Fatima Bibi 1, Shama Chaudhry 2, Hadia Riaz 3, Erum Gul 4, Rehana Yasmeen 5, Hina Ramzan 6, Haseeb Khaliq 7
Authors affiliations:
Background & objective: Eclampsia and HELLP syndrome are serious hypertensive diseases of pregnancy that are frequently admitted to the ICU. When it comes to seizure control and hypertension control, standardization of protocols in pain management is well established, although these are not commonly used; yet there is evidence that connects pain and adverse maternal outcomes. This systematic review and meta-analysis were used to assess the effectiveness of acute pain management protocols in reducing the maternal morbidity and other clinical outcomes in pregnant women admitted to the ICU for eclampsia or HELLP syndrome.
Methods: This systematic review and meta-analysis was conducted according to PRISMA 2020 guidelines. A systematic search was pursued in [PubMed], Scopus, Web of Science, and Cochrane databases for the studies produced till 2025. Inclusion criteria included RCTs, observational, and case report studies that focused on pain protocols in the obstetric ICUs. The key outcomes were maternal morbidity, ICU stay duration, and maternal-fetal survival. Assessment of risk of bias was done using the Newcastle-Ottawa Scale and Cochrane RoB tool. A random effect model of meta-analysis was used.
Results: 12 studies with 10, 153 patients were selected. Protocolized pain management, such as opioid- sparing and regional anesthesia, lowered the rate of maternal complications and stay in the ICU. The pooled OR for the better maternal outcomes was 1.23 (95% CI: 0.86–1.75), though not statistically significant. There was substantial heterogeneity (I² = 77%, p < 0.01), which was explained by protocol variation and disease severity variation.
Conclusion: Incorporating the structured pain management protocols in the obstetric ICU care for eclampsia and HELLP syndrome can ameliorate the maternal outcomes, but the current evidence is heterogeneous. Regarding the necessity of RCTs, further multicenter RCTs are needed to standardize pain protocols in the high-risk population.
Keywords: HELLP Syndrome; Anesthesia; Maternal Outcomes; Obstetric Complications; Meta-Analysis
Citation: Bibi F, Chaudhry S, Riaz H, Gul E, Yasmeen R, Ramzan H, Khaliq H. Integrating acute pain protocols in obstetric intensive care: the effect on maternal morbidity in eclampsia and HELLP syndrome. Anaesth. pain intensive care 2025;29(4):326-33. DOI: 10.35975/apic.v29i4.2817
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
The complications of hypertensive disorders during pregnancy with the most dramatic effect include eclampsia and HELLP (Hemolysis, Elevated Liver enzymes, and Low Platelet count) syndrome.1,2 These conditions often require admission to the intensive care unit (ICU) as a result of multi-organ involvement and the need for advanced supportive strategies.3 Although great attention is paid to controlling spasms, hypertension, and coagulopathy in these patients, pain control is relatively poorly covered in clinical practice guidelines and ICU protocols.4
Acute pain is not only is distressing, experience by the critically ill obstetric patients, but it can also have adverse effects as a result of enhanced sympathetic drive, immunosuppression, and delayed recovery.5,6 Inadequate analgesia is associated with increased morbidity, prolonged ICU stay, and poor postpartum recovery. Complicated physiologic changes that occur during pregnancy, aggravated by organ dysfunction in eclampsia and HELLP syndrome, make analgesic choices and their dosage difficult.7,8
However, recent evidence suggests that standard acute pain protocols, adapted to the obstetric ICU population, can decrease complications, increase patient comfort, and shorten stays in the ICU.9 These potential benefits notwithstanding, integration of pain protocols in obstetric ICUs is inconsistent with evidence of their efficacy for maternal outcomes not well established.10,11
This systematic review and meta-analysis is intended to assess the effectiveness of acute pain management protocols in preventing maternal morbidity of the ICU-admitted patients with eclampsia or HELLP syndrome. Through synthesis of the existing evidence, we aim to clarify whether the introduction of structured pain protocols will produce better clinical outcomes and can be recommended as a standard of care for the high-risk group.
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines were followed in this systematic review and meta-analysis. Nevertheless, this was not recorded on the PROSPERO database.
An extensive literature search was made on [PubMed], Scopus, Web of Science, and Cochrane Library databases for studies within the period up to March 2025. Search words used were combinations of “acute pain protocol”, “HELLP syndrome”, “eclampsia”, “obstetric ICU”, “maternal morbidity”, and “analgesia”. Appropriate Boolean operators were used for the refinement of results (AND, OR).
