Khalid A. Alnemer*
Authors’ affiliation:
*Department of internal medicine, College of medicine, Imam Mohammad Ibn Saud Islamic university (IMSIU), Riyadh, Saudi Arabia; Email: Kaalnemer@imamu.edu.sa
Correspondence: Dr. Khalid A. Alnemer; Email: Kaalnemer@imamu.edu.sa
Takotsubo cardiomyopathy (TCM) is a clinical medical condition not linked to obstructive coronary artery disease, marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure.
A 52-year-old woman with a history of generalized anxiety disorder and hypertension arrived at the emergency department after experiencing sudden chest pain and difficulty breathing that began immediately after participating in a 15-minute session of a virtual reality horror game using a headset.
This case highlights a rare and novel trigger of TCM exposure to immersive virtual reality. As virtual reality technologies become increasingly integrated into entertainment and healthcare, clinicians should be aware of their potential to provoke significant physiological stress responses, particularly in individuals with predisposing risk factors.
Abbreviations: ACS: Acute coronary syndrome, CAD: coronary artery disease, STEMI: ST-segment elevation myocardial infarction, TCM: Takotsubo cardiomyopathy, VR: virtual reality
Keywords: coronary artery disease; Heartbroken syndrome; virtual reality; Takotsubo cardiomyopathy
Citation: Alnemer KA. Takotsubo cardiomyopathy triggered by virtual reality exposure in a middle-aged woman: a novel presentation. Anaesth. pain intensive care 2025;29(5):640-645 DOI: 10.35975/apic.v29i5.2935
Received: May 10, 2025; Revised: July 06, 2025; Accepted: July 09, 2025
Takotsubo cardiomyopathy (TCM), also called "broken heart syndrome," "stress-induced cardiomyopathy," and "apical ballooning syndrome," is a clinical medical condition not linked to obstructive coronary artery disease. It is marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure.1,2
The term "takotsubo" refers to a container with a narrow neck and a round bottom used to catch octopuses in Japan, which somewhat corresponds to the TC's heart condition.3,4 There are several types of left ventricular (LV) dysfunction associated with this condition.5 The prevalence is between 1.0 and 2.5%, with the majority of cases occurring in postmenopausal women.6,7
Cardiac conditions are common across patients from different age groups.8,9 Previous literature showed that the prevalence and incidence of TCM significantly coexist with a coronary artery, which deleteriously impacts prognosis. The prevalence of TCM has gradually risen since the first documented case, accounting for 5% up to 6% of ST-segment elevation myocardial infarction (STEMI) cases in women and for 1% up to 3% of all acute coronary syndrome (ACS) cases.10,11 TCM is more prevalent in women, especially after menopause, as 90% of TCM cases are 67 to 70 aged women.5,12,13 TCM is ten times more often in women than in males, and it is five times more likely in women over the age of 55 than in those under 55.14
In 1986, the New England Journal of Medicine published a case study of a patient suffering from acute psychological stress whose psychological condition led to chest pain. Even though the condition has not yet been recognized, this TCM case is assumed to be the first case outside Japan.15 Interest in the syndrome increased significantly in Japan in 2004 after the Niigata Chuetsu earthquake. In the week following the earthquake, the number of newly diagnosed TCM cases was similar to the total TCM cases reported in the earlier decade. Later, the high incidence of TCM in New Zealand was linked to earthquakes.16,17
The specific causes of the disease remain unknown, even though it has been more than 30 years since its discovery. In addition, no randomized controlled trials have evaluated the optimal treatment course for the disease. Hence, TCM continues to be a focus of medical and scientific attention.16
During the acute phase, the immediate massive release of catecholamine from the sympathetic nerve terminals into the myocardium causes myocardial contraction band necrosis and ventricular failure, rendering histological identification of TCM.18,19 Additionally, certain studies have shown that this local catecholamine excess is more cardiotoxic than the circulating catecholamine and disrupts calcium regulation in the myocardium.20,21
While several emotional and physical stressors, such as traumatic life experiences, medical procedures, and acute sickness, have been identified as triggers for TCM, no published cases have tied immersive virtual worlds to the disease's genesis. Recent research has shown that virtual reality (VR) encounters can trigger considerable physiological stress responses, including higher heart rate, cortisol levels, and changes in electrodermal activity, indicating sympathetic nervous system activation. Despite these findings, VR has yet to be published in the medical literature as a triggering factor for TCM. This instance identifies a previously unknown trigger and emphasizes the importance of raising awareness about developing technologies as potential contributors to stress-related cardiac events.22 This article aims to report the first known case of Takotsubo Cardiomyopathy precipitated by virtual reality exposure in a previously healthy middle-aged woman.
