Elaf Hasan Mahdi 1 , Hussam Abbas Dawood 2
Authors affiliations:
Background & Objective: An arteriovenous fistula (AVF) is required in hemodialysis for better blood flow going into the dialysis machine. Almost all of the patients feel pain and anxiety from needle insertion when undergoing every session of hemodialysis. We conducted this study to determine the effect of the Valsalva maneuver on pain and anxiety levels in patients during needle insertion in the arteriovenous fistula for hemodialysis.
Methodology: A quasi-experimental design was used in the study. This study was conducted on 120 patients undergoing hemodialysis from September 19, 2024, to May 10, 2025, at the hemodialysis center at Imam Al-Hussein Medical City and the hemodialysis unit of Imam Al-Hassan Al-Mujtaba Teaching Hospital in Kerbala, Iraq. The G*Power calculator was used to determine the total number of participants.13 The sample of the study was obtained using a non-probability purposive sampling technique. The patients in the study group were demonstrated the method how to perform the Valsalva maneuver. The breath-holding typically lasted between 10 to 20 seconds during the maneuver. The Visual Analog Scale (VAS) was used to measure pain and anxiety levels.
Results: A significant reduction in pain levels was noticed among hemodialysis patients who received the Valsalva maneuver compared to the control group. The study group exhibited a more favorable pain profile, with 38% reporting mild pain and 60% reporting moderate pain. In the study group, 60% of patients reported mild anxiety, and 36% reported moderate anxiety with a mean anxiety score of 3.28 ± 1.429.
Conclusion: The findings of this study confirm the significant impact of the Valsalva maneuver in reducing pain level and anxiety among patients during needle insertion in AVF to undergo hemodialysis.
Abbreviations: AVF: arteriovenous fistula, BMI: Body Mass Index, CKD: Chronic kidney disease, NPS: Numeric Pain Scale
Keywords: anxiety; arteriovenous fistula; hemodialysis; pain; Valsalva maneuver
Citation: Mahdi EH, Dawood HA. Effect of Valsalva maneuver on pain level and anxiety during needle insertion in arteriovenous fistula among patients undergoing hemodialysis. Anaesth. pain intensive care 2025;29(5):367-375. DOI: 10.35975/apic.v29i5.2841
Received: July 09, 2025; Revised: July 26, 2025; Accepted: July 27, 2025
The global prevalence of chronic kidney disease has markedly risen over the last thirty years, with 77.5% of end-stage renal disease patients receiving kidney replacement therapy, with 43.1% undergoing dialysis exclusively. Hemodialysis (HD) constitutes 89% of the therapeutic interventions for patients with end-stage renal disease globally.1 Patients with end-stage renal disease necessitate alternative kidney therapies, including kidney transplantation, HD, or peritoneal dialysis.2 Dialysis functions as an artificial substitute for compromised renal function. Dialysis may be utilized for patients undergoing acute renal failure (temporary loss of kidney function) or for reasonably stable individuals with chronic kidney disease stage 5 (permanent kidney failure).3 The HD procedure required vascular access for extended durations.4 Vascular access is crucial for effective HD, attainable by an arteriovenous graft, an external arteriovenous shunt, a central venous catheter, or an arteriovenous fistula. Among all vascular access operations, fistulas show a superior survival rate and an extended success rate.5 The preferred method for safe vascular access in patients receiving long-term HD is the use of an arteriovenous fistula.6 Unfortunately, over one-fifth of HD patients consider the pain associated with arteriovenous fistula punctures as unpleasant and unacceptable, making it one of the most stressful issues. Patients on continuous HD feel pain from arteriovenous fistula punctures approximately 300 times a year since the procedure, which requires big needles and must be repeated three to four times per week, is necessary.7
Anxiety is a prevalent response to perceived dangers, including general hazards to life, health, and bodily integrity, among patients undergoing HD therapy with an arteriovenous shunt. Numerous investigations indicated that patients with chronic kidney disease receiving HD predominantly faced anxiety stemming from access issues, negative cognitions, and fears of mortality.8 Large needle exposure at the arteriovenous fistula (AVF) site is a major cause of stress as it occurs frequently.9
One of the simplest methods to learn and practice is the Valsalva maneuver. This method is evidence-based, safe, effective, patient-initiated, low-cost, and side-effect-free. This is accomplished by forcefully exhaling against a closed airway.10 The Valsalva maneuver involves elevating intraoral and thoracic pressures to 30 to 40 mm Hg for a duration of 10 to 20 seconds, performed while the patient is either seated or lying down. The exhalation effort is subsequently terminated abruptly. and the respiration restores.11 The Valsalva maneuver is a simple technique that alleviates venipuncture pain and discomfort without requiring specialized equipment.9 Investigation indicates that stimulating the brain region associated with pain processing can markedly impair the baroreceptor reflex's regulation of heart rate and blood pressure by inhibiting parasympathetic nervous system function and activating sympathetic nervous system activity.12
The primary objective of this study was to assess whether Valsalva maneuver performed by the patient during needle insertion in arteriovenous fistula among patients undergoing HD is effective in reducing the intensity of the pain and the level of anxiety.
The study was carried out on 120 patients undergoing HD from December 14th, 2024, to February 10th, 2025. The G*Power calculator was used to determine the total number of participants.13 The sample of the study was obtained using a non-probability purposive sampling technique. Patients with arteriovenous fistula, patients who don’t take painkillers and anti-anxiety medications, and patients who have had a fistula for more than four months. The samples were eliminated from patients with double-lumen catheters and patients who had fistulas for less than four months.
Patients were randomly divided into two groups using the sealed envelope technique. Sixty patients performed the maneuver, while the patients of the control group did not perform it. In this research, all patients were given written informed consent and an explanation of the intervention’s method (how to perform the Valsalva maneuver) as part of this interventional protocol. HD patients' application of the Valsalva maneuver during needle insertion through the consequence. To gather information, employed socio-demographic and clinical information questionnaires, including age, sex, marital status, educational level, chronic diseases, period from starting HD therapy, number of HD sessions per week, height, and weight {Body Mass Index (BMI).
