Lubna Abdulrahman Hafiz 1 , Hind Mauafaq Aljifri 2 , Shahad Muneer Abdulaal 3 , Rinad Tariq Siddiqi 4 , Asma Khalid Alamoudi 5
Authors affiliations:
Background & objective: Receiving a cancer diagnosis was often the most challenging part of the entire procedure for many survivors of primary or recurrent breast cancer. The aim of this study was to examine the prevalence of depression and anxiety among patients with breast cancer in Jeddah, Saudi Arabia.
Methodology: A cross-sectional survey study was conducted in Jeddah, Saudi Arabia between November 2024 and February 2025 to examine the prevalence of depression and anxiety among female patients diagnosed with breast cancer, with the use of Generalized Anxiety Disorder Scale-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9).
Results: A total of 137 breast cancer patients were included in the analysis. Anxiety levels were distributed among patients as follows: 46 (33.6%) had mild anxiety, 50 (36.5%) had moderate anxiety, and 41 (29.9%) experienced severe anxiety. Depression severity varied, with 11 (8.0%) reporting mild symptoms, 54 (39.4%) experiencing moderate depression, 42 (30.7%) having moderately severe depression, and 30 (21.9%) suffering from severe depression. The GAD-7 mean score was (12.6 ± 4.9) out of 21, and PHQ-9 mean score was (15.8 ± 5.21) out of 27. Patients who underwent radiotherapy had significantly higher odds of experiencing depression (AOR = 3.27, 95% CI: 1.17-9.10, P = 0.02) and nearly significant association with anxiety (AOR = 3.14, 95% CI: 0.99-10.01, P = 0.05). Additionally, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI: 0.08-1.01, P = 0.05).
Conclusion: Depression and anxiety are common psychological illnesses among females with breast cancer. Psychological intervention should be directed towards high-risk patients. Psycholoigcal support programs should be facilitated for these patients in order to improve their clinical outcomes.
Abbreviations: GAD-7: Generalized Anxiety Disorder Scale-7, PHQ-9: Patient Health Questionnaire-9
Keywords: Anxiety; Breast cancer; Depression; Saudi Arabia
Citation: Hafiz LA, Aljifri HM, Abdulaal SM, Siddiqi RT, AlamoudiAK. Prevalence of depression and anxiety among patients with breast cancer in Jeddah, Saudi Arabia. Anaesth. pain intensive care 2025;29(5):268-276. DOI: 10.35975/apic.v29i5.2850
Received: April 17, 2025; Revised: April 22, 2025; Accepted: May 10, 2025
Breast cancer is a serious public health issue and the primary cause of cancer-related deaths among women globally.1 It is projected that there would be 17 million cancer deaths and 27 million new cancer cases worldwide in 2030.2 In a population of 33,554,333, Saudi Arabia reported 10,518 cancer-related fatalities and 24,485 new cancer cases in 2018.3 Compared to 20% in industrialized nations, over 50% of breast cancer cases in Saudi Arabia are diagnosed at an advanced stage.3 Although death rates are frequently lower in high-income nations because of improved access to early detection and treatment, high-income countries generally have higher incidence rates than low- and middle-income ones.4
Regarding the variables that raise the risk of breast cancer, they can be linked to genetic, hormonal, and environmental, which is the primary risk factor for disease and shows a higher frequency in women over 50.5 Different cancer therapies and drugs are available, including radiation therapy and surgery to treat a particular tumor or part of the body, as well as chemical treatments like immunotherapy, chemotherapy, and targeted therapy. The adverse effects of cancer treatments are numerous. Adverse effects may differ between medications and treatment modalities, as well as between individuals.6-9
It is possible for the diagnosis itself to contribute to or worsen poor mental health.10,11 Receiving a cancer diagnosis was often the most challenging part of the entire procedure for many survivors of primary or recurrent breast cancer.12 Anxiety and depression are common psychological illnesses among patients diagnosed with cancer in both inpatients and outpatients’ settings.13 According to previous review articles, anxiety symptoms are widespread and last throughout the course of cancer therapy in individuals with newly diagnosed breast cancer.14-16 According to another analysis, after receiving a breast cancer diagnosis, more than 22% of women have depressed symptoms.16 The aim of this research was to examine the prevalence of anxiety and depression among female patients diagnosed with breast cancer in Saudi Arabia.
A cross-sectional survey study was conducted in Jeddah, Saudi Arabia between November 2024 and February 2025 to examine the prevalence of depression and anxiety among female patients diagnosed with breast cancer.
The study population for this research comprised of female patients diagnosed with breast cancer. The inclusion criteria for this research were adult female patients, aged above 18, and currently living in Saudi Arabia. This research did not exclude eligible patients based on the stage of their disease, socioeconomic status, or type of their cancer therapy.
The convenience sampling technique was utilized in this research. The research participation link was circulated through social media platforms including Facebook and WhatsApp. The research inclusion criteria were mentioned in the invitation letter. Patients who meet the inclusion criteria were invited to take part in this research.
This research examined female cancer patients’ demographics characteristics including their marital status, nationality, monthly income, education level, smoking status, and disease status. Besides, this research examined patients’ cancer therapy, and disease profile (comorbidities, disease duration, and metastasis). The prevalence rates of depressed and anxious symptoms were established using a cut-off point as advised by the developers of the PHQ-9 and GAD-7 scales and utilized in previous research.17-20 Depressive symptomatology will be characterized by a total score of 15 or above on the PHQ-9 instrument, signifying moderately severe or severe depression.21 Anxiety symptomatology will be characterized using the GAD-7 instrument, with a total score of 15 or higher signifying severe anxiety symptoms.22 A higher score indicates a more depressed and anxious severe case.
2.1. Statistical analysis
The Statistical Package for the Social Sciences (SPSS) software, version 29 was used to analyse the data for this research. Categorical variables were summarized as frequency and percentage, and means ± standard deviation (SD) were utilized to express continuous variable such as the GAD-7 and PHQ-9 score. Based on the literature, the scores were categorized into four categories, then the severe category in both scores were used to define the dummy variables for multiple logistic regression analyses. The findings of the regression analysis were presented as adjusted odds ratio (AOR) with its corresponding 95% confidence interval. The level of significance was defined as p-value less than 0.05.
