Muhammad Arslan Zahid 1 , Sobia Jauhar 2 , Pervaiz Ali 3 , Madiha Rehman Khan 4 , Muhammad Abdul Rehman 5 , Muhammad Farhan Hasan 6
Authors affiliations:
Objective: To assess the current status of pre-operative anesthesia assessments in a tertiary care hospital and to determine possible changes that would lead to improvement in patient safety in the perioperative period.
Study Design: Clinical audit.
Methodology: This audit was conducted at a tertiary care hospital in Pakistan, over a six-month period, from 1 January 2024 to 30 June 2024. Pre-operative anesthesia assessment records of 601 patients were reviewed, and records of 100 patients were selected randomly each month. The audit was based on 22 General Quality Indicators (GQI) such as the patient particulars, the medical history of the patient, anesthesia history and details of the procedure/s carried out. Data were analyzed using IBM SPSS Statistics software Version 26. Descriptive statistics were used to examine the frequency and percentage of data completeness of each indicator. The relationship of the completeness rates to categorical variables was determined by chi-square tests.
Results: Documentation completeness varied across the 22 indicators. Indicators such as Name of Patient, Age and Gender achieved 100% completeness while critical areas like Anesthesia History and drug history/Medication in use had completeness rates below 30%, indicating significant gaps. Indicators were categorized as ‘Completely Filled’, ‘Adequately Filled’, ‘Moderately Filled’ and ‘Poorly Filled’. Findings will be presented to the Anesthesia Department, with plans for a follow-up audit to track improvements.
The completion level of documentation also differed with some of the 22 indicators as follows. Key components, including Name of Patient, Age and Gender, were 100% complete while essential data, including Anesthesia History and Medications in use, had completeness less than 30%. This was done by creating Categories which included ‘Completely Filled’ (90-100%), ‘Adequately Filled’ (80-89%), ‘Moderately Filled’ (70-79%) and ‘Poorly Filled’ (<70%). Recommendations will be made to the Anesthesia Department.
Conclusion: The following audit identifies where there is compliance and where there are gaps regarding pre-operative anesthesia documentation. Despite meeting some special criteria, important deficiencies persist in the documentation of the history of anesthetic use and medication administration. The above deficiencies could be rectified through practice of standard documentation procedures and training of workers, enhancing patient safety and quality of care.
Recommendations: Implementing structured templates that provide targeted staff training and conducting regular follow-up audits are recommended to increase the completeness and quality of pre-operative assessments.
Abbreviations: GQI: General Quality Indicators
Keywords: pre-operative assessment; anesthesia documentation; clinical audit; patient safety; tertiary care hospital; quality improvement; General Quality Indicators (GQI).
Citation: Zahid MA, Jauhar S, Ali P, Khan MR, Rehman MA, Hasan MF. Quality of pre-anesthesia assessment: a clinical audit in a tertiary care hospital in Pakistan. Anaesth. pain intensive care 2025;29(5):260-267.
DOI: 10.35975/apic.v29i5.2849
Received: January 07, 2025; Revised: January 12, 2024; Accepted: January 14, 2025
Preoperative evaluation is an essential part of perioperative care because it sets the foundation for the anesthesia management. Evaluation of specific risk factors for a particular patient as well as anticipated operational challenges can minimize risks of adverse effects during surgery to a great extent.1,2 It is argued that pre-operative assessment is often suboptimal and failure to do proper pre-operative risks assessments has been found to be related to the development of perioperative complications especially cardiovascular and respiratory.3,4 Comprehensive documentation of pre-operative assessment is crucial so that anesthesiologists and the perioperative team of carers are made aware of the patient’s health status.5
There is much evidence that points to the fact that pre-operative anesthesia assessments are highly recommended. The documentation of the practice is generally quite diverse in healthcare facilities.6 Lack of documentation consistency may result in inadequate information, misunderstandings, missed and crucial patient information that may harm patient safety.7 Tertiary care hospitals, where patients with complicated ailments and risk factors seeking treatments are admitted and documentation is critical in such settings.8 Similar audits in the same environment have shown that there are issues with documentation of key parameters, history, allergies and anesthesia plans.9,10
Clinical audit is a useful method in assessing and enhancing the quality of services being offered by disseminating care givers by examining the level of adherence to agreed standards and defining gaps that need to be closed.11 Auditing also gives specific information on the gaps of the documentation analysis for the requisite indicators, which can be used to improve patient care as well as minimize adverse implications of lack of documentation.12 This audit not only assesses the standard of documentation prior to surgery but also determines the weaknesses in the process, so improvement strategies can be implemented. For that reason, these ideas are significant in building dependable protocols for an anesthesia procedure in a tertiary care setting and enhancing the perioperative outcomes.
The performance of pre-operative anesthesia assessment in a tertiary care hospital was assessed for the quality of documentation and for identifying certain indicators that need to be upgraded through a clinical audit study. This audit is to determine whether anesthesia departments are providing optimal preoperative assessment with a view of improving anesthesia care and patient’s wellness.