The second instrument was the Numeric Pain Scale (NPS) to evaluate pain level during needle insertion in HD patients. The total reliability for this tool was 0.934. The patient was directed to select a number from a ten-point scale representing pain intensity, categorized as no pain (0), mild pain (1-3), moderate pain (4-6), severe pain (7-9), and the most acute pain (10).14
The third instrument Visual Analog Scale for Anxiety The instrument consists of a 10-cm horizontal line labeled with “not at all anxious” on the left and “very anxious” on the right. Patient was instructed to mark the line below to indicate his or her current anxiety level.9 The total reliability for this tool was 0.934.
The selection of an analytical approach is contingent upon the characteristics of the gathered data, with quantitative research employing descriptive and inferential statistics to examine numerical data.15 The data were analyzed and interpreted utilizing the Statistical Package for Social Sciences (SPSS), version 26.0. Cronbach's alpha (α), the Kolmogorov–Smirnov test, and Levene's test in inferential statistics demographic factors are described using the variance and SD. For differential statistical tests, used the independent sample t-test, Spearman's rank correlation coefficient, and point biserial correlation.
No analgesic medications were used in patients undergoing HD. The focus was primarily on the efficacy of the Valsalva maneuver itself as a non-pharmacological intervention to manage pain and anxiety during needle insertion.
Table 1 presents the descriptive analysis of sociodemographic characteristics of patients undergoing HD. The findings reveal that the average age for patients was 45.5 ± 13.9 vs. 34.4 ± 16.6 years in the study group compared to the control group. The variance test shows no significant difference in age group, indicating homogeneity of groups (Λ = 2.497, P = .117). The sex of patients reveals that males were dominant in the study group; 66 vs. 56%. The variance test shows no significant difference between two groups (Λ = 3.576, P = .062). Regarding level of education, the highest percentage in the study group (36%) and control group (44%) was seen with primary school graduation. The variance test shows no significant difference between two groups (Λ = .263, P = .609). More of the patients were married in the study group (76%) than in control group (66%). But the difference was not significant (Λ = .536, P = .466).
Table 2 above presents the descriptive analysis of clinical characteristics of patients undergoing HD. The findings reveal that the average duration of HD was almost equivalent, with no significant difference between the two groups (Λ = .015, P = .901). The number of HD sessions refers to “3+” among 70% of patients in the study group and 60% in the control group. The variance test shows no significant difference between the two groups (Λ = 1.798, P = .183). Regarding body mass index, there was no significant difference between the two groups (P =.365). Hypertension was noted in more patients of the study group than in the control group, but the difference between the two groups was not significant (P = .907).
Table 3 reveals significant differences in pain levels between the two groups. The study group demonstrated a substantial reduction in pain severity, with 38% reporting mild pain and 60% reporting moderate pain. In contrast, the control group had no cases of mild pain, with 58% reporting moderate pain and a notable 42% experiencing severe pain. The mean pain scores also reflect this difference; with the study group having a lower mean (3.92 ± 1.047) in the study group compared to the control group (6.24 ± 1.170).
Figure 1 reveals that patients in the study group experienced a moderate level of pain (60%) after engagement in the intervention, compared to patients in the control group (42%) who showed a severe pain level. The study group reported a mean anxiety score of 3.28 ± 1.429. compared to the control group with a score of 5.80 ± 1.512.
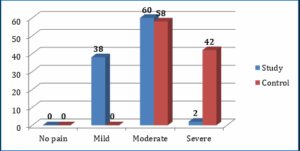
Figure 1: Level of pain among patients for study group and control group
Figure 2 shows that patients in the study group experienced a mild level of anxiety (60%) after engagement in the intervention compared to patients in the control group (64%) that showed moderate (64%) to severe (30%) levels of anxiety.
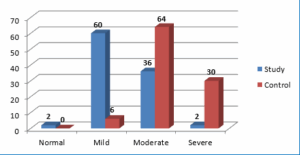
Figure 2: Comparative level of anxiety among patients of the two groups
Table 5 highlights significant differences in the level of pain between the study group, which underwent the Valsalva maneuver intervention, and the control group, which did not. The study group reported a considerably lower mean pain score (3.92 ± 1.047) compared to the control group (6.24 ± 6.24). The t-test analysis revealed a highly significant difference between the groups (t = -10.448, df = 98, P = .001), confirming the effectiveness of the Valsalva maneuver in significantly reducing pain levels among patients.
Table 6 illustrates significant differences in anxiety levels between the study group, which received the Valsalva maneuver intervention, and the control group, which did not. The study group had a lower mean anxiety score (M = 3.28, SD = 3.28) compared to the control group (M = 5.80, SD = 1.512). The t-test analysis revealed a highly significant difference between the two groups (t = -8.565, df = 98, P = .001), indicating that the Valsalva maneuver was effective in significantly reducing anxiety levels among patients.
The socio-demographic characteristics of patients undergoing HD play a crucial role in understanding their overall health status and response to clinical interventions. In this study, the lack of significant differences in age distribution suggests homogeneity between the groups, which is essential for a comparative analysis. Previous research supports that middle-aged and older adults constitute a significant proportion of HD patients, often due to the higher prevalence of chronic kidney disease (CKD) in these age groups.16 Sex distribution in this study showed no significant difference (Λ = 3.576, P = .062), indicating balanced gender representation. The studies suggest that males may experience faster disease progression due to factors such as hypertension and diabetes.17
Education level was another key variable examined, with the majority of patients in both groups having only primary-level education, with no significant differences between educational backgrounds, which may influence patients' understanding of their condition and adherence to treatment. Low health literacy has been associated with poorer disease management in HD patients, as evidenced by studies indicating that patients with limited education may struggle with treatment compliance and symptom recognition.18 Married individuals constituted the majority in both of the groups, with no significant differences observed (P = .466), perhaps due to social support from spouses.19 However, widowed individuals were more prevalent in the control group, compared to the study group (20% vs. 6%), which may have implications for emotional distress and coping mechanisms.20
In this study, the mean duration of HD was almost equivalent in the two groups, with the majority (68% vs. 64%) undergoing treatment for 1–5 years. The lack of a significant difference (Λ = 0.015, P = .901) suggests comparable treatment durations between groups, which is important for assessing intervention effects. Prior research indicates that longer dialysis vintage is associated with increased complications, such as vascular access problems and cardiovascular disease.21 However, the relatively short mean duration in this sample may reflect either early-stage CKD management or regional treatment patterns. The frequency of HD sessions per week was another key variable, with most patients in both groups receiving three or more sessions weekly (study group: 70%; control group: 60%). No significant difference was found (Λ = 1.798, P = .183), indicating similar treatment regimens.
