Kamala Kan Nur Azza 1 , Mahmud Mahmud 2 , Noor Alia Susianti 3 , Adam Moeljono 4
Authors affiliations:
Coccydynia is defined as pain localized in the coccygeal region, with clinical presentations ranging from mild discomfort to severe, debilitating pain. the most common etiologies are internal or external trauma. management strategies depend on the severity of symptoms and range from conservative therapies—such as analgesics, physical rehabilitation, and psychotherapy—to interventional approaches, including ganglion impar neurolysis. while its use remains controversial, this case report aimed to investigate whether ganglion impar neurolysis is effective in managing chronic recurrent coccydynia in an adolescent patient, so it may offer significant improvements in pain control, quality of life, and reduction in recurrence and socioeconomic burden.
Keywords: Chronic Pain; Coccydynia; Impar Ganglion; Neurolysis; Recurrent
Citation: Azza KKN, Mahmud M, Susianti NA, Moeljono A. Ganglion impar neurolysis for chronic recurrent coccydynia: a case-based evaluation of therapeutic efficacy. Anaesth. pain intensive care 2025;29(6):634-639. DOI: 10.35975/apic.v29i6.2928
Received: May 29, 2025; Revised: July 24, 2024; Accepted: July 26, 2025
Coccydynia, commonly referred to as tailbone pain, is defined as pain localized to the coccygeal region and is typically triggered or exacerbated by sitting. The intensity of pain can range from mild discomfort to severe, debilitating pain, and its impact varies from minor nuisance to significant disruption of daily activities. To date, there is no definitive report regarding the exact prevalence of coccydynia. However, it has been observed that the condition is more prevalent in females and tends to increase with advancing age.1–3
The risk factors for coccydynia are diverse. The most common cause is internal or external trauma. Minor trauma can also result from prolonged or repetitive sitting, particularly on hard, narrow, or otherwise uncomfortable surfaces. Non-traumatic coccydynia may arise from a variety of etiologies, including degenerative joint changes, disc pathology, sacrococcygeal joint hypermobility or hypomobility, infections, and anatomical variations of the coccyx.1,3,4
Management of coccydynia depends on the severity of the pain. Various therapeutic approaches have been employed. Medical management typically involves the use of laxatives and analgesics, such as NSAIDs, and rehabilitative therapy may include warm baths, use of a donut cushion, ergonomic modifications, massage, and intrathecal manipulation. Psychotherapy is also considered a supportive treatment modality. In cases where conservative treatments fail to alleviate the symptoms, invasive and surgical options may be considered, including sacrococcygeal injections, impar ganglion block, radiofrequency thermocoagulation, coccygeoplasty, and partial or complete coccygectomy.5,6
This case report presents a rare instance of recurrent chronic coccydynia, caused by repetitive trauma, occurring in an adolescent male, a demographic in which this condition is uncommon. Lirette et al. (2014) reported that minor repetitive trauma due to prolonged sitting on hard and uncomfortable surfaces may serve as a precipitating factor.7 The efficacy of impar ganglion neurolysis is still questionable in treating recurrent chronic coccydynia. This case report aims to provide insight into an alternative therapeutic option for recurrent chronic coccydynia. Appropriate management can significantly reduce pain, improve the patient’s quality of life, and potentially decrease recurrence rates and the associated socioeconomic burden on patients and their families.
A 16-year-old adolescent presented with complaints of persistent coccygeal pain that had been ongoing for approximately eight months before hospital admission. The pain was described as continuous with a baseline intensity of 4–5 out of 10 on the Numeric Rating Scale (NRS), worsening to 7–8/10 during sitting. Over the course of eight months, the pain progressively intensified, including during rest or when not seated. The patient is a student who commutes to school by riding as a passenger on a motorcycle for approximately 15 kilometers daily. There were no reported symptoms of lower extremity weakness, sensory disturbances, or bowel and bladder dysfunction. The patient also denied any signs of sexual dysfunction.
Eight months before admission, the patient underwent a peri-coccygeal steroid injection, which resulted in significant pain relief and a pain-free period lasting approximately 1.5 months. However, the pain subsequently recurred with the same characteristics as initially reported. The patient was then referred to a pain clinic, where a ganglion impar steroid injection was administered. Post-procedure, the patient was prescribed a combination of Tramadol HCl 37.5 mg with Acetaminophen 325 mg and Diclofenac Sodium 50 mg, taken twice daily for one week. This treatment provided effective analgesia, resulting in a pain-free period of approximately six months. Nevertheless, the pain gradually recurred thereafter. The patient denied any history of tuberculosis, malignancy, or other traumatic events.
