Astrandaya Ajie 1 , Ahmad Umar Alfaruq 2 , Lukman Hakim 3
Author affiliations:
Anesthesia in patients with decreased cardiac function is a challenge for anaesthesiologists, as patients with poor cardiac function are more prone to hemodynamic instability. Anaesthesiologists must conduct a thorough evaluation and select the most suitable anaesthetic management. In patients with impaired cardiac function undergoing head and neck surgeries, regional anaesthesia with a peripheral nerve block is often preferred. A 59-year-old male patient with a history of heart failure, coronary artery disease (CAD), and type 2 diabetes mellitus (T2DM) was diagnosed with a mentum abscess. Echocardiography revealed a low systolic ejection fraction (LVEF 19%). For this patient, debridement of the mentum was planned, using a combination of mental nerve block and superficial cervical plexus block for anaesthesia. No complications or hemodynamic instability were observed during the perioperative or postoperative periods. Regional anaesthesia was chosen due to its lower risk of instability compared to general anaesthesia in patients with poor heart function. The surgical area involved the mentum and neck, so a combination of mental nerve block and cervical plexus block was appropriate. Since debridement requires rapid onset and adequate duration of anaesthesia, a mix of 2% lidocaine and 0.75% ropivacaine was used.
Abbreviations: CAD: coronary artery disease, EF: Ejection fraction, HF: Heart failure, MACCE: major adverse cardiovascular and cerebrovascular events, MI: myocardial infarction, PCI: percutaneous coronary intervention, T2DM: type 2 diabetes mellitus,
Keywords: Decreased Cardiac Function; Low Ejection Fraction; Mental Nerve Block; Cervical Plexus Block; Regional Anesthesia
Citation: Ajie A, Alfaruq AU, Hakim L. Successful use of combined mental nerve block and superficial cervical plexus block for mental debridement in a patient with impaired cardiac function. Anaesth. pain intensive care 2025;29(5):418-423. DOI: 10.35975/apic.v29i5.2866
Received: April 16, 2025; Revised: June 14, 2025; Accepted: June 17, 2025
Evaluation of cardiac function, is one of the parameters that must be considered by every anesthesiologist before starting surgery. One of the most important parameters for assessing cardiac function is the ejection fraction (EF). EF is a quantitative assessment expressed as a percentage of the difference between the blood volume in the heart chamber at the end of relaxation and the blood volume in the heart chamber at the end of contraction, then divided by the blood volume at the end of relaxation.1 Patients with low ejection fraction (EF) (less than 40%) are a parameter of decreased cardiac function. Patients with decreased cardiac function have a high risk of hemodynamic instability and major adverse cardiovascular and cerebrovascular events (MACCE) during the perioperative and postoperative periods.
MACCE classification based on its findings is divided into 3 parts, namely 3-point MACCE, 4-point MACCE and 5-point MACCE. The 5-point MACCE consists of various components of total death, myocardial infarction (MI), cardiac revascularization, stroke, and hospitalization due to heart failure (HF), while the 4-point consists of cardiovascular (CV) death, non-fatal MI, non-fatal stroke, unstable angina (UA) requiring hospitalization and 3-point MACCE is CV death, non-fatal MI, or non-fatal stroke.2 Cardiac complications can lead to disability and death after surgery. Preoperative cardiac risk assessment provides an important opportunity to reduce risk, optimize the use of limited healthcare resources, and assess the quality of care. The Revised Cardiac Risk Index (RCRI) is used as a tool to measure risk in noncardiac procedures. This index shows six predictive factors listed in Box 1 that have been shown to be effective in differentiating risk levels in various noncardiac surgical procedures.3
A study by Smilowitz NR, et al. stated that more than 300 million patients with non-cardiac surgery experience MACCE.4 Therefore, anesthesiologists are required to provide safe and quality care in the operating room for patients with decreased heart function. Patients with low EF require early identification of risk factors, preoperative evaluation and optimization, appropriate medical therapy, adequate monitoring, and appropriate anaesthetic techniques and drugs.5
Regional anesthesia techniques are preferred in patients with decreased heart function compared to general anesthesia. This is because in patients with low heart function who undergo general anesthesia there is a high risk of worsening inadequate cardiac output, which was previously low, so that complications can occur during perioperative and postoperative. One of the regional anesthesia techniques that tends to be safe in patients with decreased heart function with surgery in the head and neck area is peripheral nerve block. The goals of anesthesia in patients with low cardiac function include avoiding drug-induced myocardial depression, preventing arrhythmias, and maintaining adequate cardiac output.6,7 In this case report, we discuss the peripheral nerve block technique using a combination of mental nerve block with superficial cervical plexus block for mental debridement in a patient with decreased cardiac function.
