Friskha Yuliana 1, Andi Hermawan 2, Danang Kuntoadi 3, Sigit Prasetya Utama 4
Authors affiliations:
Chronic pain associated with ankylosing spondylitis (AS) can exacerbate postoperative discomfort and heighten the overall treatment burden. Consequently, effective perioperative pain control warrants thorough attention. This case series presents our approach to pain management, emphasizing the utilization of peripheral nerve blocks alongside multimodal analgesia. This combined strategy offers opioid-sparing benefits and facilitates a smoother recovery process. Postoperatively, patients experienced marked pain relief, successful early mobilization, and no incidences of postoperative nausea and vomiting (PONV). These outcomes suggest that incorporating a multimodal pain management protocol significantly enhances postoperative recovery in AS patients undergoing total hip arthroplasty (THA).
Abbreviations: AS: Ankylosing Spondylitis, ASA-III: American Society of Anesthesiologists Class III, PENG: Pericapsular Nerve Group, PONV: Postoperative Nausea and Vomiting, THA: Total Hip Arthroplasty
Keywords: Ankylosing Spondylitis; Chronic Pain; Pain Management; Total Hip Arthroplasty
Citation: Yuliana F, Hermawan A, Kuntoadi D, Utama SP. Pain management in ankylosing spondylitis in patients undergoing total hip arthroplasty: A case series from Central Orthopedic Hospital, Indonesia. Anaesth. pain intensive care 2025;29(4):430-435. DOI: 10.35975/apic.v29i4.2833
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Ankylosing spondylitis (AS) is a chronic inflammatory condition characterized by pain and stiffness primarily affecting the spine and sacroiliac joints, often resulting in substantial functional limitations.1 Approximately 60% to 80% of individuals with AS experience chronic pain, especially in the lower back and hips, which are commonly involved sites in the inflammatory process. This persistent pain significantly impairs physical function and diminishes overall quality of life, restricting daily activities and increasing the risk of comorbid condition such as depression and anxiety.2
Hip arthritis is a frequent complications in patients with AS. Research shows that hip involvement occurs in 20% to 50% of cases, with some estimates indicating that nearly 30% of AS patients eventually develop severe hip arthritis.3 The connection between AS and hip arthritis is attributed to chronic inflammation that extends to tendons and ligaments, ultimately causing damage to the cartilage and bone structures of the hip joint. This leads to progressive pain, stiffness, and degenerative changes. When conservative treatments fail to provide relief, surgical options such as hip arthroscopy or total hip arthroplasty (THA) may be necessary to address advanced arthritis and improve joint function.4
Although THA offers significant benefits—including improved mobility and enhanced functionality—the procedure also poses challenges due to the inherent risks of major surgery. Postoperative complications such as persistent pain, extended recovery time, infection, and anesthesia-related issues may add to the patient’s burden.5 Additionally, surgery can potentially influence disease progression and joint degeneration in this population.
Effective perioperative pain management in patients with AS is essential not only to optimize surgical outcomes but also to support postoperative recovery and enhance overall quality of life. Traditional analgesic approaches relying on a single class of medication may fall short due to the complex pain mechanisms inherent in AS. In this context, a multimodal pain management strategy combining regional anesthesia techniques—such as the pericapsular nerve group (PENG) block—has gained prominence for providing targeted pain relief, comprehensive analgesia, and reducing the needs for systemic opioids.6,7 However, implementing multimodal pain control requires individualized planning and careful coordination, given the potential for interactions among different agents.
This case report presents a patient with AS who underwent THA and received a PENG block as part of perioperative pain management. We discuss the rationale for this approach, the clinical outcomes observed, and the potential implications for managing pain in this specialized patient group.
2.1. Case 1
A 28-year-old male patient, weighing 55 kg, presented with progressively worsening chronic pain in the left hip over the past year and was admitted for THA (Figure 1).
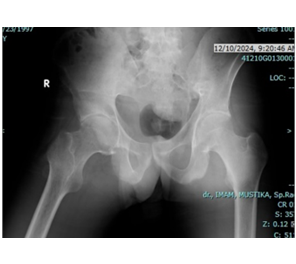
Figure 1: Case 1; Radiographic examination consistent with signs of ankylosing spondylitis
The patient was classified as ASA II. Anesthesia induction was achieved with intravenous administration of 2.5 mg midazolam, 70 mg propofol, and 150 mcg fentanyl. Perioperative pain management employed a multimodal analgesic regimen focused on opioid-sparing agents, including 1 g of paracetamol and 10 mg of dexamethasone administered 30 minutes prior to the surgical incision, alongside PENG block. The PENG block was performed under ultrasound guidance immediately before the incision (Figure 2).