This finding aligns with clinical guidelines recommending thrice-weekly HD as the standard for maintaining metabolic balance.22 However, emerging evidence suggests that more frequent sessions may improve survival and reduce complications,23 highlighting a potential area for future intervention studies.
Body mass index (BMI) distribution revealed that overweight patients constituted the largest proportion in both of the groups, with no significant differences (P = .365). Obesity (Class I–III) was present in 16% of the study group and 18% of the control group, consistent with global trends linking CKD to metabolic syndrome;24 although the "obesity paradox"—where higher BMI correlates with better survival in dialysis patients—has been observed in some studies.25
Hypertension (HT) was the most prevalent comorbidity, affecting 40% of the study group and 60% of the control group, followed by diabetes mellitus (DM) (study: 15%; control: 6%). The absence of significant differences (Λ = 0.014, P = .907) suggests comparable comorbidity burdens. These findings are consistent with epidemiological data identifying HT and DM as leading causes of CKD.26 Notably, 22% of the study group and 12% of the control group had no reported chronic diseases, possibly indicating rare or idiopathic kidney conditions. The high prevalence of HT underscores the need for integrated cardiovascular management in HD care.27 The findings presented in Table 3 demonstrate a significant reduction in pain levels among HD patients, who received the Valsalva maneuver intervention compared to the control group. The study group exhibited a more favorable pain profile, with 38% reporting mild pain and 60% reporting moderate pain; whereas, the control group had no patients with mild pain, 58% with moderate pain, and a concerning 42% with severe pain. The mean pain scores further reinforce these differences, with the study group (3.92 ± 1.047) experiencing significantly lower pain than the control group (6.24 ± 1.170). This is consistent with the findings of Sadek et al. (2024), who observed that 63.3% of pediatric HD patients in the Valsalva maneuver group reported mild pain post-intervention compared to only 3.3% in the control group.9 Similarly, Saputra & Kasiman (2020) found a significant reduction in pain intensity after VM application, reinforcing its role as an effective nonpharmacological intervention.28
There were significant differences in anxiety levels between HD patients who received the Valsalva maneuver intervention and those who did not. The study group exhibited markedly lower anxiety levels, with 60% reporting mild anxiety and 36% reporting moderate anxiety. In contrast, the control group showed substantially higher anxiety levels, with 64% experiencing moderate anxiety and a concerning 30% suffering from severe anxiety. These findings are further supported by the mean anxiety scores, which were significantly lower in the study group (3.28 ± 1.429) compared to the control group (5.80 ± 1.512). The reduction in anxiety levels in the study group (Table 4), where 60% reported mild anxiety compared to only 6% in the control group, further supports existing literature. Moosazadeh M, et al (2020) noted that the VM significantly decreased anxiety, with 63.3% of their VM group exhibiting moderate anxiety versus 96.7% severe anxiety in controls.9 Mohamed Eldesoky H and Elesawy F. (2021) found that VM led to a statistically significant decrease in both pain and anxiety during peripheral intravenous cannulation, corroborating the present study’s results.10
Our findings provide compelling evidence for the efficacy of the Valsalva maneuver in pain management for patients undergoing HD. The statistical analysis reveals a substantial difference in pain levels between the intervention and control groups, with the study group demonstrating a mean pain score nearly 40% lower than the control group (3.92 vs 6.24). The t-test result (t = -10.448, P = .001) confirms this difference is not only statistically significant but clinically meaningful too. These results align with emerging research on non-pharmacological pain interventions in dialysis settings. The VM's effectiveness may be attributed to its dual mechanism of action: activation of the parasympathetic nervous system through vagal stimulation, which modulates pain perception,29 and the gate control theory of pain, where the maneuver may compete with nociceptive signals at the spinal cord level.30
We did not use any analgesic, whether topical or systemic, in the control group. It might have been an ethically wrong practice. The pain scores and the anxiety scores are subjective feelings, and individual perception levels do not allow for exact quantitative measurements.
The analysis revealed that patients in the study group who received the Valsalva maneuver intervention experienced considerably lower pain levels compared to those in the control group. Specifically, the intervention group reported a higher percentage of mild and moderate pain levels, with no severe pain cases. In contrast, a significant proportion of control group patients experienced severe pain. The Valsalva maneuver had a notable effect on reducing anxiety levels among patients. The majority of the intervention group reported mild to moderate anxiety, with very few experiencing severe anxiety. On the other hand, the control group exhibited higher levels of moderate and severe anxiety, with a considerably higher mean anxiety score. The Valsalva maneuver is an effective and safe intervention for managing procedural pain and anxiety among hemodialysis patients. Its implementation requires minimal resources, making it highly applicable in clinical settings.
7. Data availability
The numerical data generated during this research is available from the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Acknowledgement
The researchers acknowledge the nursing staff of the hemodialysis center at Imam Al-Hussein Medical City and the hemodialysis unit of Imam Al-Hassan Al-Mujtaba Teaching Hospital for their cooperation in this study. Special thanks to all patients who participated in this study.
11. Authors’ contribution
EHM: Writing of the manuscript, critical revisions of the manuscript, analyzing data
HAD: Research design, methodology, write discussion and providing insights
Authors affiliations:
- 1. Elaf Hasan Mahdi, MSc, Adult Nursing, College of Nursing, University of Kerbala, Iraq; Email: h@s.uokerbala.edu.iq,
- Hussam Abbas Dawood, PhD, Adult Nursing, College of Nursing, University of Kerbala; Nursing Department, Al-Zahrawi University College, Kerbala, Iraq; Email: hussam.a@uokerbala.edu.iq
ABSTRACT
Background & Objective: An arteriovenous fistula (AVF) is required in hemodialysis for better blood flow going into the dialysis machine. Almost all of the patients feel pain and anxiety from needle insertion when undergoing every session of hemodialysis. We conducted this study to determine the effect of the Valsalva maneuver on pain and anxiety levels in patients during needle insertion in the arteriovenous fistula for hemodialysis.
Methodology: A quasi-experimental design was used in the study. This study was conducted on 120 patients undergoing hemodialysis from September 19, 2024, to May 10, 2025, at the hemodialysis center at Imam Al-Hussein Medical City and the hemodialysis unit of Imam Al-Hassan Al-Mujtaba Teaching Hospital in Kerbala, Iraq. The G*Power calculator was used to determine the total number of participants.13 The sample of the study was obtained using a non-probability purposive sampling technique. The patients in the study group were demonstrated the method how to perform the Valsalva maneuver. The breath-holding typically lasted between 10 to 20 seconds during the maneuver. The Visual Analog Scale (VAS) was used to measure pain and anxiety levels.