Studies were considered eligible if they were related to patients diagnosed with eclampsia or HELLP syndrome, admitted to an ICU, implemented an acute pain management strategy or protocol, and reported outcomes associated with maternal morbidity, ICU stay, seizure recurrence, maternal survival, or surgical intervention. Randomized controlled trials (RCTs), observational, and appropriate case reports were utilized in the study because of the rarity of the condition. Both reviews and editorials, the animal studies were excluded. Two independent screener reviewers screened both titles and abstracts; those meeting the criteria underwent full-text review. In case of a disagreement, it was solved based on discussion or with a third reviewer.
Data were abstracted with a standardized form of author/year, study design, sample size, confounders, interventions, outcomes, and key findings. Risk of bias was assessed utilizing the Cochrane Risk of Bias tool for RCTs and observational studies using the Newcastle-Ottawa Scale (NOS).
Meta-analysis was performed, and odds ratios (ORs) with 95% CIs were calculated. Since heterogeneity in the scope of intervention and study populations were expected, a random-effects model with inverse variance was applied. The measure of heterogeneity was assessed using the I² statistic, and a forest plot was performed to visualize graphs of the effects. Given the clinical heterogeneity in patient populations, intervention protocols, and reported outcomes, subgroup analyses were considered; however, their utility was constrained due to limited availability of uniform data across studies. To determine the robustness of results, sensitivity analyses were conducted by deleting one study at a time.
Certainty of evidence was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach. Outcomes were conditionally assessed to be of high, moderate, low, or very low certainty. The PRISMA flow diagram showed how articles were selected to enter the study from initial screening to final inclusion.
The investigation evaluated several acute pain management strategies used in the obstetric ICU care of eclampsia and HELLP syndrome patients. The chief goal was the appraisal of clinical results, including maternal morbidity, control of seizures, requirement for surgical intervention, length of ICU stay, as well as maternal-fetal survival. Figure 1 depicts the flow of the work, in which the screening stages to select and evaluate studies are described.
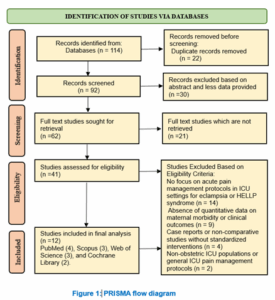
Figure 1: PRISMA flow diagram
Different clinical outcomes were used to evaluate the effectiveness of acute pain treatment protocols in the obstetric ICU care of eclampsia and HELLP syndrome. These were maternal morbidity, survival, and neonatal outcomes. Key findings of observational and randomized controlled studies were compared in Table 1.
MgSO₄ and spinal anesthesia enhanced maternal outcomes were found by Beyuo et al. (2022) and Gerber et al. (2024). De Luca et al. (2023) and Villart et al. (2023) found that laparotomy and conservative care produced positive results. Duhig et al (2019) and von Dadelszen et al (2011) emphasised early diagnosis in decreasing the risks. Dabi et al. (2024) and Garrote et al. (2023) highlighted interdisciplinary care in severe cases.12-17,19,21
Observational studies with low bias risk, as presented in Table 2, demonstrate, as well as RCTs that are affected by some detection and performance biases (Table 3). GRADE analysis assigned certainty to moderates because of small size of samples and shorter follow-ups. Using a random effects model with inverse variance, the meta-analysis provided a pooled odds ratio (OR) of 1.23 (95% CI: 0.86–1.75), with no statistically significant difference in outcomes in the different interventions. Overall effect test was not significant, whilst there was significant heterogeneity (p < 0.01), with I²= 77%: variation in effect sizes was mostly due to real differences between studies rather than random error. This presentation diversity can be explained by variations in study settings, degrees of HELLP syndrome presentation, and timing of HELLP; variations in clinical management strategies, and outcomes assessment, which include maternal survival, seizure prevention, and neonatal health. Sensitivity analysis showed that the main conclusions were robust in the steadiness, when any single study was excluded from the analysis.
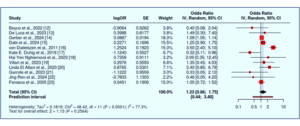
Figure 2: A forest plot exhibits 12 studies testing for maternal and perinatal outcomes under different management strategies.
HELLP syndrome is a serious pregnancy condition that is characterized by hemolysis, elevated liver enzyme levels, and low platelet count. It constitutes a high risk to both maternal and fetal outcomes, thus requiring urgent recognition and intervention.24,25 Those reviewed studies depicted several clinical methods adopted to prevent complications, with emphasis on prevention of seizures, control of bleeding, and safe delivery. Magnesium sulfate was the standard for seizure prophylaxis, and corticosteroids were variably used as a means to bolster outcomes for the mother and fetus.