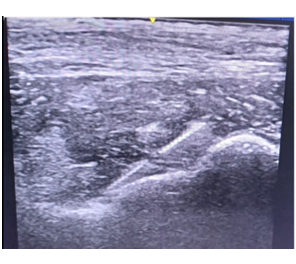
Figure 2: Case 1; Radiographic Ultrasound-guided PENG Block
2.2. Case 2
A 28-year-old man weighing 55 kg presented with progressively worsening pain in the right hip and was admitted for THA (Figure 3).

Figure 3: Case 2; Radiographic examination consistent with signs of ankylosing spondylitis
The patient was classified as ASA III. Anesthesia induction was achieved using intravenous administration of 60 mg propofol, 200 mcg fentanyl, and 30 mg atracurium. The analgesic regimen consisted of 1 g paracetamol and 10 mg dexamethasone given 30 minutes prior to the surgical incision, in addition to a PENG block. The PENG block was performed under ultrasound guidance immediately before the incision (Figure 4).
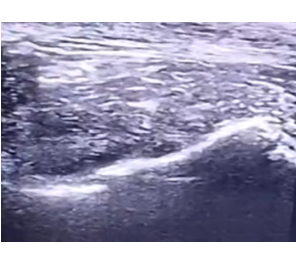
Figure 4: Case 2; Ultrasound-guided PENG Block
2.3. Case
A 28-year-old man weighing 55 kg presented with progressively worsening pain in the left hip and was admitted for THA (Figure 5).
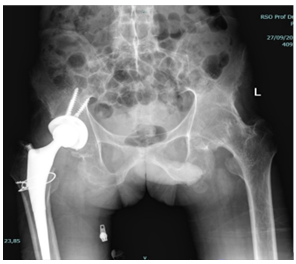
Figure 5: Case 3; Radiology examination consistent with signs of ankylosing spondylitis
He had previously undergone right THA. The patient was classified as ASA III. Anesthesia induction was carried out with intravenous administration of 60 mg propofol, 200 mcg fentanyl, and 30 mg atracurium. The analgesic plan included 1 g paracetamol and 10 mg dexamethasone administered 30 minutes before the incision, along with a PENG block performed under ultrasound guidance immediately prior to the surgery (Figure 6).
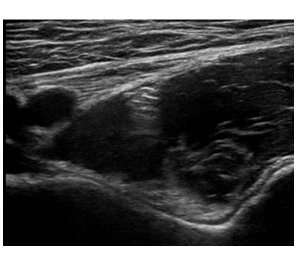
Figure 6: Case 3; Ultrasound-guided PENG Block
All patients remained in the supine position with the targeted leg slightly externally rotated during anesthesia. Strict aseptic technique was applied at the block site. Using a low-frequency curvilinear probe (2–5 MHz), placed transversely over the anterior inferior iliac spine (AIIS) and adjusted inferiorly to visualize the pubic ramus, key landmarks were identified. Through an in-plane technique, the femoral artery and iliopubic eminences were located. A 22-gauge, 100 mm nerve block needle was inserted from lateral to medial at a 30-45-degree angle relative to the ultrasound beam. After confirming negative aspiration, 20 mL of 0.25% levobupivacaine was injected. Intraoperatively, patients received 1 g of intravenous tranexamic acid to minimize bleeding. The surgeries lasted approximately two hours and were maintained under 1.5% sevoflurane with a 2:2 mixture of oxygen and nitrous oxide. Hemodynamic parameters remained stable throughout the procedures.
Postoperative analgesia consisted of administering 1 g of paracetamol every 8 hours. Postoperative assessments revealed that all patients remained hemodynamically stable, experienced no nausea or vomiting, and were able to initiate early mobilization successfully.
AS is a chronic, progressive inflammatory disease primarily affecting the spine and sacroiliac joints, often causing significant structural damage and impairment of function. Hip involvement is common among patients with AS and may necessitate THA to relieve pain and restore mobility. This case series illustrates the successful application of the PENG block for preoperative pain management in AS patients undergoing THA.