Results: A significant reduction in pain levels was noticed among hemodialysis patients who received the Valsalva maneuver compared to the control group. The study group exhibited a more favorable pain profile, with 38% reporting mild pain and 60% reporting moderate pain. In the study group, 60% of patients reported mild anxiety, and 36% reported moderate anxiety with a mean anxiety score of 3.28 ± 1.429.
Conclusion: The findings of this study confirm the significant impact of the Valsalva maneuver in reducing pain level and anxiety among patients during needle insertion in AVF to undergo hemodialysis.
Abbreviations: AVF: arteriovenous fistula, BMI: Body Mass Index, CKD: Chronic kidney disease, NPS: Numeric Pain Scale
Keywords: anxiety; arteriovenous fistula; hemodialysis; pain; Valsalva maneuver
Citation: Mahdi EH, Dawood HA. Effect of Valsalva maneuver on pain level and anxiety during needle insertion in arteriovenous fistula among patients undergoing hemodialysis. Anaesth. pain intensive care 2025;29(5):367-375. DOI: 10.35975/apic.v29i5.2841
Received: July 09, 2025; Revised: July 26, 2025; Accepted: July 27, 2025
1. INTRODUCTION
The global prevalence of chronic kidney disease has markedly risen over the last thirty years, with 77.5% of end-stage renal disease patients receiving kidney replacement therapy, with 43.1% undergoing dialysis exclusively. Hemodialysis (HD) constitutes 89% of the therapeutic interventions for patients with end-stage renal disease globally.1 Patients with end-stage renal disease necessitate alternative kidney therapies, including kidney transplantation, HD, or peritoneal dialysis.2 Dialysis functions as an artificial substitute for compromised renal function. Dialysis may be utilized for patients undergoing acute renal failure (temporary loss of kidney function) or for reasonably stable individuals with chronic kidney disease stage 5 (permanent kidney failure).3 The HD procedure required vascular access for extended durations.4 Vascular access is crucial for effective HD, attainable by an arteriovenous graft, an external arteriovenous shunt, a central venous catheter, or an arteriovenous fistula. Among all vascular access operations, fistulas show a superior survival rate and an extended success rate.5 The preferred method for safe vascular access in patients receiving long-term HD is the use of an arteriovenous fistula.6 Unfortunately, over one-fifth of HD patients consider the pain associated with arteriovenous fistula punctures as unpleasant and unacceptable, making it one of the most stressful issues. Patients on continuous HD feel pain from arteriovenous fistula punctures approximately 300 times a year since the procedure, which requires big needles and must be repeated three to four times per week, is necessary.7
Anxiety is a prevalent response to perceived dangers, including general hazards to life, health, and bodily integrity, among patients undergoing HD therapy with an arteriovenous shunt. Numerous investigations indicated that patients with chronic kidney disease receiving HD predominantly faced anxiety stemming from access issues, negative cognitions, and fears of mortality.8 Large needle exposure at the arteriovenous fistula (AVF) site is a major cause of stress as it occurs frequently.9
One of the simplest methods to learn and practice is the Valsalva maneuver. This method is evidence-based, safe, effective, patient-initiated, low-cost, and side-effect-free. This is accomplished by forcefully exhaling against a closed airway.10 The Valsalva maneuver involves elevating intraoral and thoracic pressures to 30 to 40 mm Hg for a duration of 10 to 20 seconds, performed while the patient is either seated or lying down. The exhalation effort is subsequently terminated abruptly. and the respiration restores.11 The Valsalva maneuver is a simple technique that alleviates venipuncture pain and discomfort without requiring specialized equipment.9 Investigation indicates that stimulating the brain region associated with pain processing can markedly impair the baroreceptor reflex's regulation of heart rate and blood pressure by inhibiting parasympathetic nervous system function and activating sympathetic nervous system activity.12
The primary objective of this study was to assess whether Valsalva maneuver performed by the patient during needle insertion in arteriovenous fistula among patients undergoing HD is effective in reducing the intensity of the pain and the level of anxiety.
2. METHODOLOGY
The study was carried out on 120 patients undergoing HD from December 14th, 2024, to February 10th, 2025. The G*Power calculator was used to determine the total number of participants.13 The sample of the study was obtained using a non-probability purposive sampling technique. Patients with arteriovenous fistula, patients who don’t take painkillers and anti-anxiety medications, and patients who have had a fistula for more than four months. The samples were eliminated from patients with double-lumen catheters and patients who had fistulas for less than four months.
Patients were randomly divided into two groups using the sealed envelope technique. Sixty patients performed the maneuver, while the patients of the control group did not perform it. In this research, all patients were given written informed consent and an explanation of the intervention’s method (how to perform the Valsalva maneuver) as part of this interventional protocol. HD patients' application of the Valsalva maneuver during needle insertion through the consequence. To gather information, employed socio-demographic and clinical information questionnaires, including age, sex, marital status, educational level, chronic diseases, period from starting HD therapy, number of HD sessions per week, height, and weight {Body Mass Index (BMI).
The second instrument was the Numeric Pain Scale (NPS) to evaluate pain level during needle insertion in HD patients. The total reliability for this tool was 0.934. The patient was directed to select a number from a ten-point scale representing pain intensity, categorized as no pain (0), mild pain (1-3), moderate pain (4-6), severe pain (7-9), and the most acute pain (10).14
The third instrument Visual Analog Scale for Anxiety The instrument consists of a 10-cm horizontal line labeled with “not at all anxious” on the left and “very anxious” on the right. Patient was instructed to mark the line below to indicate his or her current anxiety level.9 The total reliability for this tool was 0.934.
The selection of an analytical approach is contingent upon the characteristics of the gathered data, with quantitative research employing descriptive and inferential statistics to examine numerical data.15 The data were analyzed and interpreted utilizing the Statistical Package for Social Sciences (SPSS), version 26.0. Cronbach's alpha (α), the Kolmogorov–Smirnov test, and Levene's test in inferential statistics demographic factors are described using the variance and SD. For differential statistical tests, used the independent sample t-test, Spearman's rank correlation coefficient, and point biserial correlation.
