Yousef M. Alammari *
Author’s affiliation:
* Yousef M. Alammari, Department of Internal Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia; Email: Yalammari@gmail.com; Phone: 00966 50 046 7774
Background & objective: Non-inflammatory arthritis (NIA), a predominant musculoskeletal disorder, leading to significant chronic pain along with disability. Cupping therapy (CT), a traditional therapy, has achieved very significant interest in managing pain in different types of musculoskeletal ailments. However, its efficiency for NIA remains unclear. This meta-analysis study was aimed to comprehensively analyse the available evidences on the effectiveness of CT in the therapeutic management of NIA.
Methodology: A thorough systematic literature review was performed with the help of four electronic databases, PubMed, MEDLINE, Cochrane Central Register of Controlled Trials, and EMBASE, for available randomized controlled trials (RCTs), case-control, and cohort studies focusing on the application of CT for NIA. Cross-sectional studies, case reports, and review papers were not included. Research studies were evaluated for methodological quality and available data were extracted for relevant therapeutic outcomes, which included pain intensity, joint stiffness, functional limitations, along with quality of life. Data extracted included study features, participant demographics, intervention details, control group information, outcomes evaluated, and follow-up extent. A meta-analysis was conducted to synthesize the quantitative data.
Results: The search strategy identified a total of nine studies that specifically focused on CT for NIA. The meta-analysis conducted on subgroup analysis of Visual Analog Scale (VAS) scores between experimental and control groups revealed substantial heterogeneity due to the limited number of studies specifically targeting NIA, the results showed substantial heterogeneity (Tau2 = 40.07, Chi-square = 414.58, df = 3, p < 0.00001; I-square = 99%). Studies on other musculoskeletal conditions suggested potential benefits for pain management and function. Cupping therapy showed potential benefits across different indications such as chronic neck and shoulder pain, knee discomfort, low back pain, chronic non-specific neck pain, hyperalgesia, and muscle tension.
Conclusion: Cupping therapy shows promise as a potential pain management tool, but more research, particularly studies that employ strict inclusion criteria, utilize standardized cupping techniques and outcome measures, and target specific non-inflammatory arthritic conditions are needed to confirm its effectiveness for non-inflammatory arthritis. Future studies with standardized protocols and a focus on non-inflammatory arthritis populations will be crucial in determining its role with certainty.
Keywords: Cupping therapy; non-inflammatory arthritis; pain management; musculoskeletal disorders; meta-analysis
Citation: Alammari YM. Efficacy of cupping therapy in non-inflammatory arthritis: a meta-analysis. Anaesth. pain intensive care 2025;29(3):682-694. DOI: 10.35975/apic.v29i3.2775
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Non-inflammatory arthritis (NIA), encompassing conditions like osteoarthritis, is a leading cause of chronic musculoskeletal pain and disability globally. Characterized by progressive degeneration of articular cartilage, it leads to, joint stiffness, and functional limitations, significantly impacting patients' quality of life. Conventional management for NIA primarily focuses on pain control and symptom alleviation through pharmacological interventions and physical therapy. However, the quest for safe and effective complementary and alternative therapies (CAM) continues to grow.1
Previous research demonstrated the rising trends of hospital admissions due to different musculoskeletal conditions.2 Cupping therapy (CT), an ancient traditional medicine technique, has garnered increasing interest in recent years for its potential to manage various musculoskeletal (MSK) conditions. It involves the application of specialized cups on the skin, creating a localized negative pressure. The probable mechanisms behind the therapeutic action of CT are complex. It is supposed to arouse mechanoreceptors, leading to the release of endogenous opioids and further endorsing pain variation through the "descending inhibitory pain pathway".3 Moreover, cupping may augment microcirculation, progress in blood flow, and further ease the elimination of inflammatory mediators, potentially improving synovial inflammation and encouraging tissue healing.4
Research studies examining the effectiveness of CT for pain management in different musculoskeletal disorders, including chronic back pain have revealed promising outcomes. 5 Studies by Lauche et al. reported significant decreases in pain and better-quality mechanical thresholds in patients with chronic neck pain following CT as compared to control groups.6 Similarly, a study by Salemi et al. in 2021 found that dry CT significantly reduced pain and enhanced functional disability in group of patients with obstinate non-specific low back pain.7 Overall these research findings suggest that CT has potential as a complementary approach for the therapeutic management of pain and improving function in patients with musculoskeletal disorders.
Though research studies propose significant benefits for pain management in other conditions, the current evidence on the efficiency of CT precisely for NIA leftovers incomplete. Additional research is required to conclusively regulate its role in management of this ailment. The studies by Liu et al.8 and Ren9 discovered CT in combination with acupuncture, but for rheumatoid arthritis, which is an inflammatory type of arthritis. It's significant to differentiate between rheumatoid arthritis and NIA as they have diverse underlying causes and therapeutic approaches. Though, these research studies exploring combination therapies with CT for inflammatory arthritis do highlight an interesting area for further investigation. This might involve using CT together with other therapeutic modalities like physical therapy or medications to produce a more comprehensive treatment strategy. Additional research is needed to isolate the specific effects of CT in this framework. Furthermore, the optimal CT techniques, treatment protocols, and long-term safety profiles require further investigation. The present systematic review and meta-analysis aims to address this knowledge gap by comprehensively focussing on the available literature on the effectiveness of CT in the management of NIA. The present study will critically appraise randomized controlled trials (RCTs) and other relevant studies to assess the influence of CT on the therapeutic management of pain, stiffness, functional limitations, and overall improvement in quality of life in patients with NIA. By synthesizing the available evidences, this review will contribute valuable future insights into the potential role of CT as a complementary management approach for this prevalent and debilitating ailment.
We aimed to appraise the current body of literature from RCTs and other pertinent research studies on the efficacy of CT intended for NIA.
2.1. Search strategy
Four medical electronic databases; e.eg., MEDLINE, PubMed, Cochrane Library, and EMBASE, were thoroughly investigated to identify relevant research articles until December 2024. The search terms included a combination of keywords and Mesh terms for the following: "cupping therapy," “Hijama”, "non-inflammatory arthritis," “arthralgia”, “joints pain”. To capture all variations of keywords, Boolean operators (AND, OR) were used to syndicate search terms, and truncation was employed.
2.2. Study criteria
We included studies published in English; e.g., randomized controlled trials, case-control studies, and cohort studies related to adult participants diagnosed with NIA, and assessing the practice of CT as an intervention.
Studies not pertinent to CT or musculoskeletal pain, non-human studies and studies without full-text accessibility were excluded. Cross-sectional studies, case reports, and reviews were also not included. These study designs have limited ability to examine clinical outcomes across different time points.
The methodological excellence of each study was evaluated using suitable tools (e.g., Cochrane Risk of Bias tool for RCTs).
2.3. Study procedure
Two independent reviewers extracted data using a uniform data extraction form. Data mined included study features, participant demographics, intervention details, control group information, outcomes evaluated, and follow-up extent.
A narrative synthesis summarizing the findings of the comprised studies was executed. Besides, meta-analysis was performed to quantify the overall effect magnitude for quantitative data.
2.3.1. Risk of bias
The risk of bias for each involved study was measured using the ‘Cochrane Risk of Bias’ tool for RCTs or other appropriate tools for different study designs. Bias assessment included random sequence generation, blinding of participants and personnel, distribution concealment, blinding of outcome assessment, selective outcome reporting, incomplete outcome data, and other biases.