On physical examination, the patient reported localized pain in the coccygeal region with an intensity of 7–8 out of 10 on the numeric rating scale. There were no signs of inflammation in the affected area, such as erythema, warmth, or swelling. Neurological examination revealed no motor weakness in the lower extremities, no sensory deficits, and no pathological reflexes. Physiological reflexes were within normal limits, including bulbocavernosus, superficial anal, and cremasteric reflexes. General physical examination revealed no comorbid conditions.
The patient was scheduled to undergo ganglion impar neurolysis using 95% alcohol. The procedural steps were as follows:
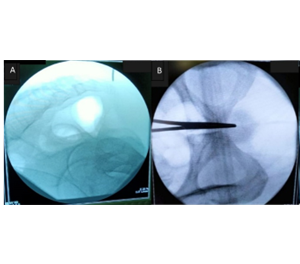
Figure 1 (A): No abnormalities were observed in the coccyx on C-arm X-ray imaging; (B): Anteroposterior view of C-arm X-ray was performed to ensure that the sacral bone was positioned along the midline.
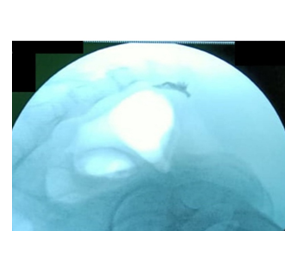
Figure 2: Injection of the contrast medium through Spinocan needle showing the ‘Coma Sign’
During the inpatient observation period, the patient received analgesic therapy consisting of ketorolac 30 mg administered intravenously every 8 hours. Throughout the observation, no signs of inflammation were noted at the intervention site, and no new neurological deficits were identified. The patient was subsequently discharged with oral medications including diclofenac sodium 50 mg twice daily, tramadol 50 mg twice daily, and vitamin B12 at a dose of 100 µg twice daily. At one-week follow-up, the patient reported complete resolution of pain. There were no signs of inflammation at the injection site, and no neurological deficits were observed. The patient was maintained on paracetamol as needed for breakthrough pain. At one-month follow-up, the patient remained pain-free without any neurological complications. The patient was advised to return for further evaluation only in the event of symptom recurrence.
Coccydynia refers to pain experienced by patients in the coccygeal bone (Fogel et al., 2004).5 Similar to this case, the patient reports pain in the coccygeal region. The pain is categorized as chronic, persisting for 8 months. Coccydynia is considered chronic if it lasts for more than 2 months.11
Coccydynia can arise from various causes. According to Lirette et al. (2014), one of the causes of coccydynia is prolonged sitting on hard surfaces.7 In this case, a risk factor identified for the patient is the long and repetitive motorcycle rides to and from school, which may have contributed to the development of coccydynia. There was no history of other trauma, signs of malignancy, or anatomical abnormalities of the coccyx, which were confirmed by X-ray imaging using C-Arm. Imaging studies, such as X-ray and MRI, are utilized to identify structural abnormalities in the coccyx that might lead to coccydynia. Assessments such as measuring the intercoccygeal line when sitting versus standing can help evaluate the hypermobility or hypomobility of the sacrococcygeal joint. Additionally, abnormal mobility of the coccyx can be evaluated by comparing its position while sitting and standing.3
In this case, the patient has undergone various treatments to manage the pain, starting from conservative pharmacological therapies to steroid injection therapy. However, none of these treatments have provided satisfactory relief, and the pain has been worsening. One therapy that could be considered before proceeding to surgical interventions is neurolysis. Although the outcomes of neurolysis remain controversial, several studies have demonstrated its success in treating recurrent chronic coccydynia that does not respond to other treatment modalities.5,6,12
Studies by LoDico & de Leon-Casacola (2014) and Cha et al. (2016) have highlighted the efficacy of ganglion impar neurolysis in cases of coccydynia. LoDico & de Leon-Casacola (2014) evaluated the effectiveness of ganglion impar neurolysis in advanced-stage cancer patients (such as cervical, colon, bladder, rectum, and endometrial cancers) who did not respond to pharmacological therapy or only experienced a 30% reduction in pain. These patients reported perineal pain characterized by a burning sensation and urgency, with referred pain in the rectum, perineum, and vagina. After the injection of neurolytic agents via a transanococcygeal procedure, some patients experienced complete pain remission, while others reported a reduction in pain by 60% to 90%.12,13
Cha et al. (2016) also reported the effectiveness of ganglion impar neurolysis in chronic coccydynia following spinal cyst removal surgery. A 42-year-old female patient experiencing severe coccygeal pain unresponsive to opioid therapy or caudal epidural blocks underwent neurolysis. Although the pain did not completely resolve, the patient reported significant pain relief, enabling her to resume daily activities and improving her quality of life.12
Similarly, in the present case, the chronic mechanical trauma resulting in recurrent coccydynia did not respond to conventional pharmacological therapy and only showed temporary improvement with pericoccygeal steroid injections. Consequently, neurolysis was performed to address the pain. Post-procedure, the patient's pain response was significantly improved, with complete pain relief reported. At a 1-month follow-up, the patient remained pain-free, demonstrating the efficacy of neurolysis in managing chronic recurrent coccydynia.