Patients with AS often face substantial challenges during surgery, particularly related to airway management and pain control, due to chronic inflammation and spinal rigidity. These factors complicate anesthesia delivery and increase the risk of postoperative complication.5 effective anesthesia management in AS requires a comprehensive, individualized approach. Spinal rigidity and postural deformities—especially affecting the cervical spine—can complicate airway assessment and management, underscoring the necessity for thorough preoperative evaluation. Measuring residual cervical mobility through cervical spine X-rays and range-of-motion assessments is essential.8
Anesthesiologists should anticipate potential ventilation and intubation difficulties. Applying the LEMON criteria can help predict the need for advanced airway techniques, such as retrograde intubation, video laryngoscopy, or fiberoptic intubation, to ensure safe and effective airway access.9
General anesthesia is typically preferred in AS patients due to its superior control over ventilation and airway management, while regional anesthesia is less frequently attempted.10 Agents with rapid onset and short duration, such as propofol, are commonly used. In this case series, a combination of general anesthesia and peripheral nerve block was employed to enhance analgesic efficacy and improve postoperative outcomes. Due to limited neck mobility, blind endotracheal intubation was successfully performed, with placement confirmed by capnography and auscultation. Hemodynamic parameters were continuously monitored throughout the procedure.
In addition to a careful anesthetic strategy, effective perioperative pain management is a vital component of care for patients with AS, particularly in THA. Employing multimodal analgesia is crucial to controlling postoperative pain while minimizing opioid use. This approach is especially important in AS patients, who often have compromised pulmonary function and are thus at increased risk for opioid-related respiratory depression.11 The multimodal analgesia regimen typically combines acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, opioids, and regional techniques such as nerve blocks or local infiltration.
One regional anesthesia method that has recently garnered attention is the PENG block. This targeted sensory nerve block can be administered safely and efficiently in the immediate preoperative period, delivering effective pain relief without the typical side effects associated with other regional blocks—such as postoperative muscle weakness and impaired mobility.12
In the present case, combining the PENG block with general anesthesia produced a synergistic effect that enhanced pain control. The PENG block specifically anesthetizes the nerve supplying the hip joint, providing targeted analgesia that reduces systemic opioid requirements. By limiting opioid use, this approach helps minimize adverse effects like sedation and respiratory depression, thereby preserving optimal respiratory function and hemodynamic stability throughout the procedure.6 Administered under ultrasound guidance prior to surgical incision, the PENG block enabled precise nerve localization, reducing the risks linked to blind injections. The favorable outcomes observed highlight the PENG block as an effective alternative to conventional analgesic strategies, particularly for patients vulnerable to opioid-related complication and those suffering from chronic pain.
A study comparing the effectiveness of the fascia iliaca block (FIB), a type of pericapsular nerve block, to the lumbar plexus block in patients undergoing hip arthroscopic demonstrated that FIB was not inferior to the lumbar plexus block in reducing postoperative pain scores in the post-anesthesia care unit.13 This finding suggests that the PENG block may serve as a viable alternative for postoperative pain management following hip surgeries, potentially offering advantages over traditional regional anesthesia techniques. Furthermore, a retrospective review evaluated the analgesic benefits of adding the PENG block to local infiltration anesthetics after primary THA. Among 123 patients meeting inclusion criteria—47 received the PENG block and 76 did not—the study found that the PENG block was associated with decreased hydromorphone consumption in the first 24 hours postoperatively.14
A recent meta-analysis study reported that the PENG block significantly reduces opioid use within 24 hours after hip arthroplasty compared to the FIB or local infiltration alone. However, there were no significant differences in numeric pain scores at 12, 24, and 48 hours post-surgery between groups.15 Quality of recovery scores at 24 and 48 hours showed significant improvement when the PENG block was included as part of a multimodal analgesic regimen alongside acetaminophen and celecoxib, despite pain score and antiemetic usage showing no notable differences.16 Another meta-analysis confirmed that the PENG block provides effective pain control for up to six hours postoperatively and prolongs the time to first opioid request following THA compared to placebo.17
Postoperative recovery is often impeded by pain, which can delay mobilization and increase the risk of complications such as deep vein thrombosis, pulmonary embolism, and extended hospital stays.5 Traditionally, postoperative analgesia after total joint replacement has relied on intravenous opioid administration or epidural analgesia, each presenting distinct benefits and drawbacks.18 The use of the PENG block in our cases resulted in a marked reduction in postoperative pain, enhancing patient comfort and enabling earlier mobilization. Early ambulation is particularly critical in patients with AS, who are predisposed to mobility-related complications due to their underlying condition. Additionally, the opioid-sparing effect of the PENG block helps minimize opioid-related adverse effects such as nausea, sedation, and respiratory depression, thereby decreasing the risk of prolonged hospitalization and improving patient satisfaction.