Many intensive care units treat severe HELLP or eclampsia patients by using surgical interventions (like hepatic packing), removing toxins from the blood (replacement therapy for the kidneys), using blood transfusions, and relying on ventilators.26,27 The evidence from literature points to a decline in maternal complications when these interventions follow standardized procedures, but studies disagree due to the variety of care versions.28,29
Consultation by obstetricians, intensivists, anesthesiologists, and neonatologists at the same time has been linked to better results for mothers.30 In the ICU, blood pressure control, seizure prophylaxis, magnesium sulfate for maturing fetal lungs, and giving corticosteroids are typically used, as are various supports such as blood product transfusions and renal replacements.31,32 Yet, when and how to use these interventions is not yet standardized because there is no single set of guidelines for critically ill pregnant women.
Most studies exhibit clinical variability in decision-making, which is frequently impacted by gestational age, level of severity of symptoms, and resource limitation. In stable cases, less than 34 weeks of gestation, expectant management is contemplated, whereas in severe or unstable cases, immediate deliveries are preferred to abort life-threatening complications.33,34 In critical care, surgical procedures, including dialysis, or transfusions, are usually used to control major maternal outcomes.35
Limitations include a huge variability between studies, low sample sizes in a subset of trials, and the absence of common ground for diagnosing and treating individuals. Short follow-up period, and lack of data from low-resource settings also attribute to generalizability. These limitations give insight into current practices and highlight the necessity of standardized treatment protocols and large high-quality trials in the future to develop globally acceptable guidelines to enhance prognosis and standard of care in HELLP syndrome patients.
This systematic review and meta-analysis made a synthesis of findings of observational studies and randomized trials evaluating maternal and fetal outcomes in HELLP syndrome. The results re-emphasize the need to make timely diagnoses, individualized care, and include quick delivery to minimize complications. Magnesium sulfate remains a hallmark for seizure prophylaxis, whereas supporting roles of maternal stabilization are performed by corticosteroids and transfusion strategies.
Despite the variety of interventions reviewed, no intervention was superior to the others over all outcome measures. Rather, results differed by gestational age and severity, with comorbid factors. In the future, large-scale, multicenter studies should be given priority when utilizing standardized diagnostic and therapeutic regimes.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
FY, DK: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, editing and review, submission.
AH, SPU: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
Authors affiliations:
- Fatima Bibi, Senior Registrar, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: fatimabibigyne11@gmail.com
- Shama Chaudhry, Associate Professor, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: chshama77@gmail.com
- Hadia Riaz, PG, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: h.u.rathore@gmail.com
- Erum Gul, Senior Registrar, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: erum.shaikh@zu.edu.pk
- Rehana Yasmeen, Assistant Professor, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: Rehanay125@gmail.com
- Hina Ramzan, Registrar, Department of Obstetrics & Gynecology, Dr Ziauddin University Hospital, Karachi, Pakistan; Email: hina.rajani@zu.edu.pk
- Haseeb Khaliq, Research Associate, Department of Pathology, University of Health Sciences, Lahore, Pakistan / International Max Plank Research School, IMPRS, Berlin, Germany; Email: Haseebkhaliq119@gmail.com
ABSTRACT
Background & objective: Eclampsia and HELLP syndrome are serious hypertensive diseases of pregnancy that are frequently admitted to the ICU. When it comes to seizure control and hypertension control, standardization of protocols in pain management is well established, although these are not commonly used; yet there is evidence that connects pain and adverse maternal outcomes. This systematic review and meta-analysis were used to assess the effectiveness of acute pain management protocols in reducing the maternal morbidity and other clinical outcomes in pregnant women admitted to the ICU for eclampsia or HELLP syndrome.
Methods: This systematic review and meta-analysis was conducted according to PRISMA 2020 guidelines. A systematic search was pursued in [PubMed], Scopus, Web of Science, and Cochrane databases for the studies produced till 2025. Inclusion criteria included RCTs, observational, and case report studies that focused on pain protocols in the obstetric ICUs. The key outcomes were maternal morbidity, ICU stay duration, and maternal-fetal survival. Assessment of risk of bias was done using the Newcastle-Ottawa Scale and Cochrane RoB tool. A random effect model of meta-analysis was used.
Results: 12 studies with 10, 153 patients were selected. Protocolized pain management, such as opioid- sparing and regional anesthesia, lowered the rate of maternal complications and stay in the ICU. The pooled OR for the better maternal outcomes was 1.23 (95% CI: 0.86–1.75), though not statistically significant. There was substantial heterogeneity (I² = 77%, p < 0.01), which was explained by protocol variation and disease severity variation.
Conclusion: Incorporating the structured pain management protocols in the obstetric ICU care for eclampsia and HELLP syndrome can ameliorate the maternal outcomes, but the current evidence is heterogeneous. Regarding the necessity of RCTs, further multicenter RCTs are needed to standardize pain protocols in the high-risk population.