The selection of neurolytic agents plays a crucial role in the success of the therapy. Phenol is a chemical substance consisting of carbolic acid, phenic acid, phenol hydroxide, hydroxybenzene, and oxybenzene. It is available in a sterile form and can achieve a maximum concentration of 6.7% in an aqueous solution. Phenol is highly soluble in organic solvents, such as alcohol and glycerol. The addition of glycerol and radiopaque contrast can enhance the concentration up to 15%. The solution can be diluted with saline and mixed with radiocontrast agents to facilitate fluoroscopic guidance during injection and to monitor the spread of the solution. When combined with glycerol, phenol diffuses slowly, which is beneficial for intrathecal injection, as the distribution is limited and localized to the area targeted for destruction.14–18
However, phenol has limitations compared to alcohol. Phenol causes nerve destruction by inducing protein precipitation, leading to the loss of cellular lipid elements, the release of myelin sheaths from axons, and axonal edema. While phenol is less effective than alcohol in damaging cell bodies and producing a strong nerve block, its effects are generally more short-lived than those of alcohol. The nerve-blocking capability of phenol primarily affects small blood vessels.14,16
In contrast, alcohol (ethyl alcohol) induces similar destructive effects as phenol but is more efficient in damaging nerve cell bodies. Previous studies have reported satisfactory analgesic effects from 33.3% alcohol injections in pain conditions. Alcohol solutions are commonly available as 95% ethanol. The mechanism of destruction by alcohol is similar to phenol, as it damages the phospholipid membrane, cholesterol, and cerebrosides of nerve tissue, precipitating mucoproteins and lipoproteins. Although alcohol concentrations ranging from 50% to 100% have been used as a neurolytic agent, the minimum concentration required for effective neurolysis remains undetermined. Local anesthetics are often used as diluents. Post-injection, patients often experience a burning sensation along the nerve distribution, which typically lasts for a few minutes and is followed by a feeling of warmth or numbness. This reaction should be evaluated after neurolysis with alcohol.14,16,18,19
However, it is important to note that neurolysis therapy requires further investigation to determine its effectiveness in treating coccydynia. In a report by Hariyanto et al. (2014), a patient with chronic coccydynia involving facet joints did not respond to ganglion impar neurolysis using 95% alcohol, 0.25% bupivacaine, and triamcinolone.20 A systematic review by Sahu et al. (2020) indicated that, in one study, ganglion impar neurolysis led to complete symptom improvement in three patients, partial improvement in three patients, and no improvement in two patients after six months of evaluation.21
It is crucial to recognize that pain in coccydynia varies depending on its etiology. Moreover, pain is a subjective experience, making it challenging to assess objectively. Therefore, the clinician's expertise and experience are essential factors influencing the success or failure of the procedure.13,22
Ganglion impar neurolysis is considered a safe procedure, with no reported complications directly related to the technique. However, there is a risk of damage to surrounding structures if the procedure is performed inaccurately. This risk can be minimized with proper clinical skill and expertise. Rare complications of ganglion impar neurolysis include local infection, bleeding, rectal perforation, periosteal injection, epidural injection, and autonomic or motor dysfunction.23–25 In this case, the follow-up for potential side effects was conducted for one month after the procedure, and no complications were reported.
If the patient experiences recurring pain in the future, radiofrequency ablation of the ganglion impar will be considered, as per the pain management algorithm for coccydynia. Radiofrequency ablation involves the application of electrical current to induce thermocoagulation and nerve damage. This procedure is used as a last resort after exhausting other pain management modalities and before considering invasive surgical options. Radiofrequency ablation is expected to provide relief in cases of coccydynia that do not respond to neurolysis.26–28
It is worth noting that the follow-up for this case was only conducted over a short period of one month. Further research involving larger sample sizes and extended follow-up durations is necessary to assess the long-term effectiveness of neurolysis in managing chronic coccydynia, particularly in cases that do not respond to other conservative treatments. Additionally, rehabilitation therapy and avoidance of risk factors are essential to prevent recurrence of pain.
Impar ganglion neurolysis has been demonstrated to be effective in managing pain associated with recurrent chronic coccydynia. This intervention may serve as an alternative treatment option, potentially improving patients’ quality of life and reducing the socioeconomic burden.
5. Acknowledgement
The author would like to express gratitude to the Department of Anesthesiology and Intensive Care Faculty of Medicine, Public Health, and Nursing of UGM and Academic Hospital Universitas Gadjah Mada as well as the patient and the patient’s family, for their support in this research
6. Conflict of Interest
The authors declare no conflicts of interest.
7. Ethical considerations
Written consent was obtained from the family to publish this case report in the academic interest.