No analgesic medications were used in patients undergoing HD. The focus was primarily on the efficacy of the Valsalva maneuver itself as a non-pharmacological intervention to manage pain and anxiety during needle insertion.
3. RESULTS
Table 1 presents the descriptive analysis of sociodemographic characteristics of patients undergoing HD. The findings reveal that the average age for patients was 45.5 ± 13.9 vs. 34.4 ± 16.6 years in the study group compared to the control group. The variance test shows no significant difference in age group, indicating homogeneity of groups (Λ = 2.497, P = .117). The sex of patients reveals that males were dominant in the study group; 66 vs. 56%. The variance test shows no significant difference between two groups (Λ = 3.576, P = .062). Regarding level of education, the highest percentage in the study group (36%) and control group (44%) was seen with primary school graduation. The variance test shows no significant difference between two groups (Λ = .263, P = .609). More of the patients were married in the study group (76%) than in control group (66%). But the difference was not significant (Λ = .536, P = .466).
| Table 1: Comparative socio-demographic characteristics of the patients in two groups | ||||
| Parameters | Study group
(N = 60) |
Control group
(N = 60) |
Variance test | |
| Age (year) | > 20 | 0 (0) | 2 (4) | Λ = 2.497 P = .117 Sig = NS |
| 20 – 29 | 9 (18) | 8 (16) | ||
| 30 – 39 | 8 (16) | 10 (20) | ||
| 40 – 49 | 12 (24) | 8 (16) | ||
| 50 – 59 | 11 (22) | 10 (20) | ||
| 60 – 69 | 7 (14) | 6 (12) | ||
| 70 – 79 | 3 (6) | 6 (12) | ||
| Total | 50 (100) | 50 (100) | ||
| M ± SD | 45.5 ± 13.9 | 34.4 ± 16.6 | ||
| Sex | Male | 33 (66) | 22 (44) | Λ = 3.576 P = .062 Sig = NS |
| Female | 17 (34) | 28 (56) | ||
| Total | 50 (100) | 50 (100) | ||
| Level of education | Can’t read / write | 4 (8) | 6 (12) | Λ = .263 P = .609 Sig = NS |
| Primary | 18 (36) | 22 (44) | ||
| Intermediate | 15 (30) | 9 (18) | ||
| Secondary | 6 (12) | 8 (16) | ||
| Diploma | 5 (10) | 3 (6) | ||
| Bachelor | 2 (4) | 2 (4) | ||
| Total | 50 (100) | 50 (100) | ||
| Marital status | Unmarried | 9 (18) | 7 (14) | Λ = .536 P = .466 Sig = NS |
| Married | 38 (76) | 33 (66) | ||
| Widowed/er | 3 (6) | 10 (20) | ||
| Total | 50 (100) | 50 (100) | ||
| No: Number, f: Frequency, %: Percentage, Λ: Levene's Test, P: Probability value, Sig: Significance, NS: Not significant, S: Significant, HS: Highly significant | ||||
Table 2 above presents the descriptive analysis of clinical characteristics of patients undergoing HD. The findings reveal that the average duration of HD was almost equivalent, with no significant difference between the two groups (Λ = .015, P = .901). The number of HD sessions refers to “3+” among 70% of patients in the study group and 60% in the control group. The variance test shows no significant difference between the two groups (Λ = 1.798, P = .183). Regarding body mass index, there was no significant difference between the two groups (P =.365). Hypertension was noted in more patients of the study group than in the control group, but the difference between the two groups was not significant (P = .907).
| Table 2: Distribution of patients according to their clinical characteristics | ||||
| Parameters
|
Study group
(N = 60) |
Control group
(N = 60) |
Variance test | |
| Duration of hemodialysis (year) | > 1 | 7 (14) | 10 (20) | Λ = .015 P = .901 Sig = NS |
| 1 – 5 | 34 (68) | 32 (64) | ||
| 6 – 10 | 9 (18) | 7 (14) | ||
| 11 – 15 | 0 (0) | 1 (2) | ||
| Total | 50 (100) | 50 (100) | ||
| M ± SD | 3.5 ± 2.6 | 3.15 ± 2.7 | ||
| Number of sessions | 1 | 1 (2) | 2 (4) | Λ = 1.798 P = .183 Sig = NS |
| 2 | 14 (28) | 18 (36) | ||
| 3 | 35 (70) | 30 (60) | ||
| Total | 50 (100) | 50 (100) | ||
| Body mass index ( | Underweight | 0 (0) | 1 (2) | Λ = .829 P = .365 Sig = NS |
| Normal | 18 (36) | 20 (40) | ||
| Overweight | 24 (48) | 20 (40) | ||
| Obesity I | 5 (10) | 7 (14) | ||
| Obesity II | 0 (0) | 0 (0) | ||
| Obesity III | 3 (6) | 6 (4) | ||
| Total | 50 (100) | 50 (100) | ||
| Presence of chronic disease | None | 11 (22) | 6 (12) | Λ = 014 P = .907 Sig = NS |
| DM | 6 (15) | 3 (6) | ||
| HT | 20 (40) | 30 (60) | ||
| HT+DM | 9 (18) | 6 (12) | ||
| HT+ Asthma | 1 (2) | 0 (0) | ||
| HT+DM+HF | 2 (4) | 3 (6) | ||
| HF+HT | 1 (2) | 2 (4) | ||
| Total | 50 (100) | 50 (100) | ||
| Data presented as n (%); DM: Diabetes mellitus, HT: Hypertension, HF: Heart failure; P < 0.05 considered as significant, | ||||
Table 3 reveals significant differences in pain levels between the two groups. The study group demonstrated a substantial reduction in pain severity, with 38% reporting mild pain and 60% reporting moderate pain. In contrast, the control group had no cases of mild pain, with 58% reporting moderate pain and a notable 42% experiencing severe pain. The mean pain scores also reflect this difference; with the study group having a lower mean (3.92 ± 1.047) in the study group compared to the control group (6.24 ± 1.170).
| Table 3: Comparative assessment of pain intensity in the two groups | ||||
| Pain intensity | Study group | Control group | ||
| N (%) | M ± SD | N (%) | M ± SD | |
| No pain | 0 (0) | 3.92 ± 1.047 | 0 (0) | 6.24 ± 1.170 |
| Mild | 19 (38) | 0 (0) | ||
| Moderate | 30 (60) | 29 (58) | ||
| Severe | 1 (2) | 21 (42) | ||
| Total | 50 (100) | 50 (100) | ||
| f: Frequency, %: Percentage, M: Mean of total score, SD Standard deviation No pain= 0, Mild= 1 – 3, Moderate= 4 – 6, Severe= 7 – 10 | ||||
Figure 1 reveals that patients in the study group experienced a moderate level of pain (60%) after engagement in the intervention, compared to patients in the control group (42%) who showed a severe pain level. The study group reported a mean anxiety score of 3.28 ± 1.429. compared to the control group with a score of 5.80 ± 1.512.
