Ali Najih Al-Awwady*
*Department of Surgery, College of Medicine, Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf, Iraq
Correspondence: Ali Najih Al-Awwadyl, Email: ali.alawwady@jmu.edu.iq
Background: Postoperative pain following lumbar laminectomy is experienced by almost all patients and may necessitate opioid use. Gabapentin is an anticonvulsant drug shown to be efficient in managing reflex sympathetic dystrophy, neuropathy associated with diabetes, post-herpetic neuralgia, and neuropathic pain. This study aimed to assess the efficacy of pre-emptive administration of gabapentin 300 mg orally for reducing postoperative pain after lumbar laminectomy.
Methodology: A randomized clinical trial was carried out on 50 patients, selected with a convenience sampling method, from July 2023 to October 2024, at Al-Sader Teaching Hospital. All patients were randomly assigned to two groups: a control group received a placebo capsule, and the study group received 300 mg of oral gabapentin 2 hours before skin incision. Postoperative analgesic outcomes were assessed over 24 hours, including total paracetamol consumption and pain intensity measured using the Visual Analogue Scale (VAS). Additionally, hemodynamic parameters were evaluated at baseline (prior to anesthesia) and 15 min after induction.
Result: During the first 24 hours postoperatively, total paracetamol consumption was higher in the control group (640.0 ± 757.18 mg) compared to the gabapentin group (200.0 ± 500.0 mg), (P < 0.05). The number of patients who requested paracetamol was higher in the control group compared to the Group G. The VAS scores during recovery, then at 2, 4, 12, and 24 hr postoperatively, were significantly lower in the Group G compared to the control group (P < 0.05). Mean arterial blood pressure and oxygen saturation were comparable in both groups before induction (baseline) and at 15 min after induction, and the differences were not statistically significant (P > 0.05). Heart rate was significantly different between groups at baseline, but there was no statistically significant difference 15 min after induction.
Conclusion: Gabapentin 300 mg orally as pre-emptive analgesia decreases postoperative pain and reduces the need for paracetamol consumption after lumbar laminectomy.
Abbreviations: BMI: Basal metabolic index, DOA: duration of anesthesia, DOS: duration of surgery, VAS: Visual Analogue Scale
Keywords: Analgesia; Gabapentin; lumbar laminectomy; pain; VAS score
Citation: Al-Awwady AN. Efficacy of preemptive oral gabapentin for postoperative pain control following lumbar laminectomy. Anaesth. pain intensive care 2025;29(6):463-68. DOI: 10.35975/apic.v29i6.2888
Postoperative pain following lumbar laminectomy is experienced in all patients and may even necessitate opioid use. As a result, the popularity of multimodal analgesic approaches, which involve various drugs acting on different analgesic mechanisms, have increased,1 and because of the many mechanisms underlying the cause of postoperative pain, a multimodal analgesia plan that combines opioid and non-opioid analgesic drugs can be used to improve the effectiveness of analgesia and reduce their adverse effects.2
Gabapentin is an anticonvulsant drug shown to be efficient in managing reflex sympathetic dystrophy, neuropathy associated with diabetes, neuropathic pain, and post-herpes zoster neuralgia.3,4 Gabapentin also selectively affects the central sensitization-based nociceptive pathway.5
Preemptive use of gabapentin can help avoid hyperalgesia around the wound in postoperative patients, and secondary hyperalgesia induced by heat has a similar mechanism.6
The most common complaint following lumbar laminectomy is pain, which is caused by a variety of factors, including surgical trauma, muscle strain, and scar tissue build-up. Additionally, failed back surgery syndrome may cause discomfort.7 Also, it is the major cause of prolonged hospital stay following the procedure.8
Pain following surgery might include visceral, neurogenic, and inflammatory origins in addition to being solely nociceptive, caused by tissue injury during surgery, which affects the muscles around the spine, that may be retracted or stretched, and the pain can be described as aching or throbbing. Hematoma, swelling, or fluid accumulation may lead to pressure around nearby strictures may also be a cause.9,10
Nerve injury or irritation during the procedure might result in neuropathic pain. Pain is affected by patient-specific factors such as age, gender, and pain threshold. According to reports, incisional pain is more intense than visceral pain and predominates during the first 48 hours following laminectomy.11
The pain experienced after laminectomy, particularly at the site of surgery, is attributed to the formation of scar tissue around the surgical site or near the nerve root and is always described as stabbing or burning pain.12
The assessment of pain severity by different tools, the most commonly used is the Visual Analogue Scale (VAS), is a common tool for determining pain severity. It has a 10-centimeter line that goes from "no pain" on the left to "worst pain imaginable" on the right. Patients mark their pain level on this line during the evaluation, and the distance from the left end is measured. This measured value represents pain severity numerically, with larger values reflecting more intense pain.13
To study the effect of oral gabapentin 300 mg given 2 hours before surgery as preemptive analgesia to attenuate post-operative pain in patients undergoing abdominal surgery.