The current clinical audit was undertaken in a tertiary care teaching hospital in Pakistan with an objective of evaluating the standards of pre-operative anesthesia evaluation. Audit was conducted retrospectively in compliance with the retrospective cohort design and documentation of pre-operative assessment from 1st January to 30th June 2024 was considered.
For this audit, the data comprised of 601 pre-operative assessment records and the average number of records samplings was 100 each month for the six months. This sample size was decided to get a diverse and representative sample of cases to understand the current practices of documentation adequately. In this study, records were selected through random sampling each month to ensure that the assessments recorded in the hospital were well represented whether concerning a male or female patient, be of any age or specialty of surgery.
The audit centered on the assessment of the GQIs 22 that are important for comprehensive preoperative assessment for anesthesia. These indicators were grouped into the core documentation components as demographic, medical, anesthesia, allergy and procedural details. Each of the indicators was checked concerning the completeness and there was adherence to the set criterion in the sense that the recorded information was complete and accurate.
Descriptive analysis involved the use of the IBM SPSS Statistics software (Version 26.0) to systematically compare the results from the observed documentation completeness against the ten indicators. The completeness rates for each of the indicators were described by frequencies and percentages. Cross-tabulation was applied to examine patterns in the documentation completeness between subgroups, including different ASA classes or specialties.
To ascertain their statistical significance, to compare completeness levels with categorical data, the Chi-square test was used to compare ASA class, Gender or Specialties. A p-value of 0.05 or less was used to define statistical significance for differences in documentation completeness across patient or procedure type.
The results from this audit will be given to the Anesthesia Department of the hospital to show what other documents can be considered to have good quality documentation and the ones that could be improved. These results will be best expressed through bar charts and frequency tables, created with the help of SPSS. A follow-up audit will be carried out with the aim of checking the effectiveness of the measures taken as a result of the current audit. This assessment will be conducted on-going to ensure documentation standard compliance, improving patient care and safety in the period perioperative period.
This audit was performed in line with the ethical consideration that is used in clinical audits. Participation of patients was voluntary and their data was anonymized to protect their identities; informed consent was also sought from the hospital’s IRB. Information was available only to certain personnel and the results were used strictly for research and development in the facility.
3.1. Demographic Characteristics
A total of 601 pre-operative assessment records were reviewed. The demographic details are presented in Table 1. The sample consisted of 272 male (45.3%) and 329 female (54.7%) patients. The majority of patients were classified as ASA Class II (67.2%), followed by ASA Class I (21.0%), Class III (9.8%) and Class IV (2.0%). The distribution of specialties indicates that the highest proportion of patients were from the General Surgery department, with notable representation from Cardiac Surgery, Neuro-surgery and Orthopedics. Table 1 provides a detailed breakdown of the demographic characteristics.
3.2. Quality Indicators and Completeness Criteria
The quality of pre-operative anesthesia assessments was evaluated using a set of predefined indicators and criteria for completeness. Table 2 lists the indicators evaluated in this study, along with the specific components required to meet the completeness standards. These indicators cover key areas, including demographic data, medical history, surgical and anesthetic history and pre-operative examination components.
3.3. Quality Indicators and Completeness Criteria
The quality of pre-operative anesthesia assessments was evaluated using a set of predefined indicators and criteria for completeness. Table 2 lists the indicators evaluated in this study, along with the specific components required to meet the completeness standards. These indicators cover key areas, including demographic data, medical history, surgical and anesthetic history and pre-operative examination components.
3.4. Completeness of Documentation
The completeness of each indicator was assessed based on the criteria outlined in Table 2. For analysis, completeness was categorized into four levels: ‘Completely Filled’ (90–100%), ‘Adequately Filled’ (80–90%), ‘Moderately Filled’ (70–80%) and ‘Poorly Filled’ (less than 70%).
Figure 1 shows the percentage that showed the completeness of the different indicators in pre-operative documentation. Under the assessment of documentation of the different indicators, it was realized that while 45.5% was fully documented as “Completely Filled,” about 22.7% was considered as “Moderately Filled,” and “Adequately Filled,” which show areas that require improvement in the documentation process.
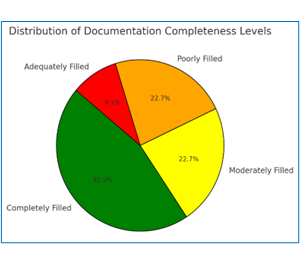
Figure 1: Distribution of Documentation Completeness Levels
Table 3 presents the frequency and completeness assessment for each indicator, highlighting areas with higher levels of deficiencies.
As illustrated in Figure 2, each of the above-mentioned indictors within the pre-operative documentation is documented to varying completeness rates. There is high completeness of data (presented in green) for the such indicators as patient details and anesthesia plan while there are significant gaps (red) in the pre-medication advice and weight documentation and therefore, the focus should be made on improving this section.
