Muniba Jalil 1, Sadia Omer 2, Afshan Khanum 3, Muhammad Usman Ajmal 4, Sajid Ali 5
Author’s affiliations:
Background & objective: Early recognition of organ dysfunction and timely intervention are essential for improved patient outcomes. The Pediatric Sequential Organ Failure Assessment (pSOFA) score is designed to assess organ dysfunction in critically ill children. This study aims to evaluate the pSOFA score in predicting the mortality in critically ill oncology patients admitted to the Pediatric Intensive Care Unit (PICU).
Methodology: This was a retrospective review of all the pediatric oncology patients admitted to the PICU from March 2023 to September 2023. pSOFA score were calculated on day 1 and day 3 of PICU admission. Outcome measures like length of PICU stay and the mortality were calculated. The data was entered in SPSS 27.0. The qualitative data were compared with the outcome by using Fisher’s exact test, and the Mann-Whitney test was used for the quantitative variables.
Results: Fifty-four patients were recruited in the present study, of which 31 (57.4%) were male and 23 (42.6%) were female. Out of 54, the majority of the patients - 37 (68.5%) survived, while 17 (31.5%) died. The median age for the surviving patients and those who died was five months (P = 0.851). The median length of PICU stay was longer, 9 days for those who died compared to those who survived, 7 days (P = 0.808) The median pSOFA score on day 1 and day 3 was significantly higher for the deceased group compared to the group of survived children (P = 0.001).
Conclusion: The findings of our study highlight that a high pSOFA score is a reliable predictor of mortality in pediatric oncology septic patients and is significantly associated with higher mortality risk.
Keywords: pSOFA score; critical care; mortality; oncology; children; sepsis
Citation: Jalil M, Omer S, Khanum A, Ajmal MU, Ali H. Pediatric Sequential Organ Failure Assessment (pSOFA) scoring as a predictor of mortality in critically unwell oncology patients with sepsis: an experience from an ICU of a cancer center. Anaesth. pain intensive care 2025;29(3):377-383. DOI: 10.35975/apic.v29i3.2787
Received: December 30, 2024; Revised: March 16, 2025; Accepted: March 23, 2025
Sepsis represents a major cause of mortality particularly in immunocompromised oncological pediatric patients.1 The mortality rate associated with sepsis in children admitted to the pediatric intensive care unit (PICU) in developing countries has been registered to be more than 50%.2 Moreover, the outcomes of organ dysfunction and sepsis in pediatric oncological patients are greatly influenced by the primary disease, preadmission co-morbidities, infection site, organisms involved, and acute organ dysfunction, which require aggressive specific therapeutic approaches to improve the outcomes.2,3
Pediatric intensive care remains a challenging field, and it has made remarkable progress with recent advancements in equipment and therapies.4 However, early recognition of organ dysfunction and timely intervention are essential to improve patient outcomes and still remain a big challenge in the developing countries.
Several outcome prediction models are available for predicting the prognosis of pediatric patients admitted to the PICU.5 Importantly, the Sequential Organ Failure Assessment (SOFA) score was designed to assess organ dysfunction and help in prioritizing patient admission, directing appropriate treatment, and improving outcomes in critically ill patients and has been extensively used in the adults.6
El-Mashad et al. in his cohort study, compared whether the SOFA score can compete with the systemic inflammatory response syndrome (SIRS) in diagnosing sepsis, and reported that diagnosis of sepsis applying a SOFA cut-off of 3 points predicted mortality better than both the SIRS and the SOFA cut off of 2 points recommended by the Sepsis-3 consensus.7 In another cross-validation study, Bloch SH compared the Pediatric Sequential Organ Failure Assessment (pSOFA) with the Pediatric Risk of Mortality III (PRISM III) score for diagnostic accuracy and showed that the pSOFA score is a good predictor for mortality with better accuracy than the PRISM III-24 score in critically ill children.8
Besides economic burden, late presentation, immune suppression, treatment abandonment, and limited access to intensive care are the major challenges in developing countries.9 The data regarding the standard management and use of the scoring system in predicting mortality in oncological pediatric patients, especially from the developing world, is scarce. Therefore, this study aims to assess the utility and effectiveness of the pSOFA in critically ill pediatric oncological patients, emphasizing its role in the early detection of organ dysfunction, timely intervention, and its potential to improve clinical outcomes like mortality in patients admitted to the PICU.