A total of 137 breast cancer patients were included in the analysis. Among those, 93 (67.9%) were married, 21 (15.3%) were single, 12 (8.8%) were divorced, and 11 (8.0%) were widowed. The majority were Saudi nationals (n= 99, 72.3%), while 38 (27.7%) were non-Saudi. Regarding monthly income, 69 (50.4%) had more than 7500 SAR monthly income, and 25 patients (18.2%) had less than 2500 SAR monthly. Most of participants (65, 47.4%) having a bachelor degree, followed by 28 participants having a high school degree (20.4%). Regarding the smoking status, only 10 patients currently smoking (7.3%), and 111 patients (81.0%) never smoked. A round half of the patients were in the first and second stage of their disease. Additional details about demographic characteristics are provided in Table 1.
The below table presents the cancer therapies received by the patients. Surgery was performed in 93 (67.9%) patients, while 44 (323.1%) didn’t undergo surgery. Chemotherapy was administered to 83 (60.6%) patients.
Furthermore, a total of 81 patients (59.1%) were given radiotherapy, and target therapy was the least common, with only 22 patients (16.1%). Additional details about cancer therapy modalities are provided in Table 2.
The most common comorbidities were hypertension (25.5%), diabetes mellitus (22.6%), and dyslipidemia (17.5%). Disease duration varied, with 39 (28.5%) patients having the cancer for 6-12 months and 34 (24.8%) for more than 2 years. The majority of patients (89.8%) didn’t have metastases (Table 3).
The most commonly reported issues were feeling tired or having little energy, with 32 (23.4%) experiencing it nearly every day and 67 (48.9%) on several days. sleep disturbances were also prevalent, with 21 (15.3%) reporting trouble sleeping nearly every day. Loss of interest or pleasure in activities affected 16 (11.7%) nearly every day, while 48 (35.0%) experienced I on several days. feelings of depression or hopelessness were reported by 7 (5.1%) nearly every day, and 45 (32.8%) on several days. Additional details about PHQ-9 score are provided in Table S-1.
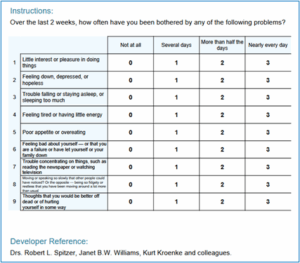
Table S-1: Patient Health Questionnaire=Depression (PHQ-9)
Feeling nervous or anxious was reported by 48 (35.0%) on several days and 9 (6.6%) nearly every day. Excessive worrying was common, with 59 (43.1%) worrying too much on several days and 13 (9.5%) nearly every day. Trouble relaxing affected 52 (38.0%) on several days, while 15 (10.9%) experienced it nearly every day. Irritable was also considerable, with 19 (13.9%) feeling easily annoyed more than half the days and 18 (13.1%) nearly every day. additional details about GaD-7 score are provided in Table S-2.
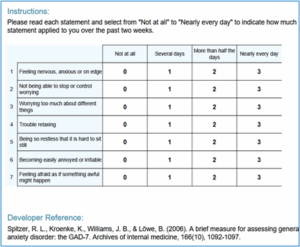
Table S-2: Generalised Anxiety Disorder Assessment (GAD-7)
Anxiety levels were distributed among patients as follows: 46 (33.6%) had mild anxiety, 50 (36.5%) had moderate anxiety, and 41 (29.9%) experienced severe anxiety. Depression severity varied, with 11 (8.0%) reporting mild symptoms, 54 (39.4%) experiencing moderate depression, 42 (30.7%) having moderately severe depression, and 30 (21.9%) suffering from severe depression. The GAD-7 mean score was (12.6 ± 4.9) out of 21, and PHQ-9 mean score was (15.8 ± 5.21) out of 27 (Table 4).
Patients who underwent radiotherapy had significantly higher odds of experiencing depression (AOR = 3.27, 95% CI: 1.17-9.10, p=0.02) and nearly significant association with anxiety (AOR=3.14, 95% CI: 0.99-10.01, P = 0.05). Additionally, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI: 0.08-1.01, P =0.05). Additional details about factors associated with anxiety and depression are provided in Table 5.
This study aimed to examine the prevalence of anxiety and depression among female patients diagnosed with breast cancer in Saudi Arabia. In this study, a round half of the patients were in the first and second stage of their disease. The most prevalent malignancy among Saudi women and the Saudi populace at large is breast cancer. Even while 72% of them report relative 5-year survival, this is still a slightly lower number than in Western nations.23,24 Low screening rates and a comparatively large percentage of presentations in advanced stages (12.5%) are likely the causes of a decreased survival rate.23 Furthermore, according to the ministry report, Saudi women are more likely than US women to receive a diagnosis at an advanced stage of their illness (57.3% of cases are regional or distant metastatic breast cancers, compared to 37% of US women.25 The majority of the Saudi Arabian data that is currently available relates to women's and health professionals' attitudes regarding screening as well as their knowledge and views of it.26
In this study, surgery was performed in 93 (67.9%) patients. The two most common methods of breast surgery are either breast-conserving surgery (lumpectomy) or complete removal of the breast (mastectomy), which is typically followed by breast reconstruction. A lumpectomy involves removing the breast tumor along with a margin of healthy tissue. "No ink on tumor" refers to the absence of tumor cells near the tissue edge, which is the recommended margins status.27 Research indicates that lumpectomy plus irradiation and complete mastectomy are comparable in terms of overall survival (OS) and relapse-free rates.28 The presence of diffuse microcalcifications (suspicious or malignant-appearing), diseases that cannot be included by local excision with a tolerable cosmetic outcome, and ATM (ataxia-telangiectasias mutated) mutations (biallelic inactivation) are among the conditions that preclude breast-conserving surgery.27
In this study, chemotherapy was administered to 83 (60.6%) of the patients Alkylating agents, antimetabolites, and tubulin inhibitors are among the families of cytotoxic drugs that make up breast cancer chemotherapy.29 Cyclophosphamide is a nitrogen mustard alkylating agent that breaks DNA strands.30 Anthracyclines (doxorubicin, daunorubicin, epirubicin, and idarubicin) work by inducing DNA intercalation, which inhibits macromolecular biosynthesis.30 Taxanes, such as docetaxel and paclitaxel, bind to microtubules and stop them from disassuring, which causes cell cycle arrest and apoptosis.31 Furthermore, a total of 81 (59.1%) patients were given radiotherapy Since Röngten's discovery of the X-ray in 1895, radiation therapy has been utilized to treat cancer.32 The entire breast or a section of it (after breast-conservative surgery), the chest wall (following mastectomy), and the local lymph nodes are exposed to high-energy radiation.33
A history of anxiety or depression, a younger age at diagnosis, a lack of social support, burdensome somatic symptoms, ongoing cancer treatment, certain medication treatments, concerns about death and disease recurrence, altered body image,34 and changes in femininity, sexuality, and attractiveness;35 are risk factors for anxiety and depression in women with breast cancer. During but not after treatment, adjuvant chemotherapy may raise the risk of anxiety, depression, or both.36
Effective methods of identifying patients who are at risk for psychological distress are essential, as depression and anxiety are common diagnoses after breast cancer.37 In the already taxing emotional state following a breast cancer diagnosis, they compound the challenges brought on by a number of social and familial issues that worsen the disease as well as therapeutic approaches like mastectomy and chemotherapy.38 Additionally, psychological distress (depression and anxiety symptoms) has been linked to increased mortality risk and worse physical function.39,40 The prevalence of depression in our study was 30.7% of the patients found having moderately severe depression, and 30 (21.9%) suffering from severe depression. which is less than the finding of study enrolled 74 patients diagnosed with breast cancer in the general surgery clinic at King Abdulaziz University Hospital in Jeddah, Saudi Arabia it was 36.5%,41 and lower than the findings of other studies, which ranged between 49.2% and 68.7%.42,43
Our study Around 29.9% of the patients experienced severe anxiety. Which is comparable with the pervious study done in general surgery clinic at King Abdulaziz University Hospital in Jeddah, Saudi Arabia measures generalized anxiety disorder (GAD) prevalence was 24.3% is lower than that of other studies,41 which ranged between 48.6% and 73.3%.42,43 We hypothesize that the reason our study's results were lower than those of previous articles was because the questionnaire's timing varied depending on the period between diagnosis and management stage, which may have affected respondents' responses.