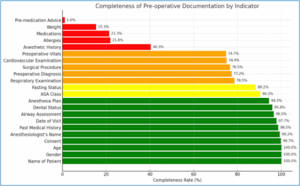
Figure 2: Completeness of pre-operative documentation by indicator
Out of 22 indicators, documentation for six indicators was marked as ‘Completely Filled’, 10 were ‘Adequately Filled’, four were ‘Moderately Filled’ and two were ‘Poorly Filled’. Indicators such as name of patient, age and gender achieved 100% completeness while others, like anesthetic history and pre-medication advice, fell below the acceptable standards. Consent was complete in 99.7% of cases and fasting status was documented in 88.2% of cases. Detailed results for each individual indicator are provided in Table 3.
This clinical audit was an effort to evaluate the standard of preoperative assessment undertaken by anesthesiologists in a tertiary care hospital. A total of 22 indicators were scored and their completeness ranged widely, suggesting there is much to commend about documentation practices as well as room for improvement. These less complex and more easily documented indicators like Name of Patient, Age and gender had very high completeness rates close to one signifying that demography documentation was consistent. Critical and history information, seen in Anesthetic History and Pre-medication Advice, were recorded sub-optimally, suggesting deficiencies in the assessment. In accordance with the previous research, the results of the present study highlighted the significance of incorporation of clear and detailed documentation while reporting anesthesia assessments in order to enhance patient safety.1-3
Measures like Consent and Anesthesiologist’s Name demonstrated a relatively good level of completeness, which corresponds to the expectations and requirements set by modern protocols, according to which, consent and the anesthesiologist’s identification should be part of the preoperative questionnaire.4 It is a legal necessity and helps inform the patient about the risks, benefits as well as other options available to them instead of anesthesia.5,6 Higher completeness in these areas indicates compliance to best practices and emphasizes of the continued need to adhere to such standards with all patients.7,8
The study reported lower completeness rates for indicators related to Surgical Procedure and Preoperative Diagnosis, as have other audits undertaken in surgical contexts.9 Failure to document some aspects of the surgeries may affect the perioperative planning and may lead to adverse events. Inadequate anesthetic history will result in wrong anesthesia strategies and consequences.10-12 For instance, previous anesthetic and operative history documentation before the surgery has been demonstrated to be linked with the decreased preoperative risks and the improved outcomes.13
The audit also identified that Medications already in use and Allergies were documented at below 30 per cent for both indicators. This is worrying because fake allergies and medications are dangerous especially for patients who require anesthesia, where an allergic reaction or incompatible drug interaction may be fatal.14
Other studies have also noted a lack of documentation on the patient’s medication history and allergy, insisting on proper procedures for documenting this information.15,16
Lack of complete documentation of medications may be due to time constraints or lack of prepared documents as recommended by prior research done on documentation procedures under pressure.17
Preoperative Vitals and Fasting Status was moderately documented with percentages ranging from 70%-90%. Fasting status is essential for anesthesia management to minimize the risks of aspiration during induction of anesthesia – an established risk factor in pre-anesthetic assessment.18 Documentation of vitals also helps in identification of a client’s health status at the start, which is critical in determining the risk before surgery.19
The average compliance rate computed across the indicators was about 85% which implies that, although in some areas high levels of documentation are attained, there is still much room for improvement in indicators labelled ‘Poorly Filled’. The variation in the level of completeness observed for the indicators is due to the differences that could be attributed to factors such as staff training, working pressure and organizational procedures. Measures focusing on the training of documentation and the organization of structured templates would likely increase the completeness of documentation in the areas currently flagged as missing.20,21
Future research should investigate whether such specific approaches as checklist-based documentation have the effect of increasing the levels of completion and accuracy of the pre-operative assessment. It is suggested that a standardized approach to the implementation of new improvements, together with periodic audits and feedback may assist in maintaining the pace of improvement over time. It is also worth exploring possibilities of how such documentation workflow might be changed to provide fewer barriers to completion from the side of the healthcare providers.
This clinical audit describes some of the key areas of compliance and areas of poor practice in pre-operative anesthesia assessments to a tertiary care hospital. Some of the aspects have always been highly documented while others such as anesthetic history and medication records were poorly documented. The deficiencies could be corrected by using proper documentations and assessment procedures where staff could be trained. Such improvements are critical for increasing patient safety and optimizing care during operations in critical clinical settings.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
MAZ: Concept
SJ and PA: Literature Review
MRK and MAR: Proof Reading
MFH: Editing
Authors affiliations:
- Muhammad Arslan Zahid, National Medical Centre, Karachi, Pakistan; Email: dr.arslanzahid@gmail.com; {ORCID:0009-0003-4707-0786}
- Sobia Jauhar, National Medical Centre, Karachi, Pakistan; Email: drsobiaali@hotmail.com
- Pervaiz Ali, National Medical Centre, Karachi, Pakistan; Email: pervaizali454@gmail.com
- Madiha Rehman Khan, National Medical Centre, Karachi, Pakistan; Email: madiha_rehman1@hotmail.com
- Muhammad Abdul Rehman, Hashim Medical City, Hayderabad, Pakistan; Email: marehman479@gmail.com
- Muhammad Farhan Hasan, Indus Hospital & Health Network, Karachi, Pakistan; Email: hunny.hasan94@gmail.com
ABSTRACT
Objective: To assess the current status of pre-operative anesthesia assessments in a tertiary care hospital and to determine possible changes that would lead to improvement in patient safety in the perioperative period.