A 59-year-old man was referred by the internal medicine department to the surgical department of Sultan Agung Islamic Hospital, with complaints of an abscess at the chin. The patient was diagnosed with a chin abscess and was planned for debridement. He had a history of heart failure, coronary artery disease 3 vessel disease (CAD3VD) post percutaneous coronary intervention (PCI), and type 2 diabetes mellitus (T2DM). Based on the MACCE classification, this patient had a history of revascularization, heart failure, and MI. The Revised Cardiac Risk Index (RCRI) in this patient was 2 points with a risk of major cardiac events of 10.1%.
Physical examination found him cooperative, with blood pressure (BP) 100/65 mmHg, pulse rate (HR) 63 x/min, respiratory rate (RR) 21 breaths/min, temperature 36.3° C, and peripheral oxygen saturation (SpO2) 99%. The patient's nutritional status was classified as normal with a body weight of 50 kg and a height of 158 cm and a BMI of 20 kg/m2. Examination of the local status found pus (+), erosion (+), yellowish crust (+), and inactive bleeding (+) in the mentum region (Figure 1). Glycemic status in this patient is controlled with a random blood sugar level of 178 mg/dL. The results of preoperative laboratory investigations showed azotemia with urea blood levels of 98 mg/dL and creatinine 1.66 mg/dL.

Figure 1: Local status of the lesion
The results of the chest x-ray postero-anterior (PA) examination of the heart showed a picture of the apex of the heart widening latero-caudal and a flattened waist of the heart; while in the lungs there was an increase in bronchovascular markings, spots in the lower middle field of the right lung, and the middle of the left lung. The impression of the chest x-ray examination results was cardiomegaly and a picture of bronchopneumonia. Based on the results of the echocardiography examination, there was dilation of the four heart chambers, severe decreased left ventricular (LV) systolic function with an LV ejection fraction (LVEF) of 19%, severe diastolic dysfunction, moderate mitral regurgitation (MR), and tricuspid regurgitation (TR). The results of the pre-operative electrocardiography (ECG) showed a normosinus rhythm.
The patient was planned to undergo debridement of the mentum abscess with the regional peripheral nerve block technique. Pre-operative preparation was fasting for 6 hours with premedication of atropine sulphate (SA) 0.25 mg, metoclopramide 10 mg, ranitidine 50 mg, and dobutamine and norepinephrine (NE) infusions.
Patients with very low EF are at greater risk of hemodynamic instability, so the regional peripheral nerve block technique was chosen. In addition, because of the location of surgery in the mentum area, bilateral mental nerve block and bilateral superficial cervical plexus block could be performed. We used a combination of 1 mL lidocaine 2% plus 2 mL ropivacaine, for each side; while for SCPB we used a combination of 2% lidocaine 1 mL and 0.75% ropivacaine 3 mL on the superior and medial branches bilaterally.
The anesthetic effect was obtained after approximately 1 min of induction. During the procedure, blood pressure dropped to 78/53 mmHg; support was given with dobutamine 5 µg/kg/min. After providing support with dobutamine, the patient's hemodynamics stabilized during the procedure. Post-surgery, the patient's hemodynamics were stable, and there were no complaints or symptoms of acute postoperative toxicity.
