Heba Ismail 1 , Ashgan Raouf Ali 2 , Mina Samir 3 , Reham Gamal 4 , Samuel Fayez 5
Author affiliations:
Background & objective: Most patients undergoing modified radical mastectomy (MRM) suffer significant acute postoperative pain. Anesthetists have tried various analgesic regimens to control the pain, including injectables and nerve blocks. This study compared the analgesic efficacy of preoperative oral gabapentin with and without intravenous infusion of dexmedetomidine (DEX) in patients undergoing MRM under general anesthesia.
Methodology: This randomized, double-blind clinical trial included 60 patients scheduled for MRM. They were randomly allocated to one of the two equal groups. Both groups received oral gabapentin 600 mg one hour before surgery. Group G (n = 30) received a 50 mL normal saline bolus and continuous intraoperative infusion (10 mL/hour). Group DG (n = 30) received a loading dose of DEX 1 µg/kg just before induction of anesthesia, followed by a continuous intraoperative infusion of DEX (0.5 µg/kg/hour). Outcome measures were duration of analgesia, intraoperative fentanyl consumption, postoperative morphine consumption, and VAS scores at rest and on movement.
Results: Duration of postoperative analgesia was significantly longer in the Group DG compared to the Group G (545 ± 49 min. vs. 288 ± 38 min., P < 0.001). Total fentanyl consumption was lower in the Group DG as compared to Group G (30.8 ± 2.0 vs. 41.6 ± 3.4 µg), P < 0.001. The two groups had no significant difference in postoperative morphine consumption (P = 0.405). VAS scores at rest and with movement were significantly lower in the Group DG during the postoperative period.
Conclusion: The analgesic effect of a combination of preoperative oral gabapentin plus perioperative dexmedetomidine infusion is superior to that of oral gabapentin alone in patients undergoing MRM for breast cancer and results in lower VAS scores at rest and with movement.
Abbreviations: α-2AR: α-2-adrenoceptor, DEX: dexmedetomidine, GA: General Anesthesia, MRM: Modified radical mastectomy, PACU: post-anesthesia care unit, VAS: Visual Analogue Scale
Keywords: Analgesia; Dexmedetomidine; Fentanyl; General Anesthesia; Modified radical mastectomy; Morphine
Citation: Ismail H, Ali AR, Samir M, Gamal RM, Fayez S. Oral gabapentin with and without intravenous dexmedetomidine for postoperative analgesia after modified radical mastectomy: a randomized, controlled, double-blind trial. Anaesth. pain intensive care 2025;29(6):447-54. DOI: 10.35975/apic.v29i6.2886
Received: September 24, 2024; Revised: January 05, 2025; Accepted: July 09, 2025
Breast cancer remains the most common women’s cancer globally,1 accounting for 33% of female cancers in Egypt.2 Surgery has been the core treatment of breast cancer for decades. Modified radical mastectomy (MRM) constitutes 31% of all breast surgeries.3 Most patients undergoing MRM suffer significant acute postoperative pain, which impairs recovery and reduces patient satisfaction. In many instances, it leads to an increased rate of chronic postmastectomy pain.4,5 Therefore, adequate analgesia is crucial for better recovery and to prevent long-standing postmastectomy pain.
Numerous approaches are tried to reduce post-mastectomy pain. Perioperative opioids are traditionally the mainstay of postoperative analgesia; however, their significant side effects, including respiratory and central nervous system depression and prolonged post-anesthesia care unit (PACU) stays, promote the shift to opioid-sparing techniques.6 Gabapentin is one of those drugs suggested to provide adequate postoperative analgesia alone or combined with other drugs.7 Preoperative gabapentin was reported to reduce postoperative pain intensity and opioid consumption in various types of surgery.8-10 Preemptive analgesia (PA) is initiating analgesic treatment before tissue injury to prevent the alteration of the central processing of afferent input.11 It is believed to be more effective in controlling postoperative pain than treatment offered after the onset of a painful stimulus.12
Multimodal analgesia combines analgesic remedies with distinct mechanisms of action to improve pain control with minimal side effects13 PA with multiple non-narcotic treatments could significantly reduce postoperative pain.14 Dexmedetomidine (DEX) is a widely used sedative with minimal effect on respiratory function15 It is a highly selective α2-adrenergic agonist with sedative, analgesic, and anxiolytic properties. Preoperative and intraoperative administration of DEX can effectively relieve the anesthesia-induced stress response and reduce anesthetic drugs. Its different site of action compared to other sedatives implies a different analgesic mechanism.
This study compared the analgesic efficacy of preoperative oral gabapentin with and without dexmedetomidine intravenous infusion in patients undergoing modified radical mastectomy under general anesthesia (GA).
This randomized, double-blind clinical trial included 60 patients scheduled for modified radical mastectomy (MRM) under GA at the National Cancer Institute from February to August 2021. The study was approved by the Ethical Committee of the anesthesia department of Kasr El-Aini Hospital. All patients provided written informed consent to participate in the study.
The inclusion criteria were females aged 18 to 65 years, ASA I or II, body mass index (BMI) 20 to 40 kg/m2, and undergoing MRM under GA. Patients with known sensitivity or contraindication to study drugs, a history of psychological disorders, chronic pain, sympathetic disorders, significant liver insufficiency, severe respiratory diseases, or those receiving medications that could result in tolerance to opioids or medicines for cancer pain were excluded from the study.
The participants were randomly allocated to one of two equal groups using computer-generated random numbers (www.Random.org). Group G (n = 30) received oral gabapentin 600 mg (Gabapentin capsules 300 mg, Neurontin; Pfizer, Cairo, Egypt) one hour before surgery. Then, the patients received 50 mL of normal saline intravenously over 10 min just before induction of anesthesia, followed by continuous intraoperative infusion of normal saline at a rate of 10 mL/hour until skin closure. Group DG (n = 30) received 600 mg of gabapentin one hour before surgery. Then, the patients received a loading dose of 1 µg/kg of dexmedetomidine (DEX) in 50 mL of normal saline intravenously over 10 min just before induction of anesthesia. This was followed by a continuous intraoperative infusion of DEX diluted in normal saline at 0.5 µg/kg/hour until skin closure. All patients were monitored for vital signs during intravenous DEX administration.
Both patients and anesthesiologists were blinded to the nature of the administered intravenous solutions prepared by an anesthesiologist with no other role in the study. The investigators collecting intra- and postoperative data were unaware of group allocation. The patients were instructed about using the visual analog score of pain (VAS; 0 = no pain and 10 = worst pain imaginable).