Furthermore, incorporating multimodal analgesia—including the PENG block, systemic analgesics such as paracetamol, and corticosteroids—significantly improved postoperative pain control and contributed to a faster recovery. Effective pain management not only enhances patient comfort but also facilitates early mobilization, which is essential for preventing complications like deep vein thrombosis or pulmonary embolism, especially in patients with limited mobility.
While multimodal analgesia has proven effective for managing postoperative pain after THA, there are challenges and limitations to consider. Regarding the PENG block, contraindications include patient refusal, infection at the injection site, allergy to local anesthetics, and coagulation disorders. Additionally, the PENG block alone cannot serve as the sole anesthesia for hip surgery, since the posteromedial hip capsule receives innervation from branches of the sacral plexus and sciatic nerve. Furthermore, not all analgesic approaches are suitable for every patient or feasible within outpatient, ambulatory, or fast-track surgical settings.19,20
Ultimately, the anesthetic management for patients with AS requires a multidisciplinary, tailored perioperative plan. By addressing the specific challenges associated with AS, anesthesiologists can optimize outcomes and improve the safety of surgical procedures. Future research should evaluate the long-term effects of the PENG block on functional recovery and patient satisfaction across diverse surgical populations.
Implementing a multimodal analgesia strategy—particularly using regional anesthesia techniques like the Pericapsular Nerve Group (PENG) block—offers targeted pain relief while reducing the risk of chronic postoperative pain and opioid dependence in AS patients undergoing major surgery. This case series highlights the importance of individualized pain management strategies and thorough preoperative planning to meet the unique needs of AS patients undergoing THA. It also supports the broader adoption of advanced regional analgesia techniques in clinical practice in the future.
5. Conflict of interest
Authors declare that there was no conflict of interest.
6. Ethical issues
Written informed consent was obtained from all of the patients to use the data for academic purposes.
7. Authors contribution
FY: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, editing and review, submission.
AH: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
DK: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, Manuscript editing and review.
SPU: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
Authors affiliations:
- Friskha Yuliana, MD, Department of Anesthesiology & Intensive Care, Orthopedic Prof. Dr. R. Soeharso Hospital, Surakarta, Indonesia; Email: friskha.yuliana@rso.go.id] {ORCID:0009-0000-7519-9681}
- Andi Hermawan, MD, Department of Anesthesiology & Intensive Care, Orthopedic Prof. Dr. R. Soeharso Hospital, Surakarta, Indonesia; Email: pakdeandi@gmail.com
- Danang Kuntoadi, MD, Department of Anesthesiology & Intensive Care, Orthopedic Prof. Dr. R. Soeharso Hospital, Surakarta, Indonesia; Email: danang.kuntoadi@rso.go.id
- Sigit Prasetya Utama, MD, Department of Anesthesiology & Intensive Care, Orthopedic Prof. Dr. R. Soeharso Hospital, Surakarta, Indonesia; Email: sigit.prasetya@rso.go.id
ABSTRACT
Chronic pain associated with ankylosing spondylitis (AS) can exacerbate postoperative discomfort and heighten the overall treatment burden. Consequently, effective perioperative pain control warrants thorough attention. This case series presents our approach to pain management, emphasizing the utilization of peripheral nerve blocks alongside multimodal analgesia. This combined strategy offers opioid-sparing benefits and facilitates a smoother recovery process. Postoperatively, patients experienced marked pain relief, successful early mobilization, and no incidences of postoperative nausea and vomiting (PONV). These outcomes suggest that incorporating a multimodal pain management protocol significantly enhances postoperative recovery in AS patients undergoing total hip arthroplasty (THA).
