excess, serum creatinine, blood sugar, and length of ICU stay differ among acid-base disorder groups, these variations lack statistical significance. Further studies are warranted to illustrate potential correlations.
Prompt diagnosis and management of acid-base disorders greatly improve outcomes in sepsis patients. Targeted interventions should be developed for early correction of acid-base disequilibrium.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflicts of interest
Authors declare no conflict of interest.
9. Author's contribution
SK: Concept and design of the study, acquisition of data, and analysis
RA: Drafting the paper and result writing
ZA: Revising and approving the article and providing the intellectual concept.
WB: Contributed to writing the manuscript, critically revised the article
10. REFERENCES
- Stephen AH, Montoya RL, Aluisio AR. Sepsis and Septic Shock in Low- and Middle-Income Countries. Surg Infect (Larchmt). 2020;21(7):571-8. ]PubMed] DOI: 1089/sur.2020.047
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063-143. ]PubMed] DOI: 1097/CCM.0000000000005337
- Al-Jaghbeer M, Kellum JA. Acid–base disturbances in intensive care patients: etiology, pathophysiology and treatment. Nephrol Dial Transplant. 2015;30(7):1104-11. ]PubMed] DOI: 1093/ndt/gfu289
- Lakhani JD, Chordiya R, Mota T, Trivedi S, Lakhani SJ. Arterial blood gas analysis in patients of sepsis. Int J Pharm Res. 2020;12:370–8. Full Text DOI: 31838/ijpr/2020.SP1.073
- Gunnerson KJ, Saul M, He S, Kellum JA. Lactate versus non-lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients. Crit Care. 2006;10(1):R22. ]PubMed] DOI: 1186/cc3987
- Sithole N, Lalla U, Davids MR, Chothia MY. The frequency of acid-base disorders on admission to the intensive care and its association with in-hospital outcome, Cape Town, South Africa: a retrospective cohort study. Pan Afr Med J. 2022;42:130. ]PubMed] DOI: 11604/pamj.2022.42.130.32570
- Kilinc Toker A, Kose S, Turken M. Comparison of SOFA Score, SIRS, qSOFA, and qSOFA + L Criteria in the Diagnosis and Prognosis of Sepsis. Eurasian J Med. 2021;53(1):40-7. ]PubMed] DOI: 5152/eurasianjmed.2021.20081
- Czajka S, Ziębińska K, Marczenko K, Posmyk B, Szczepańska AJ, Krzych ŁJ. Validation of APACHE II, APACHE III and SAPS II scores in in-hospital and one year mortality prediction in a mixed intensive care unit in Poland: a cohort study. BMC Anesthesiol. 2020;20(1):296. ]PubMed] DOI: 1186/s12871-020-01203-7
- Liu H, Zhang L, Xu F, Li S, Wang Z, Han D, et al. Establishment of a prognostic model for patients with sepsis based on SOFA: a retrospective cohort study. J Int Med Res. 2021;49(9):03000605211044892. ]PubMed] DOI: 1177/03000605211044892
- Fleischmann C, Scherag A, Adhikari NKJ, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis—current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259-72. ]PubMed] DOI: 1164/rccm.201504-0781OC
- Kamel KS, Oh MS, Halperin ML. L-lactic acidosis: pathophysiology, classification, and causes; emphasis on biochemical and metabolic basis. Kidney Int. 2020;97(1):75-88. ]PubMed] DOI: 1016/j.kint.2019.08.023
- Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Heffner AC, Kline JA, et al. Prognostic value and agreement of achieving lactate clearance or central venous oxygen saturation goals during early sepsis resuscitation. Acad Emerg Med. 2012;19(3):252-8. ]PubMed] DOI: 1111/j.1553-2712.2012.01292.x
- Kreü S, Jazrawi A, Miller J, Baigi A, Chew M. Alkalosis in critically ill patients with severe sepsis and septic shock. PLoS One. 2017;12(1):e0168563. ]PubMed] DOI: 1371/journal.pone.0168563
- Park MA, Freebairn RC. Chapter-25 Metabolic Alkalosis in Critical Care: A Classical and Physicochemical Approach. In: Contemporary Topics in Critical Care Medicine. 2022. p. 131.
- Yuan J, Liu X, Liu Y, Li W, Chen X, Chen Q, et al. Association between base excess and 28-day mortality in sepsis patients: A secondary analysis based on the MIMIC-IV database. Heliyon. 2023;9(5):e15990. ]PubMed] DOI: 1016/j.heliyon.2023.e15990
- Qi J, Bao L, Yang P, Chen D. Comparison of base excess, lactate and pH predicting 72-h mortality of multiple trauma. BMC Emerg Med. 2021;21(1):80. ]PubMed] DOI: 1186/s12873-021-00465-9
- Wasyluk W, Zwolak A. Metabolic alterations in sepsis. J Clin Med. 2021;10(11):2412. ]PubMed] DOI: 3390/jcm10112412
- Samanta S, Singh RK, Baronia AK, Mishra P, Poddar B, Azim A, et al. Early pH Change Predicts Intensive Care Unit Mortality. Indian J Crit Care Med. 2018;22(10):697-705. ]PubMed] DOI: 4103/ijccm.IJCCM_129_18