2.1. Anesthetic Management
Preoperative midazolam 0.02 mg/kg IV was administered 30 min before surgery. The patients were monitored continuously using electrocardiography, non-invasive blood pressure, peripheral oxygen saturation, and end-tidal carbon dioxide (Datex-Ohmeda S5 anesthesia monitor, model no: USE1913A). The heart rate (HR), mean arterial blood pressure (MAP), and oxygen saturation were monitored after the induction of anesthesia, with surgical incision, and at 15-minute intervals intraoperatively.
GA was induced using fentanyl 2 μg/kg and propofol 2 mg/kg. Tracheal intubation was facilitated by atracurium 0.5 mg/kg. Anaesthesia was maintained with inhaled sevoflurane in oxygen-enriched air (FiO2 = 0.5) and top-up doses of atracurium (0.1 mg/kg) as required. The patients were mechanically ventilated to keep end-tidal CO2 within the 30-35 mmHg range. All patients received 1 gm of IV paracetamol. The total intraoperative fentanyl consumption was recorded. Bispectral index (BIS) was used to monitor the depth of anesthesia, with target BIS values from 40 to 60 because all the study drugs synergize with inhaled anesthesia.
Ringer acetate was infused to replace any fluid deficit, maintenance, and losses. Hypotension was defined as MBP below 60 mmHg or 70% from baseline. Hypotension episodes were treated with ringer acetate boluses and/or 5 mg ephedrine in incremental doses to maintain MAP above 70 mmHg. Additional bolus doses of fentanyl 0.5 µg/kg were given if the MAP or HR rose above 20% of baseline values. At the end of surgery, residual neuromuscular blockade was reversed by neostigmine 0.05 mg/kg and atropine 0.02 mg/kg. Extubation was performed after complete recovery of the airway reflexes.
In the PACU, the patients were monitored for MBP, HR, and VAS pain scores immediately on arrival and at 2, 6, 12, 18, and 24 h postoperatively. Paracetamol 1 g IV was administered every 8 h. Rescue analgesia was provided as 3 mg IV boluses of morphine when the pain score was >3 with a maximum allowed daily dose of 0.5 mg/kg/24 h. The time to first rescue analgesia and the total amount of morphine consumption were recorded. Side effects, including nausea, vomiting, sedation, hallucination, and respiratory depression, were recorded. Moderate or severe postoperative nausea and vomiting were treated with 0.1 mg/kg of IV ondansetron. Sedation was assessed and scored according to Ramsay score.
The primary outcome measure was the duration of analgesia, defined as the time from the end of surgery to the first rescue analgesia. The secondary outcomes were intraoperative fentanyl consumption, postoperative morphine consumption, pain intensity, and possible complications.
2.2. Sample size
Based on the previous work by Grover et al. (2009), who reported the mean duration time of first rescue analgesia was 90 ± 61.1 min, and Alzeftawy & Elsheikh (2015), who reported 125 ± 25.7 min for DEX infusion. Using a power 80% and 5% significance level, 30 patients in each group were sufficient.16,17 The sample size was calculated using the G*Power program (University of Düsseldorf, Düsseldorf, Germany).
2.3. Statistical methods
Statistical analysis was done using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY, USA). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relation between qualitative variables. For quantitative data, comparison between the two groups was made using an independent sample t-test or Mann-Whitney test. A P < 0.05 was considered significant.
As shown in Figure 1, 76 patients were assessed for eligibility, 11 did not meet the inclusion criteria, and five refused to participate. The results are presented for the remaining 60 patients. There were no significant differences between the two studied groups regarding the baseline characteristics and duration of surgery (Table 1).
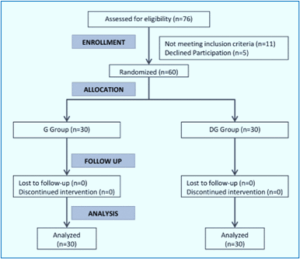
Figure 1: CONSORT flow diagram
The time from skin closure to extubation and duration of postoperative analgesia were significantly longer in the Group DG compared to the Group D. Also, significantly higher number of patients required intraoperative fentanyl (P = 0.001) in the Group G. The total intraoperative fentanyl consumption was significantly higher in the Group G compared to the DG group (P < 0.001). The two groups had no significant difference in the number of patients who requested postoperative morphine (P = 0.405). Those who needed morphine received a single dose of 3 mg. VAS scores at rest and with movement were significantly lower in the Group DG during the postoperative period (Table 3).
The MAP showed modest changes during intra- and postoperative periods in the two studied groups within the clinically accepted range. Preoperative MAP was comparable, while MAP was significantly lower in the Group DG from the induction of anesthesia till the end of surgery. MAP was comparable between the two groups at the immediate postoperative period (Table 4), with lower values after 2, 12, and 24 h.
The heart rate changed slightly in the two groups and remained within the clinically accepted range. Preoperative HR was comparable, while HR was significantly lower in the Group DG from the induction of anesthesia till the end of surgery. The HR was comparable between the two groups during the whole postoperative period (Table 5).
The sedation score was significantly higher in the DG group up to 12 h postoperatively compared to the G group. Then, the sedation scores were comparable after 18 and 24 h (Table 6). Postoperative nausea and vomiting were observed in 9 patients (30%) of the Group G and 6 (20%) of the Group DG (P = 0.371).
This study demonstrated that adding intravenous DEX to preoperative gabapentin 600 mg improved the analgesic profile in patients subjected to MRM. The combination of DEX and gabapentin was associated with a longer duration of analgesia, lower pain intensity at rest and movement, and lower intraoperative fentanyl consumption compared to gabapentin only. Also, the sedation score was significantly higher in the DG group. Postoperative morphine consumption did not change with the addition of DEX to gabapentin. However, patients who required morphine in both groups received only a single dose of 3 mg throughout the 24 postoperative hours. Both groups were hemodynamically stable, with limited postoperative nausea and vomiting cases.
To date, there is no consensus on the best analgesic option after MRM that can alleviate acute pain and prevent the development of chronic postmastectomy pain. It is believed that despite the advancement of pain control techniques, nearly half of the patients still have significant pain after breast cancer surgery.18 This study aimed to test an opioid-sparing, preemptive, multimodal approach for postoperative analgesia following MRM using gabapentin and DEX.