This prospective randomized control trial was conducted at Al-Sader Teaching Hospital between 1 July 2023 and 1 October 2024 after obtaining ethical approval from the ethical committee in the College of Medicine at Jabir ibn Hayyan University. Written informed consent was obtained from all patients enrolled in this study (No.474 JMU-7th April 2024)
Before starting the study, a careful plan was chalked out, taking into account the expected effect size, a significance level of 0.05, and a desired power of 80%. It was determined that enrolling 25 patients in each group would be sufficient to detect a meaningful difference between them, so a total of 50 patients were selected and randomly divided into two equal groups: the Group G (Group G) and the control group (Group C).
Patients from both genders, with a physical status ASA I or ASA II, 18-60 years old, with an ideal body weight or 20% more, undergoing elective laminectomy under general anesthesia were enrolled. The expected duration of surgery was less than 4 hours. Patients with chronic neurological disease, a history of psychiatric disorder, and patients who were already taking antihypertensive medications or oral gabapentin were excluded. Patients known to have an allergy to certain drugs involved in this study were also excluded.
After informed consent, patients were shown how to grade the pain from 0-10. Basic demographic data and information were recorded from all patients. Patients in Group G were given a capsule of gabapentin 300 mg with a sip of water two hours before shifting to the operating room, and Group C received a capsule of placebo. Baseline hemodynamic parameters were recorded. After being shifted to the operating room, all patients were attached to standard monitoring, e.g., ECG, pulse oximeter, non-invasive blood pressure, and temperature probe. All variables were recorded at 15-minute intervals and continued. Induction of general anesthesia started with propofol 2 mg/kg, ketamine 0.5 mg/kg, and rocuronium 0.5 mg/kg to facilitate intubation. Anesthesia was maintained with isoflurane 1% and nitrous oxide 1:1. Inj. paracetamol 1 g and nefopam 20 mg were given IV to both groups.
At the end of the surgery, isoflurane was discontinued, and the neostigmine 2.5 mg plus atropine 1 mg were injected when the patients were adequately breathing spontaneously, with positive clinical signs observed, then the patients were extubated and transferred to the post-anesthesia care unit (PACU).
Pain was measured with 0 to 10 visual analogue scale (VAS) at 0, 2, 4, 6, 8, 12, and 24 hours; 0 referred to no pain and 10 referred to the worst imaginable pain. The cutoff point to start analgesia was a VAS score of 4 or more. The time and the dosage requested for paracetamol rescue doses were recorded.
2.1. Statistical analysis
The statistical software SPSS 26.0 version was used to examine the data. The mean ± standard deviation is used to express the results for quantitative data, such as age, BMI, duration of surgery, duration of anesthesia, and pain (VAS scores). Qualitative data, such as gender and ASA status, are represented as percentages and frequencies [n (%)]. Fisher's exact tests and the chi-square tests were used to determine statistically significant differences between independent and outcome factors. A 5% threshold (P < 0.05)
was used for significance testing and correlation.
Fifty patients were enrolled in this study, 25 in each group. The mean age in Group C and Group G was 33.32 ± 7.88 and 36.36 ± 7.84, respectively. 11 males and 14 females were in Group C, while 10 males and 15 females were in Group G. The groups were comparable in age, ASA, sex, BMI, duration of anesthesia (DOA), and duration of surgery (DOS), with no statistical differences between the two groups, with a P > 0.05 (Table 1).
As observed in Table 2, at the majority of the time, the scores are significantly lower in gabapentin (Group G) as compared with control (Group C) at zero hr, at 2, 4, and 24 hr (P < 0.05); however, no significant differences showed between the group at 6 and 12 hr (P > 0.05).
The total frequency of pain in the control group was 58.95%, while it was lower in the Group G at 41.04%.
The number of times for the need of rescue analgesic paracetamol IV 10 mg/kg was significantly different between the groups. Eight patients in the control group received paracetamol once only, and 4 patients receive it 2 times. However, in the Group G, 3 patients received paracetamol once, and one patient received it 2 times (P = 0.045) (Figure 1).
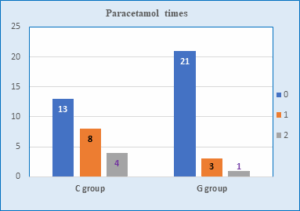
Figure 1: Times for rescue paracetamol in both of groups
Table 3 shows that the Group G received a lower rescue dose of paracetamol (200.0 ± 500.0) as compared with the control group (640.0 ± 757.18), with a P < 0.05.