This case report has been structured in accordance with the CARE (Case Report) guidelines.8–10
8. Author contribution
All authors took part in the conduct of this case, the literature search, and the preparation of this manuscript.
Authors affiliations:
- Kamala Kan Nur Azza, Anesthesiology & Intensive Care Department, Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Academic Hospital Universitas Gadjah Mada, Yogyakarta, Indonesia; Email: kamalakan99@gmail.com; {ORCID: 0009-0006-1033-5949}
- Mahmud Mahmud, Anesthesiology & Intensive Care Department, Faculty of Medicine, Public Health, and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia; Email: mahmudanestesi@ugm.ac.id; {ORCID: 0000-0002-7224-2637}
- Noor Alia Susianti, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia, Jl. Farmako, Sekip Utara, Kec. Depok, Kabupaten Sleman, Daerah Istimewa Yogyakarta 55281. Email: nooralia@mail.ugm.ac.id; {ORCID: 0000-0001-8674-7786}
- Adam Moeljono, Orthopedic & Traumatology Department, Faculty of Medicine, Public Health and Nursing, Academic Hospital Universitas Gadjah Mada, Yogyakarta, Indonesia; Email: adam_moeljono@ugm.ac.id; {ORCID: 0009-0008-0029-6696}
ABSTRACT
Coccydynia is defined as pain localized in the coccygeal region, with clinical presentations ranging from mild discomfort to severe, debilitating pain. the most common etiologies are internal or external trauma. management strategies depend on the severity of symptoms and range from conservative therapies—such as analgesics, physical rehabilitation, and psychotherapy—to interventional approaches, including ganglion impar neurolysis. while its use remains controversial, this case report aimed to investigate whether ganglion impar neurolysis is effective in managing chronic recurrent coccydynia in an adolescent patient, so it may offer significant improvements in pain control, quality of life, and reduction in recurrence and socioeconomic burden.
Keywords: Chronic Pain; Coccydynia; Impar Ganglion; Neurolysis; Recurrent
Citation: Azza KKN, Mahmud M, Susianti NA, Moeljono A. Ganglion impar neurolysis for chronic recurrent coccydynia: a case-based evaluation of therapeutic efficacy. Anaesth. pain intensive care 2025;29(6):634-639. DOI: 10.35975/apic.v29i6.2928
Received: May 29, 2025; Revised: July 24, 2024; Accepted: July 26, 2025
1. INTRODUCTION
Coccydynia, commonly referred to as tailbone pain, is defined as pain localized to the coccygeal region and is typically triggered or exacerbated by sitting. The intensity of pain can range from mild discomfort to severe, debilitating pain, and its impact varies from minor nuisance to significant disruption of daily activities. To date, there is no definitive report regarding the exact prevalence of coccydynia. However, it has been observed that the condition is more prevalent in females and tends to increase with advancing age.1–3
The risk factors for coccydynia are diverse. The most common cause is internal or external trauma. Minor trauma can also result from prolonged or repetitive sitting, particularly on hard, narrow, or otherwise uncomfortable surfaces. Non-traumatic coccydynia may arise from a variety of etiologies, including degenerative joint changes, disc pathology, sacrococcygeal joint hypermobility or hypomobility, infections, and anatomical variations of the coccyx.1,3,4
Management of coccydynia depends on the severity of the pain. Various therapeutic approaches have been employed. Medical management typically involves the use of laxatives and analgesics, such as NSAIDs, and rehabilitative therapy may include warm baths, use of a donut cushion, ergonomic modifications, massage, and intrathecal manipulation. Psychotherapy is also considered a supportive treatment modality. In cases where conservative treatments fail to alleviate the symptoms, invasive and surgical options may be considered, including sacrococcygeal injections, impar ganglion block, radiofrequency thermocoagulation, coccygeoplasty, and partial or complete coccygectomy.5,6
This case report presents a rare instance of recurrent chronic coccydynia, caused by repetitive trauma, occurring in an adolescent male, a demographic in which this condition is uncommon. Lirette et al. (2014) reported that minor repetitive trauma due to prolonged sitting on hard and uncomfortable surfaces may serve as a precipitating factor.7 The efficacy of impar ganglion neurolysis is still questionable in treating recurrent chronic coccydynia. This case report aims to provide insight into an alternative therapeutic option for recurrent chronic coccydynia. Appropriate management can significantly reduce pain, improve the patient’s quality of life, and potentially decrease recurrence rates and the associated socioeconomic burden on patients and their families.