Gabapentin and DEX are offered as effective agents for pain reduction after surgery. Zoroufchi et al. compared both drugs in laparoscopic cholecystectomy patients19 They found DEX more effective than gabapentin in pain reduction and better sedation during and after surgery. A recent prospective placebo-controlled study evaluated the gabapentin/DEX combination in patients undergoing MRM. Preoperative oral gabapentin 400 mg plus DEX infusion was associated with lower pain scores and reduced intraoperative fentanyl and postoperative morphine consumption compared to placebo.20
Preemptive analgesia (PA) is an antinociceptive treatment that blocks central and peripheral sensitization caused by surgical incisions. In addition to controlling acute postoperative pain, PA aims to prevent chronic neuropathic pain.21 A network meta-analysis compared 19 preemptive analgesia regimens regarding postoperative pain intensity and opioid consumption, and PONV. Compared with placebo, pain intensity was reduced in 10, and opioid consumption was decreased in 8 of the 19 regimens.22 The PROSPECT Working Group has recently recommended preoperative gabapentin,23 which was associated with reducing postoperative pain and morphine consumption after breast surgery.24,25
Previous studies have shown that preemptive gabapentin reduces postoperative pain and opioid consumption.8,10,26 A randomized, double-blind study found that preemptive oral gabapentin 600 mg significantly reduced postoperative pain, analgesic rescue requirements, and PONV in patients subjected to abdominal hysterectomy.8 Another study reported similar findings after oral gabapentin 1200 mg or placebo two hours before abdominal hysterectomy.9 A systematic review of 6 studies assessed the analgesic effect of gabapentin or pregabalin in patients undergoing anterior cruciate ligament reconstruction. Three studies showed that gabapentin significantly decreased pain scores and opioid consumption compared to controls.27 Preoperative gabapentin 600 mg did not reduce postoperative pain but decreased morphine consumption after video-assisted thoracoscopic surgery.28 In a meta-analysis of 9 RCTs, Jiang et al. demonstrated a reduction of morphine consumption after preoperative oral administration of gabapentin in breast cancer surgery.25
The mechanism of action of gabapentin is not fully understood. Despite its structural similarity to gamma-aminobutyric acid (GABA), it does not act directly on the GABA receptor.29 It may exert its effect through the N-methyl-D-aspartate (NMDA) neurotransmitter.30
Perioperative multimodal opioid-sparing analgesic regimens are considered the best options for pain relief following breast surgical procedures.31 The pharmacodynamic profile of DEX appoints the drug as a potential adjunct to enhance the non-opioid analgesic efficacy of preemptive gabapentin. It is a highly selective α-2-adrenoceptor (α-2AR) agonist with sedative, anxiolytic, and analgesic effects.32 Its sedative and sympatholytic effects are mediated through the activation of α-2AR of the locus coeruleus and subsequent inhibition of ascending noradrenergic pathways. However, the mechanism of its analgesic activity has not been fully explained. A potential mechanism is the activation of potassium channels, resulting in membrane hyperpolarization of nociceptive neurons. Another mechanism is that alpha-2AR activation may induce calcium conductance modulation, leading to reduced neurotransmitter release.
Intraoperative DEX was found to reduce postoperative pain and opioid consumption. In patients undergoing laparoscopic cholecystectomy, intraoperative DEX infusion decreased postoperative pain and morphine consumption and prolonged the duration of postoperative analgesia.32 A systematic review of 18 RCTs reported reduced intraoperative and postoperative opioid consumption and pain intensity in adult patients.33
A meta-analysis of 12 studies evaluated the analgesic efficacy of DEX as an adjuvant in cases of breast cancer surgery. Pooled analysis demonstrated prolonged analgesia, lower pain intensity, and reduced postoperative opioids and intraoperative fentanyl.34 A recent study evaluated the intraoperative analgesic efficacy of DEX as an adjuvant to peripheral nerve block in real time using non-invasive nociception monitoring. Intravenous DEX infusion offered rapid and proper intraoperative and postoperative analgesia with hemodynamic stability and without respiratory depression.35
In conclusion, the analgesic effect of a combination of preoperative oral gabapentin plus perioperative dexmedetomidine infusion is superior to that of gabapentin alone in patients undergoing MRM for breast cancer. The combined regimen was associated with prolonged postoperative analgesia, lower pain intensity, lower intraoperative fentanyl consumption, and better sedation. Postoperative morphine consumption was limited with gabapentin and the combined regimen. Both regimens were characterized by hemodynamic stability and minimal adverse effects.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
AS: Corresponding author, Final Approval
AZ: Scientific literature search, Data collection, Manuscript writing, Editing, Final Approval
MS: Scientific literature search
MB: Conduct of study
Author affiliations:
- Heba Ismail, Assistant Professor, Department of Anesthesia & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; Email: drheba@hotmail.com
- Ashgan Raouf Ali, Professor, Department of Anesthesia & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; Email: ashganraouf@yahoo.com
- Mina Samir, Assistant Lecturer, Department of Anesthesia & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; Email: minasamir82@yahoo.com
- Reham Mohamed Gamal, Assistant Professor, Department of Anesthesia & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; Email: rehamgamal_nci@hotmail.com
- Samuel Fayez, Lecturer, Department of Anesthesia & Pain Management, National Cancer Institute, Cairo University, Cairo, Egypt; Email: samueltwins@yahoo.com
ABSTRACT
Background & objective: Most patients undergoing modified radical mastectomy (MRM) suffer significant acute postoperative pain. Anesthetists have tried various analgesic regimens to control the pain, including injectables and nerve blocks. This study compared the analgesic efficacy of preoperative oral gabapentin with and without intravenous infusion of dexmedetomidine (DEX) in patients undergoing MRM under general anesthesia.
Methodology: This randomized, double-blind clinical trial included 60 patients scheduled for MRM. They were randomly allocated to one of the two equal groups. Both groups received oral gabapentin 600 mg one hour before surgery. Group G (n = 30) received a 50 mL normal saline bolus and continuous intraoperative infusion (10 mL/hour). Group DG (n = 30) received a loading dose of DEX 1 µg/kg just before induction of anesthesia, followed by a continuous intraoperative infusion of DEX (0.5 µg/kg/hour). Outcome measures were duration of analgesia, intraoperative fentanyl consumption, postoperative morphine consumption, and VAS scores at rest and on movement.