Based on the dermatomes (Figure 2),
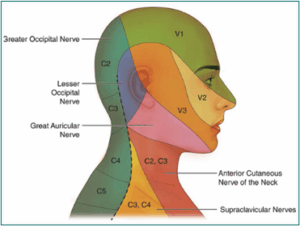
Figure 2: Dermatomes of the Head and Neck Area.8,9
the mental/submandibular area is innervated by the mental nerve, a branch of the mandibular nerve (n. V3) and has 2 rami, namely the right and left rami, so in this case a mental nerve block was performed as the scope of the operation area. In this case report, a cervical plexus block (C1-C4) was also performed to expand the operation area because debridement will be performed extensively to the anterior area of the neck (Figure 3-A).8,9
In patients with decreased heart function, the use of regional anesthesia is considered more than general anesthesia. This is because the heart function is very poor, so there is a high risk of hemodynamic instability. In this case, the patient did not experience hemodynamic instability and postoperative complications. During surgery, the patient experienced a decrease in blood pressure, but dobutamine support led to a rise in blood pressure and subsequent hemodynamic stabilization. In a previous case report of lip surgery, it was stated that the use of mental nerve blocks was proven to be safe, and there were no perioperative or postoperative complications. 10
The mental nerve is a terminal branch of the mandibular nerve, which is part of the fifth cranial nerve, the trigeminal nerve (Figure 3-B). The mental nerve innervates the ipsilateral side of the lower lip, the mucosa, and the skin of the chin. The mental nerve.
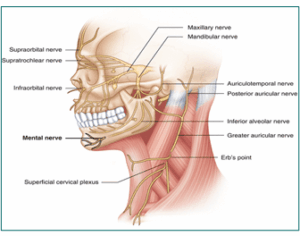
Figure 3-B: Anatomy of the Mental Nerve.11,12
leaves the mental foramen, which can be felt intraorally just caudal to the lower first and second premolars, midway between the teeth and the inferior mandibular border. The mental foramen can be located extra orally in the vertical plane with the ipsilateral pupil in the midline position. After the lips are inverted, the mental foramen can be reached intraorally by directing a 23-gauge needle with a 5 mL syringe attached to the buccal mucosa.13 To prevent nerve injury, it is advisable not to enter the mental foramen. Infiltration with 2-4 mL of anesthetic solution will be sufficient to produce effective analgesia of the lower lip and chin for surgical procedures. In this case, we used a combination of lidocaine, which has rapid onset and ropivacaine which has longer duration but has slower onset of action.14,15 This is done so that rapid analgesia occurs, and the duration of nerve blockade can be long enough. The time for analgesia to occur in the patient in this case report is about 1 min, with estimated duration of analgesia about 4-6 hours.
So far, this case report is the first successful use of mental nerve blockade in clinical practice in patients with very poor cardiac function for debridement surgery. A previous study reported the use of mental nerve blockade in lip surgery, but in that report the subject had good cardiac function.10 A similar case report reported that using regional block techniques, combined with sedation, minimized the risk of cardiovascular complications and airway obstruction, resulting in good outcomes in patients with cardiac dysfunction.16 Another study stated that bilateral mental nerve blocking is a safer and more effective alternative to general anesthesia in lower lip tumor resection, especially in elderly patients and those who have poor tolerance to general anesthesia as long as cervical node dissection is not required.17
In another study, peripheral nerve block significantly reduced perioperative complications in elderly patients with comorbidities compared with general anesthesia. This statement is consistent with the condition of the patients in this study. The authors stated that this technique provides effective analgesia while minimizing systemic effects, which is particularly beneficial for patients with cardiovascular risk.18
In addition, peripheral nerve block provides better postoperative care with excellent pain management, reduced nausea and vomiting and reduced dependence on medications. These factors collectively contribute to a shorter recovery. For example, in a case study of abdominal aortic aneurysm, thoracic spinal block was shown to be highly effective in postoperative recovery in a patient with severe COPD and ischemic heart disease.19 In another case, combined thoracic paravertebral and interscalene blocks facilitated the smooth performance of extensive breast surgery in another individual with multiple comorbidities.20
The choice of anesthetic technique is a challenge for anesthesiologists in cases of decreased cardiac function. In patients in this case report with decreased cardiac function, the use of peripheral nerve block using a combination of mental nerve block and superficial cervical plexus block has been proven safe, and there were no complications during perioperative or postoperative. Lastly, we try to aim not to take significant risks in straightforward procedures.