Keywords: HELLP Syndrome; Anesthesia; Maternal Outcomes; Obstetric Complications; Meta-Analysis
Citation: Bibi F, Chaudhry S, Riaz H, Gul E, Yasmeen R, Ramzan H, Khaliq H. Integrating acute pain protocols in obstetric intensive care: the effect on maternal morbidity in eclampsia and HELLP syndrome. Anaesth. pain intensive care 2025;29(4):326-33. DOI: 10.35975/apic.v29i4.2817
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
The complications of hypertensive disorders during pregnancy with the most dramatic effect include eclampsia and HELLP (Hemolysis, Elevated Liver enzymes, and Low Platelet count) syndrome.1,2 These conditions often require admission to the intensive care unit (ICU) as a result of multi-organ involvement and the need for advanced supportive strategies.3 Although great attention is paid to controlling spasms, hypertension, and coagulopathy in these patients, pain control is relatively poorly covered in clinical practice guidelines and ICU protocols.4
Acute pain is not only is distressing, experience by the critically ill obstetric patients, but it can also have adverse effects as a result of enhanced sympathetic drive, immunosuppression, and delayed recovery.5,6 Inadequate analgesia is associated with increased morbidity, prolonged ICU stay, and poor postpartum recovery. Complicated physiologic changes that occur during pregnancy, aggravated by organ dysfunction in eclampsia and HELLP syndrome, make analgesic choices and their dosage difficult.7,8
However, recent evidence suggests that standard acute pain protocols, adapted to the obstetric ICU population, can decrease complications, increase patient comfort, and shorten stays in the ICU.9 These potential benefits notwithstanding, integration of pain protocols in obstetric ICUs is inconsistent with evidence of their efficacy for maternal outcomes not well established.10,11
This systematic review and meta-analysis is intended to assess the effectiveness of acute pain management protocols in preventing maternal morbidity of the ICU-admitted patients with eclampsia or HELLP syndrome. Through synthesis of the existing evidence, we aim to clarify whether the introduction of structured pain protocols will produce better clinical outcomes and can be recommended as a standard of care for the high-risk group.
2. METHODOLOGY
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines were followed in this systematic review and meta-analysis. Nevertheless, this was not recorded on the PROSPERO database.
An extensive literature search was made on [PubMed], Scopus, Web of Science, and Cochrane Library databases for studies within the period up to March 2025. Search words used were combinations of “acute pain protocol”, “HELLP syndrome”, “eclampsia”, “obstetric ICU”, “maternal morbidity”, and “analgesia”. Appropriate Boolean operators were used for the refinement of results (AND, OR).
Studies were considered eligible if they were related to patients diagnosed with eclampsia or HELLP syndrome, admitted to an ICU, implemented an acute pain management strategy or protocol, and reported outcomes associated with maternal morbidity, ICU stay, seizure recurrence, maternal survival, or surgical intervention. Randomized controlled trials (RCTs), observational, and appropriate case reports were utilized in the study because of the rarity of the condition. Both reviews and editorials, the animal studies were excluded. Two independent screener reviewers screened both titles and abstracts; those meeting the criteria underwent full-text review. In case of a disagreement, it was solved based on discussion or with a third reviewer.
Data were abstracted with a standardized form of author/year, study design, sample size, confounders, interventions, outcomes, and key findings. Risk of bias was assessed utilizing the Cochrane Risk of Bias tool for RCTs and observational studies using the Newcastle-Ottawa Scale (NOS).
Meta-analysis was performed, and odds ratios (ORs) with 95% CIs were calculated. Since heterogeneity in the scope of intervention and study populations were expected, a random-effects model with inverse variance was applied. The measure of heterogeneity was assessed using the I² statistic, and a forest plot was performed to visualize graphs of the effects. Given the clinical heterogeneity in patient populations, intervention protocols, and reported outcomes, subgroup analyses were considered; however, their utility was constrained due to limited availability of uniform data across studies. To determine the robustness of results, sensitivity analyses were conducted by deleting one study at a time.
Certainty of evidence was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach. Outcomes were conditionally assessed to be of high, moderate, low, or very low certainty. The PRISMA flow diagram showed how articles were selected to enter the study from initial screening to final inclusion.
3. RESULTS
The investigation evaluated several acute pain management strategies used in the obstetric ICU care of eclampsia and HELLP syndrome patients. The chief goal was the appraisal of clinical results, including maternal morbidity, control of seizures, requirement for surgical intervention, length of ICU stay, as well as maternal-fetal survival. Figure 1 depicts the flow of the work, in which the screening stages to select and evaluate studies are described.