Study Design: Clinical audit.
Methodology: This audit was conducted at a tertiary care hospital in Pakistan, over a six-month period, from 1 January 2024 to 30 June 2024. Pre-operative anesthesia assessment records of 601 patients were reviewed, and records of 100 patients were selected randomly each month. The audit was based on 22 General Quality Indicators (GQI) such as the patient particulars, the medical history of the patient, anesthesia history and details of the procedure/s carried out. Data were analyzed using IBM SPSS Statistics software Version 26. Descriptive statistics were used to examine the frequency and percentage of data completeness of each indicator. The relationship of the completeness rates to categorical variables was determined by chi-square tests.
Results: Documentation completeness varied across the 22 indicators. Indicators such as Name of Patient, Age and Gender achieved 100% completeness while critical areas like Anesthesia History and drug history/Medication in use had completeness rates below 30%, indicating significant gaps. Indicators were categorized as ‘Completely Filled’, ‘Adequately Filled’, ‘Moderately Filled’ and ‘Poorly Filled’. Findings will be presented to the Anesthesia Department, with plans for a follow-up audit to track improvements.
The completion level of documentation also differed with some of the 22 indicators as follows. Key components, including Name of Patient, Age and Gender, were 100% complete while essential data, including Anesthesia History and Medications in use, had completeness less than 30%. This was done by creating Categories which included ‘Completely Filled’ (90-100%), ‘Adequately Filled’ (80-89%), ‘Moderately Filled’ (70-79%) and ‘Poorly Filled’ (<70%). Recommendations will be made to the Anesthesia Department.
Conclusion: The following audit identifies where there is compliance and where there are gaps regarding pre-operative anesthesia documentation. Despite meeting some special criteria, important deficiencies persist in the documentation of the history of anesthetic use and medication administration. The above deficiencies could be rectified through practice of standard documentation procedures and training of workers, enhancing patient safety and quality of care.
Recommendations: Implementing structured templates that provide targeted staff training and conducting regular follow-up audits are recommended to increase the completeness and quality of pre-operative assessments.
Abbreviations: GQI: General Quality Indicators
Keywords: pre-operative assessment; anesthesia documentation; clinical audit; patient safety; tertiary care hospital; quality improvement; General Quality Indicators (GQI).
Citation: Zahid MA, Jauhar S, Ali P, Khan MR, Rehman MA, Hasan MF. Quality of pre-anesthesia assessment: a clinical audit in a tertiary care hospital in Pakistan. Anaesth. pain intensive care 2025;29(5):260-267.
DOI: 10.35975/apic.v29i5.2849
Received: January 07, 2025; Revised: January 12, 2024; Accepted: January 14, 2025
1. INTRODUCTION
Preoperative evaluation is an essential part of perioperative care because it sets the foundation for the anesthesia management. Evaluation of specific risk factors for a particular patient as well as anticipated operational challenges can minimize risks of adverse effects during surgery to a great extent.1,2 It is argued that pre-operative assessment is often suboptimal and failure to do proper pre-operative risks assessments has been found to be related to the development of perioperative complications especially cardiovascular and respiratory.3,4 Comprehensive documentation of pre-operative assessment is crucial so that anesthesiologists and the perioperative team of carers are made aware of the patient’s health status.5
There is much evidence that points to the fact that pre-operative anesthesia assessments are highly recommended. The documentation of the practice is generally quite diverse in healthcare facilities.6 Lack of documentation consistency may result in inadequate information, misunderstandings, missed and crucial patient information that may harm patient safety.7 Tertiary care hospitals, where patients with complicated ailments and risk factors seeking treatments are admitted and documentation is critical in such settings.8 Similar audits in the same environment have shown that there are issues with documentation of key parameters, history, allergies and anesthesia plans.9,10
Clinical audit is a useful method in assessing and enhancing the quality of services being offered by disseminating care givers by examining the level of adherence to agreed standards and defining gaps that need to be closed.11 Auditing also gives specific information on the gaps of the documentation analysis for the requisite indicators, which can be used to improve patient care as well as minimize adverse implications of lack of documentation.12 This audit not only assesses the standard of documentation prior to surgery but also determines the weaknesses in the process, so improvement strategies can be implemented. For that reason, these ideas are significant in building dependable protocols for an anesthesia procedure in a tertiary care setting and enhancing the perioperative outcomes.