Results: Duration of postoperative analgesia was significantly longer in the Group DG compared to the Group G (545 ± 49 min. vs. 288 ± 38 min., P < 0.001). Total fentanyl consumption was lower in the Group DG as compared to Group G (30.8 ± 2.0 vs. 41.6 ± 3.4 µg), P < 0.001. The two groups had no significant difference in postoperative morphine consumption (P = 0.405). VAS scores at rest and with movement were significantly lower in the Group DG during the postoperative period.
Conclusion: The analgesic effect of a combination of preoperative oral gabapentin plus perioperative dexmedetomidine infusion is superior to that of oral gabapentin alone in patients undergoing MRM for breast cancer and results in lower VAS scores at rest and with movement.
Abbreviations: α-2AR: α-2-adrenoceptor, DEX: dexmedetomidine, GA: General Anesthesia, MRM: Modified radical mastectomy, PACU: post-anesthesia care unit, VAS: Visual Analogue Scale
Keywords: Analgesia; Dexmedetomidine; Fentanyl; General Anesthesia; Modified radical mastectomy; Morphine
Citation: Ismail H, Ali AR, Samir M, Gamal RM, Fayez S. Oral gabapentin with and without intravenous dexmedetomidine for postoperative analgesia after modified radical mastectomy: a randomized, controlled, double-blind trial. Anaesth. pain intensive care 2025;29(6):447-54. DOI: 10.35975/apic.v29i6.2886
Received: September 24, 2024; Revised: January 05, 2025; Accepted: July 09, 2025
1. INTRODUCTION
Breast cancer remains the most common women’s cancer globally,1 accounting for 33% of female cancers in Egypt.2 Surgery has been the core treatment of breast cancer for decades. Modified radical mastectomy (MRM) constitutes 31% of all breast surgeries.3 Most patients undergoing MRM suffer significant acute postoperative pain, which impairs recovery and reduces patient satisfaction. In many instances, it leads to an increased rate of chronic postmastectomy pain.4,5 Therefore, adequate analgesia is crucial for better recovery and to prevent long-standing postmastectomy pain.
Numerous approaches are tried to reduce post-mastectomy pain. Perioperative opioids are traditionally the mainstay of postoperative analgesia; however, their significant side effects, including respiratory and central nervous system depression and prolonged post-anesthesia care unit (PACU) stays, promote the shift to opioid-sparing techniques.6 Gabapentin is one of those drugs suggested to provide adequate postoperative analgesia alone or combined with other drugs.7 Preoperative gabapentin was reported to reduce postoperative pain intensity and opioid consumption in various types of surgery.8-10 Preemptive analgesia (PA) is initiating analgesic treatment before tissue injury to prevent the alteration of the central processing of afferent input.11 It is believed to be more effective in controlling postoperative pain than treatment offered after the onset of a painful stimulus.12
Multimodal analgesia combines analgesic remedies with distinct mechanisms of action to improve pain control with minimal side effects13 PA with multiple non-narcotic treatments could significantly reduce postoperative pain.14 Dexmedetomidine (DEX) is a widely used sedative with minimal effect on respiratory function15 It is a highly selective α2-adrenergic agonist with sedative, analgesic, and anxiolytic properties. Preoperative and intraoperative administration of DEX can effectively relieve the anesthesia-induced stress response and reduce anesthetic drugs. Its different site of action compared to other sedatives implies a different analgesic mechanism.
This study compared the analgesic efficacy of preoperative oral gabapentin with and without dexmedetomidine intravenous infusion in patients undergoing modified radical mastectomy under general anesthesia (GA).
2. METHODOLOGY
This randomized, double-blind clinical trial included 60 patients scheduled for modified radical mastectomy (MRM) under GA at the National Cancer Institute from February to August 2021. The study was approved by the Ethical Committee of the anesthesia department of Kasr El-Aini Hospital. All patients provided written informed consent to participate in the study.
The inclusion criteria were females aged 18 to 65 years, ASA I or II, body mass index (BMI) 20 to 40 kg/m2, and undergoing MRM under GA. Patients with known sensitivity or contraindication to study drugs, a history of psychological disorders, chronic pain, sympathetic disorders, significant liver insufficiency, severe respiratory diseases, or those receiving medications that could result in tolerance to opioids or medicines for cancer pain were excluded from the study.
The participants were randomly allocated to one of two equal groups using computer-generated random numbers (www.Random.org). Group G (n = 30) received oral gabapentin 600 mg (Gabapentin capsules 300 mg, Neurontin; Pfizer, Cairo, Egypt) one hour before surgery. Then, the patients received 50 mL of normal saline intravenously over 10 min just before induction of anesthesia, followed by continuous intraoperative infusion of normal saline at a rate of 10 mL/hour until skin closure. Group DG (n = 30) received 600 mg of gabapentin one hour before surgery. Then, the patients received a loading dose of 1 µg/kg of dexmedetomidine (DEX) in 50 mL of normal saline intravenously over 10 min just before induction of anesthesia. This was followed by a continuous intraoperative infusion of DEX diluted in normal saline at 0.5 µg/kg/hour until skin closure. All patients were monitored for vital signs during intravenous DEX administration.
Both patients and anesthesiologists were blinded to the nature of the administered intravenous solutions prepared by an anesthesiologist with no other role in the study. The investigators collecting intra- and postoperative data were unaware of group allocation. The patients were instructed about using the visual analog score of pain (VAS; 0 = no pain and 10 = worst pain imaginable).
2.1. Anesthetic Management
Preoperative midazolam 0.02 mg/kg IV was administered 30 min before surgery. The patients were monitored continuously using electrocardiography, non-invasive blood pressure, peripheral oxygen saturation, and end-tidal carbon dioxide (Datex-Ohmeda S5 anesthesia monitor, model no: USE1913A). The heart rate (HR), mean arterial blood pressure (MAP), and oxygen saturation were monitored after the induction of anesthesia, with surgical incision, and at 15-minute intervals intraoperatively.
GA was induced using fentanyl 2 μg/kg and propofol 2 mg/kg. Tracheal intubation was facilitated by atracurium 0.5 mg/kg. Anaesthesia was maintained with inhaled sevoflurane in oxygen-enriched air (FiO2 = 0.5) and top-up doses of atracurium (0.1 mg/kg) as required. The patients were mechanically ventilated to keep end-tidal CO2 within the 30-35 mmHg range. All patients received 1 gm of IV paracetamol. The total intraoperative fentanyl consumption was recorded. Bispectral index (BIS) was used to monitor the depth of anesthesia, with target BIS values from 40 to 60 because all the study drugs synergize with inhaled anesthesia.