2.4. Data analysis
Statistical analysis was performed using ‘RevMan’ software. Subgroup analyses were measured based on study design, length of intervention, and type of musculoskeletal pain. Sensitivity analyses was conducted to assess the robustness of the findings. The significance level was assigned as P < 0.05.
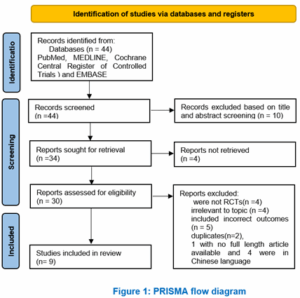
Out of 44 records identified from databases, 10 were excluded based on title and abstract screening. Reasons for exclusion included not being RCTs, case-control, or cohort study, irrelevant to topic, including incorrect outcomes, duplicates, not being full-length articles, and being in the Chinese language. The final review included 9 studies, and a summary of these studies was provided.
Table 1 summarizes findings from various studies on the effectiveness of CT for different conditions. It includes studies on knee osteoarthritis, chronic non-specific neck pain, low back pain, and other conditions. The studies yielded mixed findings regarding the effectiveness of CT. While some studies suggest potential benefits for pain management, improved function, and enhanced quality of life for patients with these conditions, substantial heterogeneity was observed across some studies. Reported heterogeneity highlights the need for further research with more standardized protocols to definitively determine the role of CT in managing these conditions. Some studies also compare CT to other interventions, such as acupuncture or physical therapy, indicating comparable or superior efficacy. Cupping therapy showed potential benefits across different indications such as chronic neck and shoulder pain, knee discomfort, low back pain, chronic non-specific neck pain, hyperalgesia, and muscle tension.
Table 2 summarizes various interventions used in studies related to CT and their outcomes. Each study presents different interventions, comparators, outcome measures, duration of intervention, primary outcomes, and secondary outcome measures include pain intensity, disability, quality of life, and physiological parameters like blood pressure and skin surface temperature. Duration of interventions varies from single sessions to multiple sessions over weeks. Primary outcomes focus on pain reduction and functional improvement, while secondary outcomes include medication usage, health-related quality of life, and adverse events.
Table 3 summarizes characteristics of participants and populations from various studies investigating the efficacy of CT for different conditions such as chronic neck and shoulder pain, knee osteoarthritis, nonspecific low back pain, and chronic non-specific neck pain. It includes details such as gender distribution, age range, sample size, intervention methods, and control arms for each study. Results suggest a variety of approaches to CT and control interventions across studies, reflecting the diversity in research methodologies and populations studied.
Figure 2 shows the meta-analysis conducted on subgroup analysis of Visual Analog Scale (VAS) scores between experimental and control groups revealed substantial heterogeneity (Tau2 = 40.07, Chi-square = 414.58, df = 3, p < 0.00001; I-square = 99%). Despite this high heterogeneity, the overall effect size was found to be 1.53, which was not statistically significant (p = 0.13).
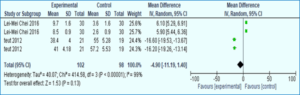
Figure 2: Meta-analyses plots (subgroup analysis of VAS score between the experimental and control groups)
Figure 3 shows the findings from a meta-analysis incorporating four included studies. In the funnel plot, two studies are positioned on the right side above 0.5 standard errors (SE) in the mean difference (MD), while two studies are situated on the left side near 1.5 SE in MD. Importantly, all four studies fall within the confines of the funnel plot, indicating no significant publication bias.
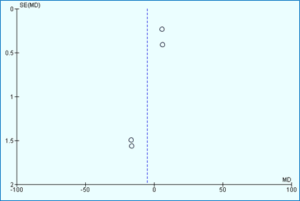
Figure 3: Funnel plot of included studies
Figure 4 presents a risk of bias assessment for all studies included in the analysis. Each study is evaluated based on various criteria to determine the likelihood of bias affecting its results. The criteria may include aspects such as randomization, blinding, completeness of outcome data, selective reporting, and other potential sources of bias. The results of the assessment are summarized in the table, providing an overview of the overall risk of bias across the included studies. This information helps to assess the quality and reliability of the evidence synthesized in the analysis. It considers factors such as selection bias, publication bias, and other potential biases that could influence the results.
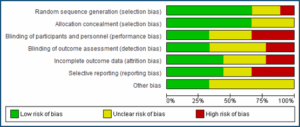
Figure 4: Risk of bias assessment of all included studies
Figure 5 provides a concise summary of included studies, offering an overview of their risk of bias. Each study's risk of bias is categorized and summarized, providing a clear indication of the overall quality and reliability of the included research. Additionally, the table may include a graphical representation, such as a graph, to visually depict the distribution of bias across the studies. This aids in quickly identifying any trends or patterns in bias among the included studies. table may include a graphical representation, such as a graph, to visually depict the distribution of bias across the studies. This aids in quickly identifying any trends or patterns in bias among the included studies.
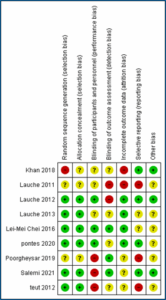
Figure 5: Summary of included studies showing risk of bias summary and graph.10–13
This systematic review and meta-analysis embarked on a comprehensive investigation into the effectiveness of CT for pain management in NIA. By meticulously analyzing studies encompassing knee osteoarthritis, chronic non-specific neck pain, and low back pain, the review aimed to shed light on the potential role of CT in this patient population.
The review's findings resonate with prior research, lending credence to the potential merits of CT for alleviating pain in osteoarthritis and chronic neck pain. Studies by Khan et al.,11 Poorgheysar et al.,12 Lauche et al.,6 and Teut et al.16 stand out in this regard. These studies consistently demonstrated significant reductions in pain intensity following CT interventions compared to control groups receiving sham cupping, (a simulated version of CT used as a control group in research studies) medication, or waitlist treatment (a control group where participants don't receive the intervention being investigated right away). This alignment with existing literature strengthens the argument for CT's potential as an analgesic intervention in NIA.
Furthermore, our review builds upon existing literature by providing a more comprehensive analysis of CT's effects. Whereas study by Wang et al.17 analyzing CT for knee osteoarthritis provided moderate-quality evidence for its pain-reducing effects. They concluded that CT improves physical function and lessens pain intensity in knees osteoarthritis patients is not well supported by the available data. Similarly, another review by Leem et al.18 on CT for chronic neck pain concluded that in terms of long-term neck discomfort intensity, cupping treatments were ineffective. Nonetheless, individuals with severe neck discomfort who had cupping treatments saw long-lasting improvements in their quality of life and physical function for up to two years. In contrast, the present meta-analysis sheds light on potential benefits across a wider range of non-inflammatory arthritic conditions. This broader perspective strengthens the case for CT's potential as a complementary or alternative pain management strategy for patients with NIA.
A randomized controlled trial by Islam et al. in 202119 investigated the efficacy of dry CT compared to soft and prolonged massage with chamomile oil in managing knee osteoarthritis. This study found statistically significant improvements in pain scores
(VAS) and all subscales of the Knee Osteoarthritis Outcome Score (KOOS) at 20 days compared to baseline in both treatment groups. Interestingly, no significant difference was observed between the cupping and massage groups, suggesting similar effectiveness for both interventions in managing knee osteoarthritis. These findings add to the growing body of evidence supporting the potential benefits of CT for pain management in NIA.