When undergoing radiation therapy, the patient must lie alone on a table with a large machine overhead, which can cause anxiety, fear, and a sense of isolation. Radiation therapy side effects are also problematic; in the United States, approximately 350,000 cancer patients receive radiation therapy annually, and cancer patients often report fears of the treatment (such as being "burned," or causing sterility, sickness, or vomiting.44 Additionally, 60% of patients experience significant anxiety before treatment, and 80% of them after.42
Previous study found that among 1346 patients receiving radiation therapy for head and neck cancer, 46% experienced emotional distress, 26% experienced anxiety, 9% experienced depression, and 27% experienced claustrophobia. Women were significantly more likely to experience emotional distress, depression, and anxiety (P < 0.001).45 Anxiety is listed as one of the common systemic toxicities of radiation treatment, along with pain, fatigue, and anorexia.46 Therefore, it is possible that the anxiety observed in our patients was a side effect of the radiation.
In our study, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI0.08-1.01, P = 0.05). Previous studies showed the psychological dysfunction rate among patients who had surgery for breast cancer ranged from 30 to 47%. There was no discernible difference between patients who had modified radical mastectomy and those who had breast-conserving surgery.47
It is important to identify depression in breast cancer patients because it has significant effects on the course and prognosis of the disease.44
Research has shown that psychological factors, such as stress and depression, can affect a person's overall quality of life and the course of their illness after receiving a cancer diagnosis. For these patients, concurrent psychiatric counseling will improve their quality of life, and psychiatric therapy for cancer patients should aim to increase resilience in addition to treating depression, anxiety, and stress.44
Depression and anxiety are common psychological illnesses among females with breast cancer. Psychological intervention should be directed towards high-risk patients. Psychological support program should be facilitated for the patients in order to improve their clinical outcomes.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Ethical approval
This study was approved by the Institutional Review Board (IRB) at Fakeeh College for Medical Sciences (Approval No: 530/IRB/2023).
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
LAH: Conceptualization, investigation, methodology, resources, validation, writing- original draft, writing – review and editing.
HMA, SMA, RTS, AKA: Investigation, resources, validation, writing- original draft, writing – review and editing.
Authors affiliations:
- Lubna Abdulrahman Hafiz, College of Medicine, Fakeeh College for Medical Sciences, Jeddah, KSA; Email: Lahafiz@fcms.edu.sa
- Hind Mauafaq Aljifri, College of Medicine, Fakeeh College for Medical Sciences, Jeddah, KSA; Email: Hind.aljifri@gmail.com
- Shahad Muneer Abdulaal, College of Medicine, Fakeeh College for Medical Sciences, Jeddah, KSA; Email: shahadabdulaal1995@gmail.com
- Rinad Tariq Siddiqi, College of Medicine, Fakeeh College for Medical Sciences, Jeddah, KSA; Email: Rinad.siddiqi@gmail.com
- Asma Khalid Alamoudi, College of Medicine, Fakeeh College for Medical Sciences, Jeddah, KSA; Email: asmaalamoudiiiii@gmail.com
ABSTRACT
Background & objective: Receiving a cancer diagnosis was often the most challenging part of the entire procedure for many survivors of primary or recurrent breast cancer. The aim of this study was to examine the prevalence of depression and anxiety among patients with breast cancer in Jeddah, Saudi Arabia.
Methodology: A cross-sectional survey study was conducted in Jeddah, Saudi Arabia between November 2024 and February 2025 to examine the prevalence of depression and anxiety among female patients diagnosed with breast cancer, with the use of Generalized Anxiety Disorder Scale-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9).
Results: A total of 137 breast cancer patients were included in the analysis. Anxiety levels were distributed among patients as follows: 46 (33.6%) had mild anxiety, 50 (36.5%) had moderate anxiety, and 41 (29.9%) experienced severe anxiety. Depression severity varied, with 11 (8.0%) reporting mild symptoms, 54 (39.4%) experiencing moderate depression, 42 (30.7%) having moderately severe depression, and 30 (21.9%) suffering from severe depression. The GAD-7 mean score was (12.6 ± 4.9) out of 21, and PHQ-9 mean score was (15.8 ± 5.21) out of 27. Patients who underwent radiotherapy had significantly higher odds of experiencing depression (AOR = 3.27, 95% CI: 1.17-9.10, P = 0.02) and nearly significant association with anxiety (AOR = 3.14, 95% CI: 0.99-10.01, P = 0.05). Additionally, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI: 0.08-1.01, P = 0.05).
Conclusion: Depression and anxiety are common psychological illnesses among females with breast cancer. Psychological intervention should be directed towards high-risk patients. Psycholoigcal support programs should be facilitated for these patients in order to improve their clinical outcomes.