A 52-year-old woman with a history of generalized anxiety disorder and hypertension arrived at the emergency department after experiencing sudden chest pain and difficulty breathing that began immediately after participating in a 15-minute session of a VR horror game using a headset. The patient described the game experience as highly immersive and emotionally intense. On examination, she was alert and conscious. Her vital signs were as follows: oxygen saturation 98% on room air, temperature 36.7°C, respiratory rate 20 breaths per minute, blood pressure 158/90 mmHg, and heart rate 102 beats per minute.
Electrocardiography (ECG) revealed ST-segment elevations in leads I, aVL, and V2-V4, with reciprocal ST depression-consistent with acute anterior STEMI (Figure 1). Initial laboratory tests showed elevated cardiac biomarkers: B-type natriuretic peptide (BNP) was 500 pg/mL, and Troponin I was 1.5 ng/mL (reference range <0.04 ng/mL). Liver function tests, renal function, and complete blood count were within normal limits.
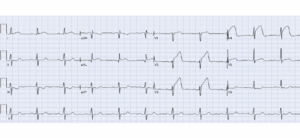
Figure 1: ECG on admission showing ST elevation in leads aVL and V2-V4 with reciprocal changes suggestive of acute anterior STEMI.
Given the concern for acute coronary syndrome, the patient underwent coronary angiography, which indicated that the coronary arteries were normal (Figure 2). Left ventriculography during the cardiac catheterization procedure demonstrates end-systolic akinesis of the mid-anterior and apical area and also the mid and distal inferior walls with clear contractility of basal segments, with depressed LV ejection fraction estimation on left ventriculogram of 40% with apical ballooning consistent with TCM (Figure 3). Transthoracic echocardiography confirmed the same findings on left ventriculography.
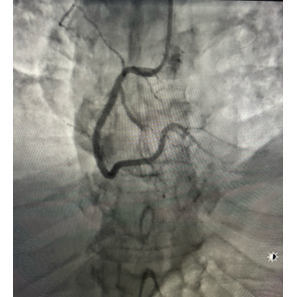
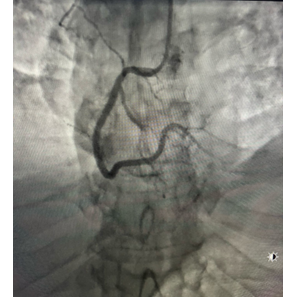
Figure 2-A: ROA cranial view of the left coronary system showing a normal epicardial angiogram. B: LOA view of the right coronary artery demonstrating a normal angiographic appearance.
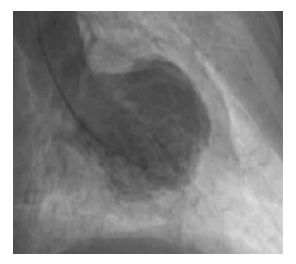
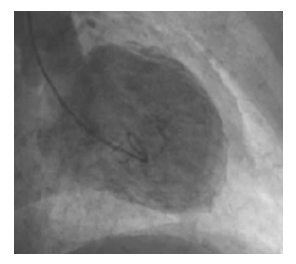
Figure 3: left ventriculogram right anterior oblique image during end systole showing apical ballooning and akinesis of the mid-anterior and apical area and the mid and distal inferior wall.
Management and Outcome
The patient was managed conservatively with low-dose aspirin, angiotensin-converting enzyme (ACE) inhibitors, and beta-blockers. Her anxiety symptoms She experienced no further chest pain and was discharged on hospital day five with a cardiology follow-up scheduled.
She experienced no further chest pain and was discharged on hospital day five with a cardiology follow-up. Her tension and anxiety were addressed through counseling and short-term use of anxiolytics.