Ringer acetate was infused to replace any fluid deficit, maintenance, and losses. Hypotension was defined as MBP below 60 mmHg or 70% from baseline. Hypotension episodes were treated with ringer acetate boluses and/or 5 mg ephedrine in incremental doses to maintain MAP above 70 mmHg. Additional bolus doses of fentanyl 0.5 µg/kg were given if the MAP or HR rose above 20% of baseline values. At the end of surgery, residual neuromuscular blockade was reversed by neostigmine 0.05 mg/kg and atropine 0.02 mg/kg. Extubation was performed after complete recovery of the airway reflexes.
In the PACU, the patients were monitored for MBP, HR, and VAS pain scores immediately on arrival and at 2, 6, 12, 18, and 24 h postoperatively. Paracetamol 1 g IV was administered every 8 h. Rescue analgesia was provided as 3 mg IV boluses of morphine when the pain score was >3 with a maximum allowed daily dose of 0.5 mg/kg/24 h. The time to first rescue analgesia and the total amount of morphine consumption were recorded. Side effects, including nausea, vomiting, sedation, hallucination, and respiratory depression, were recorded. Moderate or severe postoperative nausea and vomiting were treated with 0.1 mg/kg of IV ondansetron. Sedation was assessed and scored according to Ramsay score.
The primary outcome measure was the duration of analgesia, defined as the time from the end of surgery to the first rescue analgesia. The secondary outcomes were intraoperative fentanyl consumption, postoperative morphine consumption, pain intensity, and possible complications.
2.2. Sample size
Based on the previous work by Grover et al. (2009), who reported the mean duration time of first rescue analgesia was 90 ± 61.1 min, and Alzeftawy & Elsheikh (2015), who reported 125 ± 25.7 min for DEX infusion. Using a power 80% and 5% significance level, 30 patients in each group were sufficient.16,17 The sample size was calculated using the G*Power program (University of Düsseldorf, Düsseldorf, Germany).
2.3. Statistical methods
Statistical analysis was done using IBM© SPSS© Statistics version 22 (IBM© Corp., Armonk, NY, USA). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test was used to examine the relation between qualitative variables. For quantitative data, comparison between the two groups was made using an independent sample t-test or Mann-Whitney test. A P < 0.05 was considered significant.
3. RESULTS
As shown in Figure 1, 76 patients were assessed for eligibility, 11 did not meet the inclusion criteria, and five refused to participate. The results are presented for the remaining 60 patients. There were no significant differences between the two studied groups regarding the baseline characteristics and duration of surgery (Table 1).
Figure 1: CONSORT flow diagram
| Table 1: Baseline characteristics and duration of surgery in the two groups | |||
| Variables | Group G
(n = 30) |
Group DG
(n = 30) |
P-value |
| Age (years) | 39.0 ± 12.3 | 35.9 ± 9.8 | 0.295 |
| Weight (kg) | 75.8 ± 10.0 | 74.7 ± 6.6 | 0.617 |
| Height (cm) | 163 ± 9 | 162 ± 8 | 0.745 |
| Body mass index (kg/m2) | 28.5 ± 4.4 | 28.4 ± 3.3 | 0.860 |
| ASA physical status (I/II) | 24/6 | 27/3 | 0.278 |
| Duration of surgery (min.) | 73 ± 11 | 72 ± 12 | 0.664 |
| Data expressed as mean ± SD; ASA: American Society of Anesthesiology | |||
The time from skin closure to extubation and duration of postoperative analgesia were significantly longer in the Group DG compared to the Group D. Also, significantly higher number of patients required intraoperative fentanyl (P = 0.001) in the Group G. The total intraoperative fentanyl consumption was significantly higher in the Group G compared to the DG group (P < 0.001). The two groups had no significant difference in the number of patients who requested postoperative morphine (P = 0.405). Those who needed morphine received a single dose of 3 mg. VAS scores at rest and with movement were significantly lower in the Group DG during the postoperative period (Table 3).
| Table 2: Comparative intra- and postoperative analgesic profile of the two groups | |||
| Parameters | Group G
(n = 30) |
Group DG
(n = 30) |
P-value |
| Time from skin closure to extubation (min.) | 7.0 ± 1.2 | 9.4 ± 1.1 | < 0.001 |
| Duration of analgesia (min.) | 288 ± 38 | 545 ± 49 | < 0.001 |
| Number of patients requiring Fentanyl | 19 (63.3%) | 6 (20.0%) | 0.001 |
| Total fentanyl consumption (µg) | 41.6 ± 3.4 | 30.8 ± 2.0 | < 0.001 |
| Number of patients requiring morphine | 11 (36.7%) | 8 (26.7%) | 0.405 |
| Data expressed as mean ± SD or frequency (%) | |||
| Table 3: Comparative postoperative VAS scores at rest and with movement | |||
| Time | Group G
(n = 30) |
Group DG
(n = 30) |
P-value |
| At Rest | |||
| · Immediate | 2 (2-2) | 1 (1-1) | < 0.001 |
| · After 2 h | 2 (2-2) | 1 (1-1) | < 0.001 |
| · After 6 h | 3 (2-5) | 2 (2-2) | < 0.001 |
| · After12 h | 3 (2-3) | 2 (2-2) | < 0.001 |
| · After 18 h | 1 (1-1) | 1 (1-1) | < 0.001 |
| · After 24 h | 1 (1-1) | 0 (0-0) | < 0.001 |
| With movement | |||
| · Immediate | 2 (2-2) | 1 (1-1) | < 0.001 |
| · After 2 h | 2 (2-2) | 1 (1-1) | < 0.001 |
| · After 6 h | 3 (2-5) | 2 (2-2) | < 0.001 |
| · After12 h | 3 (3-4) | 2 (2-2) | < 0.001 |
| · After 18 h | 2 (1-2) | 1 (1-1) | < 0.001 |
| · After 24 h | 2 (1-2) | 1 (1-1) | < 0.001 |
| Data expressed as median (interquartile range) | |||
The MAP showed modest changes during intra- and postoperative periods in the two studied groups within the clinically accepted range. Preoperative MAP was comparable, while MAP was significantly lower in the Group DG from the induction of anesthesia till the end of surgery. MAP was comparable between the two groups at the immediate postoperative period (Table 4), with lower values after 2, 12, and 24 h.