This was a retrospective study done at the Pediatric Critical Care Unit (PICU) of Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore (Pakistan), from March 2023 to September 2023. The Institutional Review Board (IRB) approval was taken before collecting the data. Pediatric oncology patients from 1 year to 18 years of age, who presented with confirmed or suspected sepsis, neutropenic and non-neutropenic patients who presented with confirmed or suspected infection during the study period and pediatric oncology patients with septic shock were included in the study. Pediatric oncology patients whose parents did not give consent for inclusion in the study and pediatric oncology patients less than one year of age were excluded in this study. This data was collected from the hospital report system.
Suspected sepsis was defined according to the ‘Sepsis Six’ protocol of Surviving Sepsis Campaign, which is used in our hospital as pediatric sepsis pathway. Confirmed sepsis was diagnosed with positive blood stream infection. Furthermore, ‘Survival’ is defined as patients who were discharged alive from the PICU, and in-hospital death during the PICU stay was labelled as ‘mortality’. In our cohort ‘Organ Failure’ is defined using the pSOFA score, where higher scores, and ≥2 organ systems involvement indicate significant dysfunction. Individual organ failures were determined based on specific pSOFA component criteria, such as the need for vasopressors for cardiovascular failure or invasive ventilator support for respiratory failure.
The patients were admitted through emergency and from the pediatric inpatient department, and they were enrolled through universal sampling. The pSOFA score was calculated consistently across all patients at two time points, on day 1 of PICU admission (pSOFA 1) and on day 3 of PICU admission (pSOFA 2). The components of the score, including respiratory, cardiovascular, hepatic, renal, coagulation, and neurological dysfunction, were assessed using validated age-adjusted cut-offs, and each component scored from 0 to 4. High score or increasing score replicating severity of illness and worsening of organ dysfunction.10
The patients in our study required interventions based on their clinical condition and organ dysfunction. As the study included critically ill pediatric oncology patients admitted to the PICU, interventions such as mechanical ventilation, vasopressor support, renal replacement therapy, and antibiotic therapy were provided as per the standard sepsis and critical care management protocols. Nonetheless, we did not analyze the impact of specific interventions on outcomes. The primary outcome of the study was PICU mortality and the secondary outcome of the study was the length of PICU stay.
2.1. Statistical Analysis
The data was entered and analyzed in SPSS 27.0. Qualitative variables were presented in the form of frequency and percentages, and quantitative data was presented as median (IQR) since data was skewed. The normality of the data was checked using Kolmogorov’s Simonov test. The outcome was compared across different study variables. The qualitative data were compared with the outcome by using Fisher’s exact test, and the Mann-Whitney test was used for the quantitative variables. Unadjusted odds ratios, along with their respective 95% confidence intervals were calculated for the study variables. The binary logistic regression was used to calculate the adjusted odds ratio and 95% confidence interval for both the models.
Model 1 predictors; age, gender, and length of stay and SOFA 1,
Model 2 predictors; age, gender, and length of PICU stay and SOFA 2.
Receiver operating curve (ROC) analysis was conducted, and the Area Under the Curve (AUC) was computed with their respective 95% confidence interval limits. The significance of difference between the AUC-ROC was assessed by using Hanley and JA, McNeil BJ test. The estimated probabilities of mortality through both the binary logistic regression models were plotted against the SOFA score on day 1 and day 3 by the ROC curve. Bivariate correlations were also calculated. P ≤ 0.05 was considered significant.
In a total 54 patients were recruited in the present study, of which 37 (68.5%) survived. while 17 (31.5%) died. The median length of stay was 9 (20) days for those who died, compared to those who survived 7 (12) days. (P = 0.808) The median Sofa scores at day 1 and day 3 were significantly higher for the deceased group compared to the group of survived individuals. (P = 0.001) (Table 1).
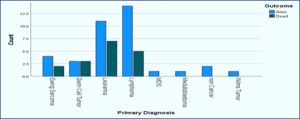
Figure1: Outcome with underlying disease of critically ill cancer patients
Regression analysis revealed that gender, age or length of stay has no strong association with the mortality; however, in both the models the pSOFA score at day 1 and at day 3 showed a significant association in predicting the mortality (Table 2).
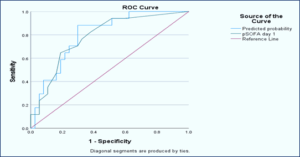
Figure 2: Receiver Operating Curve (ROC) for mortality prediction for SOFA score day 1
The area under the curve (AUC) revealed that the Sofa score on day 1 has good discriminatory power in predicting the mortality, with multivariate model slightly improving the prediction. (Unadjusted AUC: 0.783 (95% C.I: 0.655−0.911; P = 0.001); Adjusted AUC: 0.801 (95% C.I: 0.683−0.919; P = 0.0001)). Also, the sofa score on day 3 proved excellent discriminatory power in predicting the mortality, with the multivariate model slightly performing better (Unadjusted AUC: 0.915 (95% C.I: 0.840−0.990; P = 0.0001); 0.942 (95% C.I: 0.880−1.00; P = 0.0001) (Table 3).