Takotsubo cardiomyopathy, also called "broken heart syndrome," "stress-induced cardiomyopathy," and "apical ballooning syndrome," is a clinical medical condition not linked to obstructive coronary artery disease. It is marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure. It predominantly affects postmenopausal women, especially after menopause, and is typically precipitated by intense physical or emotional stressors.13
The pathophysiology of TCM is multifactorial, with catecholamine surge playing a central role. Acute stress activates the sympathetic nervous system, leading to elevated levels of catecholamines such as norepinephrine and epinephrine. These catecholamines can cause direct myocardial toxicity, induce coronary vasospasm, and lead to microvascular dysfunction, culminating in myocardial stunning and the characteristic apical ballooning observed in TCM.23,24
In this case, the patient experienced TCM following exposure to a VR horror game. VR technology, while increasingly utilized in various sectors, has been shown to elicit significant physiological stress responses. A systematic review and meta-analysis demonstrated that VR stress tasks can lead to measurable increases in heart rate, blood pressure, and cortisol levels, indicating activation of the sympathetic nervous system. This indicates activation of the sympathetic nervous system. This suggests that immersive VR experiences can serve as potent emotional stressors capable of triggering TCM in susceptible individuals.22,24
The patient's history of hypertension and anxiety disorder may have heightened her vulnerability to stress-induced cardiac events. Psychiatric conditions, including anxiety and depression, have been associated with an increased risk of TCM, possibly due to heightened sympathetic activity and altered stress responses.
Virtual reality games have exhaustively different features compared to traditional video games (i.e., desktop displays).25,26 Specifically, one of the key discrepancies is immersion level, which is described as a “quantifiable description of a technology, which includes the extent to which the computer displays are extensive, surrounding, inclusive, vivid and matching”.27
The body initiates a physiological stress response after exposure to an environmental stressor. During this response, the immune system, endocrine system, autonomic nervous system, and brain work together to maintain physiological stability and meet the demands of the stressor. These responses occur within the hypothalamus-pituitary-adrenal (HPA) axis, the sympathetic-adrenal-medullary (SAM) axis, and the sympathetic nervous system, as outlined in Selye's General Adaptation Syndrome. The HPA axis stimulates the secretion of glucocorticoids (e.g., cortisol) in the adrenal cortex, and the SAM axis stimulates the secretion of catecholamines in the adrenal medulla (e.g., epinephrine, noradrenaline, and adrenaline).28,29 Finally, the body distributes more energy by modifying the function of the cardiovascular system because of stress hormones.
The study's results included ratings of negative and positive emotions, diastolic and systolic blood pressure, and heart rate variability, which were measured before, during, and after the game. The threat assessment instructions were found to reduce heart rate variability while increasing ratings of negative emotions.30
There are no prospective randomized data on TCM, and treatment is according to expert consensus and clinical experience (level of evidence C). Initial TCM is similar to acute coronary syndrome, so initial treatment includes coronary angiography to exclude obstructive coronary artery disease, and medications include lipid-lowering drugs, ACE inhibitors, beta-blockers, and aspirin.31 Treatment is individualized for each patient based on their hematologic and clinical status. ACE inhibitors and cardio-selective beta-blockers are used for 3 to 6 months if the patient is stable with serial imaging scans to notice ventricular ejection fraction (VEF) and any abnormalities in arterial wall motion to predict improvement or progression.32
Clinically, TCM often presents with elevated cardiac biomarkers, ECG changes, and chest pain, closely resembling ACS. However, the absence of obstructive coronary lesions on angiography and the presence of wall motion abnormalities on echocardiography are distinguishing features. Management is primarily supportive, focusing on hemodynamic stabilization and addressing underlying triggers. Prognosis is generally favorable with most patients experiencing full recovery cardiac function within weeks.1
This case underscores the need for clinicians to recognize nontraditional emotional stressors, such as immersive VR experiences, as potential triggers for TCM. As VR technology becomes more prevalent, awareness of its potential physiological impact is crucial, especially for individuals with predisposing factors. Further research is warranted to explore the relationship between VR-induced stress and cardiovascular events, which may inform guidelines for safe VR use and in at-risk populations.