The performance of pre-operative anesthesia assessment in a tertiary care hospital was assessed for the quality of documentation and for identifying certain indicators that need to be upgraded through a clinical audit study. This audit is to determine whether anesthesia departments are providing optimal preoperative assessment with a view of improving anesthesia care and patient’s wellness.
2. METHODOLOGY
The current clinical audit was undertaken in a tertiary care teaching hospital in Pakistan with an objective of evaluating the standards of pre-operative anesthesia evaluation. Audit was conducted retrospectively in compliance with the retrospective cohort design and documentation of pre-operative assessment from 1st January to 30th June 2024 was considered.
For this audit, the data comprised of 601 pre-operative assessment records and the average number of records samplings was 100 each month for the six months. This sample size was decided to get a diverse and representative sample of cases to understand the current practices of documentation adequately. In this study, records were selected through random sampling each month to ensure that the assessments recorded in the hospital were well represented whether concerning a male or female patient, be of any age or specialty of surgery.
The audit centered on the assessment of the GQIs 22 that are important for comprehensive preoperative assessment for anesthesia. These indicators were grouped into the core documentation components as demographic, medical, anesthesia, allergy and procedural details. Each of the indicators was checked concerning the completeness and there was adherence to the set criterion in the sense that the recorded information was complete and accurate.
Descriptive analysis involved the use of the IBM SPSS Statistics software (Version 26.0) to systematically compare the results from the observed documentation completeness against the ten indicators. The completeness rates for each of the indicators were described by frequencies and percentages. Cross-tabulation was applied to examine patterns in the documentation completeness between subgroups, including different ASA classes or specialties.
To ascertain their statistical significance, to compare completeness levels with categorical data, the Chi-square test was used to compare ASA class, Gender or Specialties. A p-value of 0.05 or less was used to define statistical significance for differences in documentation completeness across patient or procedure type.
The results from this audit will be given to the Anesthesia Department of the hospital to show what other documents can be considered to have good quality documentation and the ones that could be improved. These results will be best expressed through bar charts and frequency tables, created with the help of SPSS. A follow-up audit will be carried out with the aim of checking the effectiveness of the measures taken as a result of the current audit. This assessment will be conducted on-going to ensure documentation standard compliance, improving patient care and safety in the period perioperative period.
This audit was performed in line with the ethical consideration that is used in clinical audits. Participation of patients was voluntary and their data was anonymized to protect their identities; informed consent was also sought from the hospital’s IRB. Information was available only to certain personnel and the results were used strictly for research and development in the facility.
3. RESULTS
3.1. Demographic Characteristics
A total of 601 pre-operative assessment records were reviewed. The demographic details are presented in Table 1. The sample consisted of 272 male (45.3%) and 329 female (54.7%) patients. The majority of patients were classified as ASA Class II (67.2%), followed by ASA Class I (21.0%), Class III (9.8%) and Class IV (2.0%). The distribution of specialties indicates that the highest proportion of patients were from the General Surgery department, with notable representation from Cardiac Surgery, Neuro-surgery and Orthopedics. Table 1 provides a detailed breakdown of the demographic characteristics.
| Table 1: Demographic summary of study population | ||
| Parameter | Category | n (%) |
| Gender | Male | 272 (45.3) |
| Female | 329 (54.7) | |
| ASA Class | I | 126 (21.0) |
| II | 404 (67.2) | |
| III | 59 (9.8) | |
| IV | 12 (2.0) | |
| Specialty | General Surgery | 150 (25.0) |
| Cardiac Surgery | 100 (16.6) | |
| Neuro-Surgery | 80 (13.3) | |
| Orthopedics | 70 (11.6) | |
| Obstetrics | 50 (8.3) | |
3.2. Quality Indicators and Completeness Criteria
The quality of pre-operative anesthesia assessments was evaluated using a set of predefined indicators and criteria for completeness. Table 2 lists the indicators evaluated in this study, along with the specific components required to meet the completeness standards. These indicators cover key areas, including demographic data, medical history, surgical and anesthetic history and pre-operative examination components.