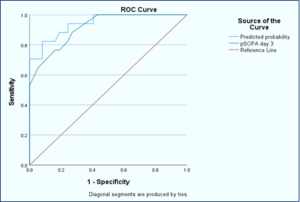
Figure 3: Receiver Operating Curve (ROC) for mortality prediction for SOFA score day 3
The ROC curve evaluates the performance of bivariate and multivariate models in predicting mortality using pSOFA score on day 1. It shows that both the models predicted well; however, the multivariate model performed slightly better, as it showed higher sensitivity and specificity compared to the bivariate model (Figure2).
The sensitivity and specificity of the multivariate model in predicting mortality by pSOFA score on day 3 were high as compared to the bivariate model (Figure3).
A strong positive and statistically significant correlation (r=0.329, P = 0.047; r=0.669, P = 0.001) was observed between SOFA score at day 1 and day3 with length of stay among the individuals who survived. This suggests that higher SOFA score is associated with the longer hospital stays, whereas lower sofa score can predict the shorter hospital stay (Table 4).
Sepsis is a predominant issue in intensive care units globally and is a significant cause of mortality, particularly in immunocompromised oncological pediatric patients.11 Early identification of patients at risk of deterioration through vigilant monitoring and inflammatory markers trends enables timely interventions, which can potentially improve outcomes.12 The sequential organ failure assessment (SOFA) score was developed to predict the morbidity and mortality of adult patients to facilitate treatment planning.10 However, limitations are there regarding its use in the pediatric population because it lacks age normalization, even though it has been validated as an independent risk predictor for adult mortality in cases of confirmed sepsis. Critically ill children often show noticeable changes in their body’s normal physiological balance. By understanding these changes, we can better gauge their severity and create a scoring system to support the care. Matics and Sanchez-Pinto introduced the pediatric version of the SOFA score (pSOFA), modifying the original SOFA score with age-adjusted thresholds for cardiovascular and renal systems and incorporating expanded respiratory criteria to include noninvasive markers of lung injury.13,14 Therefore, age-adjusted cut-offs for different body systems were incorporated into the original SOFA scores to create the pediatric SOFA (pSOFA) score.15
This study evaluated the pediatric Sequential Organ Failure Assessment (pSOFA) score for its ability to predict in-hospital mortality and PICU length of stay in children with sepsis who are critically unwell and admitted to PICU. The definitions of sepsis and septic shock are based on expert consensus as: ‘Life threatening organ dysfunction caused by a dysregulated host response to infection’.16 Studies showed that SOFA score was a better discriminant than the traditional SIRS and similarly effective to the more complex Logistic Organ Dysfunction System (LODS).17 Organ dysfunction was therefore characterized by a change in SOFA score of two or more points as a consequence of infection, which conferred an associated mortality of approximately 10%.18
Our observed mortality rate of 31.5% was lower than the rates reported in studies from other developing countries, which are more than 50%.2 5 6 The mortality prediction scores showed significantly higher values among dead patients, and pSOFA scores on Days 1 and 3 demonstrated robust predictive capability for in-hospital mortality. Moreover, mortality rates increased proportionally with rising pSOFA scores from Day 1 to Day 3 in this cohort. These findings align with previous studies in critically ill adults, where similar trends were observed.7
In our study, the pSOFA score was identified as a reliable predictor of mortality. Similarly, another study evaluated the diagnostic accuracy of the pSOFA scores in predicting mortality among critically ill children. Their findings demonstrated that non-surviving children had significantly higher pSOFA scores compared to survivors, consistent with the trends observed in our study.8
The correlation between the SOFA score and the length of stay among deceased patients was weak and insignificant, suggesting that there was no meaningful association between these variables in this group. In contrast, a strong positive correlation was observed between the SOFA score and the length of PICU stay among individuals who survived. This indicates that higher pSOFA scores are associated with longer stays, whereas lower pSOFA scores may predict shorter hospital stays. A similar result was reported in a study, which also found no correlation between pSOFA and the length of stay in the hospital.19
Our study has several limitations that warrant consideration. As a retrospective observational study, we lacked sufficient data to calculate all scores daily for dynamic assessment of patient conditions. The relatively small sample size may have led to less precise estimates of the pSOFA score's accuracy. The study limitations also include its focus on septic patients, limiting generalizability to non-septic pediatric populations, and its single-center design, which underscores the need for multicenter trials. Future research with larger cohorts and serial variable measurements at regular intervals is necessary to validate the general applicability of pSOFA especially in oncology patients.