Another interesting RCT by Teut et al. in 2013,16 on pulsatile dry CT demonstrated significant improvements in pain and function compared to a control group with knee osteoarthritis. This study found that after four weeks, patients receiving CT had greater reductions in WOMAC scores and VAS pain scores compared to controls. These benefits persisted to a lesser extent at twelve weeks. These findings support the potential of CT for pain management in knee OA, although further research comparing cupping to other active treatment options is warranted.
Our review identified encouraging signs for CT's efficacy, it also revealed inconsistencies with some prior studies. The lack of statistical significance in the overall VAS score meta-analysis (p = 0.13) despite a moderate effect size (1.53) warrants further exploration. This discrepancy could be attributed to the heterogeneity observed in the included studies, as variations in cupping techniques, treatment duration, and outcome measures can influence results. However, it is important to acknowledge that our review employed stricter methodological criteria compared to some previous research. By focusing on studies with higher methodological quality, we aimed to provide a more robust assessment of CT's effectiveness. The inconsistencies identified highlight the need for future research with standardized protocols to definitively determine CT's role relative to other treatment options. This standardized approach will allow for more conclusive comparisons across studies and strengthen the overall body of evidence.
The limitations identified in our review and prior research pave the way for future studies to refine the understanding of CT for NIA. The significant heterogeneity observed underscores the need for standardized protocols encompassing clearly defined inclusion and exclusion criteria, specific cupping techniques, and consistent outcome measures. Additionally, blinding participants and therapists whenever feasible would further enhance the methodological rigor of future research endeavours.
The potential cost-effectiveness of CT compared to conventional treatments for NIA presents a compelling avenue for future research. Although CT is comparatively less costly than some medications or surgical options, the number of therapy sessions needed and the expertise of the practitioner can impact the overall financial burden.
Integrating patient standpoints and preferences into the argument of CT is correspondingly important. Understanding the aspects that impact patient choices to seek out CT, their previous experiences with the therapy, and their apparent benefits would enrich the understanding of this modality. Qualitative research exploring patient narratives and satisfaction with CT would counterpart the clinical data obtained through randomized controlled clinical trials. This combined approach would provide a more holistic approach and understanding of CT's role in pain management for patients with NIA.
The study by Abolahrari et al.20 compared CT with physical therapy, a well-established therapeutic option in the management of knee osteoarthritis. Their finding that physical therapy showed greater benefit is comprehensible. Another study by Khan et al. 11 implemented a different approach, comparing CT to acetaminophen, a well-known pain medication. Here, the finding of comparable efficiency proposes CT might be a potential alternative therapeutic option for pain management in some cases. These discrepancies emphasize the need for further research with standardized protocols to definitively regulate the role of CT relative to other treatment options for NIA. By establishing consistent approaches, future research can strive to minimize heterogeneity and generate more conclusive findings.
Here, we outline some specific areas that warrant further investigation: High-Quality of RCTs with Standardized Protocols: Well-designed randomized controlled clinical trials (RCTs) with standardized cupping techniques, treatment protocols, and validated outcome measures are vital. These research studies should specifically emphasis on NIA patient population, with clear inclusion and exclusion criteria to ensure a homogenous study group.
This investigation should compare the costs of CT with conventional therapeutic options, bearing in mind features like treatment regularity, potential medication cost savings, and overall impact on patient well-being Patient-Centered Consequences: Forthcoming research should fit in patient-centered outcome measures to imprisonment the holistic influence of CT on patients' lives. This may comprise measures of pain, function, stiffness, quality of sleep, and overall satisfaction with treatment. Understanding patient viewpoints will be vital for optimizing treatment tactics and further improving patient care.
Incorporation with other complementary and alternative therapies (CAM) Therapies: Exploring the safety and efficacy of integrating CT with other CAM for NIA is acceptable. Exploring possible synergistic effects of combined CAM approaches may offer a more comprehensive treatment strategies for managing this condition.
By addressing these future research themes, we can move advancing with a more all-inclusive understanding of CT's role in managing NIA. This will enhance healthcare professionals in taking informed treatment decisions and offer patients with a wide range of therapeutic options in the management of their condition and improving their overall quality of life scores.
Cupping therapy shows promising evidences as a potential pain management tool, but additional research is needed to support its efficiency in managing non-inflammatory arthritis cases. Future studies with standardized protocols and a focusing on non-inflammatory arthritis patients are needed to conclusively determine its potent therapeutic role. Overall, CT confirms its promising results as a potential complementary therapeutic option in the management of non-inflammatory arthritis cases.
8. Data availability
The numerical data generated during this research are available with the authors.
9. Conflict of interest
The author declares that there was no conflict of interests.
10. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
11. Authors’ contribution
Dr. Yousef M. Alammari is the sole researcher and the author of this paper.
Author’s affiliation:
* Yousef M. Alammari, Department of Internal Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia; Email: Yalammari@gmail.com; Phone: 00966 50 046 7774
ABSTRACT
Background & objective: Non-inflammatory arthritis (NIA), a predominant musculoskeletal disorder, leading to significant chronic pain along with disability. Cupping therapy (CT), a traditional therapy, has achieved very significant interest in managing pain in different types of musculoskeletal ailments. However, its efficiency for NIA remains unclear. This meta-analysis study was aimed to comprehensively analyse the available evidences on the effectiveness of CT in the therapeutic management of NIA.
Methodology: A thorough systematic literature review was performed with the help of four electronic databases, PubMed, MEDLINE, Cochrane Central Register of Controlled Trials, and EMBASE, for available randomized controlled trials (RCTs), case-control, and cohort studies focusing on the application of CT for NIA. Cross-sectional studies, case reports, and review papers were not included. Research studies were evaluated for methodological quality and available data were extracted for relevant therapeutic outcomes, which included pain intensity, joint stiffness, functional limitations, along with quality of life. Data extracted included study features, participant demographics, intervention details, control group information, outcomes evaluated, and follow-up extent. A meta-analysis was conducted to synthesize the quantitative data.
Results: The search strategy identified a total of nine studies that specifically focused on CT for NIA. The meta-analysis conducted on subgroup analysis of Visual Analog Scale (VAS) scores between experimental and control groups revealed substantial heterogeneity due to the limited number of studies specifically targeting NIA, the results showed substantial heterogeneity (Tau2 = 40.07, Chi-square = 414.58, df = 3, p < 0.00001; I-square = 99%). Studies on other musculoskeletal conditions suggested potential benefits for pain management and function. Cupping therapy showed potential benefits across different indications such as chronic neck and shoulder pain, knee discomfort, low back pain, chronic non-specific neck pain, hyperalgesia, and muscle tension.
Conclusion: Cupping therapy shows promise as a potential pain management tool, but more research, particularly studies that employ strict inclusion criteria, utilize standardized cupping techniques and outcome measures, and target specific non-inflammatory arthritic conditions are needed to confirm its effectiveness for non-inflammatory arthritis. Future studies with standardized protocols and a focus on non-inflammatory arthritis populations will be crucial in determining its role with certainty.