Figure 1: Level of pain among patients for study group and control group
Figure 2 shows that patients in the study group experienced a mild level of anxiety (60%) after engagement in the intervention compared to patients in the control group (64%) that showed moderate (64%) to severe (30%) levels of anxiety.
Figure 2: Comparative level of anxiety among patients of the two groups
Table 5 highlights significant differences in the level of pain between the study group, which underwent the Valsalva maneuver intervention, and the control group, which did not. The study group reported a considerably lower mean pain score (3.92 ± 1.047) compared to the control group (6.24 ± 6.24). The t-test analysis revealed a highly significant difference between the groups (t = -10.448, df = 98, P = .001), confirming the effectiveness of the Valsalva maneuver in significantly reducing pain levels among patients.
| Table 5: Significant differences in the level of pain in the two groups | |||||
| Variable | Group | Mean ± SD | t | df | P-value |
| Pain | Study | 3.92 ± 1.047 | -10.448 | 98 | .001 |
| Control | 6.24 ± 6.24 | ||||
| t: t-test, df: Degree of freedom, P: Probability, P < 0.05 considered as significant, | |||||
Table 6 illustrates significant differences in anxiety levels between the study group, which received the Valsalva maneuver intervention, and the control group, which did not. The study group had a lower mean anxiety score (M = 3.28, SD = 3.28) compared to the control group (M = 5.80, SD = 1.512). The t-test analysis revealed a highly significant difference between the two groups (t = -8.565, df = 98, P = .001), indicating that the Valsalva maneuver was effective in significantly reducing anxiety levels among patients.
| Table 6: Significant differences in the anxiety level in the two groups | |||||
| Variable | Group | Mean ± SD | t | df | P-value |
| Anxiety | Study | 3.28 ± 3.28 | -8.565 | 98 | .001
|
| Control | 5.80 ± 1.512 | ||||
| t: t-test, df: Degree of freedom, P < 0.05 considered as significant, | |||||
4. DISCUSSION
The socio-demographic characteristics of patients undergoing HD play a crucial role in understanding their overall health status and response to clinical interventions. In this study, the lack of significant differences in age distribution suggests homogeneity between the groups, which is essential for a comparative analysis. Previous research supports that middle-aged and older adults constitute a significant proportion of HD patients, often due to the higher prevalence of chronic kidney disease (CKD) in these age groups.16 Sex distribution in this study showed no significant difference (Λ = 3.576, P = .062), indicating balanced gender representation. The studies suggest that males may experience faster disease progression due to factors such as hypertension and diabetes.17
Education level was another key variable examined, with the majority of patients in both groups having only primary-level education, with no significant differences between educational backgrounds, which may influence patients' understanding of their condition and adherence to treatment. Low health literacy has been associated with poorer disease management in HD patients, as evidenced by studies indicating that patients with limited education may struggle with treatment compliance and symptom recognition.18 Married individuals constituted the majority in both of the groups, with no significant differences observed (P = .466), perhaps due to social support from spouses.19 However, widowed individuals were more prevalent in the control group, compared to the study group (20% vs. 6%), which may have implications for emotional distress and coping mechanisms.20
In this study, the mean duration of HD was almost equivalent in the two groups, with the majority (68% vs. 64%) undergoing treatment for 1–5 years. The lack of a significant difference (Λ = 0.015, P = .901) suggests comparable treatment durations between groups, which is important for assessing intervention effects. Prior research indicates that longer dialysis vintage is associated with increased complications, such as vascular access problems and cardiovascular disease.21 However, the relatively short mean duration in this sample may reflect either early-stage CKD management or regional treatment patterns. The frequency of HD sessions per week was another key variable, with most patients in both groups receiving three or more sessions weekly (study group: 70%; control group: 60%). No significant difference was found (Λ = 1.798, P = .183), indicating similar treatment regimens.
This finding aligns with clinical guidelines recommending thrice-weekly HD as the standard for maintaining metabolic balance.22 However, emerging evidence suggests that more frequent sessions may improve survival and reduce complications,23 highlighting a potential area for future intervention studies.