7. Data availability:
Data is available with the primary author and can be provided on request.
8. Funding:
This research did not receive grants from funding agencies or any other resource
9. Conflict of Interest:
The authors confirmed no conflict of interest concerning the research, authorship, and publication
10. Authors’ contribution:
MJ: Concept, Data collection, manuscript preparation
AK: Data analysis, manuscript editing
SO: SA, MUA: literature search, Conduct of the study, manuscript preparation, and editing
Author’s affiliations:
- Muniba Jalil, Fellow in Pediatric Intensive Care, Department of Pediatric Intensive Care, Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, Pakistan; Email: muniba@927@gmail.com
- Sadia Omer, Consultant, Department of Pediatric Intensive Care, Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, Pakistan; Email: sadiaomer@doctors.net.uk
- Afshan Khanum, Senior Biostatistician and Cancer Epidemiologist, Department of Cancer Registry and Clinical Data Management, Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, Pakistan; Email: afshankhanum@skm.org.pk
- Muhammad Usman Ajmal, Fellow Pediatric Intensive Care, Department of Pediatric Intensive Care, Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore Pakistan; Email: usmanajmal230@gmail.com
- Sajid Ali, Senior Instructor, Department of Surgical Oncology, Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore, Pakistan; Email: dr.sajidali@yahoo.com; ORICD ID: 0000-0002-1477-6876
ABSTRACT
Background & objective: Early recognition of organ dysfunction and timely intervention are essential for improved patient outcomes. The Pediatric Sequential Organ Failure Assessment (pSOFA) score is designed to assess organ dysfunction in critically ill children. This study aims to evaluate the pSOFA score in predicting the mortality in critically ill oncology patients admitted to the Pediatric Intensive Care Unit (PICU).
Methodology: This was a retrospective review of all the pediatric oncology patients admitted to the PICU from March 2023 to September 2023. pSOFA score were calculated on day 1 and day 3 of PICU admission. Outcome measures like length of PICU stay and the mortality were calculated. The data was entered in SPSS 27.0. The qualitative data were compared with the outcome by using Fisher’s exact test, and the Mann-Whitney test was used for the quantitative variables.
Results: Fifty-four patients were recruited in the present study, of which 31 (57.4%) were male and 23 (42.6%) were female. Out of 54, the majority of the patients - 37 (68.5%) survived, while 17 (31.5%) died. The median age for the surviving patients and those who died was five months (P = 0.851). The median length of PICU stay was longer, 9 days for those who died compared to those who survived, 7 days (P = 0.808) The median pSOFA score on day 1 and day 3 was significantly higher for the deceased group compared to the group of survived children (P = 0.001).
Conclusion: The findings of our study highlight that a high pSOFA score is a reliable predictor of mortality in pediatric oncology septic patients and is significantly associated with higher mortality risk.
Keywords: pSOFA score; critical care; mortality; oncology; children; sepsis
Citation: Jalil M, Omer S, Khanum A, Ajmal MU, Ali H. Pediatric Sequential Organ Failure Assessment (pSOFA) scoring as a predictor of mortality in critically unwell oncology patients with sepsis: an experience from an ICU of a cancer center. Anaesth. pain intensive care 2025;29(3):377-383. DOI: 10.35975/apic.v29i3.2787
Received: December 30, 2024; Revised: March 16, 2025; Accepted: March 23, 2025
1. INTRODUCTION
Sepsis represents a major cause of mortality particularly in immunocompromised oncological pediatric patients.1 The mortality rate associated with sepsis in children admitted to the pediatric intensive care unit (PICU) in developing countries has been registered to be more than 50%.2 Moreover, the outcomes of organ dysfunction and sepsis in pediatric oncological patients are greatly influenced by the primary disease, preadmission co-morbidities, infection site, organisms involved, and acute organ dysfunction, which require aggressive specific therapeutic approaches to improve the outcomes.2,3
Pediatric intensive care remains a challenging field, and it has made remarkable progress with recent advancements in equipment and therapies.4 However, early recognition of organ dysfunction and timely intervention are essential to improve patient outcomes and still remain a big challenge in the developing countries.