Keywords: Cupping therapy; non-inflammatory arthritis; pain management; musculoskeletal disorders; meta-analysis
Citation: Alammari YM. Efficacy of cupping therapy in non-inflammatory arthritis: a meta-analysis. Anaesth. pain intensive care 2025;29(3):682-694. DOI: 10.35975/apic.v29i3.2775
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Non-inflammatory arthritis (NIA), encompassing conditions like osteoarthritis, is a leading cause of chronic musculoskeletal pain and disability globally. Characterized by progressive degeneration of articular cartilage, it leads to, joint stiffness, and functional limitations, significantly impacting patients' quality of life. Conventional management for NIA primarily focuses on pain control and symptom alleviation through pharmacological interventions and physical therapy. However, the quest for safe and effective complementary and alternative therapies (CAM) continues to grow.1
Previous research demonstrated the rising trends of hospital admissions due to different musculoskeletal conditions.2 Cupping therapy (CT), an ancient traditional medicine technique, has garnered increasing interest in recent years for its potential to manage various musculoskeletal (MSK) conditions. It involves the application of specialized cups on the skin, creating a localized negative pressure. The probable mechanisms behind the therapeutic action of CT are complex. It is supposed to arouse mechanoreceptors, leading to the release of endogenous opioids and further endorsing pain variation through the "descending inhibitory pain pathway".3 Moreover, cupping may augment microcirculation, progress in blood flow, and further ease the elimination of inflammatory mediators, potentially improving synovial inflammation and encouraging tissue healing.4
Research studies examining the effectiveness of CT for pain management in different musculoskeletal disorders, including chronic back pain have revealed promising outcomes. 5 Studies by Lauche et al. reported significant decreases in pain and better-quality mechanical thresholds in patients with chronic neck pain following CT as compared to control groups.6 Similarly, a study by Salemi et al. in 2021 found that dry CT significantly reduced pain and enhanced functional disability in group of patients with obstinate non-specific low back pain.7 Overall these research findings suggest that CT has potential as a complementary approach for the therapeutic management of pain and improving function in patients with musculoskeletal disorders.
Though research studies propose significant benefits for pain management in other conditions, the current evidence on the efficiency of CT precisely for NIA leftovers incomplete. Additional research is required to conclusively regulate its role in management of this ailment. The studies by Liu et al.8 and Ren9 discovered CT in combination with acupuncture, but for rheumatoid arthritis, which is an inflammatory type of arthritis. It's significant to differentiate between rheumatoid arthritis and NIA as they have diverse underlying causes and therapeutic approaches. Though, these research studies exploring combination therapies with CT for inflammatory arthritis do highlight an interesting area for further investigation. This might involve using CT together with other therapeutic modalities like physical therapy or medications to produce a more comprehensive treatment strategy. Additional research is needed to isolate the specific effects of CT in this framework. Furthermore, the optimal CT techniques, treatment protocols, and long-term safety profiles require further investigation. The present systematic review and meta-analysis aims to address this knowledge gap by comprehensively focussing on the available literature on the effectiveness of CT in the management of NIA. The present study will critically appraise randomized controlled trials (RCTs) and other relevant studies to assess the influence of CT on the therapeutic management of pain, stiffness, functional limitations, and overall improvement in quality of life in patients with NIA. By synthesizing the available evidences, this review will contribute valuable future insights into the potential role of CT as a complementary management approach for this prevalent and debilitating ailment.
We aimed to appraise the current body of literature from RCTs and other pertinent research studies on the efficacy of CT intended for NIA.
2. METHODOLOGY
2.1. Search strategy
Four medical electronic databases; e.eg., MEDLINE, PubMed, Cochrane Library, and EMBASE, were thoroughly investigated to identify relevant research articles until December 2024. The search terms included a combination of keywords and Mesh terms for the following: "cupping therapy," “Hijama”, "non-inflammatory arthritis," “arthralgia”, “joints pain”. To capture all variations of keywords, Boolean operators (AND, OR) were used to syndicate search terms, and truncation was employed.
2.2. Study criteria
We included studies published in English; e.g., randomized controlled trials, case-control studies, and cohort studies related to adult participants diagnosed with NIA, and assessing the practice of CT as an intervention.
Studies not pertinent to CT or musculoskeletal pain, non-human studies and studies without full-text accessibility were excluded. Cross-sectional studies, case reports, and reviews were also not included. These study designs have limited ability to examine clinical outcomes across different time points.
The methodological excellence of each study was evaluated using suitable tools (e.g., Cochrane Risk of Bias tool for RCTs).
2.3. Study procedure
Two independent reviewers extracted data using a uniform data extraction form. Data mined included study features, participant demographics, intervention details, control group information, outcomes evaluated, and follow-up extent.
A narrative synthesis summarizing the findings of the comprised studies was executed. Besides, meta-analysis was performed to quantify the overall effect magnitude for quantitative data.
2.3.1. Risk of bias
The risk of bias for each involved study was measured using the ‘Cochrane Risk of Bias’ tool for RCTs or other appropriate tools for different study designs. Bias assessment included random sequence generation, blinding of participants and personnel, distribution concealment, blinding of outcome assessment, selective outcome reporting, incomplete outcome data, and other biases.
2.4. Data analysis
Statistical analysis was performed using ‘RevMan’ software. Subgroup analyses were measured based on study design, length of intervention, and type of musculoskeletal pain. Sensitivity analyses was conducted to assess the robustness of the findings. The significance level was assigned as P < 0.05.
Out of 44 records identified from databases, 10 were excluded based on title and abstract screening. Reasons for exclusion included not being RCTs, case-control, or cohort study, irrelevant to topic, including incorrect outcomes, duplicates, not being full-length articles, and being in the Chinese language. The final review included 9 studies, and a summary of these studies was provided.
3. RESULTS
Table 1 summarizes findings from various studies on the effectiveness of CT for different conditions. It includes studies on knee osteoarthritis, chronic non-specific neck pain, low back pain, and other conditions. The studies yielded mixed findings regarding the effectiveness of CT. While some studies suggest potential benefits for pain management, improved function, and enhanced quality of life for patients with these conditions, substantial heterogeneity was observed across some studies. Reported heterogeneity highlights the need for further research with more standardized protocols to definitively determine the role of CT in managing these conditions. Some studies also compare CT to other interventions, such as acupuncture or physical therapy, indicating comparable or superior efficacy. Cupping therapy showed potential benefits across different indications such as chronic neck and shoulder pain, knee discomfort, low back pain, chronic non-specific neck pain, hyperalgesia, and muscle tension.