| Table 2: GQI indicators and completeness criteria | |
| Indicator | Predefined components for completeness |
| Name of Patient | Full name (first and last) present |
| Age | Age value recorded with unit (years/months) |
| Gender | Gender specified |
| Date of Visit | Date of visit clearly recorded (day/month/year) |
| Anesthesiologist’s Name | Name of anesthesiologist documented |
| Past Medical History | Details of previous or coexisting illnesses, with duration and any treatments |
| Preoperative Diagnosis | Diagnosis accurately recorded |
| Surgical Procedure | Surgical procedure specified |
| Anesthetic History | Details of previous surgeries, anesthesia type, duration and any complications |
| Medications | Specific type, dosage and administration route of medications listed |
| Allergies | Allergens and severity of reaction mentioned |
| Fasting Status | Fasting status mentioned or advice documented |
| Preoperative Vitals | Heart rate, blood pressure |
| Weight | Weight value with unit of measurement |
| Airway Assessment | Documentation of Mallampati grading, jaw slide and neck movement |
| Dental Status | Dental status noted (e.g., healthy, non-natural, broken, loose, missing or artificial) |
| Cardiovascular Examination | Auscultation or findings recorded for cardiovascular health |
| Respiratory Examination | Auscultation or findings recorded for respiratory health |
| ASA Class | ASA Classification recorded |
| Pre-medication Advice | Details on type, dosage and administration route of any pre-medications |
| Anesthesia Plan | Specific anesthesia plan documented |
| Consent | Signed consent available and accessible |
3.3. Quality Indicators and Completeness Criteria
The quality of pre-operative anesthesia assessments was evaluated using a set of predefined indicators and criteria for completeness. Table 2 lists the indicators evaluated in this study, along with the specific components required to meet the completeness standards. These indicators cover key areas, including demographic data, medical history, surgical and anesthetic history and pre-operative examination components.
3.4. Completeness of Documentation
The completeness of each indicator was assessed based on the criteria outlined in Table 2. For analysis, completeness was categorized into four levels: ‘Completely Filled’ (90–100%), ‘Adequately Filled’ (80–90%), ‘Moderately Filled’ (70–80%) and ‘Poorly Filled’ (less than 70%).
Figure 1 shows the percentage that showed the completeness of the different indicators in pre-operative documentation. Under the assessment of documentation of the different indicators, it was realized that while 45.5% was fully documented as “Completely Filled,” about 22.7% was considered as “Moderately Filled,” and “Adequately Filled,” which show areas that require improvement in the documentation process.
Figure 1: Distribution of Documentation Completeness Levels
Table 3 presents the frequency and completeness assessment for each indicator, highlighting areas with higher levels of deficiencies.
As illustrated in Figure 2, each of the above-mentioned indictors within the pre-operative documentation is documented to varying completeness rates. There is high completeness of data (presented in green) for the such indicators as patient details and anesthesia plan while there are significant gaps (red) in the pre-medication advice and weight documentation and therefore, the focus should be made on improving this section.
Figure 2: Completeness of pre-operative documentation by indicator
Out of 22 indicators, documentation for six indicators was marked as ‘Completely Filled’, 10 were ‘Adequately Filled’, four were ‘Moderately Filled’ and two were ‘Poorly Filled’. Indicators such as name of patient, age and gender achieved 100% completeness while others, like anesthetic history and pre-medication advice, fell below the acceptable standards. Consent was complete in 99.7% of cases and fasting status was documented in 88.2% of cases. Detailed results for each individual indicator are provided in Table 3.
| Table 3: Completeness of pre-operative documentation | ||||
| Indicator | n (%) | Complete | Incomplete | Assessment |
| Name of Patient | 601 (100.0) | 601 | 0 | ‘Completely Filled’ |
| Age | 601 (100.0) | 601 | 0 | ‘Completely Filled’ |
| Gender | 601 (100.0) | 601 | 0 | ‘Completely Filled’ |
| Date of Visit | 587 (97.7) | 587 | 14 | ‘Completely Filled’ |
| Anesthesiologist’s Name | 596 (99.2) | 596 | 5 | ‘Completely Filled’ |
| Past Medical History | 592 (98.5) | 592 | 9 | ‘Completely Filled’ |
| Preoperative Diagnosis | 464 (77.2) | 464 | 137 | ‘Moderately Filled’ |
| Surgical Procedure | 460 (76.5) | 460 | 141 | ‘Moderately Filled’ |
| Anesthetic History | 242 (40.3) | 242 | 359 | ‘Poorly Filled’ |
| Medications | 128 (21.3) | 128 | 473 | ‘Poorly Filled’ |
| Allergies | 131 (21.8) | 131 | 470 | ‘Poorly Filled’ |
| Fasting Status | 530 (88.2) | 530 | 71 | ‘Adequately Filled’ |
| Preoperative Vitals | 449 (74.7) | 449 | 152 | ‘Moderately Filled’ |
| Weight | 92 (15.3) | 92 | 508 | ‘Poorly Filled’ |
| Airway Assessment | 580 (96.5) | 580 | 21 | ‘Completely Filled’ |
| Dental Status | 576 (95.8) | 576 | 25 | ‘Completely Filled’ |
| Cardiovascular Examination | 450 (74.9) | 450 | 151 | ‘Moderately Filled’ |
| Respiratory Examination | 472 (78.5) | 472 | 128 | ‘Moderately Filled’ |
| ASA Class | 543 (90.3) | 543 | 57 | ‘Adequately Filled’ |
| Pre-medication Advice | 6 (1.0) | 6 | 594 | ‘Poorly Filled’ |
| Anesthesia Plan | 567 (94.3) | 567 | 33 | ‘Completely Filled’ |
| Consent | 599 (99.7) | 599 | 1 | ‘Completely Filled’ |
4. DISCUSSION
This clinical audit was an effort to evaluate the standard of preoperative assessment undertaken by anesthesiologists in a tertiary care hospital. A total of 22 indicators were scored and their completeness ranged widely, suggesting there is much to commend about documentation practices as well as room for improvement. These less complex and more easily documented indicators like Name of Patient, Age and gender had very high completeness rates close to one signifying that demography documentation was consistent. Critical and history information, seen in Anesthetic History and Pre-medication Advice, were recorded sub-optimally, suggesting deficiencies in the assessment. In accordance with the previous research, the results of the present study highlighted the significance of incorporation of clear and detailed documentation while reporting anesthesia assessments in order to enhance patient safety.1-3