Several outcome prediction models are available for predicting the prognosis of pediatric patients admitted to the PICU.5 Importantly, the Sequential Organ Failure Assessment (SOFA) score was designed to assess organ dysfunction and help in prioritizing patient admission, directing appropriate treatment, and improving outcomes in critically ill patients and has been extensively used in the adults.6
El-Mashad et al. in his cohort study, compared whether the SOFA score can compete with the systemic inflammatory response syndrome (SIRS) in diagnosing sepsis, and reported that diagnosis of sepsis applying a SOFA cut-off of 3 points predicted mortality better than both the SIRS and the SOFA cut off of 2 points recommended by the Sepsis-3 consensus.7 In another cross-validation study, Bloch SH compared the Pediatric Sequential Organ Failure Assessment (pSOFA) with the Pediatric Risk of Mortality III (PRISM III) score for diagnostic accuracy and showed that the pSOFA score is a good predictor for mortality with better accuracy than the PRISM III-24 score in critically ill children.8
Besides economic burden, late presentation, immune suppression, treatment abandonment, and limited access to intensive care are the major challenges in developing countries.9 The data regarding the standard management and use of the scoring system in predicting mortality in oncological pediatric patients, especially from the developing world, is scarce. Therefore, this study aims to assess the utility and effectiveness of the pSOFA in critically ill pediatric oncological patients, emphasizing its role in the early detection of organ dysfunction, timely intervention, and its potential to improve clinical outcomes like mortality in patients admitted to the PICU.
2. METHODOLOGY
This was a retrospective study done at the Pediatric Critical Care Unit (PICU) of Shaukat Khanum Memorial Cancer Hospital & Research Center, Lahore (Pakistan), from March 2023 to September 2023. The Institutional Review Board (IRB) approval was taken before collecting the data. Pediatric oncology patients from 1 year to 18 years of age, who presented with confirmed or suspected sepsis, neutropenic and non-neutropenic patients who presented with confirmed or suspected infection during the study period and pediatric oncology patients with septic shock were included in the study. Pediatric oncology patients whose parents did not give consent for inclusion in the study and pediatric oncology patients less than one year of age were excluded in this study. This data was collected from the hospital report system.
Suspected sepsis was defined according to the ‘Sepsis Six’ protocol of Surviving Sepsis Campaign, which is used in our hospital as pediatric sepsis pathway. Confirmed sepsis was diagnosed with positive blood stream infection. Furthermore, ‘Survival’ is defined as patients who were discharged alive from the PICU, and in-hospital death during the PICU stay was labelled as ‘mortality’. In our cohort ‘Organ Failure’ is defined using the pSOFA score, where higher scores, and ≥2 organ systems involvement indicate significant dysfunction. Individual organ failures were determined based on specific pSOFA component criteria, such as the need for vasopressors for cardiovascular failure or invasive ventilator support for respiratory failure.
The patients were admitted through emergency and from the pediatric inpatient department, and they were enrolled through universal sampling. The pSOFA score was calculated consistently across all patients at two time points, on day 1 of PICU admission (pSOFA 1) and on day 3 of PICU admission (pSOFA 2). The components of the score, including respiratory, cardiovascular, hepatic, renal, coagulation, and neurological dysfunction, were assessed using validated age-adjusted cut-offs, and each component scored from 0 to 4. High score or increasing score replicating severity of illness and worsening of organ dysfunction.10
The patients in our study required interventions based on their clinical condition and organ dysfunction. As the study included critically ill pediatric oncology patients admitted to the PICU, interventions such as mechanical ventilation, vasopressor support, renal replacement therapy, and antibiotic therapy were provided as per the standard sepsis and critical care management protocols. Nonetheless, we did not analyze the impact of specific interventions on outcomes. The primary outcome of the study was PICU mortality and the secondary outcome of the study was the length of PICU stay.
2.1. Statistical Analysis
The data was entered and analyzed in SPSS 27.0. Qualitative variables were presented in the form of frequency and percentages, and quantitative data was presented as median (IQR) since data was skewed. The normality of the data was checked using Kolmogorov’s Simonov test. The outcome was compared across different study variables. The qualitative data were compared with the outcome by using Fisher’s exact test, and the Mann-Whitney test was used for the quantitative variables. Unadjusted odds ratios, along with their respective 95% confidence intervals were calculated for the study variables. The binary logistic regression was used to calculate the adjusted odds ratio and 95% confidence interval for both the models.
Model 1 predictors; age, gender, and length of stay and SOFA 1,
Model 2 predictors; age, gender, and length of PICU stay and SOFA 2.
Receiver operating curve (ROC) analysis was conducted, and the Area Under the Curve (AUC) was computed with their respective 95% confidence interval limits. The significance of difference between the AUC-ROC was assessed by using Hanley and JA, McNeil BJ test. The estimated probabilities of mortality through both the binary logistic regression models were plotted against the SOFA score on day 1 and day 3 by the ROC curve. Bivariate correlations were also calculated. P ≤ 0.05 was considered significant.