| Table 1: Summary of study findings | |
| Authors | Description |
| Chi et al.10 | Cupping therapy increased skin surface temperature at the GB 21(gallbladder 21 acupuncture point) acupuncture points significantly compared to the control group and significantly reduced neck pain intensity severity scores. The study demonstrated that one treatment of CT increased skin surface temperature SST and reduced the subjective experience of chronic neck and shoulder pain intensity. |
| Khan et al. 11 | Cupping therapy showed significant and better results in managing knee osteoarthritis, with efficacy comparable to acetaminophen and can be recommended for other painful conditions. |
| Poorgheysar et al. 12 | In patients with knee osteoarthritis, CT is effective in reducing pain, rigidity, and disability. After the CT intervention, there was a substantial reduction in the intensity of the knee discomfort. The results of the study indicate that heated intermittent CT is likely to be a safe and effective treatment option for patients with knee osteoarthritis. |
| Salemi et al.7 | Cupping therapy resulted in a significant reduction in pain intensity and functional disability compared to the sham group, "sham group" refers to a control group where participants undergo a treatment that appears to be the same as the actual treatment being studied (in this case, CT), but it doesn't have the active components or effects of the real treatment. with effects lasting through the follow-up period. The therapy also showed a lower rate in physical and psychosocial factors for people with low back pain. |
| Lauche et al.13 | Patients who received a series of five dry cupping treatments had significantly less pain after the therapy compared to the control group. Pain diaries revealed a gradual decrease in neck pain in the treatment group, and significant differences in pain reported by the two groups after the fifth cupping session. In summary, the results indicated that a sequence of five dry cupping interventions was effective in alleviating chronic non-specific neck pain, as evidenced by improvements in both mechanical pain sensitivity and subjective measures. |
| Lauche et al.6 | In chronic non-specific neck pain, a single application of traditional cupping may be an effective treatment for enhancing hyperalgesia, quality of life, and pain. These findings necessitate additional research to verify them and to assess the efficacy of cupping in comparison to conventional therapies. |
| Lauche et al.14 | Progressive muscle relaxation is not substantially more effective than cupping massage in reducing chronic non-specific neck pain. However, it may be more effective in enhancing well-being and reducing pressure pain hypersensitivity. Cupping massage and progressive muscle relaxation are both readily accessible at home and can alleviate pain to a minimal degree that is clinically relevant. - According to popular belief, cupping massage primarily functions by alleviating agonizing muscle tension and enhancing local blood circulation. In order to verify these findings, additional investigations with larger populations and extended follow-up periods are required. |
| Pontes et al.15 | The primary results of the study are the description of a sham-controlled, randomized, and single-blind study that was conducted to assess the impact of dry cupping on the quality of life, function, and pain of women with knee osteoarthritis. Additionally, the study addressed concerns regarding participant blinding and the control of other therapeutic modalities. |
| Teut et al.16 | In comparison to no intervention, knee osteoarthritis symptoms were alleviated by dry cupping with a pulsatile cupping device. Most of the outcome measures showed statistically significant differences between osteoarthritis patients who received pulsatile dry cupping for 4 weeks and those who did not receive any intervention after 4 weeks. Pulsatile cupping may be a beneficial treatment in ambulatory health care services, in addition to other analgesic therapies. |
Table 2 summarizes various interventions used in studies related to CT and their outcomes. Each study presents different interventions, comparators, outcome measures, duration of intervention, primary outcomes, and secondary outcome measures include pain intensity, disability, quality of life, and physiological parameters like blood pressure and skin surface temperature. Duration of interventions varies from single sessions to multiple sessions over weeks. Primary outcomes focus on pain reduction and functional improvement, while secondary outcomes include medication usage, health-related quality of life, and adverse events.
| Table 2: Summary of interventions used and outcome measured in the included studies | |||||
| Authors | Intervention (comparator) | Outcome measured | Duration | Primary outcome | Secondary outcome |
| Chi et al.10 | Cupping therapy at SI 15, GB 21, and LI 15 acupuncture points using fire, with each cup placed for 10 min on each side of the body, totalling 20 min | Skin surface temperature (SST) at the SI 15, GB 21, and LI 15 acupuncture points; Blood pressure (BP); Pain intensity assessed using the visual analog scale (VAS) for neck pain intensity and shoulder pain intensity before and after specific movements | The duration of the intervention was 20 min per session, with a total of five sessions conducted over an unspecified period of time. | Changes in SST at specific acupuncture points (SI 15, GB 21, and LI 15). | Pain intensity using the VAS and BP. neck pain intensity (NPI) severity scores |
| Khan et al.11 | The intervention(s) that the study participants received was CT, which involved 11 sittings over the course of the study on specific anatomical sites for 15 min each time. | Relieving pain in knee osteoarthritis | 15 days | Evaluation of the effect of CT on knee osteoarthritis. |
Comparison of the therapeutic effectiveness of CT with acetaminophen 650 mg thrice a day orally. |
| Poorgheysar et al.12 | Medications related to osteoarthritis as prescribed before the study; CT involving the application of four cups around the knee in a vacuum position for 1-2 min, repeated four times. The treatment sessions are conducted every four days for sixteen days, with each session lasting 15-10 min. The therapy was conducted at the traditional medicine clinic of Gonabad University of Medical Sciences under the supervision of a traditional Iranian medicine practitioner. The procedure involved the use of an alcohol pad and a drop of chamomile oil to ignite the cups. The therapy was administered by a female researcher to female patients. | Pain intensity, stiffness, and disability | 16 days | Measures of pain intensity using the VAS and the evaluation of stiffness, pain intensity, and disability using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). | Demographic characteristics of the participants, the homogeneity of the CT and control groups, and the comparison of medication usage between the two groups. |
| Salemi et al.7 | The intervention consisted of CT with 17 reusable acrylic cups of medium diameter applied to specific acupuncture points related to low back pain and emotional aspects, for five 10-minute sessions, twice a week, with a total treatment time of 20 min per session. The cups were initially applied through two suctions by a hand pump generating a negative pressure of approximately 300 millibar. Coconut oil was applied before the session if signs of dehydration were identified. The specific acupuncture points included BL23, BL24, BL25, GV4, BL30, BL40, and BL58 for low back pain and HT3 and ST36 for emotional aspects. | VAS for pain intensity and Oswestry Disability Index (ODI) for functional disability | The duration of the intervention was 20 min per session, with a total of five sessions conducted over an unspecified period of time. | Pain Intensity: Measured using the VAS | Functional Disability: Assessed using the ODI questionnaire, Physical and Psychosocial Factors: Measured through the Start Back Screening Tool (SBST) questionnaire, Number of Days per Week of Pain: Recorded in a weekly pain diary, |
| Table 2: Summary of interventions used and outcome measured in the included studies (Contd) | |||||
| Lauche et al.6 | A series of 5 dry cupping treatments over a period of 2 weeks, with cups placed on afflicted areas for 10 to 20 min, repeated every 3 to 4 days | Pain at rest (PR) and maximal pain related to movement (PM) on a 100-mm VAS, NDI, Pressure-pain thresholds (PPT) at pain-related and control areas | The duration of the cupping intervention in this study is 2 weeks, with treatments occurring every 3 to 4 days. | Self-reported pain measures, including PR and PM on a 100-mm VAS, as well as pain diary (PD) data on a 0-10 numeric rating scale (NRS). | Neck Disability Index and quality of life (SF-36). Mechanical-detection thresholds (MDT), vibration-detection thresholds (VDT), and PPT at pain-related and control areas Specific subscales of the SF-36, including bodily pain and vitality |