Abbreviations: GAD-7: Generalized Anxiety Disorder Scale-7, PHQ-9: Patient Health Questionnaire-9
Keywords: Anxiety; Breast cancer; Depression; Saudi Arabia
Citation: Hafiz LA, Aljifri HM, Abdulaal SM, Siddiqi RT, AlamoudiAK. Prevalence of depression and anxiety among patients with breast cancer in Jeddah, Saudi Arabia. Anaesth. pain intensive care 2025;29(5):268-276. DOI: 10.35975/apic.v29i5.2850
Received: April 17, 2025; Revised: April 22, 2025; Accepted: May 10, 2025
1. INTRODUCTION
Breast cancer is a serious public health issue and the primary cause of cancer-related deaths among women globally.1 It is projected that there would be 17 million cancer deaths and 27 million new cancer cases worldwide in 2030.2 In a population of 33,554,333, Saudi Arabia reported 10,518 cancer-related fatalities and 24,485 new cancer cases in 2018.3 Compared to 20% in industrialized nations, over 50% of breast cancer cases in Saudi Arabia are diagnosed at an advanced stage.3 Although death rates are frequently lower in high-income nations because of improved access to early detection and treatment, high-income countries generally have higher incidence rates than low- and middle-income ones.4
Regarding the variables that raise the risk of breast cancer, they can be linked to genetic, hormonal, and environmental, which is the primary risk factor for disease and shows a higher frequency in women over 50.5 Different cancer therapies and drugs are available, including radiation therapy and surgery to treat a particular tumor or part of the body, as well as chemical treatments like immunotherapy, chemotherapy, and targeted therapy. The adverse effects of cancer treatments are numerous. Adverse effects may differ between medications and treatment modalities, as well as between individuals.6-9
It is possible for the diagnosis itself to contribute to or worsen poor mental health.10,11 Receiving a cancer diagnosis was often the most challenging part of the entire procedure for many survivors of primary or recurrent breast cancer.12 Anxiety and depression are common psychological illnesses among patients diagnosed with cancer in both inpatients and outpatients’ settings.13 According to previous review articles, anxiety symptoms are widespread and last throughout the course of cancer therapy in individuals with newly diagnosed breast cancer.14-16 According to another analysis, after receiving a breast cancer diagnosis, more than 22% of women have depressed symptoms.16 The aim of this research was to examine the prevalence of anxiety and depression among female patients diagnosed with breast cancer in Saudi Arabia.
2. METHODOLOGY
A cross-sectional survey study was conducted in Jeddah, Saudi Arabia between November 2024 and February 2025 to examine the prevalence of depression and anxiety among female patients diagnosed with breast cancer.
The study population for this research comprised of female patients diagnosed with breast cancer. The inclusion criteria for this research were adult female patients, aged above 18, and currently living in Saudi Arabia. This research did not exclude eligible patients based on the stage of their disease, socioeconomic status, or type of their cancer therapy.
The convenience sampling technique was utilized in this research. The research participation link was circulated through social media platforms including Facebook and WhatsApp. The research inclusion criteria were mentioned in the invitation letter. Patients who meet the inclusion criteria were invited to take part in this research.
This research examined female cancer patients’ demographics characteristics including their marital status, nationality, monthly income, education level, smoking status, and disease status. Besides, this research examined patients’ cancer therapy, and disease profile (comorbidities, disease duration, and metastasis). The prevalence rates of depressed and anxious symptoms were established using a cut-off point as advised by the developers of the PHQ-9 and GAD-7 scales and utilized in previous research.17-20 Depressive symptomatology will be characterized by a total score of 15 or above on the PHQ-9 instrument, signifying moderately severe or severe depression.21 Anxiety symptomatology will be characterized using the GAD-7 instrument, with a total score of 15 or higher signifying severe anxiety symptoms.22 A higher score indicates a more depressed and anxious severe case.
2.1. Statistical analysis
The Statistical Package for the Social Sciences (SPSS) software, version 29 was used to analyse the data for this research. Categorical variables were summarized as frequency and percentage, and means ± standard deviation (SD) were utilized to express continuous variable such as the GAD-7 and PHQ-9 score. Based on the literature, the scores were categorized into four categories, then the severe category in both scores were used to define the dummy variables for multiple logistic regression analyses. The findings of the regression analysis were presented as adjusted odds ratio (AOR) with its corresponding 95% confidence interval. The level of significance was defined as p-value less than 0.05.
3. RESULTS
A total of 137 breast cancer patients were included in the analysis. Among those, 93 (67.9%) were married, 21 (15.3%) were single, 12 (8.8%) were divorced, and 11 (8.0%) were widowed. The majority were Saudi nationals (n= 99, 72.3%), while 38 (27.7%) were non-Saudi. Regarding monthly income, 69 (50.4%) had more than 7500 SAR monthly income, and 25 patients (18.2%) had less than 2500 SAR monthly. Most of participants (65, 47.4%) having a bachelor degree, followed by 28 participants having a high school degree (20.4%). Regarding the smoking status, only 10 patients currently smoking (7.3%), and 111 patients (81.0%) never smoked. A round half of the patients were in the first and second stage of their disease. Additional details about demographic characteristics are provided in Table 1.
| Table 1: Demographic characteristics among breast cancer patients | ||
| Demographic characteristics | N (%) | |
| Marital status | Single | 21(15.3) |
| Married | 93(67.9) | |
| Divorced | 12(8.8) | |
| Widowed | 11(8.0) | |
| Nationality | Non-Saudi | 38(27.7) |
| Saudi | 99(72.3) | |
| Monthly income | Less than 2500 SAR | 25(18.2) |
| 2500-5000 SAR | 22(16.1) | |
| 5000-7500 SAR | 21(15.3) | |
| More than 7500 SAR | 69(50.4) | |
| Education level | Primary school or less | 19(13.9) |
| High school | 28(20.4) | |
| Diploma | 11(8.0) | |
| Bachelor | 65(47.4) | |
| Post graduate | 14(10.2) | |
| Smoking status | Non-Smoking | 111(81.0) |
| Previous smoking | 16(11.7) | |
| Currently smoking | 10(7.3) | |
| Disease stage | Unknown | 35(25.5) |
| 1st degree | 34(24.8) | |
| 2nd degree | 34(24.8) | |
| 3rd degree | 16(11.7) | |
| 4th degree | 18(13.1) | |
| SAR: Saudi Arabia Riyal; Data presented as n (%) | ||
The below table presents the cancer therapies received by the patients. Surgery was performed in 93 (67.9%) patients, while 44 (323.1%) didn’t undergo surgery. Chemotherapy was administered to 83 (60.6%) patients.