3. RESULTS
In a total 54 patients were recruited in the present study, of which 37 (68.5%) survived. while 17 (31.5%) died. The median length of stay was 9 (20) days for those who died, compared to those who survived 7 (12) days. (P = 0.808) The median Sofa scores at day 1 and day 3 were significantly higher for the deceased group compared to the group of survived individuals. (P = 0.001) (Table 1).
| Table 1: Comparative analysis of outcome | |||||
| Variables | Outcome | Total | P-Value | ||
| Alive | Dead | ||||
| Gender* |
Male | 22 (52.95) | 9 (52.95) | 31 (57.4) | 0.769 |
| Female | 15 (40.5) | 8 (47.1) | 23 (46) | 0.769 | |
| Age** | 5 (9) | 5 (5) | 5 (7) | 0.851 | |
| Length of Stay** | 7 (12) | 9 (20) | 8 (13) | 0.808 | |
| pSOFA 1** | 2 (5) | 6 (6) | 3 (7) | 0.001*** | |
| pSOFA 2** | 2 (13) | 13 (9) | 4 (9) | 0.001*** | |
| * Fisher’s Exact test; **Mann Whitney Test, *** P-value = highly significant. Note: Gender data presented as n (%).and the remaining variables presented as median (IQR) | |||||
Figure1: Outcome with underlying disease of critically ill cancer patients
Regression analysis revealed that gender, age or length of stay has no strong association with the mortality; however, in both the models the pSOFA score at day 1 and at day 3 showed a significant association in predicting the mortality (Table 2).
| Table 2: Adjusted and unadjusted odds ratio comparison | |||
| Variables | Crude OR
(95% CI) |
Adjusted OR
(95% CI)# |
Adjusted OR
(95% CI)@ |
| Gender | 0.767 (0.241−2.43 | 0.898 (0.236−3.423) | 2.427 (0.306−19.2) |
| Age | 0.969 (0.86−1.10) | 0.881 (0.742−1.046) | 0.758 (0.551−1.042) |
| SOFA Day 1 | 1.259 (1.07−1.48) | 1.311 (1.098−1.565) | |
| SOFA Day 3 | 1.488 (1.21−1.83) | 1.76 (1.274−2.453) | |
| Length of Stay | 1.05 (0.97−1.07) | 1.004 (0.950−1.061) | 0.946 (0.869−1.030) |
| Model 1: predictors; age, gender and length of stay and SOFA day 1, @: Model 2: predictors; age, gender and length of stay and SOFA day 3; Data presented as odds ratio (95%CI) | |||
Figure 2: Receiver Operating Curve (ROC) for mortality prediction for SOFA score day 1
The area under the curve (AUC) revealed that the Sofa score on day 1 has good discriminatory power in predicting the mortality, with multivariate model slightly improving the prediction. (Unadjusted AUC: 0.783 (95% C.I: 0.655−0.911; P = 0.001); Adjusted AUC: 0.801 (95% C.I: 0.683−0.919; P = 0.0001)). Also, the sofa score on day 3 proved excellent discriminatory power in predicting the mortality, with the multivariate model slightly performing better (Unadjusted AUC: 0.915 (95% C.I: 0.840−0.990; P = 0.0001); 0.942 (95% C.I: 0.880−1.00; P = 0.0001) (Table 3).
| Table 3: ROC Analysis | ||||
| Score | Bivariate | Multivariate | ||
| AUC (95% CI) | P-value | AUC (95% CI) | P-value | |
| pSOFA 1 | 0.783 (0.655−0.911) | 0.001** | 0.801 (0.683−0.919) | 0.0001** |
| pSOFA 2 | 0.915 (0.840−0.990) | 0.0001** | 0.942 (0.880−1.000) | 0.0001** |
| P-value1 | 0.080 | 0.038* | ||
| 1: Hanley & McNeil test for goodness of fit test, * significant, ** highly significant | ||||
Figure 3: Receiver Operating Curve (ROC) for mortality prediction for SOFA score day 3
The ROC curve evaluates the performance of bivariate and multivariate models in predicting mortality using pSOFA score on day 1. It shows that both the models predicted well; however, the multivariate model performed slightly better, as it showed higher sensitivity and specificity compared to the bivariate model (Figure2).
The sensitivity and specificity of the multivariate model in predicting mortality by pSOFA score on day 3 were high as compared to the bivariate model (Figure3).