| Lauche et al.13 | The intervention for the treatment group was a single cupping treatment involving disinfection of the skin, superficial incisions, use of double-walled glass cups, and removal of the cups after 10 to 15 min. | Pain at rest, pain related to movement, quality of life, and pressure pain thresholds at pain areas | Not mentioned | Chronic nonspecific neck pain (CNP), specifically focusing on PR, PM, and the impact on the quality of life, as measured by the SF-36 questionnaire. | MDT, VDT, and PPT measured before and three days after a single cupping treatment. Additionally, the study explores the impact of CT on NDI and patients' self-reported pain and medication diary (PaDi, MeDi) throughout the study. |
| Lauche et al.14 | The study participants received self-directed cupping massage and progressive muscle relaxation interventions. The cupping massage intervention involved attending a one-hour practical workshop, with two treatment sessions per week of 10-15 min' duration each. The progressive muscle relaxation intervention included attending a one-hour session led by a psychologist, practicing a shortened version of the PMR technique, and practicing relaxation at home twice a week for 20 min a session. | Current neck pain intensity measured on a 100 mm VAS after 12 weeks | The duration of the intervention in the study was 12 weeks, with participants undertaking the assigned treatment twice weekly for the entire duration. | Current neck pain intensity after 12 weeks, assessed using a 0–100 mm VAS. | Motion-induced discomfort. Pain perception that is emotional. Disabilities that are functional.Psychological distress. Well-being. Health-related quality of life. Pressure pain thresholds. Events that are detrimental. |
| Pontes et al.15 | Dry CT with acrylic cups around the knee, lasting 15 min, two times a week over six consecutive weeks, for a total of 12 sessions. | Pain intensity (Numerical Pain Rating Scale) (NPRS) | The duration of the intervention is 6 weeks, with sessions occurring two times a week for a total of 12 sessions, and each session lasting 15 min. | Pain intensity, measured using the Numerical Pain Rating Scale. | The Western Ontario and McMaster Universities Osteoarthritis Index was used to evaluate the health status of the knee. The functional capacity was assessed using the 8-step stair climb test, the 40-meter fast-paced walk test, and the 30-second chair stand test. Quality of life, measured using the Short-Form 36 questionnaire.Global perceived effect. |
| 1. Table 2: Summary of interventions used and outcome measured in the included studies (Contd) | |||||
| Teut et al. 16 | Pulsatile dry cupping is performed using a mechanical cupping device that applies flexible silicone cups to the knee joint and plastic glasses to the epidermis of the lower back region. Within a four-week period, the treatment involved eight sessions, each taken twice a week. The lower back area was cupped for 5 min with 2 cups on each side, and the entire afflicted knee was cupped for 10 min with a large, adaptable silicone cup (vacuum: 100-200 mbar, interval: 2 sec, pulse: 30-50%). | WOMAC score, pain intensity on VAS, Quality of Life (SF-36) | The duration of the intervention was 4 weeks. | Western Ontario and McMaster Universities Osteoarthritis score, | 2. Pain Intensity on a VAS: 3. Quality of Life (SF-36): 4. Paracetamol Consumption: the use of Paracetamol within the 4-week treatment period, serving as an additional measure of pain management. |
Table 3 summarizes characteristics of participants and populations from various studies investigating the efficacy of CT for different conditions such as chronic neck and shoulder pain, knee osteoarthritis, nonspecific low back pain, and chronic non-specific neck pain. It includes details such as gender distribution, age range, sample size, intervention methods, and control arms for each study. Results suggest a variety of approaches to CT and control interventions across studies, reflecting the diversity in research methodologies and populations studied.
| Table 3: Characteristics of participants and population of the included studies | ||||
| Authors | Characteristics of participants | Sample size (participants) | Intervention arm | Control arm |
| Chi et al.10 | Female: 91.7% Male: 8.3% Age range: 24-61 yr Work-related chronic neck and shoulder pain | Total: 62 | Cupping group that received CT at specific acupuncture points (SI 15, GB 21, and LI 15) using fire cupping for 10 min on each side of the body. | The control arm in this study involved participants receiving no intervention and resting for 20 min. |
| Khan et al.11 | Diagnosed cases of knee osteoarthritis aged between 30 and 60 yr old - Majority female participants - Majority of the participants in the age group of 50-60 yr old | Total: 47 | CT group. | The control arm in this study is the group that was given Acetaminophen 650 mg thrice a day orally with water. |
| Poorgheysar et al.12 | Patients with knee osteoarthritis aged between 40-60 yr, with a gender distribution of 58% female and 42% male. The study was conducted in Iran at the Gonabad Rheumatology Specialty Clinic. | Total: 36 CT group: 21 Control group: 15 | CT group | In this trial, the control arm consisted of patients who received solely medications prescribed by a rheumatologist and received no intervention. |
| Salemi et al.7 | The population characteristics include adults aged 18-59 yr with nonspecific low back pain, with the majority of participants being young females. | Total: 38 CT: 19 Sham:18 | CT group received five 10-minute sessions of CT targeting specific acupuncture points related to low back pain and emotional aspects. | Sham group |
| Table 3: Characteristics of participants and population of the included studies (Contd.) | ||||
| Lauche et al.6 | The population characteristics include patients with chronic non-specific neck pain, aged between 18 and 75 yr, with specific causes for neck pain excluded by an orthopaedist or a neurologist. Patients with certain medical conditions or recent invasive treatments were excluded from the study. | Total: 50 | Treatment group (TG) that received a series of 5 cupping treatments over a period of 2 weeks, performed by the study physician. | The control arm in this study is a waiting-list control group, which did not receive any treatment during the study period but was offered cupping treatment after completing their post-intervention assessment. |
| Lauche et al.13 | Female:66%, Male: 34%, Age range:18-75 Average age:56 Average duration of neck pain: 11 yr. Majority did not receive concurrent treatment before the study |
Total: 50 Treatment Group: 25 Waiting List Control Group: 25 | Group that received a single cupping treatment, referred to as the TG. The cupping procedure involved disinfecting the skin, making superficial incisions at the areas of pain, heating the air inside double-walled glass cups, placing the cups on the incisions to create a vacuum, leaving them in place for 10 to 15 min, removing the cups, disinfecting the skin, and applying a plaster. | Waiting list control group (WL), which consisted of 25 patients who did not receive any treatment during the study period. |
| Lauche et al.14 | Mean age: 54.1 yr - 73.8% female Patients with chronic non-specific neck pain, Age range: 18-75 |
Total: 61 Cupping massage: 30 Progressive muscle relaxation: 31 | Group of patients who received partner-delivered home-based cupping massage. | The control arm in this study is the group of patients who were assigned to the progressive muscle relaxation (PMR) intervention. |
| Pontes et al.15 | Women aged 50 to 75 yr diagnosed with knee osteoarthritis based on American College of Rheumatology clinical criteria, with a higher prevalence of knee osteoarthritis in women over the age of 50 yr. Recruitment of volunteers from a patient waiting list and through advertising on a local radio station. | Total: 62, Real: 31, Sham dry cupping: 31 |
Real dry cupping | The control arm in this study is the group receiving sham dry cupping. |
| Teut et al.16 | The investigation encompassed male and female patients aged 40 to 80 who were diagnosed with osteoarthritis of the knee in accordance with the ACR criteria (American College of Rheumatology). In the cupping group, the mean age of the patients was 68.1 ± 7.2, while in the control group, it was 69.3 ± 6.8. | Total: 40 Cupping group: 21 Control group: 19 |
In this trial, the intervention arm consists of a group of patients who underwent eight sessions of pulsatile dry cupping twice a week over a four-week period. The mechanical cupping device was used to apply flexible silicone cups to the knee joint and plastic glasses to the skin of the lower back region. | The control arm in this study refers to the group of patients who did not receive any cupping intervention during the 12-week study period. |
Figure 2 shows the meta-analysis conducted on subgroup analysis of Visual Analog Scale (VAS) scores between experimental and control groups revealed substantial heterogeneity (Tau2 = 40.07, Chi-square = 414.58, df = 3, p < 0.00001; I-square = 99%). Despite this high heterogeneity, the overall effect size was found to be 1.53, which was not statistically significant (p = 0.13).