This case highlights a rare and novel trigger of Takotsubo cardiomyopathy-exposure to immersive VR. As VR technologies become increasingly integrated into entertainment and healthcare, clinicians should be aware of their potential to provoke significant physiological stress responses, particularly in individuals with predisposing risk factors. Early recognition and supportive management remain essential for favorable outcomes in stress-induced cardiomyopathy. Further research is warranted to better understand the cardiovascular implications of immersive digital experiences.
5. Conflict of interest
The author declares that there was no conflict of interest.
6. Ethical considerations
Written informed consent was obtained from the patient to use this report for academic purposes.
7. Authors’ contribution
Dr. Khalid A. Alnemer managed this case and prepared this manuscript as the sole author.
Authors’ affiliation:
*Department of internal medicine, College of medicine, Imam Mohammad Ibn Saud Islamic university (IMSIU), Riyadh, Saudi Arabia; Email: Kaalnemer@imamu.edu.sa
Correspondence: Dr. Khalid A. Alnemer; Email: Kaalnemer@imamu.edu.sa
ABSTRACT
Takotsubo cardiomyopathy (TCM) is a clinical medical condition not linked to obstructive coronary artery disease, marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure.
A 52-year-old woman with a history of generalized anxiety disorder and hypertension arrived at the emergency department after experiencing sudden chest pain and difficulty breathing that began immediately after participating in a 15-minute session of a virtual reality horror game using a headset.
This case highlights a rare and novel trigger of TCM exposure to immersive virtual reality. As virtual reality technologies become increasingly integrated into entertainment and healthcare, clinicians should be aware of their potential to provoke significant physiological stress responses, particularly in individuals with predisposing risk factors.
Abbreviations: ACS: Acute coronary syndrome, CAD: coronary artery disease, STEMI: ST-segment elevation myocardial infarction, TCM: Takotsubo cardiomyopathy, VR: virtual reality
Keywords: coronary artery disease; Heartbroken syndrome; virtual reality; Takotsubo cardiomyopathy
Citation: Alnemer KA. Takotsubo cardiomyopathy triggered by virtual reality exposure in a middle-aged woman: a novel presentation. Anaesth. pain intensive care 2025;29(5):640-645 DOI: 10.35975/apic.v29i5.2935
Received: May 10, 2025; Revised: July 06, 2025; Accepted: July 09, 2025
1. INTRODUCTION
Takotsubo cardiomyopathy (TCM), also called "broken heart syndrome," "stress-induced cardiomyopathy," and "apical ballooning syndrome," is a clinical medical condition not linked to obstructive coronary artery disease. It is marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure.1,2
The term "takotsubo" refers to a container with a narrow neck and a round bottom used to catch octopuses in Japan, which somewhat corresponds to the TC's heart condition.3,4 There are several types of left ventricular (LV) dysfunction associated with this condition.5 The prevalence is between 1.0 and 2.5%, with the majority of cases occurring in postmenopausal women.6,7
Cardiac conditions are common across patients from different age groups.8,9 Previous literature showed that the prevalence and incidence of TCM significantly coexist with a coronary artery, which deleteriously impacts prognosis. The prevalence of TCM has gradually risen since the first documented case, accounting for 5% up to 6% of ST-segment elevation myocardial infarction (STEMI) cases in women and for 1% up to 3% of all acute coronary syndrome (ACS) cases.10,11 TCM is more prevalent in women, especially after menopause, as 90% of TCM cases are 67 to 70 aged women.5,12,13 TCM is ten times more often in women than in males, and it is five times more likely in women over the age of 55 than in those under 55.14
In 1986, the New England Journal of Medicine published a case study of a patient suffering from acute psychological stress whose psychological condition led to chest pain. Even though the condition has not yet been recognized, this TCM case is assumed to be the first case outside Japan.15 Interest in the syndrome increased significantly in Japan in 2004 after the Niigata Chuetsu earthquake. In the week following the earthquake, the number of newly diagnosed TCM cases was similar to the total TCM cases reported in the earlier decade. Later, the high incidence of TCM in New Zealand was linked to earthquakes.16,17