A strong positive and statistically significant correlation (r=0.329, P = 0.047; r=0.669, P = 0.001) was observed between SOFA score at day 1 and day3 with length of stay among the individuals who survived. This suggests that higher SOFA score is associated with the longer hospital stays, whereas lower sofa score can predict the shorter hospital stay (Table 4).
| Table 4: Association of SOFA score and length of stay | |||
| Outcome | SOFA | Correlation | P-value |
| Alive | Day 1 | 0.329 | 0.047* |
| Day 3 | 0.669 | <0.001** | |
| Dead | Day 1 | -0.301 | 0.241 |
| Day 3 | -0.230 | 0.374 | |
| * Significant, ** highly significant | |||
4. DISCUSSION
Sepsis is a predominant issue in intensive care units globally and is a significant cause of mortality, particularly in immunocompromised oncological pediatric patients.11 Early identification of patients at risk of deterioration through vigilant monitoring and inflammatory markers trends enables timely interventions, which can potentially improve outcomes.12 The sequential organ failure assessment (SOFA) score was developed to predict the morbidity and mortality of adult patients to facilitate treatment planning.10 However, limitations are there regarding its use in the pediatric population because it lacks age normalization, even though it has been validated as an independent risk predictor for adult mortality in cases of confirmed sepsis. Critically ill children often show noticeable changes in their body’s normal physiological balance. By understanding these changes, we can better gauge their severity and create a scoring system to support the care. Matics and Sanchez-Pinto introduced the pediatric version of the SOFA score (pSOFA), modifying the original SOFA score with age-adjusted thresholds for cardiovascular and renal systems and incorporating expanded respiratory criteria to include noninvasive markers of lung injury.13,14 Therefore, age-adjusted cut-offs for different body systems were incorporated into the original SOFA scores to create the pediatric SOFA (pSOFA) score.15
This study evaluated the pediatric Sequential Organ Failure Assessment (pSOFA) score for its ability to predict in-hospital mortality and PICU length of stay in children with sepsis who are critically unwell and admitted to PICU. The definitions of sepsis and septic shock are based on expert consensus as: ‘Life threatening organ dysfunction caused by a dysregulated host response to infection’.16 Studies showed that SOFA score was a better discriminant than the traditional SIRS and similarly effective to the more complex Logistic Organ Dysfunction System (LODS).17 Organ dysfunction was therefore characterized by a change in SOFA score of two or more points as a consequence of infection, which conferred an associated mortality of approximately 10%.18
Our observed mortality rate of 31.5% was lower than the rates reported in studies from other developing countries, which are more than 50%.2 5 6 The mortality prediction scores showed significantly higher values among dead patients, and pSOFA scores on Days 1 and 3 demonstrated robust predictive capability for in-hospital mortality. Moreover, mortality rates increased proportionally with rising pSOFA scores from Day 1 to Day 3 in this cohort. These findings align with previous studies in critically ill adults, where similar trends were observed.7
In our study, the pSOFA score was identified as a reliable predictor of mortality. Similarly, another study evaluated the diagnostic accuracy of the pSOFA scores in predicting mortality among critically ill children. Their findings demonstrated that non-surviving children had significantly higher pSOFA scores compared to survivors, consistent with the trends observed in our study.8
The correlation between the SOFA score and the length of stay among deceased patients was weak and insignificant, suggesting that there was no meaningful association between these variables in this group. In contrast, a strong positive correlation was observed between the SOFA score and the length of PICU stay among individuals who survived. This indicates that higher pSOFA scores are associated with longer stays, whereas lower pSOFA scores may predict shorter hospital stays. A similar result was reported in a study, which also found no correlation between pSOFA and the length of stay in the hospital.19
5. LIMITATIONS
Our study has several limitations that warrant consideration. As a retrospective observational study, we lacked sufficient data to calculate all scores daily for dynamic assessment of patient conditions. The relatively small sample size may have led to less precise estimates of the pSOFA score's accuracy. The study limitations also include its focus on septic patients, limiting generalizability to non-septic pediatric populations, and its single-center design, which underscores the need for multicenter trials. Future research with larger cohorts and serial variable measurements at regular intervals is necessary to validate the general applicability of pSOFA especially in oncology patients.
6. CONCLUSION
The pSOFA score is a reliable predictor of mortality in pediatric oncology patients who are unwell due to sepsis. Our findings highlight its strong prognostic performance, making it a valuable tool for clinical decision-making in pediatric sepsis management.7. Data availability:
Data is available with the primary author and can be provided on request.