Body mass index (BMI) distribution revealed that overweight patients constituted the largest proportion in both of the groups, with no significant differences (P = .365). Obesity (Class I–III) was present in 16% of the study group and 18% of the control group, consistent with global trends linking CKD to metabolic syndrome;24 although the "obesity paradox"—where higher BMI correlates with better survival in dialysis patients—has been observed in some studies.25
Hypertension (HT) was the most prevalent comorbidity, affecting 40% of the study group and 60% of the control group, followed by diabetes mellitus (DM) (study: 15%; control: 6%). The absence of significant differences (Λ = 0.014, P = .907) suggests comparable comorbidity burdens. These findings are consistent with epidemiological data identifying HT and DM as leading causes of CKD.26 Notably, 22% of the study group and 12% of the control group had no reported chronic diseases, possibly indicating rare or idiopathic kidney conditions. The high prevalence of HT underscores the need for integrated cardiovascular management in HD care.27 The findings presented in Table 3 demonstrate a significant reduction in pain levels among HD patients, who received the Valsalva maneuver intervention compared to the control group. The study group exhibited a more favorable pain profile, with 38% reporting mild pain and 60% reporting moderate pain; whereas, the control group had no patients with mild pain, 58% with moderate pain, and a concerning 42% with severe pain. The mean pain scores further reinforce these differences, with the study group (3.92 ± 1.047) experiencing significantly lower pain than the control group (6.24 ± 1.170). This is consistent with the findings of Sadek et al. (2024), who observed that 63.3% of pediatric HD patients in the Valsalva maneuver group reported mild pain post-intervention compared to only 3.3% in the control group.9 Similarly, Saputra & Kasiman (2020) found a significant reduction in pain intensity after VM application, reinforcing its role as an effective nonpharmacological intervention.28
There were significant differences in anxiety levels between HD patients who received the Valsalva maneuver intervention and those who did not. The study group exhibited markedly lower anxiety levels, with 60% reporting mild anxiety and 36% reporting moderate anxiety. In contrast, the control group showed substantially higher anxiety levels, with 64% experiencing moderate anxiety and a concerning 30% suffering from severe anxiety. These findings are further supported by the mean anxiety scores, which were significantly lower in the study group (3.28 ± 1.429) compared to the control group (5.80 ± 1.512). The reduction in anxiety levels in the study group (Table 4), where 60% reported mild anxiety compared to only 6% in the control group, further supports existing literature. Moosazadeh M, et al (2020) noted that the VM significantly decreased anxiety, with 63.3% of their VM group exhibiting moderate anxiety versus 96.7% severe anxiety in controls.9 Mohamed Eldesoky H and Elesawy F. (2021) found that VM led to a statistically significant decrease in both pain and anxiety during peripheral intravenous cannulation, corroborating the present study’s results.10
| Table 4: Comparative assessment of anxiety level in the two groups | ||||
| Anxiety level | Study group | Control group | ||
| N (%) | Mean ± SD | N (%) | M ± SD | |
| Normal | 1 (2) | 3.28 ± 1.429 | 0 (0) | 5.80 ± 1.512 |
| Mild | 30 (60) | 3 (6) | ||
| Moderate | 18 (36) | 32 (64) | ||
| Severe | 1 (2) | 15 (30) | ||
| Total | 50 (100) | 50 (100) | ||
| f: Frequency, %: Percentage, Mean: Mean of total score, SD Standard deviation Normal= 0, Mild= 1 – 3, Moderate= 4 – 6, Severe= 7 – 10 | ||||
Our findings provide compelling evidence for the efficacy of the Valsalva maneuver in pain management for patients undergoing HD. The statistical analysis reveals a substantial difference in pain levels between the intervention and control groups, with the study group demonstrating a mean pain score nearly 40% lower than the control group (3.92 vs 6.24). The t-test result (t = -10.448, P = .001) confirms this difference is not only statistically significant but clinically meaningful too. These results align with emerging research on non-pharmacological pain interventions in dialysis settings. The VM's effectiveness may be attributed to its dual mechanism of action: activation of the parasympathetic nervous system through vagal stimulation, which modulates pain perception,29 and the gate control theory of pain, where the maneuver may compete with nociceptive signals at the spinal cord level.30
5. LIMITATIONS
We did not use any analgesic, whether topical or systemic, in the control group. It might have been an ethically wrong practice. The pain scores and the anxiety scores are subjective feelings, and individual perception levels do not allow for exact quantitative measurements.
6. CONCLUSION
The analysis revealed that patients in the study group who received the Valsalva maneuver intervention experienced considerably lower pain levels compared to those in the control group. Specifically, the intervention group reported a higher percentage of mild and moderate pain levels, with no severe pain cases. In contrast, a significant proportion of control group patients experienced severe pain. The Valsalva maneuver had a notable effect on reducing anxiety levels among patients. The majority of the intervention group reported mild to moderate anxiety, with very few experiencing severe anxiety. On the other hand, the control group exhibited higher levels of moderate and severe anxiety, with a considerably higher mean anxiety score. The Valsalva maneuver is an effective and safe intervention for managing procedural pain and anxiety among hemodialysis patients. Its implementation requires minimal resources, making it highly applicable in clinical settings.
7. Data availability
The numerical data generated during this research is available from the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Acknowledgement
The researchers acknowledge the nursing staff of the hemodialysis center at Imam Al-Hussein Medical City and the hemodialysis unit of Imam Al-Hassan Al-Mujtaba Teaching Hospital for their cooperation in this study. Special thanks to all patients who participated in this study.
11. Authors’ contribution
EHM: Writing of the manuscript, critical revisions of the manuscript, analyzing data
HAD: Research design, methodology, write discussion and providing insights
12. REFERENCES
- Al-Husayn AJA, Al-Jubboori AK, Alzeyadi S, Athbi HA, Faris SH, Hashim GA, et al. Adherence to self-care management among patients with end-stage renal disease at Habib Ibn-Mudaher in Kerbala City. Indian Journal of Public Health Research & Development 2018;9(8): 1057-1061. DOI:5958/0976-5506.2018.00870.7
- Sahathevan S, Khor BH, Ng, HM, Abdul Gafor, AH, Mat Daud, ZA, Mafra D, and Karupaiah T. Understanding development of malnutrition in hemodialysis patients: a narrative review. Nutrients 2020;12(10):3147. PMID: 33076282 PMCID: PMC7602515 DOI: 3390/nu12103147
- Dawood HA. Assessment of Patient’s Knowledge Regarding Hemodialysis Therapy at Imam Hussein Medical City in Holy Karbala Governorate. Indian Journal of Forensic Medicine & Toxicology 2020;14(3): 868-875. DOI: https://doi.org/10.37506/ijfmt.v14i3.10480
- Athbi HAA, Mohammed WK. 2012. Effect of Infection Control Education Program on Nurses Staff’s Knowledge in Hemodialysis Units in Baghdad Teaching Hospitals’. In Tenth National Scientific Conference (pp. 529-550).