The specific causes of the disease remain unknown, even though it has been more than 30 years since its discovery. In addition, no randomized controlled trials have evaluated the optimal treatment course for the disease. Hence, TCM continues to be a focus of medical and scientific attention.16
During the acute phase, the immediate massive release of catecholamine from the sympathetic nerve terminals into the myocardium causes myocardial contraction band necrosis and ventricular failure, rendering histological identification of TCM.18,19 Additionally, certain studies have shown that this local catecholamine excess is more cardiotoxic than the circulating catecholamine and disrupts calcium regulation in the myocardium.20,21
While several emotional and physical stressors, such as traumatic life experiences, medical procedures, and acute sickness, have been identified as triggers for TCM, no published cases have tied immersive virtual worlds to the disease's genesis. Recent research has shown that virtual reality (VR) encounters can trigger considerable physiological stress responses, including higher heart rate, cortisol levels, and changes in electrodermal activity, indicating sympathetic nervous system activation. Despite these findings, VR has yet to be published in the medical literature as a triggering factor for TCM. This instance identifies a previously unknown trigger and emphasizes the importance of raising awareness about developing technologies as potential contributors to stress-related cardiac events.22 This article aims to report the first known case of Takotsubo Cardiomyopathy precipitated by virtual reality exposure in a previously healthy middle-aged woman.
2. CASE REPORT
A 52-year-old woman with a history of generalized anxiety disorder and hypertension arrived at the emergency department after experiencing sudden chest pain and difficulty breathing that began immediately after participating in a 15-minute session of a VR horror game using a headset. The patient described the game experience as highly immersive and emotionally intense. On examination, she was alert and conscious. Her vital signs were as follows: oxygen saturation 98% on room air, temperature 36.7°C, respiratory rate 20 breaths per minute, blood pressure 158/90 mmHg, and heart rate 102 beats per minute.
Electrocardiography (ECG) revealed ST-segment elevations in leads I, aVL, and V2-V4, with reciprocal ST depression-consistent with acute anterior STEMI (Figure 1). Initial laboratory tests showed elevated cardiac biomarkers: B-type natriuretic peptide (BNP) was 500 pg/mL, and Troponin I was 1.5 ng/mL (reference range <0.04 ng/mL). Liver function tests, renal function, and complete blood count were within normal limits.
Figure 1: ECG on admission showing ST elevation in leads aVL and V2-V4 with reciprocal changes suggestive of acute anterior STEMI.
Given the concern for acute coronary syndrome, the patient underwent coronary angiography, which indicated that the coronary arteries were normal (Figure 2). Left ventriculography during the cardiac catheterization procedure demonstrates end-systolic akinesis of the mid-anterior and apical area and also the mid and distal inferior walls with clear contractility of basal segments, with depressed LV ejection fraction estimation on left ventriculogram of 40% with apical ballooning consistent with TCM (Figure 3). Transthoracic echocardiography confirmed the same findings on left ventriculography.
Figure 2-A: ROA cranial view of the left coronary system showing a normal epicardial angiogram. B: LOA view of the right coronary artery demonstrating a normal angiographic appearance.
Figure 3: left ventriculogram right anterior oblique image during end systole showing apical ballooning and akinesis of the mid-anterior and apical area and the mid and distal inferior wall.
Management and Outcome
The patient was managed conservatively with low-dose aspirin, angiotensin-converting enzyme (ACE) inhibitors, and beta-blockers. Her anxiety symptoms She experienced no further chest pain and was discharged on hospital day five with a cardiology follow-up scheduled.
She experienced no further chest pain and was discharged on hospital day five with a cardiology follow-up. Her tension and anxiety were addressed through counseling and short-term use of anxiolytics.