| Table 4: Changes in mean arterial pressure during the intraoperative and postoperative periods | |||
| Time | Group G
(n = 30) |
Group DG
(n = 30) |
p-value |
| Preoperative | 78 ± 5 | 79 ± 5 | 0.442 |
| · Post-induction | 68 ± 4 | 64 ± 4 | < 0.001 |
| · With incision | 70 ± 4 | 66 ± 5 | 0.001 |
| Intraoperative | |||
| · After 15 mins | 71 ± 4 | 67 ± 4 | < 0.001 |
| · After 30 mins | 88 ± 15 | 77 ± 16 | 0.008 |
| · After 60 mins | 81 ± 8 | 71 ± 4 | < 0.001 |
| Postoperative | |||
| · Immediate | 85 ± 3 | 85 ± 4 | 0.888 |
| · After 2 h | 88 ± 4 | 86 ± 4 | 0.031 |
| · After 6 h | 92 ± 4 | 90 ± 4 | 0.070 |
| · After12 h | 94 ± 4 | 92 ± 4 | 0.026 |
| · After 18 h | 94 ± 6 | 93 ± 4 | 0.471 |
| · After 24 h | 92 ± 3 | 90 ± 3 | 0.026 |
| Data expressed as mean ± SD | |||
The heart rate changed slightly in the two groups and remained within the clinically accepted range. Preoperative HR was comparable, while HR was significantly lower in the Group DG from the induction of anesthesia till the end of surgery. The HR was comparable between the two groups during the whole postoperative period (Table 5).
| Table 5: Comparative heart rates during the intraoperative and postoperative periods | |||
| Time | Group G
(n = 30) |
Group DG
(n = 30) |
P - value |
| Preoperative | 74 ± 7 | 73 ± 5 | 0.527 |
| · Post-induction | 63 ± 4 | 59 ± 4 | < 0.001 |
| · With incision | 65 ± 5 | 59 ± 5 | < 0.001 |
| Intraoperative | |||
| · After 15 mins | 66 ± 4 | 62 ± 4 | < 0.001 |
| · After 30 mins | 82 ± 15 | 72 ± 16 | 0.015 |
| · After 60 mins | 75 ± 8 | 68 ± 4 | < 0.001 |
| Postoperative | |||
| Immediate | 66 ± 4 | 65 ± 4 | 0.115 |
| · After 2 h | 69 ± 4 | 68 ± 4 | 0.337 |
| · After 6 h | 74 ± 4 | 72 ± 4 | 0.058 |
| · After12 h | 76 ± 4 | 74 ± 4 | 0.058 |
| · After 18 h | 77 ± 4 | 76 ± 3 | 0.337 |
| · After 24 h | 74 ± 3 | 73 ± 3 | 0.202 |
| Data expressed as mean ± SD | |||
The sedation score was significantly higher in the DG group up to 12 h postoperatively compared to the G group. Then, the sedation scores were comparable after 18 and 24 h (Table 6). Postoperative nausea and vomiting were observed in 9 patients (30%) of the Group G and 6 (20%) of the Group DG (P = 0.371).
| Table 6: Comparative sedation scores during the postoperative period | |||
| Group G
(n = 30) |
Group DG
(n = 30) |
P-value | |
| Immediate | 2 (1-2) | 4 (3-4) | < 0.001 |
| After 2 h | 2 (1-2) | 4 (3-4) | < 0.001 |
| After 6 h | 2 (1-2) | 3 (2-3) | < 0.001 |
| After12 h | 2 (1-2) | 3 (2-3) | < 0.001 |
| After 18 h | 2 (1-2) | 2 (1-2) | 0.253 |
| After 24 h | 1 (1-2) | 2 (1-2) | 0.382 |
| Data expressed as median (interquartile range) | |||
4. DISCUSSION
This study demonstrated that adding intravenous DEX to preoperative gabapentin 600 mg improved the analgesic profile in patients subjected to MRM. The combination of DEX and gabapentin was associated with a longer duration of analgesia, lower pain intensity at rest and movement, and lower intraoperative fentanyl consumption compared to gabapentin only. Also, the sedation score was significantly higher in the DG group. Postoperative morphine consumption did not change with the addition of DEX to gabapentin. However, patients who required morphine in both groups received only a single dose of 3 mg throughout the 24 postoperative hours. Both groups were hemodynamically stable, with limited postoperative nausea and vomiting cases.
To date, there is no consensus on the best analgesic option after MRM that can alleviate acute pain and prevent the development of chronic postmastectomy pain. It is believed that despite the advancement of pain control techniques, nearly half of the patients still have significant pain after breast cancer surgery.18 This study aimed to test an opioid-sparing, preemptive, multimodal approach for postoperative analgesia following MRM using gabapentin and DEX.
Gabapentin and DEX are offered as effective agents for pain reduction after surgery. Zoroufchi et al. compared both drugs in laparoscopic cholecystectomy patients19 They found DEX more effective than gabapentin in pain reduction and better sedation during and after surgery. A recent prospective placebo-controlled study evaluated the gabapentin/DEX combination in patients undergoing MRM. Preoperative oral gabapentin 400 mg plus DEX infusion was associated with lower pain scores and reduced intraoperative fentanyl and postoperative morphine consumption compared to placebo.20
Preemptive analgesia (PA) is an antinociceptive treatment that blocks central and peripheral sensitization caused by surgical incisions. In addition to controlling acute postoperative pain, PA aims to prevent chronic neuropathic pain.21 A network meta-analysis compared 19 preemptive analgesia regimens regarding postoperative pain intensity and opioid consumption, and PONV. Compared with placebo, pain intensity was reduced in 10, and opioid consumption was decreased in 8 of the 19 regimens.22 The PROSPECT Working Group has recently recommended preoperative gabapentin,23 which was associated with reducing postoperative pain and morphine consumption after breast surgery.24,25
Previous studies have shown that preemptive gabapentin reduces postoperative pain and opioid consumption.8,10,26 A randomized, double-blind study found that preemptive oral gabapentin 600 mg significantly reduced postoperative pain, analgesic rescue requirements, and PONV in patients subjected to abdominal hysterectomy.8 Another study reported similar findings after oral gabapentin 1200 mg or placebo two hours before abdominal hysterectomy.9 A systematic review of 6 studies assessed the analgesic effect of gabapentin or pregabalin in patients undergoing anterior cruciate ligament reconstruction. Three studies showed that gabapentin significantly decreased pain scores and opioid consumption compared to controls.27 Preoperative gabapentin 600 mg did not reduce postoperative pain but decreased morphine consumption after video-assisted thoracoscopic surgery.28 In a meta-analysis of 9 RCTs, Jiang et al. demonstrated a reduction of morphine consumption after preoperative oral administration of gabapentin in breast cancer surgery.25
The mechanism of action of gabapentin is not fully understood. Despite its structural similarity to gamma-aminobutyric acid (GABA), it does not act directly on the GABA receptor.29 It may exert its effect through the N-methyl-D-aspartate (NMDA) neurotransmitter.30
Perioperative multimodal opioid-sparing analgesic regimens are considered the best options for pain relief following breast surgical procedures.31 The pharmacodynamic profile of DEX appoints the drug as a potential adjunct to enhance the non-opioid analgesic efficacy of preemptive gabapentin. It is a highly selective α-2-adrenoceptor (α-2AR) agonist with sedative, anxiolytic, and analgesic effects.32 Its sedative and sympatholytic effects are mediated through the activation of α-2AR of the locus coeruleus and subsequent inhibition of ascending noradrenergic pathways. However, the mechanism of its analgesic activity has not been fully explained. A potential mechanism is the activation of potassium channels, resulting in membrane hyperpolarization of nociceptive neurons. Another mechanism is that alpha-2AR activation may induce calcium conductance modulation, leading to reduced neurotransmitter release.