Furthermore, a total of 81 patients (59.1%) were given radiotherapy, and target therapy was the least common, with only 22 patients (16.1%). Additional details about cancer therapy modalities are provided in Table 2.
| Table 2: Distribution of cancer therapy modalities among breast cancer patients | |
| Cancer therapy | N (%) |
| Surgery | 93 (67.9) |
| Chemotherapy | 83 (60.6) |
| Radiotherapy | 81 (59.1) |
| Target therapy | 22 (16.1) |
| Immunotherapy | 20 (14.6) |
| Hormonal therapy | 72 (52.6) |
| Unknown | 15 (10.9) |
The most common comorbidities were hypertension (25.5%), diabetes mellitus (22.6%), and dyslipidemia (17.5%). Disease duration varied, with 39 (28.5%) patients having the cancer for 6-12 months and 34 (24.8%) for more than 2 years. The majority of patients (89.8%) didn’t have metastases (Table 3).
| Table 3: Comorbidities, disease duration, and mental health in breast cancer patients | ||
| Variables | N (%) | |
| Comorbidities | Diabetes mellitus | 31 (22.6) |
| Hypertension | 35 (25.5) | |
| Cardiovascular diseases | 7 (5.1) | |
| Respiratory | 11 (8.0) | |
| Dyslipidemia | 24 (17.5) | |
| Others | 78 (56.9) | |
| Disease duration | Less than 6 months | 33 (24.1) |
| 6-12 month | 39 (28.5) | |
| 1-2 years | 31 (22.6) | |
| More than 2 years | 34 (24.8) | |
| Metastasis | 14 (10.2) | |
| Diagnosed with anxiety | 23 (16.8) | |
| Diagnosed with depression | 14 (10.2) | |
The most commonly reported issues were feeling tired or having little energy, with 32 (23.4%) experiencing it nearly every day and 67 (48.9%) on several days. sleep disturbances were also prevalent, with 21 (15.3%) reporting trouble sleeping nearly every day. Loss of interest or pleasure in activities affected 16 (11.7%) nearly every day, while 48 (35.0%) experienced I on several days. feelings of depression or hopelessness were reported by 7 (5.1%) nearly every day, and 45 (32.8%) on several days. Additional details about PHQ-9 score are provided in Table S-1.
Table S-1: Patient Health Questionnaire=Depression (PHQ-9)
Feeling nervous or anxious was reported by 48 (35.0%) on several days and 9 (6.6%) nearly every day. Excessive worrying was common, with 59 (43.1%) worrying too much on several days and 13 (9.5%) nearly every day. Trouble relaxing affected 52 (38.0%) on several days, while 15 (10.9%) experienced it nearly every day. Irritable was also considerable, with 19 (13.9%) feeling easily annoyed more than half the days and 18 (13.1%) nearly every day. additional details about GaD-7 score are provided in Table S-2.
Table S-2: Generalised Anxiety Disorder Assessment (GAD-7)
Anxiety levels were distributed among patients as follows: 46 (33.6%) had mild anxiety, 50 (36.5%) had moderate anxiety, and 41 (29.9%) experienced severe anxiety. Depression severity varied, with 11 (8.0%) reporting mild symptoms, 54 (39.4%) experiencing moderate depression, 42 (30.7%) having moderately severe depression, and 30 (21.9%) suffering from severe depression. The GAD-7 mean score was (12.6 ± 4.9) out of 21, and PHQ-9 mean score was (15.8 ± 5.21) out of 27 (Table 4).
| Table 4: The GAD-7 and PHQ-9 categories | ||
| Depression and anxiety status classification | N (%) | |
| GAD-7 | Mild | 46 (33.6) |
| Moderate | 50 (36.5) | |
| Severe | 41 (29.9) | |
| PHQ-9 | Mild | 11 (8.0) |
| Moderate | 54 (39.4) | |
| Moderately severe | 42 (30.7) | |
| Severe | 30 (21.9) | |
| GAD-7: Generalized Anxiety Disorder Scale-7
PHQ-9: Patient Health Questionnaire-9 Data presented as n (%) |
||
Patients who underwent radiotherapy had significantly higher odds of experiencing depression (AOR = 3.27, 95% CI: 1.17-9.10, p=0.02) and nearly significant association with anxiety (AOR=3.14, 95% CI: 0.99-10.01, P = 0.05). Additionally, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI: 0.08-1.01, P =0.05). Additional details about factors associated with anxiety and depression are provided in Table 5.