Measures like Consent and Anesthesiologist’s Name demonstrated a relatively good level of completeness, which corresponds to the expectations and requirements set by modern protocols, according to which, consent and the anesthesiologist’s identification should be part of the preoperative questionnaire.4 It is a legal necessity and helps inform the patient about the risks, benefits as well as other options available to them instead of anesthesia.5,6 Higher completeness in these areas indicates compliance to best practices and emphasizes of the continued need to adhere to such standards with all patients.7,8
The study reported lower completeness rates for indicators related to Surgical Procedure and Preoperative Diagnosis, as have other audits undertaken in surgical contexts.9 Failure to document some aspects of the surgeries may affect the perioperative planning and may lead to adverse events. Inadequate anesthetic history will result in wrong anesthesia strategies and consequences.10-12 For instance, previous anesthetic and operative history documentation before the surgery has been demonstrated to be linked with the decreased preoperative risks and the improved outcomes.13
The audit also identified that Medications already in use and Allergies were documented at below 30 per cent for both indicators. This is worrying because fake allergies and medications are dangerous especially for patients who require anesthesia, where an allergic reaction or incompatible drug interaction may be fatal.14
Other studies have also noted a lack of documentation on the patient’s medication history and allergy, insisting on proper procedures for documenting this information.15,16
Lack of complete documentation of medications may be due to time constraints or lack of prepared documents as recommended by prior research done on documentation procedures under pressure.17
Preoperative Vitals and Fasting Status was moderately documented with percentages ranging from 70%-90%. Fasting status is essential for anesthesia management to minimize the risks of aspiration during induction of anesthesia – an established risk factor in pre-anesthetic assessment.18 Documentation of vitals also helps in identification of a client’s health status at the start, which is critical in determining the risk before surgery.19
The average compliance rate computed across the indicators was about 85% which implies that, although in some areas high levels of documentation are attained, there is still much room for improvement in indicators labelled ‘Poorly Filled’. The variation in the level of completeness observed for the indicators is due to the differences that could be attributed to factors such as staff training, working pressure and organizational procedures. Measures focusing on the training of documentation and the organization of structured templates would likely increase the completeness of documentation in the areas currently flagged as missing.20,21
5. FUTURE PROSPECT
Future research should investigate whether such specific approaches as checklist-based documentation have the effect of increasing the levels of completion and accuracy of the pre-operative assessment. It is suggested that a standardized approach to the implementation of new improvements, together with periodic audits and feedback may assist in maintaining the pace of improvement over time. It is also worth exploring possibilities of how such documentation workflow might be changed to provide fewer barriers to completion from the side of the healthcare providers.
6. CONCLUSION
This clinical audit describes some of the key areas of compliance and areas of poor practice in pre-operative anesthesia assessments to a tertiary care hospital. Some of the aspects have always been highly documented while others such as anesthetic history and medication records were poorly documented. The deficiencies could be corrected by using proper documentations and assessment procedures where staff could be trained. Such improvements are critical for increasing patient safety and optimizing care during operations in critical clinical settings.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
MAZ: Concept
SJ and PA: Literature Review
MRK and MAR: Proof Reading
MFH: Editing
REFERENCES
- Bunare M, Belay F, Tageza T. The practice of documentation at a pre-admission anesthesia clinic among anesthesia professionals for outpatient surgical patients. Biomed Rev J Basic Appl Med Sci. 2023;10(1):4–12. Full Text
- Tank GP, Tank P, Shah P. An observational study of role of medical record department in tertiary care teaching hospital. Natl J Physiol Pharm Pharmacol. 2023;13(1):138–42. DOI: 5455/njppp.2023.13.10486202219112022
- Azer M, Chandrasekar N, Jacqueline J, Lai V, Yang JJ, Zhuo T, et al. Patient compliance with preoperative instructions prior to an elective procedure: a quality improvement audit. Anaesth Intensive Care. 2023;51(3):226–8. ]PubMed] DOI: 1177/0310057X221141104
- Subramani Y, Querney J, Singh P, Zhang Y, Fochesato LA, Fatima N, et al. Preoperative anesthesia virtual video consultations in a preadmission clinic: quality improvement study. JMIR Perioper Med. 2024;7(1):e57541. ]]PubMed]] DOI: 2196/57541
- Hassan AG, Elqaffas EO, Elbouridy AM, Shawky MM, El-Fayoumi TA. A closed-loop clinical audit of surgical documentation of inpatient records at a tertiary level hospital in Egypt. Cureus. 2023;15(12). ]]PubMed]] DOI: 7759/cureus.49862
- Choo LY. The perioperative care of super morbidly obese parturients at King Edward Memorial Hospital for Women in Western Australia: a pilot clinical audit. Anaesth Intensive Care. 2023;51(3S):1–5.