Intraoperative DEX was found to reduce postoperative pain and opioid consumption. In patients undergoing laparoscopic cholecystectomy, intraoperative DEX infusion decreased postoperative pain and morphine consumption and prolonged the duration of postoperative analgesia.32 A systematic review of 18 RCTs reported reduced intraoperative and postoperative opioid consumption and pain intensity in adult patients.33
A meta-analysis of 12 studies evaluated the analgesic efficacy of DEX as an adjuvant in cases of breast cancer surgery. Pooled analysis demonstrated prolonged analgesia, lower pain intensity, and reduced postoperative opioids and intraoperative fentanyl.34 A recent study evaluated the intraoperative analgesic efficacy of DEX as an adjuvant to peripheral nerve block in real time using non-invasive nociception monitoring. Intravenous DEX infusion offered rapid and proper intraoperative and postoperative analgesia with hemodynamic stability and without respiratory depression.35
5. CONCLUSION
In conclusion, the analgesic effect of a combination of preoperative oral gabapentin plus perioperative dexmedetomidine infusion is superior to that of gabapentin alone in patients undergoing MRM for breast cancer. The combined regimen was associated with prolonged postoperative analgesia, lower pain intensity, lower intraoperative fentanyl consumption, and better sedation. Postoperative morphine consumption was limited with gabapentin and the combined regimen. Both regimens were characterized by hemodynamic stability and minimal adverse effects.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
AS: Corresponding author, Final Approval
AZ: Scientific literature search, Data collection, Manuscript writing, Editing, Final Approval
MS: Scientific literature search
MB: Conduct of study
REFERENCES
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-49. PubMed DOI: 3322/caac.21660
- Ibrahim AS, Khaled HM, Mikhail NN, Baraka H, Kamel H. Cancer incidence in Egypt: results of the national population-based cancer registry program. J Cancer Epidemiol. 2014;2014:437971. PubMed DOI: 1155/2014/437971
- Gupta K, Srikanth K, Girdhar KK, Chan V. Analgesic efficacy of ultrasound-guided paravertebral block versus serratus plane block for modified radical mastectomy: a randomised, controlled trial. Indian J Anaesth. 2017;61(5):381-6. PubMed DOI: 4103/ija.IJA_62_17
- Alves Nogueira Fabro E, Bergmann A, do Amaral E Silva B, Padula Ribeiro AC, de Souza Abrahão K, da Costa Leite Ferreira MG, et al. Post-mastectomy pain syndrome: incidence and risks. Breast. 2012;21(3):321-5. PubMed DOI: 1016/j.breast.2012.01.019
- Tait RC, Zoberi K, Ferguson M, Levenhagen K, Luebbert RA, Rowland K, et al. Persistent post-mastectomy pain: risk factors and current approaches to treatment. J Pain. 2018;19(12):1367-83. PubMed DOI: 1016/j.jpain.2018.06.002
- Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019;74(5):651-62. PubMed DOI: 1111/anae.14582
- Koepke EJ, Manning EL, Miller TE, Ganesh A, Williams DGA, Manning MW. The rising tide of opioid use and abuse: the role of the anesthesiologist. Perioper Med. 2018;7:16. PubMed DOI: 1186/s13741-018-0097-4
- Ajori L, Nazari L, Mazloomfard MM, Amiri Z. Effects of gabapentin on postoperative pain, nausea and vomiting after abdominal hysterectomy: a double blind randomized clinical trial. Arch Gynecol Obstet. 2012;285(3):677-82. PubMed DOI: 1007/s00404-011-2023-6
- Frouzanfard F, Fazel MR, Abolhasani A, Fakharian E, Mousavi G, Moravveji A. Effects of gabapentin on pain and opioid consumption after abdominal hysterectomy. Pain Res Manag. 2018;2018:94-6. PubMed DOI: 1155/2013/787401
- Wang J, Fu G, Liu J, Yu Y, Wang N. Effect of preoperative gabapentin after transurethral prostate resection under general anesthesia: a randomized double-blind, placebo-controlled trial. Saudi Med J. 2020;41(6):640-4. PubMed DOI: 15537/smj.2020.6.25132
- Kissin I. Preemptive analgesia. Anesthesiology. 2000;93(4):1138-43. PubMed DOI: 1097/00000542-200010000-00040
- Aglio LS, Abd-El-Barr MM, Orhurhu V, Kim GY, Zhou J, Gugino LD, et al. Preemptive analgesia for postoperative pain relief in thoracolumbosacral spine operations: a double-blind, placebo-controlled randomized trial. J Neurosurg Spine. 2018;29(6):647-53. PubMed DOI: 3171/2018.5.SPINE171380
- Helander EM, Menard BL, Harmon CM, Homra BK, Allain AV, Bordelon GJ, et al. Multimodal analgesia, current concepts, and acute pain considerations. Curr Pain Headache Rep. 2017;21(1):3. PubMed DOI: 1007/s11916-017-0607-y
- Ni JM, Zhu X, Wang P. Effectiveness of combined pregabalin and celecoxib for treatment of acute postoperative pain: a meta-analysis and systematic review. Medicine. 2022;101(3):e29356. PubMed DOI: 1097/MD.0000000000032080
- Chrysostomou C, Schmitt CG. Dexmedetomidine: sedation, analgesia and beyond. Expert Opin Drug Metab Toxicol. 2008;4(5):619-27. PubMed DOI: 1517/17425255.4.5.619