3. DISCUSSION
Takotsubo cardiomyopathy, also called "broken heart syndrome," "stress-induced cardiomyopathy," and "apical ballooning syndrome," is a clinical medical condition not linked to obstructive coronary artery disease. It is marked by temporary left ventricular wall motion disturbances that lead to reversible, acute heart failure. It predominantly affects postmenopausal women, especially after menopause, and is typically precipitated by intense physical or emotional stressors.13
The pathophysiology of TCM is multifactorial, with catecholamine surge playing a central role. Acute stress activates the sympathetic nervous system, leading to elevated levels of catecholamines such as norepinephrine and epinephrine. These catecholamines can cause direct myocardial toxicity, induce coronary vasospasm, and lead to microvascular dysfunction, culminating in myocardial stunning and the characteristic apical ballooning observed in TCM.23,24
In this case, the patient experienced TCM following exposure to a VR horror game. VR technology, while increasingly utilized in various sectors, has been shown to elicit significant physiological stress responses. A systematic review and meta-analysis demonstrated that VR stress tasks can lead to measurable increases in heart rate, blood pressure, and cortisol levels, indicating activation of the sympathetic nervous system. This indicates activation of the sympathetic nervous system. This suggests that immersive VR experiences can serve as potent emotional stressors capable of triggering TCM in susceptible individuals.22,24
The patient's history of hypertension and anxiety disorder may have heightened her vulnerability to stress-induced cardiac events. Psychiatric conditions, including anxiety and depression, have been associated with an increased risk of TCM, possibly due to heightened sympathetic activity and altered stress responses.
Virtual reality games have exhaustively different features compared to traditional video games (i.e., desktop displays).25,26 Specifically, one of the key discrepancies is immersion level, which is described as a “quantifiable description of a technology, which includes the extent to which the computer displays are extensive, surrounding, inclusive, vivid and matching”.27
The body initiates a physiological stress response after exposure to an environmental stressor. During this response, the immune system, endocrine system, autonomic nervous system, and brain work together to maintain physiological stability and meet the demands of the stressor. These responses occur within the hypothalamus-pituitary-adrenal (HPA) axis, the sympathetic-adrenal-medullary (SAM) axis, and the sympathetic nervous system, as outlined in Selye's General Adaptation Syndrome. The HPA axis stimulates the secretion of glucocorticoids (e.g., cortisol) in the adrenal cortex, and the SAM axis stimulates the secretion of catecholamines in the adrenal medulla (e.g., epinephrine, noradrenaline, and adrenaline).28,29 Finally, the body distributes more energy by modifying the function of the cardiovascular system because of stress hormones.
The study's results included ratings of negative and positive emotions, diastolic and systolic blood pressure, and heart rate variability, which were measured before, during, and after the game. The threat assessment instructions were found to reduce heart rate variability while increasing ratings of negative emotions.30
There are no prospective randomized data on TCM, and treatment is according to expert consensus and clinical experience (level of evidence C). Initial TCM is similar to acute coronary syndrome, so initial treatment includes coronary angiography to exclude obstructive coronary artery disease, and medications include lipid-lowering drugs, ACE inhibitors, beta-blockers, and aspirin.31 Treatment is individualized for each patient based on their hematologic and clinical status. ACE inhibitors and cardio-selective beta-blockers are used for 3 to 6 months if the patient is stable with serial imaging scans to notice ventricular ejection fraction (VEF) and any abnormalities in arterial wall motion to predict improvement or progression.32
Clinically, TCM often presents with elevated cardiac biomarkers, ECG changes, and chest pain, closely resembling ACS. However, the absence of obstructive coronary lesions on angiography and the presence of wall motion abnormalities on echocardiography are distinguishing features. Management is primarily supportive, focusing on hemodynamic stabilization and addressing underlying triggers. Prognosis is generally favorable with most patients experiencing full recovery cardiac function within weeks.1
This case underscores the need for clinicians to recognize nontraditional emotional stressors, such as immersive VR experiences, as potential triggers for TCM. As VR technology becomes more prevalent, awareness of its potential physiological impact is crucial, especially for individuals with predisposing factors. Further research is warranted to explore the relationship between VR-induced stress and cardiovascular events, which may inform guidelines for safe VR use and in at-risk populations.
4. CONCLUSION
This case highlights a rare and novel trigger of Takotsubo cardiomyopathy-exposure to immersive VR. As VR technologies become increasingly integrated into entertainment and healthcare, clinicians should be aware of their potential to provoke significant physiological stress responses, particularly in individuals with predisposing risk factors. Early recognition and supportive management remain essential for favorable outcomes in stress-induced cardiomyopathy. Further research is warranted to better understand the cardiovascular implications of immersive digital experiences.