5. Acknowledgement
We would like to extend our sincere thanks to the multidisciplinary team involved in the patient's care, including the surgeon, anaesthesiologist, pain management specialists, and nursing staff. Their teamwork played a crucial role in delivering thorough care and enhancing pain management strategies. We also express our appreciation to the patient for her resilience and cooperation throughout her treatment, which greatly contributed to the positive results seen during her hospitalization.
6. Declaration of patient consent
The authors confirm that they have received all necessary patient consent forms. The patient has granted permission for his images and clinical information to be published in the journal. He is aware that his name and initials will not be disclosed, and efforts will be made to protect his identity; however, complete anonymity cannot be assured.
7. Financial support
No funding was received
8. Conflicts of interest
There were no conflict of interest.
9. Author contribution
AA: conceptualization, conduction of the study, writing - original draft, writing - review & editing
AUA: conduction of the study, writing - original draft, writing - review & editing
LH: writing - review & editing
Author affiliations:
- Astrandaya Ajie, Terboyo Kulon, Genuk, Semarang, Central Java, 50112. Indonesia; Email: ajieastrandaya@gmail.com
- Ahmad Umar Alfaruq, Terboyo Kulon, Genuk, Semarang, Central Java, 50112. Indonesia; Email: ahmadumaralfaruq@gmail.com
- Lukman Hakim, Terboyo Kulon, Genuk, Semarang, Central Java, 50112. Indonesia; Email: lukman20hkm@gmail.com
ABSTRACT
Anesthesia in patients with decreased cardiac function is a challenge for anaesthesiologists, as patients with poor cardiac function are more prone to hemodynamic instability. Anaesthesiologists must conduct a thorough evaluation and select the most suitable anaesthetic management. In patients with impaired cardiac function undergoing head and neck surgeries, regional anaesthesia with a peripheral nerve block is often preferred. A 59-year-old male patient with a history of heart failure, coronary artery disease (CAD), and type 2 diabetes mellitus (T2DM) was diagnosed with a mentum abscess. Echocardiography revealed a low systolic ejection fraction (LVEF 19%). For this patient, debridement of the mentum was planned, using a combination of mental nerve block and superficial cervical plexus block for anaesthesia. No complications or hemodynamic instability were observed during the perioperative or postoperative periods. Regional anaesthesia was chosen due to its lower risk of instability compared to general anaesthesia in patients with poor heart function. The surgical area involved the mentum and neck, so a combination of mental nerve block and cervical plexus block was appropriate. Since debridement requires rapid onset and adequate duration of anaesthesia, a mix of 2% lidocaine and 0.75% ropivacaine was used.
Abbreviations: CAD: coronary artery disease, EF: Ejection fraction, HF: Heart failure, MACCE: major adverse cardiovascular and cerebrovascular events, MI: myocardial infarction, PCI: percutaneous coronary intervention, T2DM: type 2 diabetes mellitus,
Keywords: Decreased Cardiac Function; Low Ejection Fraction; Mental Nerve Block; Cervical Plexus Block; Regional Anesthesia
Citation: Ajie A, Alfaruq AU, Hakim L. Successful use of combined mental nerve block and superficial cervical plexus block for mental debridement in a patient with impaired cardiac function. Anaesth. pain intensive care 2025;29(5):418-423. DOI: 10.35975/apic.v29i5.2866
Received: April 16, 2025; Revised: June 14, 2025; Accepted: June 17, 2025
1. INTRODUCTION
Evaluation of cardiac function, is one of the parameters that must be considered by every anesthesiologist before starting surgery. One of the most important parameters for assessing cardiac function is the ejection fraction (EF). EF is a quantitative assessment expressed as a percentage of the difference between the blood volume in the heart chamber at the end of relaxation and the blood volume in the heart chamber at the end of contraction, then divided by the blood volume at the end of relaxation.1 Patients with low ejection fraction (EF) (less than 40%) are a parameter of decreased cardiac function. Patients with decreased cardiac function have a high risk of hemodynamic instability and major adverse cardiovascular and cerebrovascular events (MACCE) during the perioperative and postoperative periods.