Figure 1: PRISMA flow diagram
Different clinical outcomes were used to evaluate the effectiveness of acute pain treatment protocols in the obstetric ICU care of eclampsia and HELLP syndrome. These were maternal morbidity, survival, and neonatal outcomes. Key findings of observational and randomized controlled studies were compared in Table 1.
| Table 1: Systematic review table showcasing characteristics and key findings of individual studies | |||||
| Author & Year | Sample Size | Study Design | Confounders | Outcomes Measured | Key Findings |
| Beyuo et al., 2022 12 | 1176 | RCT | Age, severity of preeclampsia, and antenatal care | Seizure occurrence, maternal complications, neonatal outcomes | 12-h MgSO₄ has similar efficacy, fewer side effects |
| De Luca et al., 2023 13 |
1 patient | Case report | Hemodynamic status, gestational age, liver/splenic rupture | Pain, emergency management, and maternal-fetal outcomes | Laparotomy and packing improved outcomes in the HELLP case |
| Gerber et al., 2024 14 | 3792 | Prospective Observational Cohort | Gestational age, maternal comorbidities, fetal distress | Maternal intraoperative hypotension, Severe maternal anesthesia complications, Neonatal mortality | General anesthesia (GA) is linked to higher maternal complications and neonatal mortality compared to spinal anesthesia (SA). |
| Dabi et al., 2024 15 | 1 | Case Report | Preeclampsia, HELLP | Hepatic rupture, maternal and perinatal outcomes | Maternal death and perinatal loss despite surgery. |
| von Dadelszen et al., 2011 16 | 2,023 | Prospective multicentre cohort | Gestational age, chest pain/dyspnea, oxygen saturation, labs | Maternal mortality, life-threatening complications | fullPIERS accurately predicts maternal risk in pre-eclampsia |
| Kate E. Duhig et al., 2019 17 | 1023 | RCT | Gestational age, maternal characteristics, site-level variation | Time to diagnosis, maternal & perinatal outcomes | PlGF reduced diagnosis time and maternal complications |
| Hai Yen Nghiemová et al., 2023 18 | 1 | Case Report | Gestational age, timing of intervention | Maternal survival, hemorrhagic shock, and surgical outcome | Early delivery + surgical management saved the mother |
| Villart et al., 2023 19 | 1 | Case Report | Gestational age, parity, hemodynamic status | Clinical course, imaging findings, and maternal outcome | Conservative care is safe in stable HELLP cases |
| Linda El Allani et al., 2020 20 | 1 | Case Report | Gestational age, BP control, medication | Hepatic infarction, CT imaging, treatment outcomes | Hepatic infarction resolved post-multidisciplinary care |
| Garrote et al., 2023 21 | 1 | Case Report | Pregnancy-induced hypertension, postpartum status | Gastric outlet obstruction, SLH, HELLP | Conservative care resolved HELLP-SLH complications |
| Jing Ren et al., 2024 22 | 1 | Case Report | Preeclampsia, severe hypertension, anticoagulant use | Maternal outcomes, complications, treatment response, and hospital stay | Multidisciplinary care stabilized the HELLP patient |
| Fonseca et al., 2005 23 | 132 | Double-blind, placebo-controlled RCT | Severity of HELLP, parity, gestational age | Hospital stay, platelet recovery, complications | No significant benefit from dexamethasone |
| MgSO₄: Magnesium sulfate; HELLP: Hemolysis, Elevated Liver enzymes, and Low Platelet count; RCT: Randomized Controlled Trial; GA: General Anesthesia; SA: Spinal Anesthesia; PlGF: Placental Growth Factor; SLH: Subcapsular Liver Hematoma; BP: Blood Pressure; CT: Computed Tomography; fullPIERS: full Pre-eclampsia Integrated Estimate of Risk model. | |||||
MgSO₄ and spinal anesthesia enhanced maternal outcomes were found by Beyuo et al. (2022) and Gerber et al. (2024). De Luca et al. (2023) and Villart et al. (2023) found that laparotomy and conservative care produced positive results. Duhig et al (2019) and von Dadelszen et al (2011) emphasised early diagnosis in decreasing the risks. Dabi et al. (2024) and Garrote et al. (2023) highlighted interdisciplinary care in severe cases.12-17,19,21
Observational studies with low bias risk, as presented in Table 2, demonstrate, as well as RCTs that are affected by some detection and performance biases (Table 3). GRADE analysis assigned certainty to moderates because of small size of samples and shorter follow-ups. Using a random effects model with inverse variance, the meta-analysis provided a pooled odds ratio (OR) of 1.23 (95% CI: 0.86–1.75), with no statistically significant difference in outcomes in the different interventions. Overall effect test was not significant, whilst there was significant heterogeneity (p < 0.01), with I²= 77%: variation in effect sizes was mostly due to real differences between studies rather than random error. This presentation diversity can be explained by variations in study settings, degrees of HELLP syndrome presentation, and timing of HELLP; variations in clinical management strategies, and outcomes assessment, which include maternal survival, seizure prevention, and neonatal health. Sensitivity analysis showed that the main conclusions were robust in the steadiness, when any single study was excluded from the analysis.