Abbreviations: AS: Ankylosing Spondylitis, ASA-III: American Society of Anesthesiologists Class III, PENG: Pericapsular Nerve Group, PONV: Postoperative Nausea and Vomiting, THA: Total Hip Arthroplasty
Keywords: Ankylosing Spondylitis; Chronic Pain; Pain Management; Total Hip Arthroplasty
Citation: Yuliana F, Hermawan A, Kuntoadi D, Utama SP. Pain management in ankylosing spondylitis in patients undergoing total hip arthroplasty: A case series from Central Orthopedic Hospital, Indonesia. Anaesth. pain intensive care 2025;29(4):430-435. DOI: 10.35975/apic.v29i4.2833
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Ankylosing spondylitis (AS) is a chronic inflammatory condition characterized by pain and stiffness primarily affecting the spine and sacroiliac joints, often resulting in substantial functional limitations.1 Approximately 60% to 80% of individuals with AS experience chronic pain, especially in the lower back and hips, which are commonly involved sites in the inflammatory process. This persistent pain significantly impairs physical function and diminishes overall quality of life, restricting daily activities and increasing the risk of comorbid condition such as depression and anxiety.2
Hip arthritis is a frequent complications in patients with AS. Research shows that hip involvement occurs in 20% to 50% of cases, with some estimates indicating that nearly 30% of AS patients eventually develop severe hip arthritis.3 The connection between AS and hip arthritis is attributed to chronic inflammation that extends to tendons and ligaments, ultimately causing damage to the cartilage and bone structures of the hip joint. This leads to progressive pain, stiffness, and degenerative changes. When conservative treatments fail to provide relief, surgical options such as hip arthroscopy or total hip arthroplasty (THA) may be necessary to address advanced arthritis and improve joint function.4
Although THA offers significant benefits—including improved mobility and enhanced functionality—the procedure also poses challenges due to the inherent risks of major surgery. Postoperative complications such as persistent pain, extended recovery time, infection, and anesthesia-related issues may add to the patient’s burden.5 Additionally, surgery can potentially influence disease progression and joint degeneration in this population.
Effective perioperative pain management in patients with AS is essential not only to optimize surgical outcomes but also to support postoperative recovery and enhance overall quality of life. Traditional analgesic approaches relying on a single class of medication may fall short due to the complex pain mechanisms inherent in AS. In this context, a multimodal pain management strategy combining regional anesthesia techniques—such as the pericapsular nerve group (PENG) block—has gained prominence for providing targeted pain relief, comprehensive analgesia, and reducing the needs for systemic opioids.6,7 However, implementing multimodal pain control requires individualized planning and careful coordination, given the potential for interactions among different agents.
This case report presents a patient with AS who underwent THA and received a PENG block as part of perioperative pain management. We discuss the rationale for this approach, the clinical outcomes observed, and the potential implications for managing pain in this specialized patient group.
2. CASE SERIES
2.1. Case 1
A 28-year-old male patient, weighing 55 kg, presented with progressively worsening chronic pain in the left hip over the past year and was admitted for THA (Figure 1).
Figure 1: Case 1; Radiographic examination consistent with signs of ankylosing spondylitis
The patient was classified as ASA II. Anesthesia induction was achieved with intravenous administration of 2.5 mg midazolam, 70 mg propofol, and 150 mcg fentanyl. Perioperative pain management employed a multimodal analgesic regimen focused on opioid-sparing agents, including 1 g of paracetamol and 10 mg of dexamethasone administered 30 minutes prior to the surgical incision, alongside PENG block. The PENG block was performed under ultrasound guidance immediately before the incision (Figure 2).
Figure 2: Case 1; Radiographic Ultrasound-guided PENG Block
2.2. Case 2
A 28-year-old man weighing 55 kg presented with progressively worsening pain in the right hip and was admitted for THA (Figure 3).
Figure 3: Case 2; Radiographic examination consistent with signs of ankylosing spondylitis
The patient was classified as ASA III. Anesthesia induction was achieved using intravenous administration of 60 mg propofol, 200 mcg fentanyl, and 30 mg atracurium. The analgesic regimen consisted of 1 g paracetamol and 10 mg dexamethasone given 30 minutes prior to the surgical incision, in addition to a PENG block. The PENG block was performed under ultrasound guidance immediately before the incision (Figure 4).
Figure 4: Case 2; Ultrasound-guided PENG Block
2.3. Case
A 28-year-old man weighing 55 kg presented with progressively worsening pain in the left hip and was admitted for THA (Figure 5).
Figure 5: Case 3; Radiology examination consistent with signs of ankylosing spondylitis
He had previously undergone right THA. The patient was classified as ASA III. Anesthesia induction was carried out with intravenous administration of 60 mg propofol, 200 mcg fentanyl, and 30 mg atracurium. The analgesic plan included 1 g paracetamol and 10 mg dexamethasone administered 30 minutes before the incision, along with a PENG block performed under ultrasound guidance immediately prior to the surgery (Figure 6).