| Table 5: Factors associated with anxiety and depression | |||||
|
Factors |
PHQ-9 | GAD-7 | |||
| AOR (95%CI) | P value | AOR (95%CI) | P value | ||
| Marital status | Single | Reference | Reference | ||
| Married | 1.32 (0.38-4.56) | 0.665 | 0.95 (0.25-3.63) | 0.937 | |
| Divorced | 3.09 (0.45-21.48) | 0.253 | 1.20 (0.18-8.14) | 0.849 | |
| Widowed | 0.95 (0.12-7.38) | 0.960 | 0.10 (0.00-2.02) | 0.132 | |
| Income | < 2500 SAR | Reference | Reference | ||
| 2500-5000 SAR | 1.60 (0.34-7.42) | 0.551 | 0.63 (0.13-3.07) | 0.565 | |
| 5000-7500 SAR | 1.57 (0.36-6.92) | 0.552 | 0.54 (0.11-2.59) | 0.438 | |
| > 7500 SAR | 1.14 (0.26-5.03) | 0.858 | 0.62 (0.13-2.81) | 0.532 | |
| Nationality | Non-Saudi | Reference | Reference | ||
| Saudi | 0.85 (0.27-2.66) | 0.782 | 1.26 (0.38-4.21) | 0.704 | |
| Education level | Primary school or less | Reference | Reference | ||
| High school | 1.32 (0.30-5.80) | 0.714 | 0.65 (0.13-3.25) | 0.595 | |
| Diploma | 3.91 (0.55-27.64) | 0.171 | 1.72 (0.23-13.02) | 0.601 | |
| Bachelor | 1.96 (0.40-9.51) | 0.403 | 1.20 (0.21-6.71) | 0.836 | |
| Post graduate | 1.12 (0.16-7.70) | 0.907 | 0.45 (0.04-4.65) | 0.500 | |
| Smoking | Non-Smoking | Reference | Reference | ||
| Previous smoking | 1.82 (0.44-7.43) | 0.405 | 1.27 (0.30-5.33) | 0.743 | |
| Currently smoking | 0.84 (0.18-4.01) | 0.826 | 2.55 (0.51-12.75) | 0.255 | |
| Disease stage | Unknown | Reference | Reference | ||
| 1st degree | 0.41 (0.11-1.55) | 0.188 | 1.54 (0.37-6.38) | 0.550 | |
| 2nd degree | 0.53 (0.13-2.07) | 0.358 | 1.29 (0.29-5.74) | 0.739 | |
| 3rd degree | 0.21 (0.04-1.10) | 0.065 | 0.24 (0.03-2.07) | 0.196 | |
| 4th degree | 0.89 (0.19-4.16) | 0.883 | 1.29 (0.27-6.26) | 0.752 | |
| Surgery | No | Reference | Reference | ||
| Yes | 0.44 (0.14-1.34) | 0.149 | 0.29 (0.08-1.01) | 0.051 | |
| Chemotherapy | No | Reference | Reference | ||
| Yes | 2.57 (0.92-7.17) | 0.073 | 2.14 (0.70-6.50) | 0.181 | |
| Radiotherapy | No | Reference | Reference | ||
| Yes | 3.27 (1.17-9.10) | 0.023 | 3.14 (0.99-10.01) | 0.053 | |
| Target | No | Reference | Reference | ||
| Yes | 0.35 (0.11-1.18) | 0.091 | 0.48 (0.12-1.89) | 0.291 | |
| Immunotherapy | No | Reference | Reference | ||
| Yes | 1.28 (0.36-4.49) | 0.704 | 2.46 (0.63-9.65) | 0.198 | |
| Hormonal therapy | No` | Reference | Reference | ||
| Yes | 1.17 (0.45-3.01) | 0.744 | 0.73 (0.25-2.13) | 0.566 | |
| GAD-7: Generalized Anxiety Disorder Scale-7; PHQ-9: Patient Health Questionnaire-9; SAR: Saudi Arabia Riyal
Data presented as median (range); P < 0.05 considered as significant |
|||||
4. DISCUSSION
This study aimed to examine the prevalence of anxiety and depression among female patients diagnosed with breast cancer in Saudi Arabia. In this study, a round half of the patients were in the first and second stage of their disease. The most prevalent malignancy among Saudi women and the Saudi populace at large is breast cancer. Even while 72% of them report relative 5-year survival, this is still a slightly lower number than in Western nations.23,24 Low screening rates and a comparatively large percentage of presentations in advanced stages (12.5%) are likely the causes of a decreased survival rate.23 Furthermore, according to the ministry report, Saudi women are more likely than US women to receive a diagnosis at an advanced stage of their illness (57.3% of cases are regional or distant metastatic breast cancers, compared to 37% of US women.25 The majority of the Saudi Arabian data that is currently available relates to women's and health professionals' attitudes regarding screening as well as their knowledge and views of it.26
In this study, surgery was performed in 93 (67.9%) patients. The two most common methods of breast surgery are either breast-conserving surgery (lumpectomy) or complete removal of the breast (mastectomy), which is typically followed by breast reconstruction. A lumpectomy involves removing the breast tumor along with a margin of healthy tissue. "No ink on tumor" refers to the absence of tumor cells near the tissue edge, which is the recommended margins status.27 Research indicates that lumpectomy plus irradiation and complete mastectomy are comparable in terms of overall survival (OS) and relapse-free rates.28 The presence of diffuse microcalcifications (suspicious or malignant-appearing), diseases that cannot be included by local excision with a tolerable cosmetic outcome, and ATM (ataxia-telangiectasias mutated) mutations (biallelic inactivation) are among the conditions that preclude breast-conserving surgery.27
In this study, chemotherapy was administered to 83 (60.6%) of the patients Alkylating agents, antimetabolites, and tubulin inhibitors are among the families of cytotoxic drugs that make up breast cancer chemotherapy.29 Cyclophosphamide is a nitrogen mustard alkylating agent that breaks DNA strands.30 Anthracyclines (doxorubicin, daunorubicin, epirubicin, and idarubicin) work by inducing DNA intercalation, which inhibits macromolecular biosynthesis.30 Taxanes, such as docetaxel and paclitaxel, bind to microtubules and stop them from disassuring, which causes cell cycle arrest and apoptosis.31 Furthermore, a total of 81 (59.1%) patients were given radiotherapy Since Röngten's discovery of the X-ray in 1895, radiation therapy has been utilized to treat cancer.32 The entire breast or a section of it (after breast-conservative surgery), the chest wall (following mastectomy), and the local lymph nodes are exposed to high-energy radiation.33
A history of anxiety or depression, a younger age at diagnosis, a lack of social support, burdensome somatic symptoms, ongoing cancer treatment, certain medication treatments, concerns about death and disease recurrence, altered body image,34 and changes in femininity, sexuality, and attractiveness;35 are risk factors for anxiety and depression in women with breast cancer. During but not after treatment, adjuvant chemotherapy may raise the risk of anxiety, depression, or both.36
Effective methods of identifying patients who are at risk for psychological distress are essential, as depression and anxiety are common diagnoses after breast cancer.37 In the already taxing emotional state following a breast cancer diagnosis, they compound the challenges brought on by a number of social and familial issues that worsen the disease as well as therapeutic approaches like mastectomy and chemotherapy.38 Additionally, psychological distress (depression and anxiety symptoms) has been linked to increased mortality risk and worse physical function.39,40 The prevalence of depression in our study was 30.7% of the patients found having moderately severe depression, and 30 (21.9%) suffering from severe depression. which is less than the finding of study enrolled 74 patients diagnosed with breast cancer in the general surgery clinic at King Abdulaziz University Hospital in Jeddah, Saudi Arabia it was 36.5%,41 and lower than the findings of other studies, which ranged between 49.2% and 68.7%.42,43
Our study Around 29.9% of the patients experienced severe anxiety. Which is comparable with the pervious study done in general surgery clinic at King Abdulaziz University Hospital in Jeddah, Saudi Arabia measures generalized anxiety disorder (GAD) prevalence was 24.3% is lower than that of other studies,41 which ranged between 48.6% and 73.3%.42,43 We hypothesize that the reason our study's results were lower than those of previous articles was because the questionnaire's timing varied depending on the period between diagnosis and management stage, which may have affected respondents' responses.