The mean arterial blood pressure (MAP) showed no significant differences at baseline in either the control group (76.60 ± 10.42) or the Group G (77.360 ± 9.72), with a P = 0.791. The MAP 15 min after induction was 75.08 ± 8.12 mmHg for Group C and 74.48 ± 10.58 mmHg for Group G (P = 0.823).
The heart rate (HR) showed statistically significant differences at baseline in the control group compared to Group G (78.56 ± 6.79 vs. 85.96 ± 6.80; P < 0.001). There were insignificant differences for the HR 15 min after induction for the control group and Group G (79.20 ± 5.13 vs. 78.96 ± 6.26; P = 0.883).
The blood oxygen saturation (SpO2) described in Figure 2 shows no significant differences at baseline in either the Group C (97.16 ± 1.214) or the Group G (96.88 ± 1.16), with a P = 0.410. The SpO2 15 min after induction for the control group (99.12 ± 0.88) and Group G (99.44 ± 0.71), and the P = 0.164.
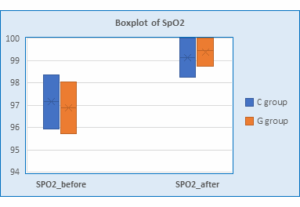
Figure 2: SpO2 before and after induction in the two groups
This study proved that administration of a single dose of gabapentin 300 mg orally two hours before surgery in patients undergoing elective lumbar laminectomy under general anesthesia decreased postoperative VAS scores at 0, 2, 4, and 24 hours and reduced the need for rescue analgesics when compared to the control group.
By blocking the stimulation of neurotransmitter excitation, gabapentin significantly reduces acute postoperative pain in the α2δ voltage-dependent calcium channels subunit.13
The study reported by Goa KL et al. (2023) proved that with 300 mg of single oral gabapentin, the usual highest level of plasma concentration was reached in 2 to 3 hours, and it's dose-related.14 Eckhardt K et al. (2020) found that giving gabapentin 2 hours before surgery shows in reaching plasma concentration at the time of surgical stimulation, which corresponds to how long its antihyperalgesic effect lasts.15 Since gabapentin was given two hours before surgery, we noticed that this effect persisted from the recovery room period until 24 hours after surgery. This fact-corroborative study was reported by Modak et al.,16 who observed that the control group had a considerably higher VAS score and rescue analgesia in the first hour postoperatively.
Turon et al. (2024) used 1.2 g of gabapentin, 1 hr of spinal anesthesia, and concluded that there was a reduction in morphine consumption.17 This result was not in agreement with what Bartholdy et al. (2018) found.18 The 800 mg oral gabapentin and placebo groups did not significantly differ in their post-hysterectomy pain levels, according to the authors; however, gabapentin decreased morphine use by 32%. Gabapentin takes one to two hours to start working as an antihyperalgesic, according to earlier research. Bartholdy et al. fortunately administered it 30 minutes before surgery. Another factor that may have contributed to the reference study's reported delay in gabapentin's efficacy was the brief operation (30 min).
Pandey CK et al. (2018) studied four groups receiving administration of gabapentin according to doses ranging from 300 to 1200 mg 2 hours before surgery.19 The outcome was that patients who received 600, 900, and 1200 mg were associated with lower values of VAS scores at all times compared with 300 mg gabapentin. Our research study used only 300 mg of gabapentin, which found a reduction in VAS scores, but not at all times, only at 6hs, and 12 hrs. was comparable with the control group. The dosage was in agreement with the 300–1200 mg, 3 times a day, a single dose of gabapentin that is advised for the treatment of neuropathic pain. Since it was discovered that there was no extra advantage to raising the dosage of gabapentin to 600 mg or higher, we chose to use the lowest possible dose of 300 mg.
Logan et al. (2021) examined that during lumber laminectomy, 300 mg of gabapentin didn’t affect postoperative pain relief; they proved that smaller doses are ineffective, which is not in line with current research.20
The primary goal of mixing various analgesic medications is to achieve additive or synergistic analgesia, which enables a lower dosage of each medication with a better safety profile.21
For intraoperative pain management, we established a fixed-dose regimen of paracetamol and acupan, with paracetamol provided as a rescue analgesic that is administered only upon patient request postoperatively. We found that the Group G requested fewer paracetamol times and dosage versus the control group.
Gabapentin has a good tolerance rate. While used to treat chronic pain, it has few adverse effects and just a few mild interactions with other medications.22 A single oral dosage of gabapentin did not cause any noticeable adverse effects in our experience. Our findings are consistent with other investigations that have been published.23
According to the study's findings, patients having spine surgeries can effectively manage their postoperative pain with a single oral dosage of gabapentin as a pre-emptive analgesic. The gabapentin's effects not only extend the duration but also minimize the necessity for rescue analgesics.