2. CASE REPORT
A 16-year-old adolescent presented with complaints of persistent coccygeal pain that had been ongoing for approximately eight months before hospital admission. The pain was described as continuous with a baseline intensity of 4–5 out of 10 on the Numeric Rating Scale (NRS), worsening to 7–8/10 during sitting. Over the course of eight months, the pain progressively intensified, including during rest or when not seated. The patient is a student who commutes to school by riding as a passenger on a motorcycle for approximately 15 kilometers daily. There were no reported symptoms of lower extremity weakness, sensory disturbances, or bowel and bladder dysfunction. The patient also denied any signs of sexual dysfunction.
Eight months before admission, the patient underwent a peri-coccygeal steroid injection, which resulted in significant pain relief and a pain-free period lasting approximately 1.5 months. However, the pain subsequently recurred with the same characteristics as initially reported. The patient was then referred to a pain clinic, where a ganglion impar steroid injection was administered. Post-procedure, the patient was prescribed a combination of Tramadol HCl 37.5 mg with Acetaminophen 325 mg and Diclofenac Sodium 50 mg, taken twice daily for one week. This treatment provided effective analgesia, resulting in a pain-free period of approximately six months. Nevertheless, the pain gradually recurred thereafter. The patient denied any history of tuberculosis, malignancy, or other traumatic events.
On physical examination, the patient reported localized pain in the coccygeal region with an intensity of 7–8 out of 10 on the numeric rating scale. There were no signs of inflammation in the affected area, such as erythema, warmth, or swelling. Neurological examination revealed no motor weakness in the lower extremities, no sensory deficits, and no pathological reflexes. Physiological reflexes were within normal limits, including bulbocavernosus, superficial anal, and cremasteric reflexes. General physical examination revealed no comorbid conditions.
The patient was scheduled to undergo ganglion impar neurolysis using 95% alcohol. The procedural steps were as follows:
- The patient was positioned in the prone position, and standard monitoring devices were applied to continuously monitor hemodynamic parameters throughout the procedure. The procedural area was prepared using aseptic techniques, and a sterile drape was applied.
- A radiologic technologist positioned the C-arm X-ray fluoroscopy unit, with the X-ray generator placed inferiorly and the image intensifier superiorly, to guide the procedure. No anatomical abnormalities of the coccygeal bone were identified on fluoroscopic imaging, ensuring it was centrally aligned both horizontally and vertically.
- The sacrum was identified in the anteroposterior (AP) (Figure 1A) and lateral (Figure 1B) view under fluoroscopy, ensuring it was centrally aligned both horizontally and vertically.
- A skin marker was placed over the sacrococcygeal junction. Local infiltration anesthesia was administered using 1% lidocaine.
- A Spinocan needle was inserted through the sacrococcygeal ligament Once the needle tip reached just below the sacrococcygeal joint, 1 mL of iohexol contrast agent was injected
- Lateral fluoroscopic imaging was used to confirm the presence of the characteristic "coma sign" and to ensure that the needle tip was positioned correctly above the ganglion impar (Figure 2).
- An additional 2 mL of 2% lidocaine was administered through the needle, and a two-minute waiting period was observed to allow the anesthetic effect to take place.
- Subsequently, 5 mL of 95% alcohol mixed with a contrast agent was injected. The persistence of the "coma sign" confirmed that the contrast-stained alcohol remained confined to the target area without extravasation.
- The Spinocan needle was then withdrawn, and the puncture site was covered with a sterile dressing. The patient was monitored for one hour in the recovery room to evaluate hemodynamic stability, pain level, and any potential complications. If the patient remained pain-free, hemodynamically stable, and without any complaints, they were transferred to the ward for 24-hour observation.
Figure 1 (A): No abnormalities were observed in the coccyx on C-arm X-ray imaging; (B): Anteroposterior view of C-arm X-ray was performed to ensure that the sacral bone was positioned along the midline.
Figure 2: Injection of the contrast medium through Spinocan needle showing the ‘Coma Sign’
During the inpatient observation period, the patient received analgesic therapy consisting of ketorolac 30 mg administered intravenously every 8 hours. Throughout the observation, no signs of inflammation were noted at the intervention site, and no new neurological deficits were identified. The patient was subsequently discharged with oral medications including diclofenac sodium 50 mg twice daily, tramadol 50 mg twice daily, and vitamin B12 at a dose of 100 µg twice daily. At one-week follow-up, the patient reported complete resolution of pain. There were no signs of inflammation at the injection site, and no neurological deficits were observed. The patient was maintained on paracetamol as needed for breakthrough pain. At one-month follow-up, the patient remained pain-free without any neurological complications. The patient was advised to return for further evaluation only in the event of symptom recurrence.