Figure 6: Case 3; Ultrasound-guided PENG Block
All patients remained in the supine position with the targeted leg slightly externally rotated during anesthesia. Strict aseptic technique was applied at the block site. Using a low-frequency curvilinear probe (2–5 MHz), placed transversely over the anterior inferior iliac spine (AIIS) and adjusted inferiorly to visualize the pubic ramus, key landmarks were identified. Through an in-plane technique, the femoral artery and iliopubic eminences were located. A 22-gauge, 100 mm nerve block needle was inserted from lateral to medial at a 30-45-degree angle relative to the ultrasound beam. After confirming negative aspiration, 20 mL of 0.25% levobupivacaine was injected. Intraoperatively, patients received 1 g of intravenous tranexamic acid to minimize bleeding. The surgeries lasted approximately two hours and were maintained under 1.5% sevoflurane with a 2:2 mixture of oxygen and nitrous oxide. Hemodynamic parameters remained stable throughout the procedures.
Postoperative analgesia consisted of administering 1 g of paracetamol every 8 hours. Postoperative assessments revealed that all patients remained hemodynamically stable, experienced no nausea or vomiting, and were able to initiate early mobilization successfully.
3. DISCUSSION
AS is a chronic, progressive inflammatory disease primarily affecting the spine and sacroiliac joints, often causing significant structural damage and impairment of function. Hip involvement is common among patients with AS and may necessitate THA to relieve pain and restore mobility. This case series illustrates the successful application of the PENG block for preoperative pain management in AS patients undergoing THA.
Patients with AS often face substantial challenges during surgery, particularly related to airway management and pain control, due to chronic inflammation and spinal rigidity. These factors complicate anesthesia delivery and increase the risk of postoperative complication.5 effective anesthesia management in AS requires a comprehensive, individualized approach. Spinal rigidity and postural deformities—especially affecting the cervical spine—can complicate airway assessment and management, underscoring the necessity for thorough preoperative evaluation. Measuring residual cervical mobility through cervical spine X-rays and range-of-motion assessments is essential.8
Anesthesiologists should anticipate potential ventilation and intubation difficulties. Applying the LEMON criteria can help predict the need for advanced airway techniques, such as retrograde intubation, video laryngoscopy, or fiberoptic intubation, to ensure safe and effective airway access.9
General anesthesia is typically preferred in AS patients due to its superior control over ventilation and airway management, while regional anesthesia is less frequently attempted.10 Agents with rapid onset and short duration, such as propofol, are commonly used. In this case series, a combination of general anesthesia and peripheral nerve block was employed to enhance analgesic efficacy and improve postoperative outcomes. Due to limited neck mobility, blind endotracheal intubation was successfully performed, with placement confirmed by capnography and auscultation. Hemodynamic parameters were continuously monitored throughout the procedure.
In addition to a careful anesthetic strategy, effective perioperative pain management is a vital component of care for patients with AS, particularly in THA. Employing multimodal analgesia is crucial to controlling postoperative pain while minimizing opioid use. This approach is especially important in AS patients, who often have compromised pulmonary function and are thus at increased risk for opioid-related respiratory depression.11 The multimodal analgesia regimen typically combines acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, opioids, and regional techniques such as nerve blocks or local infiltration.
One regional anesthesia method that has recently garnered attention is the PENG block. This targeted sensory nerve block can be administered safely and efficiently in the immediate preoperative period, delivering effective pain relief without the typical side effects associated with other regional blocks—such as postoperative muscle weakness and impaired mobility.12
In the present case, combining the PENG block with general anesthesia produced a synergistic effect that enhanced pain control. The PENG block specifically anesthetizes the nerve supplying the hip joint, providing targeted analgesia that reduces systemic opioid requirements. By limiting opioid use, this approach helps minimize adverse effects like sedation and respiratory depression, thereby preserving optimal respiratory function and hemodynamic stability throughout the procedure.6 Administered under ultrasound guidance prior to surgical incision, the PENG block enabled precise nerve localization, reducing the risks linked to blind injections. The favorable outcomes observed highlight the PENG block as an effective alternative to conventional analgesic strategies, particularly for patients vulnerable to opioid-related complication and those suffering from chronic pain.