Figure 2: Meta-analyses plots (subgroup analysis of VAS score between the experimental and control groups)
Figure 3 shows the findings from a meta-analysis incorporating four included studies. In the funnel plot, two studies are positioned on the right side above 0.5 standard errors (SE) in the mean difference (MD), while two studies are situated on the left side near 1.5 SE in MD. Importantly, all four studies fall within the confines of the funnel plot, indicating no significant publication bias.
Figure 3: Funnel plot of included studies
Figure 4 presents a risk of bias assessment for all studies included in the analysis. Each study is evaluated based on various criteria to determine the likelihood of bias affecting its results. The criteria may include aspects such as randomization, blinding, completeness of outcome data, selective reporting, and other potential sources of bias. The results of the assessment are summarized in the table, providing an overview of the overall risk of bias across the included studies. This information helps to assess the quality and reliability of the evidence synthesized in the analysis. It considers factors such as selection bias, publication bias, and other potential biases that could influence the results.
Figure 4: Risk of bias assessment of all included studies
Figure 5 provides a concise summary of included studies, offering an overview of their risk of bias. Each study's risk of bias is categorized and summarized, providing a clear indication of the overall quality and reliability of the included research. Additionally, the table may include a graphical representation, such as a graph, to visually depict the distribution of bias across the studies. This aids in quickly identifying any trends or patterns in bias among the included studies. table may include a graphical representation, such as a graph, to visually depict the distribution of bias across the studies. This aids in quickly identifying any trends or patterns in bias among the included studies.
Figure 5: Summary of included studies showing risk of bias summary and graph.10–13
4. DISCUSSION
This systematic review and meta-analysis embarked on a comprehensive investigation into the effectiveness of CT for pain management in NIA. By meticulously analyzing studies encompassing knee osteoarthritis, chronic non-specific neck pain, and low back pain, the review aimed to shed light on the potential role of CT in this patient population.
The review's findings resonate with prior research, lending credence to the potential merits of CT for alleviating pain in osteoarthritis and chronic neck pain. Studies by Khan et al.,11 Poorgheysar et al.,12 Lauche et al.,6 and Teut et al.16 stand out in this regard. These studies consistently demonstrated significant reductions in pain intensity following CT interventions compared to control groups receiving sham cupping, (a simulated version of CT used as a control group in research studies) medication, or waitlist treatment (a control group where participants don't receive the intervention being investigated right away). This alignment with existing literature strengthens the argument for CT's potential as an analgesic intervention in NIA.
Furthermore, our review builds upon existing literature by providing a more comprehensive analysis of CT's effects. Whereas study by Wang et al.17 analyzing CT for knee osteoarthritis provided moderate-quality evidence for its pain-reducing effects. They concluded that CT improves physical function and lessens pain intensity in knees osteoarthritis patients is not well supported by the available data. Similarly, another review by Leem et al.18 on CT for chronic neck pain concluded that in terms of long-term neck discomfort intensity, cupping treatments were ineffective. Nonetheless, individuals with severe neck discomfort who had cupping treatments saw long-lasting improvements in their quality of life and physical function for up to two years. In contrast, the present meta-analysis sheds light on potential benefits across a wider range of non-inflammatory arthritic conditions. This broader perspective strengthens the case for CT's potential as a complementary or alternative pain management strategy for patients with NIA.
A randomized controlled trial by Islam et al. in 202119 investigated the efficacy of dry CT compared to soft and prolonged massage with chamomile oil in managing knee osteoarthritis. This study found statistically significant improvements in pain scores
(VAS) and all subscales of the Knee Osteoarthritis Outcome Score (KOOS) at 20 days compared to baseline in both treatment groups. Interestingly, no significant difference was observed between the cupping and massage groups, suggesting similar effectiveness for both interventions in managing knee osteoarthritis. These findings add to the growing body of evidence supporting the potential benefits of CT for pain management in NIA.
Another interesting RCT by Teut et al. in 2013,16 on pulsatile dry CT demonstrated significant improvements in pain and function compared to a control group with knee osteoarthritis. This study found that after four weeks, patients receiving CT had greater reductions in WOMAC scores and VAS pain scores compared to controls. These benefits persisted to a lesser extent at twelve weeks. These findings support the potential of CT for pain management in knee OA, although further research comparing cupping to other active treatment options is warranted.
Our review identified encouraging signs for CT's efficacy, it also revealed inconsistencies with some prior studies. The lack of statistical significance in the overall VAS score meta-analysis (p = 0.13) despite a moderate effect size (1.53) warrants further exploration. This discrepancy could be attributed to the heterogeneity observed in the included studies, as variations in cupping techniques, treatment duration, and outcome measures can influence results. However, it is important to acknowledge that our review employed stricter methodological criteria compared to some previous research. By focusing on studies with higher methodological quality, we aimed to provide a more robust assessment of CT's effectiveness. The inconsistencies identified highlight the need for future research with standardized protocols to definitively determine CT's role relative to other treatment options. This standardized approach will allow for more conclusive comparisons across studies and strengthen the overall body of evidence.
The limitations identified in our review and prior research pave the way for future studies to refine the understanding of CT for NIA. The significant heterogeneity observed underscores the need for standardized protocols encompassing clearly defined inclusion and exclusion criteria, specific cupping techniques, and consistent outcome measures. Additionally, blinding participants and therapists whenever feasible would further enhance the methodological rigor of future research endeavours.
The potential cost-effectiveness of CT compared to conventional treatments for NIA presents a compelling avenue for future research. Although CT is comparatively less costly than some medications or surgical options, the number of therapy sessions needed and the expertise of the practitioner can impact the overall financial burden.
Integrating patient standpoints and preferences into the argument of CT is correspondingly important. Understanding the aspects that impact patient choices to seek out CT, their previous experiences with the therapy, and their apparent benefits would enrich the understanding of this modality. Qualitative research exploring patient narratives and satisfaction with CT would counterpart the clinical data obtained through randomized controlled clinical trials. This combined approach would provide a more holistic approach and understanding of CT's role in pain management for patients with NIA.
The study by Abolahrari et al.20 compared CT with physical therapy, a well-established therapeutic option in the management of knee osteoarthritis. Their finding that physical therapy showed greater benefit is comprehensible. Another study by Khan et al. 11 implemented a different approach, comparing CT to acetaminophen, a well-known pain medication. Here, the finding of comparable efficiency proposes CT might be a potential alternative therapeutic option for pain management in some cases. These discrepancies emphasize the need for further research with standardized protocols to definitively regulate the role of CT relative to other treatment options for NIA. By establishing consistent approaches, future research can strive to minimize heterogeneity and generate more conclusive findings.
6. Future Research Directions:
Here, we outline some specific areas that warrant further investigation: High-Quality of RCTs with Standardized Protocols: Well-designed randomized controlled clinical trials (RCTs) with standardized cupping techniques, treatment protocols, and validated outcome measures are vital. These research studies should specifically emphasis on NIA patient population, with clear inclusion and exclusion criteria to ensure a homogenous study group.