3. DISCUSSION
Coccydynia refers to pain experienced by patients in the coccygeal bone (Fogel et al., 2004).5 Similar to this case, the patient reports pain in the coccygeal region. The pain is categorized as chronic, persisting for 8 months. Coccydynia is considered chronic if it lasts for more than 2 months.11
Coccydynia can arise from various causes. According to Lirette et al. (2014), one of the causes of coccydynia is prolonged sitting on hard surfaces.7 In this case, a risk factor identified for the patient is the long and repetitive motorcycle rides to and from school, which may have contributed to the development of coccydynia. There was no history of other trauma, signs of malignancy, or anatomical abnormalities of the coccyx, which were confirmed by X-ray imaging using C-Arm. Imaging studies, such as X-ray and MRI, are utilized to identify structural abnormalities in the coccyx that might lead to coccydynia. Assessments such as measuring the intercoccygeal line when sitting versus standing can help evaluate the hypermobility or hypomobility of the sacrococcygeal joint. Additionally, abnormal mobility of the coccyx can be evaluated by comparing its position while sitting and standing.3
In this case, the patient has undergone various treatments to manage the pain, starting from conservative pharmacological therapies to steroid injection therapy. However, none of these treatments have provided satisfactory relief, and the pain has been worsening. One therapy that could be considered before proceeding to surgical interventions is neurolysis. Although the outcomes of neurolysis remain controversial, several studies have demonstrated its success in treating recurrent chronic coccydynia that does not respond to other treatment modalities.5,6,12
Studies by LoDico & de Leon-Casacola (2014) and Cha et al. (2016) have highlighted the efficacy of ganglion impar neurolysis in cases of coccydynia. LoDico & de Leon-Casacola (2014) evaluated the effectiveness of ganglion impar neurolysis in advanced-stage cancer patients (such as cervical, colon, bladder, rectum, and endometrial cancers) who did not respond to pharmacological therapy or only experienced a 30% reduction in pain. These patients reported perineal pain characterized by a burning sensation and urgency, with referred pain in the rectum, perineum, and vagina. After the injection of neurolytic agents via a transanococcygeal procedure, some patients experienced complete pain remission, while others reported a reduction in pain by 60% to 90%.12,13
Cha et al. (2016) also reported the effectiveness of ganglion impar neurolysis in chronic coccydynia following spinal cyst removal surgery. A 42-year-old female patient experiencing severe coccygeal pain unresponsive to opioid therapy or caudal epidural blocks underwent neurolysis. Although the pain did not completely resolve, the patient reported significant pain relief, enabling her to resume daily activities and improving her quality of life.12
Similarly, in the present case, the chronic mechanical trauma resulting in recurrent coccydynia did not respond to conventional pharmacological therapy and only showed temporary improvement with pericoccygeal steroid injections. Consequently, neurolysis was performed to address the pain. Post-procedure, the patient's pain response was significantly improved, with complete pain relief reported. At a 1-month follow-up, the patient remained pain-free, demonstrating the efficacy of neurolysis in managing chronic recurrent coccydynia.
The selection of neurolytic agents plays a crucial role in the success of the therapy. Phenol is a chemical substance consisting of carbolic acid, phenic acid, phenol hydroxide, hydroxybenzene, and oxybenzene. It is available in a sterile form and can achieve a maximum concentration of 6.7% in an aqueous solution. Phenol is highly soluble in organic solvents, such as alcohol and glycerol. The addition of glycerol and radiopaque contrast can enhance the concentration up to 15%. The solution can be diluted with saline and mixed with radiocontrast agents to facilitate fluoroscopic guidance during injection and to monitor the spread of the solution. When combined with glycerol, phenol diffuses slowly, which is beneficial for intrathecal injection, as the distribution is limited and localized to the area targeted for destruction.14–18
However, phenol has limitations compared to alcohol. Phenol causes nerve destruction by inducing protein precipitation, leading to the loss of cellular lipid elements, the release of myelin sheaths from axons, and axonal edema. While phenol is less effective than alcohol in damaging cell bodies and producing a strong nerve block, its effects are generally more short-lived than those of alcohol. The nerve-blocking capability of phenol primarily affects small blood vessels.14,16
In contrast, alcohol (ethyl alcohol) induces similar destructive effects as phenol but is more efficient in damaging nerve cell bodies. Previous studies have reported satisfactory analgesic effects from 33.3% alcohol injections in pain conditions. Alcohol solutions are commonly available as 95% ethanol. The mechanism of destruction by alcohol is similar to phenol, as it damages the phospholipid membrane, cholesterol, and cerebrosides of nerve tissue, precipitating mucoproteins and lipoproteins. Although alcohol concentrations ranging from 50% to 100% have been used as a neurolytic agent, the minimum concentration required for effective neurolysis remains undetermined. Local anesthetics are often used as diluents. Post-injection, patients often experience a burning sensation along the nerve distribution, which typically lasts for a few minutes and is followed by a feeling of warmth or numbness. This reaction should be evaluated after neurolysis with alcohol.14,16,18,19
However, it is important to note that neurolysis therapy requires further investigation to determine its effectiveness in treating coccydynia. In a report by Hariyanto et al. (2014), a patient with chronic coccydynia involving facet joints did not respond to ganglion impar neurolysis using 95% alcohol, 0.25% bupivacaine, and triamcinolone.20 A systematic review by Sahu et al. (2020) indicated that, in one study, ganglion impar neurolysis led to complete symptom improvement in three patients, partial improvement in three patients, and no improvement in two patients after six months of evaluation.21
It is crucial to recognize that pain in coccydynia varies depending on its etiology. Moreover, pain is a subjective experience, making it challenging to assess objectively. Therefore, the clinician's expertise and experience are essential factors influencing the success or failure of the procedure.13,22
Ganglion impar neurolysis is considered a safe procedure, with no reported complications directly related to the technique. However, there is a risk of damage to surrounding structures if the procedure is performed inaccurately. This risk can be minimized with proper clinical skill and expertise. Rare complications of ganglion impar neurolysis include local infection, bleeding, rectal perforation, periosteal injection, epidural injection, and autonomic or motor dysfunction.23–25 In this case, the follow-up for potential side effects was conducted for one month after the procedure, and no complications were reported.