A study comparing the effectiveness of the fascia iliaca block (FIB), a type of pericapsular nerve block, to the lumbar plexus block in patients undergoing hip arthroscopic demonstrated that FIB was not inferior to the lumbar plexus block in reducing postoperative pain scores in the post-anesthesia care unit.13 This finding suggests that the PENG block may serve as a viable alternative for postoperative pain management following hip surgeries, potentially offering advantages over traditional regional anesthesia techniques. Furthermore, a retrospective review evaluated the analgesic benefits of adding the PENG block to local infiltration anesthetics after primary THA. Among 123 patients meeting inclusion criteria—47 received the PENG block and 76 did not—the study found that the PENG block was associated with decreased hydromorphone consumption in the first 24 hours postoperatively.14
A recent meta-analysis study reported that the PENG block significantly reduces opioid use within 24 hours after hip arthroplasty compared to the FIB or local infiltration alone. However, there were no significant differences in numeric pain scores at 12, 24, and 48 hours post-surgery between groups.15 Quality of recovery scores at 24 and 48 hours showed significant improvement when the PENG block was included as part of a multimodal analgesic regimen alongside acetaminophen and celecoxib, despite pain score and antiemetic usage showing no notable differences.16 Another meta-analysis confirmed that the PENG block provides effective pain control for up to six hours postoperatively and prolongs the time to first opioid request following THA compared to placebo.17
Postoperative recovery is often impeded by pain, which can delay mobilization and increase the risk of complications such as deep vein thrombosis, pulmonary embolism, and extended hospital stays.5 Traditionally, postoperative analgesia after total joint replacement has relied on intravenous opioid administration or epidural analgesia, each presenting distinct benefits and drawbacks.18 The use of the PENG block in our cases resulted in a marked reduction in postoperative pain, enhancing patient comfort and enabling earlier mobilization. Early ambulation is particularly critical in patients with AS, who are predisposed to mobility-related complications due to their underlying condition. Additionally, the opioid-sparing effect of the PENG block helps minimize opioid-related adverse effects such as nausea, sedation, and respiratory depression, thereby decreasing the risk of prolonged hospitalization and improving patient satisfaction.
Furthermore, incorporating multimodal analgesia—including the PENG block, systemic analgesics such as paracetamol, and corticosteroids—significantly improved postoperative pain control and contributed to a faster recovery. Effective pain management not only enhances patient comfort but also facilitates early mobilization, which is essential for preventing complications like deep vein thrombosis or pulmonary embolism, especially in patients with limited mobility.
While multimodal analgesia has proven effective for managing postoperative pain after THA, there are challenges and limitations to consider. Regarding the PENG block, contraindications include patient refusal, infection at the injection site, allergy to local anesthetics, and coagulation disorders. Additionally, the PENG block alone cannot serve as the sole anesthesia for hip surgery, since the posteromedial hip capsule receives innervation from branches of the sacral plexus and sciatic nerve. Furthermore, not all analgesic approaches are suitable for every patient or feasible within outpatient, ambulatory, or fast-track surgical settings.19,20
Ultimately, the anesthetic management for patients with AS requires a multidisciplinary, tailored perioperative plan. By addressing the specific challenges associated with AS, anesthesiologists can optimize outcomes and improve the safety of surgical procedures. Future research should evaluate the long-term effects of the PENG block on functional recovery and patient satisfaction across diverse surgical populations.
4. CONCLUSION
Implementing a multimodal analgesia strategy—particularly using regional anesthesia techniques like the Pericapsular Nerve Group (PENG) block—offers targeted pain relief while reducing the risk of chronic postoperative pain and opioid dependence in AS patients undergoing major surgery. This case series highlights the importance of individualized pain management strategies and thorough preoperative planning to meet the unique needs of AS patients undergoing THA. It also supports the broader adoption of advanced regional analgesia techniques in clinical practice in the future.
5. Conflict of interest
Authors declare that there was no conflict of interest.
6. Ethical issues
Written informed consent was obtained from all of the patients to use the data for academic purposes.
7. Authors contribution
FY: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, editing and review, submission.
AH: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
DK: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, Manuscript editing and review.