8. Funding:
This research did not receive grants from funding agencies or any other resource
9. Conflict of Interest:
The authors confirmed no conflict of interest concerning the research, authorship, and publication
10. Authors’ contribution:
MJ: Concept, Data collection, manuscript preparation
AK: Data analysis, manuscript editing
SO: SA, MUA: literature search, Conduct of the study, manuscript preparation, and editing
11. REFERENCES
- Nates JL, Pène F, Darmon M, Mokart D, Castro P, David S, et al. Septic shock in the immunocompromised cancer patient: a narrative review. Crit Care. 2024;28(1):285. PubMed DOI: 1186/s13054-024-05073-0
- Lalitha AV, Satish JK, Reddy M, Ghosh S, George J, Pujari C. Sequential organ failure assessment score as a predictor of outcome in sepsis in the pediatric intensive care unit. J Pediatr Intensive Care. 2021;10(2):110–7. PubMed DOI: 1055/s-0040-1714705
- Patton MJ. Biomedical informatic analysis of critical care outcomes & chronic sequelae of SARS-CoV-2 infection [dissertation]. Univ Alabama at Birmingham; 2023.
- Maheshwari N, Agarwal N. The role of pediatric sequential organ failure assessment lactate score in predicting the clinical outcome of critically ill children: a single-center, prospective, observational study. J Pediatr Crit Care. 2023;10(5):193–8. DOI: 4103/jpcc.jpcc_17_23
- Aczon MD, Ledbetter DR, Laksana E, Ho LV, Wetzel RC. Continuous prediction of mortality in the PICU: a recurrent neural network model in a single-center dataset. Pediatr Crit Care Med. 2021;22(6):519–29. PubMed DOI: 1097/PCC.0000000000002682
- Jamnani AN, Baradari AG, Kargar-Soleimanabad S, Javaheri S. Predictive performance of SOFA and qSOFA for in-hospital mortality in ICU patients with COVID-19: a retrospective study. Ann Med Surg. 2023;85(11):5414–9. PubMed DOI: 1097/MS9.0000000000001304
- El-Mashad GM, El-Mekkawy MS, Zayan MH. Paediatric sequential organ failure assessment (pSOFA) score: a new mortality prediction score in the paediatric intensive care unit. An Pediatr (Engl Ed). 2020;92(5):277–85. PubMed DOI: 1016/j.anpedi.2019.05.018
- Baloch SH, Shaikh I, Gowa MA, Lohano PD, Ibrahim MN. Comparison of pediatric sequential organ failure assessment and pediatric risk of mortality III score as mortality prediction in pediatric intensive care unit. Cureus. 2022;14(1). PubMed DOI: 7759/cureus.21055
- Hordofa DF, Ahmed M, Birhanu Z, Weitzman S, Broas J, Shad A, et al. Childhood cancer presentation and initial outcomes in Ethiopia: findings from a recently opened pediatric oncology unit. PLoS Glob Public Health. 2024;4(7):e0003379. PubMed DOI: 1371/journal.pgph.0003379
- Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score—development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23:374. PubMed DOI: 1186/s13054-019-2663-7
- La Via L, Sangiorgio G, Stefani S, Marino A, Nunnari G, Cocuzza S, et al. The global burden of sepsis and septic shock. Epidemiologia. 2024;5(3):456–78. PubMed DOI: 3390/epidemiologia5030032
- Blythe R. Real-time clinical decision support systems for the prevention of deterioration in acute care [dissertation]. Queensland Univ Technol; 2024.
- Matics TJ, Sanchez-Pinto LN. Adaptation and validation of a pediatric sequential organ failure assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatr. 2017;171(10):e172352. PubMed DOI: 1001/jamapediatrics.2017.2352
- De Backer D, Dorman T. Surviving sepsis guidelines: a continuous move toward better care of patients with sepsis. JAMA. 2017;317(8):807–8. PubMed DOI: 1001/jama.2017.0059
- Malik A, Taksande A, Meshram R. Pediatric sequential organ assessment score: a comprehensive review of the prognostic marker in the pediatric intensive care unit. Cureus. 2024;16(5). PubMed DOI: 7759/cureus.60034
- Jacobi J. The pathophysiology of sepsis—2021 update: part 2, organ dysfunction and assessment. Am J Health Syst Pharm. 2022;79(6):424–36. PubMed DOI: 1093/ajhp/zxab393
- Hu T, Lv H, Jiang Y. The association between four scoring systems and 30-day mortality among intensive care patients with sepsis: a cohort study. Sci Rep. 2021;11(1):11214. PubMed DOI: 1038/s41598-021-90806-2
- McCarthy SL, Stewart L, Shaikh F, Murray CK, Tribble DR, Blyth DM. Prognostic value of sequential organ failure assessment (SOFA) score in critically-ill combat-injured patients. J Intensive Care Med. 2022;37(11):1426–34. PubMed DOI: 1177/08850666221078196
- Dewi R. Pediatric sequential organ failure assessment score: modified scoring system for sepsis in pediatrics patient. J In Med Allied Sci. 2020;70(2):176. Full Text