This investigation should compare the costs of CT with conventional therapeutic options, bearing in mind features like treatment regularity, potential medication cost savings, and overall impact on patient well-being Patient-Centered Consequences: Forthcoming research should fit in patient-centered outcome measures to imprisonment the holistic influence of CT on patients' lives. This may comprise measures of pain, function, stiffness, quality of sleep, and overall satisfaction with treatment. Understanding patient viewpoints will be vital for optimizing treatment tactics and further improving patient care.
Incorporation with other complementary and alternative therapies (CAM) Therapies: Exploring the safety and efficacy of integrating CT with other CAM for NIA is acceptable. Exploring possible synergistic effects of combined CAM approaches may offer a more comprehensive treatment strategies for managing this condition.
By addressing these future research themes, we can move advancing with a more all-inclusive understanding of CT's role in managing NIA. This will enhance healthcare professionals in taking informed treatment decisions and offer patients with a wide range of therapeutic options in the management of their condition and improving their overall quality of life scores.
7. CONCLUSION
Cupping therapy shows promising evidences as a potential pain management tool, but additional research is needed to support its efficiency in managing non-inflammatory arthritis cases. Future studies with standardized protocols and a focusing on non-inflammatory arthritis patients are needed to conclusively determine its potent therapeutic role. Overall, CT confirms its promising results as a potential complementary therapeutic option in the management of non-inflammatory arthritis cases.
8. Data availability
The numerical data generated during this research are available with the authors.
9. Conflict of interest
The author declares that there was no conflict of interests.
10. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
11. Authors’ contribution
Dr. Yousef M. Alammari is the sole researcher and the author of this paper.
12. REFERENCES
- Coaccioli S, Sarzi-Puttini P, Zis P, Rinonapoli G, Varrassi G. Osteoarthritis: new insight on its pathophysiology. J Clin Med. 2022;11(20). PubMed DOI: 3390/jcm11206013
- Mustafa Ali S, Naser AY, Alghanemi AG, AbuAlhommos AK, Sabha M, Mustafa Ali MK, et al. Musculoskeletal system and connective tissue related hospital admission in England and Wales between 1999 and 2019: an ecologic study. Cureus. 2022;14(12):e32453. PubMed DOI: 7759/cureus.32453
- Lv Q, Wu F, Gan X, Yang X, Zhou L, Chen J, He Y, et al. The involvement of descending pain inhibitory system in electroacupuncture-induced analgesia. Front Integr Neurosci. 2019;13:38. PubMed DOI: 3389/fnint.2019.00038
- Al-Bedah AMN, Elsubai IS, Qureshi NA, Aboushanab TS, Ali GIM, El-Olemy AT, et al. The medical perspective of cupping therapy: effects and mechanisms of action. J Tradit Complement Med. 2019;9(2):90–7. PubMed DOI: 1016/j.jtcme.2018.03.003
- Moura CC, Chaves ÉCL, Cardoso A, Nogueira DA, Corrêa HP, Chianca TCM. Cupping therapy and chronic back pain: systematic review and meta-analysis. Rev Lat Am Enfermagem. 2018;26:e3094. PubMed DOI: 1590/1518-8345.2888.3094
- Lauche R, Cramer H, Hohmann C, Choi KE, Rampp T, Saha FJ, Musial F, et al. The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomised controlled pilot study. Evid Based Complement Alternat Med. 2012;2012:429718. PubMed DOI: 1155/2012/429718
- Salemi MM, Gomes VMDSA, Bezerra LMR, Melo TMS, Alencar GG, Montenegro IHPM, et al. Effect of dry cupping therapy on pain and functional disability in persistent non-specific low back pain: a randomized controlled clinical trial. J Acupunct Meridian Stud. 2021;14(6):219–30. PubMed DOI: 51507/j.jams.2021.14.6.219
- Liu YR, Qiao SQ. Acupuncture combined with vesiculating cupping for 110 patients with rheumatoid arthritis. World J Acupunct Moxibustion. 2015;25(4):38–42. DOI: 1016/S1003-5257(17)30079-X
- Sun ZR, Yue JH, Zhang QH. Electroacupuncture at Jing-jiaji points for neck pain caused by cervical spondylosis: a study protocol for a randomized controlled pilot trial. Trials. 2013;14:360. PubMed DOI: 1186/1745-6215-14-360
- Chi LM, Lin LM, Chen CL, Wang SF, Lai HL, Peng TC. The effectiveness of cupping therapy on relieving chronic neck and shoulder pain: a randomized controlled trial. Evid Based Complement Alternat Med. 2016;2016:7358918. PubMed DOI: 1155/2016/7358918
- Khan AA, Jahangir U, Urooj S. Management of knee osteoarthritis with cupping therapy. J Adv Pharm Technol Res. 2013;4(4):217–23. PubMed DOI: 4103/2231-4040.121417
- Poorgheysar A, Shareinia H, Hosein M, Nouroozi A. The effect of hot intermittent cupping on pain, stiffness and disability of patients with knee osteoarthritis. Tradit Med Res. 2019;4(1):25–32. DOI: 53388/TMR201915096
- Lauche R, Cramer H, Choi KE, Rampp T, Saha FJ, Dobos GJ, et al. The influence of a series of five dry cupping treatments on pain and mechanical thresholds in patients with chronic non-specific neck pain: a randomised controlled pilot study. BMC Complement Altern Med. 2011;11:63. PubMed DOI: 1186/1472-6882-11-63
- Lauche R, Materdey S, Cramer H, Haller H, Stange R, Dobos G, et al. Effectiveness of home-based cupping massage compared to progressive muscle relaxation in patients with chronic neck pain: a randomized controlled trial. PLoS One. 2013;8(6):e65378. PubMed DOI: 1371/journal.pone.0065378
- Pontes NS, Barbosa GM, Almeida Silva HJ, Scattone Silva R, Souza CG, Lins CAA, et al. Effects of dry cupping on pain, function and quality of life in women with knee osteoarthritis: a protocol for a sham-controlled randomised trial. BMJ Open. 2020;10(12):e039857. PubMed DOI: 1136/bmjopen-2020-039857
- Teut M, Kaiser S, Ortiz M, Roll S, Binting S, Willich SN, et al. Pulsatile dry cupping in patients with osteoarthritis of the knee: a randomized controlled exploratory trial. BMC Complement Altern Med. 2012;12:184. PubMed DOI: 10.1186/1472-6882-12-184
- Wang YL, An CM, Song S, Lei FL, Wang Y. Cupping therapy for knee osteoarthritis: a synthesis of evidence. Complement Med Res. 2018;25(4):249–55. PubMed DOI: 1159/000488707
- Leem J. Long-term effect of cupping for chronic neck pain. Integr Med Res. 2014;3(4):217–9. PubMed DOI: 1016/j.imr.2014.10.001
- Islam MU, Nayab M, Ansari AN. Effect of dry cupping versus soft and prolonged massage in the management of knee osteoarthritis: a randomized controlled clinical trial. J Complement Integr Med. 2021;18(4):797–804. PubMed DOI: 1515/jcim-2020-0350
- Abolahrari-Shirazi S, Ghaffari-Nejad F, Ahmadpour Z, Zare L, Emami F. Is cupping therapy in combination with routine physical therapy effective in the management of knee osteoarthritis? J Rehabil Sci Res. 2018;5(4):93–8. DOI: 30476/jrsr.2018.44678