- Babamohamadi H, Ameri Z, Asadi I, Asgari MR. Comparison of the Effect of EMLA™ Cream and the Valsalva Maneuver on Pain Severity during Vascular Needle Insertion in Hemodialysis Patients: A Controlled, Randomized, Clinical Trial. Evid Based Complement Alternat Med. 2022 Aug 31;2022:8383021. PMID: 36091600 PMCID: PMC9451986 DOI: 1155/2022/8383021
- Huber TS, Berceli SA, Scali ST, Neal D, Anderson EM, Allon M, et al. Arteriovenous Fistula Maturation, Functional Patency, and Intervention Rates. JAMA Surg. 2021 Dec 1;156(12):1111-1118. PMCID: PMC8459303 DOI: 1001/jamasurg.2021.4527
- Moosazadeh M, Nesami, MB, and Goudarzian, AH. Effect of cryotherapy on arteriovenous fistula puncture-related pain in hemodialysis patients: a systematic review and meta-analysis. Complement Ther Med. 2020 Mar;49:102326. DOI: 1016/j.ctim.2020.102326
- Nafisah S, Irawati M, Hidayati W. Anxiety of Hemodialysis Patient With Access Arteriovenous Fistula (AV-Shunt): A Qualitative Study. Nurse and Health: Jurnal Keperawatan 2021;10(2):240-248. DOI:36720/nhjk.v10i2.240
- Sadek EH, Elhay A, Azouz H. Effectiveness of Valsalva Maneuver on Pain Intensity and Anxiety in Children Undergoing Hemodialysis. Port Said Scientific Journal of Nursing 2024;11(3):112-141. DOI:21608/pssjn.2024.269654.1298
- Mohamed Eldesoky H, Elesawy F. Valsalva Maneuver: Reducing Procedural Pain and Anxiety for Patients Undergoing Peripheral Intravenous Cannulation. Egyptian Journal of Nursing and Health Sciences 2021;2(2):44-63. DOI: 21608/ejnhs.2021.234491
- Ghods AA, Roshani A, Mirmohammadkhani M, and Soleimani M. Effects of the Valsalva maneuver on pain and vasovagal reaction during the removal of the femoral arterial sheath after percutaneous coronary intervention: a randomized controlled trial. J Perianesth Nurs2022;37(6): 900-906. DOI: 1016/j.jopan.2022.01.016
- Di Credico C, Rosenberg M, Eastwood P, Buzzacott P, and Walsh J. Baroreflex sensitivity derived from the Valsalva maneuver: A physiological protective factor for anxiety induced by breathing CO2-enriched air. Int J Psychophysiol. 2022 Sep;179:101-109. DOI: 1016/j.ijpsycho.2022.06.019
- Bartlett J. Introduction to sample size calculation using G*Power. European Journal of Social Psychology 2019;1:36.
- Begum MR, Hossain MA. Validity and reliability of Visual Analogue Scale (VAS) for pain measurement. Journal of Medical Case Reports and Reviews [Internet]. 2022 Jan. 29 [cited 2025 Aug. 5];2(11). Available from: https://jmcrr.info/index.php/jmcrr/article/view/44
- O'Connor S. Secondary Data Analysis in Nursing Research: A Contemporary Discussion. Clin Nurs Res. 2020 Jun; 29(5):279-284. doi: 10.1177/1054773820927144. PMID: 32503394; PMCID: PMC7551215.
- Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. The Lancet 2017;389(10075):1238-1252. DOI: 1016/S0140-6736(16)32064-5
- Carrero JJ, Hecking M, Chesnaye NC, Jager KJ. 2018. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat Rev Nephrol. 2018 Mar;14(3):151-164. DOI: 1038/nrneph.2017.181
- Taylor DM, Fraser S, Dudley C, Oniscu GC, Tomson C, Ravanan R, Roderick P; ATTOM investigators. Health literacy and patient outcomes in chronic kidney disease: a systematic review. Nephrol Dial Transplant. 2018 Sep 1;33(9):1545-1558. DOI: 1093/ndt/gfx293
- Hoang VL, Green T, Bonner A. Examining social support, psychological status and health-related quality of life in people receiving haemodialysis. J Ren Care. 2022 Jun;48(2):102-111.. DOI: 1111/jorc.12380
- Masood A, Kamran F, Rashid S, Mazahir S. Life-orientation, Subjective Well-being and Social Support as Predictors of Quality of Life in Patients with End Stage Renal Disease. Bangladesh J Med Sci [Internet]. 2017 Jun. 9 [cited 2025 Aug. 5];16(3):346-53. Available from: https://banglajol.info/index.php/BJMS/article/view/32845. DOI: https://doi.org/10.3329/bjms.v16i3.32845
- The interaction analysis between advanced age and longer dialysis vintage on the survival of patients receiving maintenance hemodialysis. J Int Med Res. 2022 Apr;50(4):3000605221088557. PMCID: PMC9014717 DOI: 1177/03000605221088557
- Northover RE. 2024. Impact of the Application of a Nutrition Guideline for Adults on Hemodialysis (Doctoral dissertation, Grand Canyon University).
- Bello AK, Okpechi IG, Osman MA, Cho Y, Cullis B, Htay H, et al. Epidemiology of peritoneal dialysis outcomes. Nat Rev Nephro 2022;18(12):779-793. PMCID: PMC9483482 DOI: 1038/s41581-022-00623-7
- Kittiskulnam P, Thokanit NS, Katavetin P, Susanthitaphong P, Srisawat N, Praditpornsilpa K, et al. The magnitude of obesity and metabolic syndrome among the diabetic chronic kidney disease population: A nationwide study. PLoS One. 2018 May 9;13(5):e0196332. PMCID: PMC5942778 DOI: 1371/journal.pone.0196332
- Vareldzis R, Naljayan M, Reisin E. The incidence and pathophysiology of the obesity paradox: should peritoneal dialysis and kidney transplant be offered to patients with obesity and end-stage renal disease?. Curr Hypertens Rep. 2018;20:1-8. PMCID: PMC9058972 DOI: 1007/s11906-018-0882-y
- McQueen RB, Farahbakhshian S, Bell KF, Nair KV, Saseen JJ. Economic burden of comorbid chronic kidney disease and diabetes. J Med Econ. 2017;20(6):585-591. DOI: 1080/13696998.2017.1288127
- Vora, J, Cherney, D, Kosiborod, MN, Spaak, J, Kanumilli, N, Khunti, K, et al. Interrelationships between cardiovascular, renal, and metabolic diseases: underlying evidence and implications for integrated interdisciplinary care and management. Diabetes, Obes Metab, 2024 May;26(5):1567-1581. doi: 1111/dom.15485 . Epub 2024 Feb 8. PMID: 38328853.
- Saputra M, Kasiman S. 2020. Valsalva maneuver to decrease pain intensity during arteriovenous fistula insertion in hemodialysis patients. Jurnal Keperawatan Indonesia, 23 (2), 136–144 DOI:7454/jki.v23i2.645
- Forte G, Troisi G, Pazzaglia M, Pascalis VD, Casagrande M. 2022. Heart rate variability and pain: a systematic review. Brain Sci. 2022 Jan 24;12(2):153. doi: 10.3390/brainsci12020153. PMID: 35203917
- Heitler B. Primary Afferent Depolarization and the Gate Control Theory of Pain: A Tutorial Simulation. J Undergrad Neurosci Educ. 2023 Dec 17;22(1):A58-A65. PMID: 38322407 DOI: 59390/PWFC1224