MACCE classification based on its findings is divided into 3 parts, namely 3-point MACCE, 4-point MACCE and 5-point MACCE. The 5-point MACCE consists of various components of total death, myocardial infarction (MI), cardiac revascularization, stroke, and hospitalization due to heart failure (HF), while the 4-point consists of cardiovascular (CV) death, non-fatal MI, non-fatal stroke, unstable angina (UA) requiring hospitalization and 3-point MACCE is CV death, non-fatal MI, or non-fatal stroke.2 Cardiac complications can lead to disability and death after surgery. Preoperative cardiac risk assessment provides an important opportunity to reduce risk, optimize the use of limited healthcare resources, and assess the quality of care. The Revised Cardiac Risk Index (RCRI) is used as a tool to measure risk in noncardiac procedures. This index shows six predictive factors listed in Box 1 that have been shown to be effective in differentiating risk levels in various noncardiac surgical procedures.3
A study by Smilowitz NR, et al. stated that more than 300 million patients with non-cardiac surgery experience MACCE.4 Therefore, anesthesiologists are required to provide safe and quality care in the operating room for patients with decreased heart function. Patients with low EF require early identification of risk factors, preoperative evaluation and optimization, appropriate medical therapy, adequate monitoring, and appropriate anaesthetic techniques and drugs.5
Regional anesthesia techniques are preferred in patients with decreased heart function compared to general anesthesia. This is because in patients with low heart function who undergo general anesthesia there is a high risk of worsening inadequate cardiac output, which was previously low, so that complications can occur during perioperative and postoperative. One of the regional anesthesia techniques that tends to be safe in patients with decreased heart function with surgery in the head and neck area is peripheral nerve block. The goals of anesthesia in patients with low cardiac function include avoiding drug-induced myocardial depression, preventing arrhythmias, and maintaining adequate cardiac output.6,7 In this case report, we discuss the peripheral nerve block technique using a combination of mental nerve block with superficial cervical plexus block for mental debridement in a patient with decreased cardiac function.
2. CASE REPORT
A 59-year-old man was referred by the internal medicine department to the surgical department of Sultan Agung Islamic Hospital, with complaints of an abscess at the chin. The patient was diagnosed with a chin abscess and was planned for debridement. He had a history of heart failure, coronary artery disease 3 vessel disease (CAD3VD) post percutaneous coronary intervention (PCI), and type 2 diabetes mellitus (T2DM). Based on the MACCE classification, this patient had a history of revascularization, heart failure, and MI. The Revised Cardiac Risk Index (RCRI) in this patient was 2 points with a risk of major cardiac events of 10.1%.
| Box 1: The Revised Cardiac Risk Index.3 | |
| Risk Factor | Definition |
| High-risk surgery | a. Intraperitoneal b. Intrathoracic c. Suprainguinal vascular |
| History of ischemic heart disease | a. History oof myocardial infarction b. History of positive exercise test c. Current chest pain due to myocardial ischemia d. ECG with pathologic Q waves |
| History of congestive heart failure | a. Pulmonary edema b. Bilateral rales or 53 gallop c. Paroxysmal nocturnal dyspnea d. X-ray showing pulmonary vascular redistribution |
| History of cerebrovascular disease |
a. Prior transient ischemic attack b. Stroke |
| Preoperative treatment with insulin | |
| Preoperative creatinine > 177 µmol/L | |
Physical examination found him cooperative, with blood pressure (BP) 100/65 mmHg, pulse rate (HR) 63 x/min, respiratory rate (RR) 21 breaths/min, temperature 36.3° C, and peripheral oxygen saturation (SpO2) 99%. The patient's nutritional status was classified as normal with a body weight of 50 kg and a height of 158 cm and a BMI of 20 kg/m2. Examination of the local status found pus (+), erosion (+), yellowish crust (+), and inactive bleeding (+) in the mentum region (Figure 1). Glycemic status in this patient is controlled with a random blood sugar level of 178 mg/dL. The results of preoperative laboratory investigations showed azotemia with urea blood levels of 98 mg/dL and creatinine 1.66 mg/dL.