The total incidence of pain was approximately 59% in the control group; however, it was as low as 41% in the Group G.
Limitations
The pain reduction observed in our study could be limited by the lower dosage used. As the study used a single, relatively low dose of gabapentin (300 mg), which might not be the most effective dose for every patient. Previous research used higher doses, such as 600 to 1200 mg, that may offer more consistent and prolonged pain relief.
The study being conducted at a single center with only 25 patients in each group, the findings may not be widely applicable. To strengthen the evidence and improve the generalizability, further studies involving multiple centers are recommended.
Recommendation
This research involved patients undergoing elective spine surgeries, a broad surgery field that increases the chance of bias. Therefore, we recommended applying this method to specific types of surgery.
Additional research is also needed with a large sample size.
*Department of Surgery, College of Medicine, Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf, Iraq
Correspondence: Ali Najih Al-Awwadyl, Email: ali.alawwady@jmu.edu.iq
ABSTRACT
Background: Postoperative pain following lumbar laminectomy is experienced by almost all patients and may necessitate opioid use. Gabapentin is an anticonvulsant drug shown to be efficient in managing reflex sympathetic dystrophy, neuropathy associated with diabetes, post-herpetic neuralgia, and neuropathic pain. This study aimed to assess the efficacy of pre-emptive administration of gabapentin 300 mg orally for reducing postoperative pain after lumbar laminectomy.
Methodology: A randomized clinical trial was carried out on 50 patients, selected with a convenience sampling method, from July 2023 to October 2024, at Al-Sader Teaching Hospital. All patients were randomly assigned to two groups: a control group received a placebo capsule, and the study group received 300 mg of oral gabapentin 2 hours before skin incision. Postoperative analgesic outcomes were assessed over 24 hours, including total paracetamol consumption and pain intensity measured using the Visual Analogue Scale (VAS). Additionally, hemodynamic parameters were evaluated at baseline (prior to anesthesia) and 15 min after induction.
Result: During the first 24 hours postoperatively, total paracetamol consumption was higher in the control group (640.0 ± 757.18 mg) compared to the gabapentin group (200.0 ± 500.0 mg), (P < 0.05). The number of patients who requested paracetamol was higher in the control group compared to the Group G. The VAS scores during recovery, then at 2, 4, 12, and 24 hr postoperatively, were significantly lower in the Group G compared to the control group (P < 0.05). Mean arterial blood pressure and oxygen saturation were comparable in both groups before induction (baseline) and at 15 min after induction, and the differences were not statistically significant (P > 0.05). Heart rate was significantly different between groups at baseline, but there was no statistically significant difference 15 min after induction.
Conclusion: Gabapentin 300 mg orally as pre-emptive analgesia decreases postoperative pain and reduces the need for paracetamol consumption after lumbar laminectomy.
Abbreviations: BMI: Basal metabolic index, DOA: duration of anesthesia, DOS: duration of surgery, VAS: Visual Analogue Scale
Keywords: Analgesia; Gabapentin; lumbar laminectomy; pain; VAS score
Citation: Al-Awwady AN. Efficacy of preemptive oral gabapentin for postoperative pain control following lumbar laminectomy. Anaesth. pain intensive care 2025;29(6):463-68. DOI: 10.35975/apic.v29i6.2888
1. INTRODUCTION
Postoperative pain following lumbar laminectomy is experienced in all patients and may even necessitate opioid use. As a result, the popularity of multimodal analgesic approaches, which involve various drugs acting on different analgesic mechanisms, have increased,1 and because of the many mechanisms underlying the cause of postoperative pain, a multimodal analgesia plan that combines opioid and non-opioid analgesic drugs can be used to improve the effectiveness of analgesia and reduce their adverse effects.2
Gabapentin is an anticonvulsant drug shown to be efficient in managing reflex sympathetic dystrophy, neuropathy associated with diabetes, neuropathic pain, and post-herpes zoster neuralgia.3,4 Gabapentin also selectively affects the central sensitization-based nociceptive pathway.5
Preemptive use of gabapentin can help avoid hyperalgesia around the wound in postoperative patients, and secondary hyperalgesia induced by heat has a similar mechanism.6
The most common complaint following lumbar laminectomy is pain, which is caused by a variety of factors, including surgical trauma, muscle strain, and scar tissue build-up. Additionally, failed back surgery syndrome may cause discomfort.7 Also, it is the major cause of prolonged hospital stay following the procedure.8
Pain following surgery might include visceral, neurogenic, and inflammatory origins in addition to being solely nociceptive, caused by tissue injury during surgery, which affects the muscles around the spine, that may be retracted or stretched, and the pain can be described as aching or throbbing. Hematoma, swelling, or fluid accumulation may lead to pressure around nearby strictures may also be a cause.9,10
Nerve injury or irritation during the procedure might result in neuropathic pain. Pain is affected by patient-specific factors such as age, gender, and pain threshold. According to reports, incisional pain is more intense than visceral pain and predominates during the first 48 hours following laminectomy.11
The pain experienced after laminectomy, particularly at the site of surgery, is attributed to the formation of scar tissue around the surgical site or near the nerve root and is always described as stabbing or burning pain.12
The assessment of pain severity by different tools, the most commonly used is the Visual Analogue Scale (VAS), is a common tool for determining pain severity. It has a 10-centimeter line that goes from "no pain" on the left to "worst pain imaginable" on the right. Patients mark their pain level on this line during the evaluation, and the distance from the left end is measured. This measured value represents pain severity numerically, with larger values reflecting more intense pain.13
To study the effect of oral gabapentin 300 mg given 2 hours before surgery as preemptive analgesia to attenuate post-operative pain in patients undergoing abdominal surgery.