SPU: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
8. REFERENCES
- Boonen A, van der Linden SM. The burden of ankylosing spondylitis. J Rheumatol Suppl. 2006;78:4–11. PubMed
- Gau SY, Lee YH, Tsou HK, Huang JY, Chen X, Ye Z, et al. Patients with ankylosing spondylitis are associated with high risk of fibromyalgia: a nationwide population-based cohort study. Front Med. 2021;8:618594. PubMed DOI: 3389/fmed.2021.618594
- Vander Cruyssen B, Munoz-Gomariz E, Font P, Mulero J, De Vlam K, Boonen A, et al. Hip involvement in ankylosing spondylitis: epidemiology and risk factors associated with hip replacement surgery. Rheumatology. 2010;49(1):73–81. PubMed DOI: 1093/rheumatology/kep174
- Zhu W, He X, Cheng K, Zhang L, Chen D, Wang X, et al. Ankylosing spondylitis: etiology, pathogenesis, and treatments. Bone Res. 2019;7(1):22. PubMed DOI: 1038/s41413-019-0057-8
- Blizzard DJ, Penrose CT, Sheets CZ, Seyler TM, Bolognesi MP, Brown CR. Ankylosing spondylitis increases perioperative and postoperative complications after total hip arthroplasty. J Arthroplasty. 2017;32(8):2474–9. PubMed DOI: 1016/j.arth.2017.03.041
- Aliste J, Layera S, Bravo D, Jara Á, Muñoz G, Barrientos C, et al. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Reg Anesth Pain Med. 2021;46(10):874–8. PubMed DOI: 1136/rapm-2021-102997
- Lin DY, Brown B, Morrison C, Fraser NS, Chooi CSL, Cehic MG, et al. The Pericapsular Nerve Group (PENG) block combined with Local Infiltration Analgesia (LIA) compared to placebo and LIA in hip arthroplasty surgery: a multi-center double-blinded randomized-controlled trial. BMC Anesthesiol. 2022;22(1):252. PubMed DOI: 1186/s12871-022-01787-2
- Oliveira CRD. Ankylosing spondylitis and anesthesia. Rev Bras Anestesiol. 2007;57:214–22. PubMed DOI: 1590/s0034-70942007000200011
- Talikoti AT, Dinesh K, Kumar A. Ankylosing spondylitis: A challenge to anaesthesiologists due to difficulties in airway management and systemic involvement of disease. Indian J Anaesth. 2010;54(1):70–1. PubMed DOI: 4103/0019-5049.60507
- Saringcarinkul A. Anesthetic considerations in severe Ankylosing spondylitis. Chiang Mai Med J. 2009;48(2):57–63. Full Text
- Karam JA, Schwenk ES, Parvizi J. An update on multimodal pain management after total joint arthroplasty. J Bone Joint Surg Am. 2021;103(17):1652–62. PubMed DOI: 2106/JBJS.19.01423
- Fernicola, Jacob Tannehill I, Tucker CJ, Robert Volk W, Dickens JF. The pericapsular nerve group block for perioperative pain management for hip arthroscopy. Arthrosc Tech. 2021;10(7):e1799–803. PubMed DOI: 1016/j.eats.2021.03.029
- Badiola I, Liu J, Huang S, Kelly JD 4th, Elkassabany N. A comparison of the fascia iliaca block to the lumbar plexus block in providing analgesia following arthroscopic hip surgery: a randomized controlled clinical trial. J Clin Anesth. 2018;49:26–9. PubMed DOI: 1016/j.jclinane.2018.05.012
- Mysore K, Sancheti SA, Howells SR, Ballah EE, Sutton JL, Uppal V. Postoperative analgesia with pericapsular nerve group (PENG) block for primary total hip arthroplasty: a retrospective study. Can J Anaesth. 2020;67:1673–4. PubMed DOI: 1007/s12630-020-01751-z
- Kim E, Shin WC, Lee SM, Choi MJ, Moon NH. Efficacy of pericapsular nerve group block for pain reduction and opioid consumption after total hip arthroplasty: a meta-analysis of randomized controlled trials. Hip Pelvis. 2023;35(2):63. PubMed DOI: 5371/hp.2023.35.2.63
- Kukreja P, Uppal V, Kofskey AM, Feinstein J, Northern T, Davis C, et al. Quality of recovery after pericapsular nerve group (PENG) block for primary total hip arthroplasty under spinal anaesthesia: a randomised controlled observer-blinded trial. Br J Anaesth. 2023;130(6):773–9. PubMed DOI: 1016/j.bja.2023.02.017
- She C, Liu H. The efficacy of pericapsular nerve group block for reducing pain and opioid consumption after total hip arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2024;19(1):229. PubMed DOI: 1186/s13018-024-04707-x
- Maheshwari AV, Blum YC, Shekhar L, Ranawat AS, Ranawat CS. Multimodal pain management after total hip and knee arthroplasty at the Ranawat Orthopaedic Center. Clin Orthop Relat Res. 2009;467:1418–23. PubMed DOI: 1007/s11999-009-0728-7
- Kraus M, Foley B, Misra L, Hartigan D, Girardo M, Seamans D. A retrospective study of anesthetic considerations in hip arthroscopy: regional versus general. Open J Anesthesiol. 2018;8(12):295–304. DOI: 4236/ojanes.2018.812030
- De Leeuw MA, Zuurmond WWA, Perez R. The psoas compartment block for hip surgery: the past, present, and future. Anesthesiol Res Pract. 2011;2011(1):159541. PubMed DOI: 1155/2011/159541