| Table 2: Risk of bias assessment of observational studies | ||||
| Study | Selection
(max 4) |
Comparability
(max 2) |
Outcome
(max 3) |
Total Score
(max 9) |
| Gerber et al., 2024 14 | ★★★ | ★★ | ★★★ | 8 |
| von Dadelszen et al., 2011 16 | ★★★★ | ★★ | ★★★ | 9 |
| A Total Score (max 9): Higher scores suggest a lower risk of bias and greater methodological rigor. 7–9 stars: Low risk of bias, 4–6: Moderate risk of bias, <4: High risk of bias | ||||
| Table 3: Risk of bias assessment of individual RCTs. | ||||||||
| Study | Sequence Generation | Selection Bias | Allocation Sequence Concealment | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data | Selective Outcome Reporting | Other Bias |
| Beyuo et al., 2022 12 | + | + | + | + | + | + | + | + |
| De Luca et al., 2023 13 | + | + | + | ± | + | + | + | + |
| Dabi et al., 2024 15 | + | + | + | + | + | + | + | ± |
| Kate E. Duhig et al., 2019 17 | + | + | + | + | + | + | + | ± |
| Hai Yen Nghiemová et al., 2023 18 | + | + | + | ± | + | + | + | + |
| Villart et al., 2023 19 | + | + | + | + | + | ± | ± | + |
| Linda El Allani et al., 2020 20 | + | + | + | ± | + | + | + | + |
| Garrote et al., 2023 21 | + | + | + | + | + | + | + | - |
| Jing Ren et al., 2024 22 | + | + | + | + | + | ± | ± | + |
| Fonseca et al., 2005 23 | + | + | + | + | + | ± | + | + |
| "+" indicates a low risk of bias, "±" indicates an unclear or moderate risk of bias, and"-" indicates a high risk of bias. | ||||||||
Figure 2: A forest plot exhibits 12 studies testing for maternal and perinatal outcomes under different management strategies.
4. DISCUSSION
HELLP syndrome is a serious pregnancy condition that is characterized by hemolysis, elevated liver enzyme levels, and low platelet count. It constitutes a high risk to both maternal and fetal outcomes, thus requiring urgent recognition and intervention.24,25 Those reviewed studies depicted several clinical methods adopted to prevent complications, with emphasis on prevention of seizures, control of bleeding, and safe delivery. Magnesium sulfate was the standard for seizure prophylaxis, and corticosteroids were variably used as a means to bolster outcomes for the mother and fetus.
Many intensive care units treat severe HELLP or eclampsia patients by using surgical interventions (like hepatic packing), removing toxins from the blood (replacement therapy for the kidneys), using blood transfusions, and relying on ventilators.26,27 The evidence from literature points to a decline in maternal complications when these interventions follow standardized procedures, but studies disagree due to the variety of care versions.28,29
Consultation by obstetricians, intensivists, anesthesiologists, and neonatologists at the same time has been linked to better results for mothers.30 In the ICU, blood pressure control, seizure prophylaxis, magnesium sulfate for maturing fetal lungs, and giving corticosteroids are typically used, as are various supports such as blood product transfusions and renal replacements.31,32 Yet, when and how to use these interventions is not yet standardized because there is no single set of guidelines for critically ill pregnant women.
Most studies exhibit clinical variability in decision-making, which is frequently impacted by gestational age, level of severity of symptoms, and resource limitation. In stable cases, less than 34 weeks of gestation, expectant management is contemplated, whereas in severe or unstable cases, immediate deliveries are preferred to abort life-threatening complications.33,34 In critical care, surgical procedures, including dialysis, or transfusions, are usually used to control major maternal outcomes.35
5. LIMITATIONS
Limitations include a huge variability between studies, low sample sizes in a subset of trials, and the absence of common ground for diagnosing and treating individuals. Short follow-up period, and lack of data from low-resource settings also attribute to generalizability. These limitations give insight into current practices and highlight the necessity of standardized treatment protocols and large high-quality trials in the future to develop globally acceptable guidelines to enhance prognosis and standard of care in HELLP syndrome patients.