2. METHODOLOGY
This prospective randomized control trial was conducted at Al-Sader Teaching Hospital between 1 July 2023 and 1 October 2024 after obtaining ethical approval from the ethical committee in the College of Medicine at Jabir ibn Hayyan University. Written informed consent was obtained from all patients enrolled in this study (No.474 JMU-7th April 2024)
Before starting the study, a careful plan was chalked out, taking into account the expected effect size, a significance level of 0.05, and a desired power of 80%. It was determined that enrolling 25 patients in each group would be sufficient to detect a meaningful difference between them, so a total of 50 patients were selected and randomly divided into two equal groups: the Group G (Group G) and the control group (Group C).
Patients from both genders, with a physical status ASA I or ASA II, 18-60 years old, with an ideal body weight or 20% more, undergoing elective laminectomy under general anesthesia were enrolled. The expected duration of surgery was less than 4 hours. Patients with chronic neurological disease, a history of psychiatric disorder, and patients who were already taking antihypertensive medications or oral gabapentin were excluded. Patients known to have an allergy to certain drugs involved in this study were also excluded.
After informed consent, patients were shown how to grade the pain from 0-10. Basic demographic data and information were recorded from all patients. Patients in Group G were given a capsule of gabapentin 300 mg with a sip of water two hours before shifting to the operating room, and Group C received a capsule of placebo. Baseline hemodynamic parameters were recorded. After being shifted to the operating room, all patients were attached to standard monitoring, e.g., ECG, pulse oximeter, non-invasive blood pressure, and temperature probe. All variables were recorded at 15-minute intervals and continued. Induction of general anesthesia started with propofol 2 mg/kg, ketamine 0.5 mg/kg, and rocuronium 0.5 mg/kg to facilitate intubation. Anesthesia was maintained with isoflurane 1% and nitrous oxide 1:1. Inj. paracetamol 1 g and nefopam 20 mg were given IV to both groups.
At the end of the surgery, isoflurane was discontinued, and the neostigmine 2.5 mg plus atropine 1 mg were injected when the patients were adequately breathing spontaneously, with positive clinical signs observed, then the patients were extubated and transferred to the post-anesthesia care unit (PACU).
Pain was measured with 0 to 10 visual analogue scale (VAS) at 0, 2, 4, 6, 8, 12, and 24 hours; 0 referred to no pain and 10 referred to the worst imaginable pain. The cutoff point to start analgesia was a VAS score of 4 or more. The time and the dosage requested for paracetamol rescue doses were recorded.
2.1. Statistical analysis
The statistical software SPSS 26.0 version was used to examine the data. The mean ± standard deviation is used to express the results for quantitative data, such as age, BMI, duration of surgery, duration of anesthesia, and pain (VAS scores). Qualitative data, such as gender and ASA status, are represented as percentages and frequencies [n (%)]. Fisher's exact tests and the chi-square tests were used to determine statistically significant differences between independent and outcome factors. A 5% threshold (P < 0.05)
was used for significance testing and correlation.
3. RESULTS
Fifty patients were enrolled in this study, 25 in each group. The mean age in Group C and Group G was 33.32 ± 7.88 and 36.36 ± 7.84, respectively. 11 males and 14 females were in Group C, while 10 males and 15 females were in Group G. The groups were comparable in age, ASA, sex, BMI, duration of anesthesia (DOA), and duration of surgery (DOS), with no statistical differences between the two groups, with a P > 0.05 (Table 1).