If the patient experiences recurring pain in the future, radiofrequency ablation of the ganglion impar will be considered, as per the pain management algorithm for coccydynia. Radiofrequency ablation involves the application of electrical current to induce thermocoagulation and nerve damage. This procedure is used as a last resort after exhausting other pain management modalities and before considering invasive surgical options. Radiofrequency ablation is expected to provide relief in cases of coccydynia that do not respond to neurolysis.26–28
It is worth noting that the follow-up for this case was only conducted over a short period of one month. Further research involving larger sample sizes and extended follow-up durations is necessary to assess the long-term effectiveness of neurolysis in managing chronic coccydynia, particularly in cases that do not respond to other conservative treatments. Additionally, rehabilitation therapy and avoidance of risk factors are essential to prevent recurrence of pain.
4. CONCLUSION
Impar ganglion neurolysis has been demonstrated to be effective in managing pain associated with recurrent chronic coccydynia. This intervention may serve as an alternative treatment option, potentially improving patients’ quality of life and reducing the socioeconomic burden.
5. Acknowledgement
The author would like to express gratitude to the Department of Anesthesiology and Intensive Care Faculty of Medicine, Public Health, and Nursing of UGM and Academic Hospital Universitas Gadjah Mada as well as the patient and the patient’s family, for their support in this research
6. Conflict of Interest
The authors declare no conflicts of interest.
7. Ethical considerations
Written consent was obtained from the family to publish this case report in the academic interest.
This case report has been structured in accordance with the CARE (Case Report) guidelines.8–10
8. Author contribution
All authors took part in the conduct of this case, the literature search, and the preparation of this manuscript.
9. REFERENCES
- Garg B, Ahuja K. Coccydynia-A comprehensive review on etiology, radiological features and management options. J Clin Orthop Trauma. 2021;12(1):123-9. [PubMed] DOI: 1016/j.jcot.2020.09.025
- Arif A, Sardar S, Farah Gilani M, Muneer R, Naz A, Manzoor N, et al. Prevalence of Coccydynia Among Postpartum Women. Pak J Health Sci. 2022;:108-12. DOI: 54393/pjhs.v3i07.418
- Dave B, Bang P, Degulmadi D, Samel P, Shah D, Krishnan A. A clinical and radiological study of nontraumatic coccygodynia in Indian population. Indian Spine J. 2019;2(2):128. DOI: 4103/isj.isj_15_18
- Junaid Meer M, Muhammad Atif M, Afzal F, Aslam I, Khurshid A, Zulfiqar H, et al. Causes and Risk Factors of Coccydynia in Postpartum Women in Dhq Sargodha. J Pharm Res Int. 2022;34:8-14. DOI: 9734/jpri/2022/v34i31B36090
- Gufeld L, Vossen JA, Urquia D. Coccydynia: Diagnostic and Management Guidance. J Nurse Pract. 2020;16(10):735-43. DOI: 1016/j.nurpra.2020.08.008
- Swain BP, Vidhya S, Kumar S. Ganglion Impar Block: A Magic Bullet to Fix Idiopathic Coccygodynia. Cureus. 2023;15(1):e33911. [PubMed] DOI: 7759/cureus.33911
- Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: An overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner J. 2014;14(1):84-7. [PubMed]
- Heart Views. Guidelines To Writing A Clinical Case Report. Heart Views. 2017;18(3):104-5. [PubMed] DOI: 4103/1995-705X.217857
- Rison RA. How to write a neurology case report. J Med Case Rep. 2016;10(1):91. [PubMed] DOI: 1186/s13256-016-0867-x
- Riley DS, Barber MS, Kienle GS, Aronson JK, von Schoen-Angerer T, Tugwell P, et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017;89:218-35. [PubMed] DOI: 1016/j.jclinepi.2017.04.026