Figure 1: Local status of the lesion
The results of the chest x-ray postero-anterior (PA) examination of the heart showed a picture of the apex of the heart widening latero-caudal and a flattened waist of the heart; while in the lungs there was an increase in bronchovascular markings, spots in the lower middle field of the right lung, and the middle of the left lung. The impression of the chest x-ray examination results was cardiomegaly and a picture of bronchopneumonia. Based on the results of the echocardiography examination, there was dilation of the four heart chambers, severe decreased left ventricular (LV) systolic function with an LV ejection fraction (LVEF) of 19%, severe diastolic dysfunction, moderate mitral regurgitation (MR), and tricuspid regurgitation (TR). The results of the pre-operative electrocardiography (ECG) showed a normosinus rhythm.
The patient was planned to undergo debridement of the mentum abscess with the regional peripheral nerve block technique. Pre-operative preparation was fasting for 6 hours with premedication of atropine sulphate (SA) 0.25 mg, metoclopramide 10 mg, ranitidine 50 mg, and dobutamine and norepinephrine (NE) infusions.
Patients with very low EF are at greater risk of hemodynamic instability, so the regional peripheral nerve block technique was chosen. In addition, because of the location of surgery in the mentum area, bilateral mental nerve block and bilateral superficial cervical plexus block could be performed. We used a combination of 1 mL lidocaine 2% plus 2 mL ropivacaine, for each side; while for SCPB we used a combination of 2% lidocaine 1 mL and 0.75% ropivacaine 3 mL on the superior and medial branches bilaterally.
The anesthetic effect was obtained after approximately 1 min of induction. During the procedure, blood pressure dropped to 78/53 mmHg; support was given with dobutamine 5 µg/kg/min. After providing support with dobutamine, the patient's hemodynamics stabilized during the procedure. Post-surgery, the patient's hemodynamics were stable, and there were no complaints or symptoms of acute postoperative toxicity.
3. DISCUSSION
Based on the dermatomes (Figure 2),
Figure 2: Dermatomes of the Head and Neck Area.8,9
the mental/submandibular area is innervated by the mental nerve, a branch of the mandibular nerve (n. V3) and has 2 rami, namely the right and left rami, so in this case a mental nerve block was performed as the scope of the operation area. In this case report, a cervical plexus block (C1-C4) was also performed to expand the operation area because debridement will be performed extensively to the anterior area of the neck (Figure 3-A).8,9
In patients with decreased heart function, the use of regional anesthesia is considered more than general anesthesia. This is because the heart function is very poor, so there is a high risk of hemodynamic instability. In this case, the patient did not experience hemodynamic instability and postoperative complications. During surgery, the patient experienced a decrease in blood pressure, but dobutamine support led to a rise in blood pressure and subsequent hemodynamic stabilization. In a previous case report of lip surgery, it was stated that the use of mental nerve blocks was proven to be safe, and there were no perioperative or postoperative complications. 10
The mental nerve is a terminal branch of the mandibular nerve, which is part of the fifth cranial nerve, the trigeminal nerve (Figure 3-B). The mental nerve innervates the ipsilateral side of the lower lip, the mucosa, and the skin of the chin. The mental nerve.
Figure 3-B: Anatomy of the Mental Nerve.11,12
leaves the mental foramen, which can be felt intraorally just caudal to the lower first and second premolars, midway between the teeth and the inferior mandibular border. The mental foramen can be located extra orally in the vertical plane with the ipsilateral pupil in the midline position. After the lips are inverted, the mental foramen can be reached intraorally by directing a 23-gauge needle with a 5 mL syringe attached to the buccal mucosa.13 To prevent nerve injury, it is advisable not to enter the mental foramen. Infiltration with 2-4 mL of anesthetic solution will be sufficient to produce effective analgesia of the lower lip and chin for surgical procedures. In this case, we used a combination of lidocaine, which has rapid onset and ropivacaine which has longer duration but has slower onset of action.14,15 This is done so that rapid analgesia occurs, and the duration of nerve blockade can be long enough. The time for analgesia to occur in the patient in this case report is about 1 min, with estimated duration of analgesia about 4-6 hours.