| Table 1: Demographic profiles | |||
| Parameter | Group C
(n = 25) |
Group G
(n = 25) |
P-value |
| Age (years) | 33.32 ± 7.88 | 36.36 ± 7.84 | 0.178 |
| BMI (Kg/m2) | 26.39 ± 3.29 | 25.572 ± 2.47 | 0.325 |
| DOS (min) | 43.60 ± 7.29 | 46.00 ± 10.0 | 0.337 |
| DOA (min) | 63.80 ± 7.67 | 66.20 ± 14.16 | 0.460 |
| Gender (M : F) | 11:14 | 10:15 | 0.774 |
| ASA (I : II) | 16:9 | 16:9 | - |
| Data presented as mean ± SD or n (%); ASA: American Society of Anesthesia, BMI: body mass index, DOS: duration of surgery, DOA: duration of anesthesia; P < 0.05 considered as significant | |||
As observed in Table 2, at the majority of the time, the scores are significantly lower in gabapentin (Group G) as compared with control (Group C) at zero hr, at 2, 4, and 24 hr (P < 0.05); however, no significant differences showed between the group at 6 and 12 hr (P > 0.05).
| Table 2: Comparative postoperative VAS scores in the two groups | |||
| Time | Group C
(n=25) |
Group G
(n=25) |
P-value |
| 0 hr | 4.64 ± 1.75 | 2.88 ± 1.50 | < 0.001** |
| 2 hr | 3.92 ± 1.255 | 2.08 ± 1.41 | < 0.001** |
| 4 hr | 3.76 ± 1.200 | 1.80 ± 0.81 | < 0.001** |
| 6 hr | 2.96 ± 1.274 | 2.48 ± 0.91 | 0.133 |
| 12 hr | 2.24 ± 0.925 | 1.76 ± 1.58 | 0.198 |
| 24 hr | 1.84 ± 0.800 | 1.28 ± 0.67 | 0.010* |
| Mean ± SD; VAS: visual analog score, * = significant, ** = highly significant. | |||
The total frequency of pain in the control group was 58.95%, while it was lower in the Group G at 41.04%.
The number of times for the need of rescue analgesic paracetamol IV 10 mg/kg was significantly different between the groups. Eight patients in the control group received paracetamol once only, and 4 patients receive it 2 times. However, in the Group G, 3 patients received paracetamol once, and one patient received it 2 times (P = 0.045) (Figure 1).
Figure 1: Times for rescue paracetamol in both of groups
Table 3 shows that the Group G received a lower rescue dose of paracetamol (200.0 ± 500.0) as compared with the control group (640.0 ± 757.18), with a P < 0.05.
| Table 3: Comparative paracetamol consumption over 24 hours in groups | ||||
| Group C | Group G | P-value | ||
| Paracetamol consumed (mg) | 640.0 ± 757.18 | 200.0 ± 500.0 | 0.019* | |
| Mean ± SD; VAS: visual analog score, * = significant, ** = highly significant. | ||||
The mean arterial blood pressure (MAP) showed no significant differences at baseline in either the control group (76.60 ± 10.42) or the Group G (77.360 ± 9.72), with a P = 0.791. The MAP 15 min after induction was 75.08 ± 8.12 mmHg for Group C and 74.48 ± 10.58 mmHg for Group G (P = 0.823).
The heart rate (HR) showed statistically significant differences at baseline in the control group compared to Group G (78.56 ± 6.79 vs. 85.96 ± 6.80; P < 0.001). There were insignificant differences for the HR 15 min after induction for the control group and Group G (79.20 ± 5.13 vs. 78.96 ± 6.26; P = 0.883).
The blood oxygen saturation (SpO2) described in Figure 2 shows no significant differences at baseline in either the Group C (97.16 ± 1.214) or the Group G (96.88 ± 1.16), with a P = 0.410. The SpO2 15 min after induction for the control group (99.12 ± 0.88) and Group G (99.44 ± 0.71), and the P = 0.164.
Figure 2: SpO2 before and after induction in the two groups
4. DISCUSSION
This study proved that administration of a single dose of gabapentin 300 mg orally two hours before surgery in patients undergoing elective lumbar laminectomy under general anesthesia decreased postoperative VAS scores at 0, 2, 4, and 24 hours and reduced the need for rescue analgesics when compared to the control group.
By blocking the stimulation of neurotransmitter excitation, gabapentin significantly reduces acute postoperative pain in the α2δ voltage-dependent calcium channels subunit.13
The study reported by Goa KL et al. (2023) proved that with 300 mg of single oral gabapentin, the usual highest level of plasma concentration was reached in 2 to 3 hours, and it's dose-related.14 Eckhardt K et al. (2020) found that giving gabapentin 2 hours before surgery shows in reaching plasma concentration at the time of surgical stimulation, which corresponds to how long its antihyperalgesic effect lasts.15 Since gabapentin was given two hours before surgery, we noticed that this effect persisted from the recovery room period until 24 hours after surgery. This fact-corroborative study was reported by Modak et al.,16 who observed that the control group had a considerably higher VAS score and rescue analgesia in the first hour postoperatively.