- Grover D, Yang J, Ford D, Tavaré S, Tower J. Simultaneous tracking of movement and gene expression in multiple Drosophila melanogaster flies using GFP and DsRED fluorescent reporter transgenes. BMC Res Notes. 2009;2:58. PubMed DOI: 1186/1756-0500-2-58
- Kim WH, Cho D, Lee B, Song JJ, Shin TJ. Changes in brain activation during sedation induced by dexmedetomidine. J Int Med Res. 2017;45(3):1158-66. PubMed DOI: 1177/0300060517705477
- Beguinot M, Monrigal E, Kwiatkowski F, Ginzac A, Joly D, Gayraud G, et al. Continuous wound infiltration with ropivacaine after mastectomy: a randomized controlled trial. J Surg Res. 2020;254:318-26. PubMed DOI: 1016/j.jss.2020.05.006
- Zoroufchi BH, Zangian H, Abdollahpour A. Examination of the sedative and analgesic effects of gabapentin and dexmedetomidine in patients undergoing laparoscopic cholecystectomy surgery: a randomized controlled trial. J Family Med Prim Care. 2020;9(2):1042-7. PubMed DOI: 4103/jfmpc.jfmpc_890_19
- Abdallah NM, Bakeer AH. A multimodal analgesic protocol with gabapentin-dexmedetomidine for post-operative pain management after modified radical mastectomy surgery: a randomized placebo-controlled study. Open Access Maced J Med Sci. 2022;10(F):1453-8. DOI: 3889/oamjms.2022.9698
- Vadivelu N, Mitra S, Schermer E, Kodumudi V, Kaye AD, Urman RD. Preventive analgesia for postoperative pain control: a broader concept. Local Reg Anesth. 2014;7:17-22. PubMed DOI: 2147/LRA.S62160
- Xuan C, Yan W, Wang D, Li C, Ma H, Mueller A, et al. Efficacy of preemptive analgesia treatments for the management of postoperative pain: a network meta-analysis. Br J Anaesth. 2022;129(6):946-58. PubMed DOI: 1016/j.bja.2022.08.038
- Jacobs A, Lemoine A, Joshi GP, Van de Velde M, Bonnet F, PROSPECT Working Group. PROSPECT guideline for oncological breast surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2020;75(5):664-73. PubMed DOI: 1111/anae.14964
- Rai AS, Khan JS, Dhaliwal J, Busse JW, Choi S, Devereaux PJ, et al. Preoperative pregabalin or gabapentin for acute and chronic postoperative pain among patients undergoing breast cancer surgery: a systematic review and meta-analysis of randomized controlled trials. J Plast Reconstr Aesthet Surg. 2017;70(10):1317-28. PubMed DOI: 1016/j.bjps.2017.05.054
- Jiang Y, Li J, Lin H, Huang Q, Wang T, Zhang S, et al. The efficacy of gabapentin in reducing pain intensity and morphine consumption after breast cancer surgery: a meta-analysis. Medicine. 2018;97(22):e11581. PubMed DOI: 1097/MD.0000000000011581
- Mardani-Kivi M, Karimi Mobarakeh M, Keyhani S, Haghighi M, Hashemi-Motlagh K, Saheb-Ekhtiari K. Arthroscopic Bankart surgery: does gabapentin reduce postoperative pain and opioid consumption? A triple-blinded randomized clinical trial. Orthop Traumatol Surg Res. 2016;102(4):549-53. PubMed DOI: 1016/j.otsr.2016.01.028
- Blaber OK, Aman ZS, DePhillipo NN, LaPrade RF, Dekker TJ. Perioperative gabapentin may reduce opioid requirement for early postoperative pain in patients undergoing anterior cruciate ligament reconstruction: a systematic review of randomized controlled trials. Arthroscopy. 2022;38(5):S0749-8063(22)00768-X. PubMed DOI: 1016/j.arthro.2022.11.024
- Shamsaddini M, Abrishami R, Farzanegan B, Baniasadi S. Effectiveness of short-term use of gabapentin as pre-emptive analgesia in reducing pain after video assisted thoracoscopic surgery. Tanaffos. 2022;21(1):90-5. PubMed
- Tan M, Law LS, Gan TJ. Optimizing pain management to facilitate enhanced recovery after surgery pathways. Can J Anaesth. 2015;62(2):203-18. PubMed DOI: 1007/s12630-014-0275-x
- Kier LB, Dowd CS. The chemistry and physics of drugs used in anesthesia. 2nd ed. Park Ridge: American Association of Nurse Anesthetists; 2014.
- Afonso AM, Newman MI, Seeley N, Hutchins J, Smith KL, Mena G, et al. Multimodal analgesia in breast surgical procedures: technical and pharmacological considerations for liposomal bupivacaine use. Plast Reconstr Surg Glob Open. 2017;5(1):e1480. PubMed DOI: 1097/GOX.0000000000001480
- Bielka K, Kuchyn I, Babych V, Martycshenko K, Inozemtsev O. Dexmedetomidine infusion as an analgesic adjuvant during laparoscopic cholecystectomy: a randomized controlled trial. BMC Anesthesiol. 2018;18:44. PubMed DOI: 1186/s12871-018-0508-6
- Le Bot A, Michelet D, Hilly J, Maesani M, Dilly MP, Brasher C, et al. Efficacy of intraoperative dexmedetomidine compared with placebo for surgery in adults: a meta-analysis of published studies. Minerva Anestesiol. 2015;81:1105-17. PubMed
- Liu C, Wang W, Shan Z, Zhang H, Yan Q. Dexmedetomidine as an adjuvant for patients undergoing breast cancer surgery. Medicine. 2020;99:e23667. PubMed DOI: 1097/MD.0000000000023667
- Wang X, Zhang S, Wang C, Huang Y, Wu H, Zhao G, et al. Real-time evaluation of the independent analgesic efficacy of dexmedetomidine. BMC Anesthesiol. 2023;23:68. PubMed DOI: 10.1186/s12871-023-02022-2