5. Conflict of interest
The author declares that there was no conflict of interest.
6. Ethical considerations
Written informed consent was obtained from the patient to use this report for academic purposes.
7. Authors’ contribution
Dr. Khalid A. Alnemer managed this case and prepared this manuscript as the sole author.
8. REFERENCES
- Ghadri JR, Wittstein IS, Prasad A, Sharkey S, Dote K, Akashi YJ, et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur Heart J. 2018;39(22):2032-46. PubMed DOI: 1093/eurheartj/ehy076
- Matta A, Delmas C, Campelo-Parada F, Lhermusier T, Bouisset F, Elbaz M, et al. Takotsubo cardiomyopathy. Rev Cardiovasc Med. 2022;23(1):38. PubMed DOI: 31083/j.rcm2301038
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006;27(13):1523-9. PubMed DOI: 1093/eurheartj/ehl032
- Patankar GR, Choi JW, Schussler JM. Reverse takotsubo cardiomyopathy: two case reports and review of the literature. J Med Case Rep. 2013;7:84. PubMed DOI: 1186/1752-1947-7-84
- Roshanzamir S, Showkathali R. Takotsubo cardiomyopathy a short review. Curr Cardiol Rev. 2013;9(3):191-6. PubMed DOI: 2174/1573403x11309030003
- Amin HZ, Amin LZ, Pradipta A. Takotsubo Cardiomyopathy: A Brief Review. J Med Life. 2020;13(1):3-7. PubMed DOI: 25122/jml-2018-0067
- Sharkey SW, Lesser JR, Maron MS, Maron BJ. Why not just call it tako-tsubo cardiomyopathy: a discussion of nomenclature. J Am Coll Cardiol. 2011;57(13):1496-7. PubMed DOI: 1016/j.jacc.2010.11.029
- Hemmo SI, Naser AY, Alwafi H, Mansour MM, Alanazi AFR, Jalal Z, et al. Hospital Admissions Due to Ischemic Heart Diseases and Prescriptions of Cardiovascular Diseases Medications in England and Wales in the Past Two Decades. Int J Environ Res Public Health. 2021;18(13). PubMed DOI: 3390/ijerph18137041
- Naser AY, Al-Shehri H. Admissions Due to Perinatal Respiratory and Cardiovascular Disorders in England. J Multidiscip Healthc. 2023;16:199-207. PubMed DOI: 2147/JMDH.S396406
- Prasad A, Dangas G, Srinivasan M, Yu J, Gersh BJ, Mehran R, et al. Incidence and angiographic characteristics of patients with apical ballooning syndrome (takotsubo/stress cardiomyopathy) in the HORIZONS-AMI trial: an analysis from a multicenter, international study of ST-elevation myocardial infarction. Catheter Cardiovasc Interv. 2014;83(3):343-8. PubMed DOI: 1002/ccd.23441
- Redfors B, Vedad R, Angerås O, Råmunddal T, Petursson P, Haraldsson I, et al. Mortality in takotsubo syndrome is similar to mortality in myocardial infarction - A report from the SWEDEHEART registry. Int J Cardiol. 2015;185:282-9. PubMed DOI: 1016/j.ijcard.2015.03.162
- Schneider B, Athanasiadis A, Stöllberger C, Pistner W, Schwab J, Gottwald U, et al. Gender differences in the manifestation of tako-tsubo cardiomyopathy. Int J Cardiol. 2013;166(3):584-8. PubMed DOI: 1016/j.ijcard.2011.11.027
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med. 2015;373(10):929-38. PubMed DOI: 1056/NEJMoa1406761
- Rozema T, Klein LR. Takotsubo cardiomyopathy: a case report and literature review. Cardiol Young. 2016;26(2):406-9. PubMed DOI: 1017/S1047951115001249
- Akashi YJ, Ishihara M. Takotsubo Syndrome: Insights from Japan. Heart Fail Clin. 2016;12(4):587-95. PubMed DOI: 1016/j.hfc.2016.06.009
- Boyd B, Solh T. Takotsubo cardiomyopathy: Review of broken heart syndrome. JAAPA. 2020;33(3):24-9. PubMed DOI: 1097/01.JAA.0000654368.35241.fc