Turon et al. (2024) used 1.2 g of gabapentin, 1 hr of spinal anesthesia, and concluded that there was a reduction in morphine consumption.17 This result was not in agreement with what Bartholdy et al. (2018) found.18 The 800 mg oral gabapentin and placebo groups did not significantly differ in their post-hysterectomy pain levels, according to the authors; however, gabapentin decreased morphine use by 32%. Gabapentin takes one to two hours to start working as an antihyperalgesic, according to earlier research. Bartholdy et al. fortunately administered it 30 minutes before surgery. Another factor that may have contributed to the reference study's reported delay in gabapentin's efficacy was the brief operation (30 min).
Pandey CK et al. (2018) studied four groups receiving administration of gabapentin according to doses ranging from 300 to 1200 mg 2 hours before surgery.19 The outcome was that patients who received 600, 900, and 1200 mg were associated with lower values of VAS scores at all times compared with 300 mg gabapentin. Our research study used only 300 mg of gabapentin, which found a reduction in VAS scores, but not at all times, only at 6hs, and 12 hrs. was comparable with the control group. The dosage was in agreement with the 300–1200 mg, 3 times a day, a single dose of gabapentin that is advised for the treatment of neuropathic pain. Since it was discovered that there was no extra advantage to raising the dosage of gabapentin to 600 mg or higher, we chose to use the lowest possible dose of 300 mg.
Logan et al. (2021) examined that during lumber laminectomy, 300 mg of gabapentin didn’t affect postoperative pain relief; they proved that smaller doses are ineffective, which is not in line with current research.20
The primary goal of mixing various analgesic medications is to achieve additive or synergistic analgesia, which enables a lower dosage of each medication with a better safety profile.21
For intraoperative pain management, we established a fixed-dose regimen of paracetamol and acupan, with paracetamol provided as a rescue analgesic that is administered only upon patient request postoperatively. We found that the Group G requested fewer paracetamol times and dosage versus the control group.
Gabapentin has a good tolerance rate. While used to treat chronic pain, it has few adverse effects and just a few mild interactions with other medications.22 A single oral dosage of gabapentin did not cause any noticeable adverse effects in our experience. Our findings are consistent with other investigations that have been published.23
5. CONCLUSION
According to the study's findings, patients having spine surgeries can effectively manage their postoperative pain with a single oral dosage of gabapentin as a pre-emptive analgesic. The gabapentin's effects not only extend the duration but also minimize the necessity for rescue analgesics.
The total incidence of pain was approximately 59% in the control group; however, it was as low as 41% in the Group G.
Limitations
The pain reduction observed in our study could be limited by the lower dosage used. As the study used a single, relatively low dose of gabapentin (300 mg), which might not be the most effective dose for every patient. Previous research used higher doses, such as 600 to 1200 mg, that may offer more consistent and prolonged pain relief.
The study being conducted at a single center with only 25 patients in each group, the findings may not be widely applicable. To strengthen the evidence and improve the generalizability, further studies involving multiple centers are recommended.
Recommendation
This research involved patients undergoing elective spine surgeries, a broad surgery field that increases the chance of bias. Therefore, we recommended applying this method to specific types of surgery.
Additional research is also needed with a large sample size.
REFERENCES
- Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Block CL. Efficacy of postoperative epidural analgesia: A meta-analysis. JAMA. 2003;290(18):2455-63. [PubMed] DOI: 1001/jama.290.18.2455
- Fishman S, Borsook D. Opioids in pain management. In: Benzon H, Raja S, Molloy RE, Strichartz G, editors. Essentials of pain medicine and regional anesthesia. 2nd ed. New York: Churchill Livingstone; 2005.