So far, this case report is the first successful use of mental nerve blockade in clinical practice in patients with very poor cardiac function for debridement surgery. A previous study reported the use of mental nerve blockade in lip surgery, but in that report the subject had good cardiac function.10 A similar case report reported that using regional block techniques, combined with sedation, minimized the risk of cardiovascular complications and airway obstruction, resulting in good outcomes in patients with cardiac dysfunction.16 Another study stated that bilateral mental nerve blocking is a safer and more effective alternative to general anesthesia in lower lip tumor resection, especially in elderly patients and those who have poor tolerance to general anesthesia as long as cervical node dissection is not required.17
In another study, peripheral nerve block significantly reduced perioperative complications in elderly patients with comorbidities compared with general anesthesia. This statement is consistent with the condition of the patients in this study. The authors stated that this technique provides effective analgesia while minimizing systemic effects, which is particularly beneficial for patients with cardiovascular risk.18
In addition, peripheral nerve block provides better postoperative care with excellent pain management, reduced nausea and vomiting and reduced dependence on medications. These factors collectively contribute to a shorter recovery. For example, in a case study of abdominal aortic aneurysm, thoracic spinal block was shown to be highly effective in postoperative recovery in a patient with severe COPD and ischemic heart disease.19 In another case, combined thoracic paravertebral and interscalene blocks facilitated the smooth performance of extensive breast surgery in another individual with multiple comorbidities.20
4. CONCLUSION
The choice of anesthetic technique is a challenge for anesthesiologists in cases of decreased cardiac function. In patients in this case report with decreased cardiac function, the use of peripheral nerve block using a combination of mental nerve block and superficial cervical plexus block has been proven safe, and there were no complications during perioperative or postoperative. Lastly, we try to aim not to take significant risks in straightforward procedures.
5. Acknowledgement
We would like to extend our sincere thanks to the multidisciplinary team involved in the patient's care, including the surgeon, anaesthesiologist, pain management specialists, and nursing staff. Their teamwork played a crucial role in delivering thorough care and enhancing pain management strategies. We also express our appreciation to the patient for her resilience and cooperation throughout her treatment, which greatly contributed to the positive results seen during her hospitalization.
6. Declaration of patient consent
The authors confirm that they have received all necessary patient consent forms. The patient has granted permission for his images and clinical information to be published in the journal. He is aware that his name and initials will not be disclosed, and efforts will be made to protect his identity; however, complete anonymity cannot be assured.
7. Financial support
No funding was received
8. Conflicts of interest
There were no conflict of interest.