- Kalstad AM, Knobloch RG, Finsen V. The treatment of coccydynia in adolescents A case-COntrol study. Bone Jt Open. 2020;1(5):115-20. [PubMed] DOI: 1302/2633-1462.15.BJO-2020-0017
- Cha YD, Yang CW, Han JU, Song JH, Na W, Oh S, et al. Transsacrococcygeal approach to ganglion impar block for treatment of chronic coccygodynia after spinal arachnoid cyst removal A case report. Medicine. 2016;95(39):e4980. [PubMed] DOI: 1097/MD.0000000000005010
- LoDico MJP, de Leon-Casasola O. Neurolysis of the Sympathetic Axis for Cancer Pain Management. In: Benzon HT, Wu CL, Rathmell JP, Turk DC, Huley RW, editors. Practical Management of Pain. 5th ed. Elsevier; 2014. p. 794-801. Available from: https://www.sciencedirect.com/book/9780323083409/practical-management-of-pain#book-description
- Rowe DS. Neurolytic Techniques For Pain Management. Coccyx. 1998. Full Text
- Turchan A, Fahmi A, Subianto H. Impar ganglion block with combination of neurolysis drugs and radiofrequency thermocoagulation for perineal pain. Asian J Neurosurg. 2018;13(3):838-41. [PubMed] DOI: 4103/ajns.AJNS_306_16
- Gupta M, Abdallah RT, Abd-Elsayed A, Chakravarthy K, Day M, Deer T, et al. A Review of Nonsurgical Neurolytic Procedures for Neuropathic Pain. J Pain Res. 2025;18:879-95. [PubMed] DOI: 2147/JPR.S491330
- Wu R, Majdalany BS, Lilly M, Prologo JD, Kokabi N. Agents Used for Nerve Blocks and Neurolysis. Semin Intervent Radiol. 2022;39(4):387-93. [PubMed] DOI: 1055/s-0042-1757315
- Goyal S, Kumar A, Goyal D, Attar P, Bhandari B, Purohit G, et al. Efficacy of splanchnic nerve neurolysis in the management of upper abdominal cancer pain: A systematic review and meta‑analysis. Indian J Anaesth. 2023;67(12):1036-45. [PubMed] DOI: 4103/ija.ija_439_23
- Koyyalagunta D, Engle MP, Yu J, Feng L, Novy DM. The effectiveness of alcohol versus phenol based splanchnic nerve neurolysis for the treatment of intra-abdominal cancer pain. Pain Physician. 2016;19(4):281-92. [PubMed]
- Hariyanto H, Yahya CQ, Tantra AH. Chronic Coccydynia with Facet Joint Involvement. Anest Crit Care. 2014;32(3):9-12. Full Text
- Sahu SK, Samal S, Dash A. Effectiveness of Ganglion Impar Block for the Management of Chronic Refractory Coccygodynia. 2020;29(8):2612-7.
- Batista JD, Pereira GS, Batista JD, Silva LD. Efficacy and Clinical Applicability of Impar Ganglion Block in the Treatment of Pudendal Neuralgia : A Systematic Review. Surg Tech Dev. 2025;14(2). DOI: 3390/std14020014
- Ferreira F, Pedro A. Ganglion Impar Neurolysis in the Management of Pelvic and Perineal Cancer-Related Pain. Case Rep Oncol. 2020;13(1):29-34. [PubMed] DOI: 1159/000505181
- Asmaranto, Susila D. Ganglion Impar Block and Neurolysis for Perineal Pain in Anal Adenocarcinoma: A Case Report. Pharmacogn J. 2024;16(3):711-5. DOI: 5530/pj.2024.16.120
- Okçu M, Şencan S, Gündüz OH. Rare complication of ganglion impar blockade with the transsacrococcygeal approach: A case of rectal perforation. Turk J Phys Med Rehabil. 2023;69(1):121-4. [PubMed] DOI: 5606/tftrd.2022.8874
- Patijn J, Marcus J, Hayek S, Mekhail N, Van Zundert J, Van Kleef M. Coccygodynia. In: Evidence-Based Interventional Pain Medicine According to Clinical Diagnoses. Wiley-Blackwell; 2012. p. 103-6.
- Chen Y, Huang-Lionnet JHY, Cohen SP. Radiofrequency ablation in Coccydynia: A case series and comprehensive, evidence-based review. Pain Med. 2017;18(6):1111-30. [PubMed] DOI: 1093/pm/pnw268
- Can E, Yildiz G, Akkaya ÖT, Perdecioğlu GRG, Yürük D. Ultrasound-Guided Coccygeal Nerve Radiofrequency Ablation and Steroid Injection: Combination Therapy for Coccydynia. J Ultrasound Med. 2024;43(1):57-64. [PubMed] DOI: 1002/jum.16334