When undergoing radiation therapy, the patient must lie alone on a table with a large machine overhead, which can cause anxiety, fear, and a sense of isolation. Radiation therapy side effects are also problematic; in the United States, approximately 350,000 cancer patients receive radiation therapy annually, and cancer patients often report fears of the treatment (such as being "burned," or causing sterility, sickness, or vomiting.44 Additionally, 60% of patients experience significant anxiety before treatment, and 80% of them after.42
Previous study found that among 1346 patients receiving radiation therapy for head and neck cancer, 46% experienced emotional distress, 26% experienced anxiety, 9% experienced depression, and 27% experienced claustrophobia. Women were significantly more likely to experience emotional distress, depression, and anxiety (P < 0.001).45 Anxiety is listed as one of the common systemic toxicities of radiation treatment, along with pain, fatigue, and anorexia.46 Therefore, it is possible that the anxiety observed in our patients was a side effect of the radiation.
In our study, surgery showed a borderline protective association with anxiety (AOR = 0.29, 95% CI0.08-1.01, P = 0.05). Previous studies showed the psychological dysfunction rate among patients who had surgery for breast cancer ranged from 30 to 47%. There was no discernible difference between patients who had modified radical mastectomy and those who had breast-conserving surgery.47
It is important to identify depression in breast cancer patients because it has significant effects on the course and prognosis of the disease.44
Research has shown that psychological factors, such as stress and depression, can affect a person's overall quality of life and the course of their illness after receiving a cancer diagnosis. For these patients, concurrent psychiatric counseling will improve their quality of life, and psychiatric therapy for cancer patients should aim to increase resilience in addition to treating depression, anxiety, and stress.44
5. CONCLUSION
Depression and anxiety are common psychological illnesses among females with breast cancer. Psychological intervention should be directed towards high-risk patients. Psychological support program should be facilitated for the patients in order to improve their clinical outcomes.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Ethical approval
This study was approved by the Institutional Review Board (IRB) at Fakeeh College for Medical Sciences (Approval No: 530/IRB/2023).
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
LAH: Conceptualization, investigation, methodology, resources, validation, writing- original draft, writing – review and editing.
HMA, SMA, RTS, AKA: Investigation, resources, validation, writing- original draft, writing – review and editing.
REFERENCES
- da Silva PA, Riul SS. Breast cancer: risk factors and early detection. Rev Bras Enferm. 2011;64(6):1016-21. [PubMed] DOI: 1590/s0034-71672011000600005
- National Cancer Institute - INCA. Breast cancer. 2022. Available from: https://www.gov.br/inca/pt-br/assuntos/cancer/tipos/mama. Accessed March 17, 2025
- Almutlaq BA, Almuazzi RF, Almuhayfir AA. Breast cancer in Saudi Arabia and its possible risk factors. J Cancer Policy. 2017;12:83-9. DOI: 1016/j.jcpo.2017.03.004
- Bray F, Laversanne M, Sung H. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-63. [PubMed] DOI: 3322/caac.21834
- Xiong X, Zheng LW, Ding Y. Breast cancer: pathogenesis and treatments. Signal Transduct Target Ther. 2025;10(1):49. [PubMed] DOI: 1038/s41392-024-02108-4
- Alyami HS, Naser AY, Dahmash EZ. Clinical and therapeutic characteristics of cancer patients in the southern region of Saudi Arabia: a cross-sectional study. Int J Environ Res Public Health. 2021;18(12). [PubMed] DOI: 3390/ijerph18126654
- Hameed HA, Naser AY, Talib NM. Clinical and therapeutic characteristics and medical cost of managing cancer patients in Al-Anbar, Iraq: a cross-sectional study. Saudi Pharm J. 2022;30(12):1802-8. [PubMed] DOI: 1016/j.jsps.2022.10.009
- Alyami HS, Naser AY, Alyami MH, Banihameem IS, Almusabi M, Alqahtani AM, et al. Clinical and therapeutic characteristics of hospitalized cancer patients in the Najran Region of Saudi Arabia: a cross-sectional study. Saudi Pharm J. 2022;12(4):245-54. DOI: 22146/jmpf.78654
- Kedida BD, Mukacho MM, Alemayehu M. Women's experiences with breast cancer during diagnosis and therapy, Wolaita, Ethiopia: a qualitative study. BMC Womens Health. 2024;24(1):176. [PubMed] DOI: 1186/s12905-024-03016-z
- Drageset S, Lindstrøm TC, Giske T, Underlid K. "The support I need": women's experiences of social support after having received breast cancer diagnosis and awaiting surgery. Cancer Nurs. 2012;35(6):E39-47. [PubMed] DOI: 1097/NCC.0b013e31823634aa
- Epping-Jordan JE, Compas BE, Osowiecki DM. Psychological adjustment in breast cancer: processes of emotional distress. Health Psychol. 1999;18(4):315-26. [PubMed] DOI: 1037//0278-6133.18.4.315
- Bower JE. Behavioral symptoms in patients with breast cancer and survivors. J Clin Oncol. 2008;26(5):768-77. [PubMed] DOI: 1200/JCO.2007.14.3248
- Naser AY, Hameed AN, Mustafa N. Depression and anxiety in patients with cancer: a cross-sectional study. Front Psychol. 2021;12:585534. [PubMed] DOI: 3389/fpsyg.2021.585534
- Lim CC, Devi MK, Ang E. Anxiety in women with breast cancer undergoing treatment: a systematic review. Int J Evid Based Healthc. 2011;9(3):215-35. [PubMed] DOI: 1111/j.1744-1609.2011.00221.x
- Maass SW, Roorda C, Berendsen AJ, Verhaak PF, de Bock GH. The prevalence of long-term symptoms of depression and anxiety after breast cancer treatment: a systematic review. Maturitas. 2015;82(1):100-8. [PubMed] DOI: 1016/j.maturitas.2015.04.010
- Mitchell AJ, Chan M, Bhatti H. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis. Lancet Oncol. 2011;12(2):160-74. [PubMed] DOI: 1016/S1470-2045(11)70002-X
- Alsairafi Z, Naser AY, Alsaleh FM, Awad A, Jalal Z. Mental health status of healthcare professionals and students in Kuwait during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(4). [PubMed] DOI: 3390/ijerph18042203
- Naser AY, Dahmash EZ, Al-Rousan R. Mental health status during COVID-19 outbreak in Jordan: a cross-sectional study. Brain Behav. 2020;10(8):e01730. [PubMed] DOI: 1002/brb3.1730
- Naser AY, Alwafi H, Amara NA. Epidemiology of depression and anxiety among undergraduate students. Int J Clin Pract. 2021;75(9):e14414. [PubMed] DOI: 1111/ijcp.14414
- Alhemedi AJ, Qasaimeh MG, Abdo N. Depression among university students in Jordan after the COVID-19 pandemic: a cross-sectional study. Psychol Res Behav Manag. 2023;16:4237-49. [PubMed] DOI: 2147/PRBM.S436293
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13. [PubMed] DOI: 1046/j.1525-1497.2001.016009606.x
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-7. [PubMed] DOI: 1001/archinte.166.10.1092
- Allemani C, Weir HK, Carreira H. Global surveillance of cancer survival 1995–2009: analysis of data from 279 registries in 67 countries (CONCORD-2). Lancet. 2015;385(9972):977-1010. [PubMed] DOI: 1016/S0140-6736(14)62038-9
- Chirlaque MD, Salmerón D, Galceran J. Cancer survival in adult patients in Spain. Clin Transl Oncol. 2018;20(2):201-11. [PubMed] DOI: 1007/s12094-017-1710-6
- El Bcheraoui C, Basulaiman M, Wilson S. Breast cancer screening in Saudi Arabia: free but almost no takers. PLoS One. 2015;10(3):e0119051. [PubMed] DOI: 1371/journal.pone.0119051
- Al-Alaboud L, Kurashi N. Barriers of breast cancer screening programs among PHHC female physicians. Middle East J Fam Med. 2006;4(5):11-4.