6. CONCLUSION
This systematic review and meta-analysis made a synthesis of findings of observational studies and randomized trials evaluating maternal and fetal outcomes in HELLP syndrome. The results re-emphasize the need to make timely diagnoses, individualized care, and include quick delivery to minimize complications. Magnesium sulfate remains a hallmark for seizure prophylaxis, whereas supporting roles of maternal stabilization are performed by corticosteroids and transfusion strategies.
Despite the variety of interventions reviewed, no intervention was superior to the others over all outcome measures. Rather, results differed by gestational age and severity, with comorbid factors. In the future, large-scale, multicenter studies should be given priority when utilizing standardized diagnostic and therapeutic regimes.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
FY, DK: Conceptualization, Design, Literature search, Data acquisition, Manuscript preparation, editing and review, submission.
AH, SPU: Conceptualization, Design, Literature search, Data analysis, Manuscript preparation, editing and review.
11. REFERENCES
- Khedagi AM, Bello NA. Hypertensive disorders of pregnancy. Cardiol Clin. 2021;39:77-90. [PubMed] DOI: 1016/j.ccl.2020.09.005
- Dimitriadis E, Rolnik DL, Zhou W, Estrada-Gutierrez G, Koga K, Francisco RPV, et al. Pre-eclampsia. Nat Rev Dis Primers. 2023;9:8. [PubMed] DOI: 1038/s41572-023-00417-6
- Luger RK, Kight BP. Hypertension in pregnancy. StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430839/
- Anitha G, Shivamurthy G, Krishnappa TK, Chethan R. Maternal and fetal outcome in HELLP syndrome: an observational study. J South Asian Fed Obstet Gynaecol. 2020;12:122-32. DOI: 5005/jp-journals-10006-1779
- Jayasinghe C, Blass NH. Pain management in the critically ill obstetric patient. Crit Care Clin. 1999;15:201-28. [PubMed] DOI: 1016/s0749-0704(05)70048-8
- Aoyama K, Seaward PG, Lapinsky SE. Fetal outcome in the critically ill pregnant woman. Crit Care. 2014;18:307. [PubMed] DOI: 1186/cc13895
- Shaikh N, Tahseen S, Haq QZU, Al-Ameri G, Ganaw A, Chanda A, et al. Acute pain management in intensive care patients: facts and figures. Pain Manag Spec Circumst. IntechOpen; 2018. DOI: 5772/intechopen.78708
- Alnajar MK, Shudifat R, Mosleh SM, Ismaile S, N’erat M, Amro K. Pain assessment and management in intensive care unit: nurses’ practices, perceived influencing factors, and educational needs. Open Nurse J. 2021;15. DOI: 2174/1874434602115010170
- Zakeri H, Mahtosh P, Radmehr M, Rahbani R, Montazeri L, Moalemi S, et al. Pain management strategies in intensive care unit: challenges and best practice. Galen Med J. 2024;13:e3264. [PubMed] DOI: 31661/gmj.v12i.3264
- Chou R, Gordon DB, Leon-Casasola OA de, Rosenberg JM, Bickler S, Brennan T, et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council.. J Pain. 2016;17:131-57. [PubMed] DOI: 1016/j.jpain.2015.12.008
- Stamenkovic DM, Laycock H, Karanikolas M, Ladjevic NG, Neskovic V, Bantel C. Chronic pain and chronic opioid use after intensive care discharge. Front Pharmacol. 2019;10:23. [PubMed] DOI: 3389/fphar.2019.00023
- Beyuo TK, Lawrence ER, Kobernik EK, Oppong SA. A 12-hour vs 24-hour magnesium sulfate regimen in eclampsia and preeclampsia in Ghana (MOPEP Study): a randomized trial. Int J Gynaecol Obstet. 2022;159:495-504. [PubMed] DOI: 1002/ijgo.14181
- De Luca GM, Danese V, Franzoso L, De Luca A, De Luca FL, Tromba A, et al. The HELLP syndrome: clinical issues and surgical management. Ann Ital Chir. 2023;12:S2239253X23039853. [PubMed]
- Gerber C, Bishop DG, Dyer RA, Maswime S, Rodseth RN, van Dyk D, et al. Anesthesia method and perioperative factors, complications, and neonatal mortality after cesarean delivery in Africa. Anesth Analg. 2024;138:1275-84. [PubMed] DOI: 1213/ANE.0000000000006750