9. Author contribution
AA: conceptualization, conduction of the study, writing - original draft, writing - review & editing
AUA: conduction of the study, writing - original draft, writing - review & editing
LH: writing - review & editing
10. REFERENCES
- Shibuya M, Kimura Y, Takuma S, Kamekura N, Fujisawa T. Cardiovascular considerations in anesthetic management for a patient with antiphospholipid syndrome and decreased cardiac function: a case study. Anesth Prog. 2021;68(1). [PubMed] DOI: 2344/anpr-67-03-07
- Choi BG, Rha SW, Yoon SG, Choi CU, Lee MW, Kim SW. Association of major adverse cardiac events up to 5 years in patients with chest pain without significant coronary artery disease in the Korean population. J Am Heart Assoc. 2019;8(12). [PubMed] DOI: 1161/JAHA.118.010541
- Beattie WS. A simple, reliable, and validated preoperative cardiac risk index. Can J Cardiol. 2021;37. [PubMed] DOI: 1016/j.cjca.2021.06.009
- Smilowitz NR, Gupta N, Ramakrishna H, Guo Y, Berger JS, Bangalore S. Perioperative major adverse cardiovascular and cerebrovascular events associated with noncardiac surgery. JAMA Cardiol. 2017;2(2):181. [PubMed] DOI: 1001/jamacardio.2016.4792
- Gemawan T, Handoko A, Misturiansyah NI. Anesthesia in low ejection fraction patient: case report. J Profesi Med. 2023;17(2). DOI: 33533/jpm.v17i2.6198
- Shaheen MSA, Sardar K, Chowdhury AN, Rahman MM, Alam MNA, Ahmed R, et al. Ejection fraction <35% – anaesthetic experience of 236 cases: a retrospective study. Anwer Khan Mod Med Coll J. 2018;9(2). Full Text
- Desai N, El-Boghdadly K, Albrecht E. Peripheral nerve blockade and novel analgesic modalities for ambulatory anesthesia. Curr Opin Anaesthesiol. 2020;33. [PubMed] DOI: 1097/ACO.0000000000000928
- Baker QF, Adds PJ. Anatomy: Regional, Surgical, and Applied (1st ed.). CRC Press; 2022. DOI: 1201/9781003312895
- Vasil’ev YuL, Rabinovich SA, Dydykin SS, Toropina GG, Demyanenko SA. Objective assessment of mental nerve local anesthesia. Stomatologiia. 2019;98(5). [PubMed] DOI: 17116/stomat20199805199
- Tan SL, Schiere S, Reidinga AC, Wit F, Veldman PH. Blockade of the mental nerve for lower lip surgery as a safe alternative to general anesthesia in two very old patients. Local Reg Anesth. 2015;8. [PubMed] DOI: 2147/LRA.S63246
- Rose SE, Gulati A. Mental nerve entrapment. In: Tubbs RS, Rizk E, Shoja MM, et al., eds. Peripheral nerve entrapments: clinical diagnosis and management; 2016.
- Sarkar AK, O’Connor CM, Goldstein RB. Superficial cervical plexus nerve block. In: Bendtsen TF, ed. Bedside pain management interventions; 2022.
- Xie L, Zhao Z, Huang L, Qin C, Wang W, Xu C. The anatomical research on the mental foramen related to the mental nerve block. Yangtze Med. 2021;5(1). DOI: 4236/ym.2021.51006
- Desai N, Albrecht E. Local anaesthetic adjuncts for peripheral nerve blockade. Curr Opin Anaesthesiol. 2023;36. [PubMed] DOI: 1097/ACO.0000000000001272
- Desai N, Kirkham KR, Albrecht E. Local anaesthetic adjuncts for peripheral regional anaesthesia: a narrative review. Anaesthesia. 2021;76. [PubMed] DOI: 1111/anae.15245
- Kuntoadi D, Utama SP, Yuliana F, Hermawan A. Peripheral nerve block as a safer alternative than general anesthesia in high-risk patients with multiple comorbidities: a case report. Solo J Anesth Pain Crit Care. 2025;5(1). Full Text
- Khater A, Elzahaby IA, Hamdy M, Zuhdy M, Hamdy O, Ezzat M, et al. Evaluation of bilateral mental nerve block as an alternative to general anesthesia for resection of lower lip tumors. Surg Sci. 2017;8(8). DOI: 4236/ss.2017.88035
- Al Harbi M, Alshaghroud S, Aljahdali M, Ghorab F, Baba F, Al Dosary R, et al. Regional anesthesia for geriatric population. Saudi J Anaesth. 2023;17. [PubMed] DOI: 4103/sja.sja_424_23
- Sada F, Kavaja F, Hamza A, Ukperaj BM. A 74-year-old man with severe comorbidities and successful abdominal aortic aneurysm repair with thoracic segmental spinal anesthesia: a case report. Am J Case Rep. 2024;25. [PubMed] DOI: 12659/AJCR.943702
- Paśnicki M, Król A, Kosson D, Kołacz M. The safety of peripheral nerve blocks: the role of triple monitoring in regional anaesthesia, a comprehensive review. Healthcare. 2024;12(7):769. [PubMed] DOI: 3390/healthcare12070769