- Schnitt SJ, Moran MS, Giuliano AE. Lumpectomy margins for breast cancer: guideline recommendations and impact. J Clin Oncol. 2020;38(20):2240-5. [PubMed] DOI: 1200/JCO.19.03213
- Fisher B, Anderson S, Bryant J. Twenty-year follow-up of a randomized trial for invasive breast cancer. N Engl J Med. 2002;347(16):1233-41. [PubMed] DOI: 1056/NEJMoa022152
- Nabholtz JM, Gligorov J. The role of taxanes in breast cancer treatment. Expert Opin Pharmacother. 2005;6(7):1073-94. [PubMed] DOI: 1517/14656566.6.7.1073
- Penel N, Adenis A, Bocci G. Cyclophosphamide-based metronomic chemotherapy: 10 years of experience. Crit Rev Oncol Hematol. 2012;82(1):40-50. [PubMed] DOI: 1016/j.critrevonc.2011.04.009
- Gewirtz DA. Mechanisms of antitumor effects of anthracyclines. Biochem Pharmacol. 1999;57(7):727-41. [PubMed] DOI: 1016/s0006-2952(98)00307-4
- Grubbé EH. Priority in the therapeutic use of X-rays. Radiology. 1993;21(2):156-62. DOI: 1148/21.2.156
- Boyages J. Radiation therapy and early breast cancer: current controversies. Med J Aust. 2017;207(5):216-22. [PubMed] DOI: 5694/mja16.01020
- Vahdaninia M, Omidvari S, Montazeri A. Predictors of anxiety and depression in breast cancer patients. Soc Psychiatry Psychiatr Epidemiol. 2010;45(3):355-61. [PubMed] DOI: 1007/s00127-009-0068-7
- Reich M, Lesur A, Perdrizet-Chevallier C. Depression, quality of life and breast cancer: a review. Breast Cancer Res Treat. 2008;110(1):9-17. [PubMed] DOI: 1007/s10549-007-9706-5
- Burgess C, Cornelius V, Love S, Graham J, Richards M, Ramirez A. Depression and anxiety in early breast cancer: a five-year study. BMJ. 2005;330(7493):702. [PubMed] DOI: 1136/bmj.38343.670868.D3
- Tsaras K, Papathanasiou IV, Mitsi D. Depression and anxiety in breast cancer patients: prevalence and factors. Asian Pac J Cancer Prev. 2018;19(6):1661-9. [PubMed] DOI: 22034/APJCP.2018.19.6.1661
- Dean C, Roberts MM, French K, Robinson S. Psychiatric morbidity after breast cancer screening. J Epidemiol Community Health. 1986;40(1):71-5. [PubMed] DOI: 1136/jech.40.1.71
- Batty GD, Russ TC, Stamatakis E, Kivimäki M. Psychological distress and site-specific cancer mortality. BMJ. 2017;356:j108. [PubMed] DOI: 1136/bmj.j108
- Faller H, Brähler E, Härter M. Unmet needs in gynecological vs breast cancer: quality of life impact. Patient Educ Couns. 2017;100(10):1934-42. [PubMed] DOI: 1016/j.pec.2017.05.031
- Bukhari AA, Alammari A. Prevalence of depression and anxiety in breast cancer patients: a cross-sectional study. World Fam Med J. 2022;20(3):6-14. Full Text
- Chen AM, Daly ME, Vazquez E. Depression among long-term survivors of head and neck cancer treated with radiation therapy. JAMA Otolaryngol Head Neck Surg. 2013;139(9):885-9. [PubMed] DOI: 1001/jamaoto.2013.4072
- Kriston L, Scholl I, Hölzel L, Simon D, Loh A, Härter M. The 9-item Shared Decision Making Questionnaire (SDM-Q-9): development and validation. Patient Educ Couns. 2010;80(1):94-9. [PubMed] DOI: 1016/j.pec.2009.09.034
- Mungase M, Chaudhury S, Patil AA, Jagtap B, Jain V. Stress, anxiety, depression and resilience in cancer radiotherapy patients. Ind Psychiatry J. 2021;30(2):346-52. [PubMed] DOI: 4103/ipj.ipj_78_20
- Pelland ME, Lambert L, Filion E. Depression, anxiety and claustrophobia in radiotherapy for head and neck cancer. Radiother Oncol. 2017;123(Suppl):S317-8.
- Koontz BF. Radiation therapy treatment effects: an evidence-based guide. New York: Demos; 2017.
- İzci F, İlgün AS, Fındıklı E, Özmen V. Psychiatric symptoms and psychosocial problems in breast cancer. J Breast Health. 2016;12(3):94-101. [PubMed] DOI: 5152/tjbh.2016.3041