- Backonja M, Beydoun A, Edwards KR, Schwartz SL, Fonseca V, Hes M, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA. 1998;280(21):1831-6. [PubMed] DOI: 1001/jama.280.21.1831
- Rowbotham M, Harden N, Stacey B, Bernstein P, Magnus-Miller L. Gabapentin for the treatment of postherpetic neuralgia: A randomized controlled trial. JAMA. 1998;280(21):1837-42. [PubMed] DOI: 1001/jama.280.21.1837
- Mao J, Chen LL. Gabapentin in pain management. Anesth Analg. 2000;91(3):680-7. [PubMed] DOI: 1097/00000539-200009000-00034
- Dirks J, Moiniche S, Hilsted KL, Dahl JB. Mechanisms of postoperative pain: Clinical indications for a contribution of central neuronal sensitization. Anesthesiology. 2002;97(6):1591-6. [PubMed] DOI: 1097/00000542-200212000-00035
- Bisgaard T, Klarskov B, Rosenberg J, Kehlet H. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain. 2001;90(3):261-9. [PubMed] DOI: 1016/S0304-3959(00)00406-1
- Liu YY, Yeh CN, Lee HL, Wang SY, Tsai CY, Lin CC, et al. Local anesthesia with ropivacaine for patients undergoing laparoscopic cholecystectomy. World J Gastroenterol. 2009;15(19):2376-80. [PubMed] DOI: 3748/wjg.15.2376
- Siddiqui NA, Azami R, Murtaza G, Nasim S. Postoperative port-site pain after gall bladder retrieval from epigastric vs. umbilical port in laparoscopic cholecystectomy: A randomized controlled trial. Int J Surg. 2012;10(4):213-6. [PubMed] DOI: 1016/j.ijsu.2012.03.008
- Lee IO, Kim SH, Kong MH, Lee MK, Kim NS, Choi YS, et al. Pain after laparoscopic cholecystectomy: The effect and timing of incisional and intraperitoneal bupivacaine. Can J Anesth. 2001;48(6):545-50. [PubMed] DOI: 1007/BF03016830
- Jackson SA, Laurence AS, Hill JC. Does post-laparoscopy pain relate to residual carbon dioxide? Anaesthesia. 1996;51(5):485-7. [PubMed] DOI: 1111/j.1365-2044.1996.tb07798.x
- Manan A, Khan AA, Ahmad I, Usman M. Intraperitoneal bupivacaine as post-laparoscopic cholecystectomy analgesia. J Coll Physicians Surg Pak. 2020;30(1):9-12. [PubMed] DOI: 29271/jcpsp.2020.01.09
- Parikh H, Dash S, Upasani C. Study of the effect of oral gabapentin used as preemptive analgesia to attenuate post-operative pain in patients undergoing abdominal surgery under general anesthesia. Saudi J Anaesth. 2010;4(2):137-41. [PubMed] DOI: 4103/1658-354X.71409
- Goa KL, Sorkin EM. Gabapentin: A review of its pharmacological properties and clinical potential in epilepsy. Drugs. 1993;46(3):409-27. [PubMed] DOI: 2165/00003495-199346030-00007
- Eckhardt K, Ammar S, Hofmann U, Riebe A, Gugeler N, Mikus G. Gabapentin enhances the analgesic effect of morphine in healthy volunteers. Anesth Analg. 2000;91(3):185-91. [PubMed] DOI: 1097/00000539-200007000-00035
- Modak SD, Magar J, Kakad V. Pre-emptive gabapentin for postoperative pain relief in abdominal hysterectomy. Int J Res Med Sci. 2016;4(7):2755-9. DOI: 18203/2320-6012.ijrms20162607
- Turan A, Karamanlioğlu B, Memiş D, Usar P, Pamukçu Z, Türe M. The analgesic effect of gabapentin after total abdominal hysterectomy. Anesth Analg. 2004;98(5):1370-3. [PubMed] DOI: 1213/01.ane.0000108964.70485.b2
- Bartholdy J, Hilsted KL, Hjortsoe NC, Engbaek J, Dahl JB. Effect of gabapentin on morphine demand and pain after laparoscopic sterilization using Filshie clips: A double-blind, randomized clinical trial. BMC Anesthesiol. 2006;6:12. [PubMed] DOI: 1186/1471-2253-6-12
- Pandey CK, Navkar DV, Giri PJ, Raza M, Behari S, Singh RB, et al. Evaluation of optimal preemptive dose of gabapentin for postoperative pain relief after lumbar diskectomy: A randomized, double-blind, placebo-controlled study. J Neurosurg Anesthesiol. 2005;17(2):65-8. [PubMed] DOI: 1097/01.ana.0000151407.62650.51
- Moore L, Norwood C. Gabapentin reduces postoperative pain and opioid consumption in patients who underwent lumbar laminectomy: A randomized, double-blind placebo-controlled trial. J Am Pharm Assoc. 2021;61(5):87-174. [PubMed] DOI: 1016/j.japh.2021.05.002
- Mellick GA, Mellick LB. Reflex sympathetic dystrophy treated with gabapentin. Arch Phys Med Rehabil. 1997;78(1):98-105. [PubMed] DOI: 1016/s0003-9993(97)90020-4
- Pandey CK, Priye S, Singh S, Singh U, Singh RB, Singh PK. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can J Anesth. 2004;51(4):358-63. [PubMed] DOI: 1007/BF03018240
- Rorarius MG, Mennander S, Suominen P, Rintala S, Puura A, Pirhonen R, et al. Gabapentin for the prevention of postoperative pain after vaginal hysterectomy. Pain. 2004;110(1-2):175-81. [PubMed] DOI: 1016/j.pain.2004.03.023