- Thiagarajan M, Thomas V, Sebastian A, Thomas DS, Chandy R, Daniel S, et al. Compliance of surgical care in patients with carcinoma endometrium in a tertiary care centre in South India, to European Society of Gynaecologic Oncology (ESGO) quality indicators. Indian J Surg Oncol. 2024;15(3):557-562. ]]PubMed]] DOI: 1007/s13193-024-01954-6
- Shahbaz MA, Abdullah M, Rizwan M, Tanveer F, Amin N. Evaluation of patient satisfaction level and its predictor with pre-operative anesthesia care at Ali Fatima Hospital, Lahore. Int J Healthc Prof. 2024;3:3–7. DOI: 71395/ijhp.1.1.2024.2-6
- Mendonca J, Upadya M, Arora M. A prospective clinical audit of pre-operative fasting practices at a tertiary care hospital in India. Br J Surg. 2023;110(Suppl 6):znad258.157. DOI: 1093/bjs/znad258.157
- Hui JH, Hurley K, Murphy S. Comprehensive geriatric assessment in high-risk pre-admission clinic: service evaluation and clinical audit. Abstract
- Ahmad MB, Ansar F, Shakoor K, Adnan M, Naqi SA, Tahir Z, et al. Compliance with percutaneous endoscopic gastrostomy tube insertion guidelines and associated complications in a tertiary care setting: a clinical audit. Cureus. 2023;15(8). ]PubMed] DOI: 7759/cureus.43566
- Kurmanandh K, VamsiKrishna BK, Chandrasekhar K, Sampathirao B, Dandu N, Rekha YC. Pre-anaesthetic clinic teaching programme: new methods of teaching pre-anaesthetic checkup for undergraduate students. Full Text
- Burger R, Smit M, Plenge U, Gibbs MW. Informed consent for peripheral nerve blocks at a tertiary level hospital in South Africa: a quality improvement project. South Afr J Anaesth Analg. 2024;30(2):62–72. Full Text
- Gurunthalingam MP, Keche YN, Gaikwad NR, Dhaneria S, Singh MP. Appropriateness of surgical antibiotic prophylaxis in a tertiary care teaching hospital in central India: a retrospective analysis. Cureus. 2023;15(5). ]PubMed] DOI: 7759/cureus.38844
- Yang MM, Wang L, Yu ZH, Ying-Zhang. Implementing evidence-based pre-operative education in hospitalized patients undergoing total knee replacement: a best practice implementation project. JBI Evid Implement. 2024;22(1):53–60.
- Snober M, Mustafa Q. A clinical audit of orthopaedic clinical documentation of acute ankle fractures: a quality improvement project. Cureus. 2023;15(11). ]PubMed] DOI: 7759/cureus.49001
- Collada-Fernández L, Tapiador-Gómez G, García-Tomé L, Pardo-Mora MC, Díaz-Rodríguez MR, Prado-Rodríguez Barbero M, et al. Post-operative pain management in a surgical unit in a tertiary hospital in Spain: a best practice implementation project. JBI Evid Implement. 2024;22(1):29–36. ]PubMed] DOI: 1097/XEB.0000000000000462
- Ambulkar R, Kunte AR, Sarangi A, Nair S, Negussie T, Lima I, Tara M. Long-term sustainability of peri-operative infection control practices: implementation of “Clean Cut,” a checklist-based quality improvement program in India. Surg Infect. 2024;25(6):452–8. ]PubMed] DOI: 1089/sur.2023.334
- Priya V, Bais PS, Rastogi A, Shamim R, Aggarwal A, Patro A. Peri-operative management of diabetes mellitus: a survey of current practices among Indian anesthesiologists. J Anaesthesiol Clin Pharmacol. 2023;39(3):411–21. ]PubMed] DOI: 4103/joacp.joacp_463_21
- Koris J, Hopkins C. Improving the quality of the surgical preoperative assessment in a district general hospital. BMJ Open Qual. 2015;4(1):w3406. ]PubMed] DOI: 1136/bmjquality.u205381.w3406
- Shahzad S, Younas T, Khan EUD. Clinical audit on quality of paranesthesia evaluation. Anaesth. pain intensive care. 2021;25(1):15–20. DOI: 35975/apic.v25i1.1429