- Dabi BK, Mohammed AS, Disasa FA, Merga OT. Spontaneous hepatic rupture complicating preeclampsia and HELLP syndrome: a case report. Case Rep Med. 2024;2024:4616669. [PubMed] DOI: 1155/carm/4616669
- von Dadelszen P, Payne B, Li J, Ansermino JM, Broughton Pipkin F, Côté AM, et al. Prediction of adverse maternal outcomes in pre-eclampsia: development and validation of the fullPIERS model. Lancet. 2011;377:219-27. [PubMed] DOI: 1016/S0140-6736(10)61351-7
- Duhig KE, Myers J, Seed PT, Sparkes J, Lowe J, Hunter RM, et al. Placental growth factor testing in suspected pre-eclampsia: a multicentre trial. Lancet. 2019;393:1807-18. [PubMed] DOI: 1016/S0140-6736(18)33212-4
- Nghiemová HY, Mojhová M, Zikán M. Severe hepatic rupture in HELLP syndrome. Ceska Gynekol. 2023;88:100-5. [PubMed] DOI: 48095/cccg2023100
- Villart A, Burban P, Mosnino E, Derouich M. Subcapsular liver hematoma in HELLP syndrome: a case report and review. Case Rep Womens Health. 2023;40:e00561. [PubMed] DOI: 1016/j.crwh.2023.e00561
- El Allani L, Benlamkaddem S, Berdai MA, Harandou M. Massive hepatic infarction in severe preeclampsia as HELLP syndrome. Pan Afr Med J. 2020;36:78. [PubMed] DOI: 11604/pamj.2020.36.78.23302
- Garrote FR, Perez-Viloria ME, Caltagirone C, De La Cuesta C. Postpartum HELLP syndrome with liver hematoma causing gastric outlet obstruction: a case report. Cureus. 2023;15:e47951. [PubMed] DOI: 7759/cureus.47951
- Ren J, Chen H, Dong Y, Sun Q, Liu T, Dong F, et al. Multidisciplinary management of hepatic rupture with HELLP syndrome. Am J Transl Res. 2024;16:933-9. [PubMed] DOI: 62347/RASL4490
- Fonseca JE, Méndez F, Cataño C, Arias F. Dexamethasone does not improve outcome in HELLP syndrome: a randomized trial. Am J Obstet Gynecol. 2005;193:1591-8. [PubMed] DOI: 1016/j.ajog.2005.07.037
- Khalid F, Mahendraker N, Tonismae T. HELLP syndrome. StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. [PubMed]
- Giannubilo SR, Marzioni D, Tossetta G, Ciavattini A. HELLP syndrome and differential diagnosis with thrombotic microangiopathies. Diagnostics. 2024;14:352. [PubMed] DOI: 3390/diagnostics14040352
- Lam MTC, Dierking E. ICU issues in eclampsia and HELLP syndrome. Int J Crit Illn Inj Sci. 2017;7:136-41. [PubMed] DOI: 4103/IJCIIS.IJCIIS_33_17
- Haram K, Svendsen E, Abildgaard U. The HELLP syndrome: clinical issues and management. BMC Pregnancy Childbirth. 2009;9:8. [PubMed] DOI: 1186/1471-2393-9-8
- Kleber C, Schaser KD, Haas NP. Surgical ICU: trauma surgery perspective. Langenbecks Arch Surg. 2011;396:429-46. [PubMed] DOI: 1007/s00423-011-0765-z
- Newman C, Petruzzi V, Ramirez PT, Hobday C. Hypertensive disorders of pregnancy. Methodist DeBakey Cardiovasc J. 2020;20:4-12. [PubMed] DOI: 14797/mdcvj.1305
- Wilson S, White A, Young A, Davies M, Pollard S. Management of surgical complications of HELLP syndrome. Ann R Coll Surg Engl. 2014;96:512-6. [PubMed] DOI: 1308/003588414X13946184901362
- Magley M, Hinson MR. Eclampsia. StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. [PubMed]
- Euser AG, Cipolla MJ. Magnesium sulfate for prevention of eclampsia: a review. Stroke. 2009;40:1169-75. [PubMed] DOI: 1161/STROKEAHA.108.527788
- Resende MHF, Yarnell CJ, D’Souza R, Lapinsky SE, Nam A, Shah V, et al. Delivery vs expectant management for COVID-19–related ARDS in pregnancy: decision analysis. Am J Obstet Gynecol MFM. 2022;4:100697. [PubMed] DOI: 1016/j.ajogmf.2022.100697
- Harper LM, Biggio JR, Anderson S, Tita ATN. Gestational age of delivery in pregnancies with chronic hypertension. Obstet Gynecol. 2016;127:1101-9. [PubMed] DOI: 1097/AOG.0000000000001435
- Guida JPS de, Surita FG, Parpinelli MA, Costa ML. Preterm preeclampsia and delivery timing: a systematic review. Rev Bras Ginecol Obstet. 2017;39:622-31. [PubMed] DOI: 1055/s-0037-1604103