- Chan C, Elliott J, Troughton R, Frampton C, Smyth D, Crozier I, et al. Acute myocardial infarction and stress cardiomyopathy following the Christchurch earthquakes. PLoS One. 2013;8(7):e68504. PubMed DOI: 1371/journal.pone.0068504
- Kume T, Kawamoto T, Okura H, Toyota E, Neishi Y, Watanabe N, et al. Local release of catecholamines from the hearts of patients with tako-tsubo-like left ventricular dysfunction. Circ J. 2008;72(1):106-8. PubMed DOI: 1253/circj.72.106
- Mizutani K, Shioya A, Hirose Y, Saito R, Yamada S. Serious takotsubo cardiomyopathy: an autopsy case presenting severe irreversible myocardial damage after frequent episodes of recurrence. Diagn Pathol. 2020;15(1):90. PubMed DOI: 1186/s13000-020-01006-x
- Matta AG, Carrié D. Epidemiology, Pathophysiology, Diagnosis, and Principles of Management of Takotsubo Cardiomyopathy: A Review. Med Sci Monit. 2023;29:e939020. PubMed DOI: 12659/MSM.939020
- Nef HM, Möllmann H, Troidl C, Kostin S, Voss S, Hilpert P, et al. Abnormalities in intracellular Ca2+ regulation contribute to the pathomechanism of Tako-Tsubo cardiomyopathy. Eur Heart J. 2009;30(17):2155-64. PubMed DOI: 1093/eurheartj/ehp240
- Dammen LV, Finseth TT, McCurdy BH, Barnett NP, Conrady RA, Leach AG, et al. Evoking stress reactivity in virtual reality: A systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;138:104709. PubMed DOI: 1016/j.neubiorev.2022.104709
- Lyon AR, Bossone E, Schneider B, Sechtem U, Citro R, Underwood SR, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016;18(1):8-27. PubMed DOI: 1002/ejhf.424
- Robinson J, Razak M. Comparing physiological and psychological effects of virtual reality vs. traditional high-intensity interval training in healthy individuals: results from a preliminary pilot randomised controlled trial. Bull Fac Phys Ther. 2025;30. DOI: 1186/s43161-025-00265-3
- Munafo J, Diedrick M, Stoffregen TA. The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp Brain Res. 2017;235(3):889-901. PubMed DOI: 1007/s00221-016-4846-7
- Pallavicini F, Pepe A, Minissi ME. Gaming in Virtual Reality: What Changes in Terms of Usability, Emotional Response and Sense of Presence Compared to Non-Immersive Video Games? Simul Gaming. 2019;50(2):136-59. DOI: 1177/1046878119831420
- Pallavicini F, Pepe A. Virtual Reality Games and the Role of Body Involvement in Enhancing Positive Emotions and Decreasing Anxiety: Within-Subjects Pilot Study. JMIR Serious Games. 2020;8(2):e15635. PubMed DOI: 2196/15635
- Gerra G, Zaimovic A, Mascetti GG, Gardini S, Zambelli U, Timpano M, et al. Neuroendocrine responses to experimentally-induced psychological stress in healthy humans. Psychoneuroendocrinology. 2001;26(1):91-107. PubMed DOI: 1016/s0306-4530(00)00046-9
- Schöder H, Silverman DH, Campisi R, Sayre JW, Phelps ME, Schelbert HR, et al. Regulation of myocardial blood flow response to mental stress in healthy individuals. Am J Physiol Heart Circ Physiol. 2000;278(2):H360-6. PubMed DOI: 1152/ajpheart.2000.278.2.H360
- Porter AM, Goolkasian P. Video Games and Stress: How Stress Appraisals and Game Content Affect Cardiovascular and Emotion Outcomes. Front Psychol. 2019;10:967. PubMed DOI: 3389/fpsyg.2019.00967
- Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001;38(1):11-8. PubMed DOI: 1016/s0735-1097(01)01316-x
- Ahmad SA KN, Ibrahim MA. Takotsubo Cardiomyopathy StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK430798/