Minatallah Ali Elshafie 1, Mohammed Abdelrahman Salem 2, Asmaa Morsy Ghoniem 3, Amal Ismail Abdelrahman 4
Author affiliation:
Background & objective: Transjugular intrahepatic portosystemic shunt (TIPS) is used to form a tract between the portal and the hepatic veins, with a metallic stent bridged through the hepatic parenchyma for patients who have chronic liver disease causing multisystem physiological disruption. The purpose of this study was to compare the quality of sedation in the radiology suit during TIPS procedure with propofol using target-controlled infusion (TCI) versus manual infusion.
Methodology: This prospective study enrolled 78 ASA II patients, scheduled for TIPS procedure, who were randomly allocated into two equal groups; TCI group to have sedation with propofol guided with TCI system, and MCI group (manual infusion group) received propofol manually. We aimed primarily to study the effectiveness of TCI in sedation for TIPS procedure regarding SedLine levels and sedation-related complications, while the secondary outcomes were to evaluate the amount of total propofol consumption, the recovery time, with recording the patient and interventional radiologist satisfaction.
Results: There were statistically highly significant higher SedLine readings in the MCI group at times of venography and balloon dilation compared to TCI group respectively (P < 0.001). The TCI group showed more stable hemodynamics when compared to MCI group. While there was highly significant lower result in the TCI than MCI group regarding propofol dose (589.6 ± 174.9 vs. 711.6 ± 53.3 mg) and Recovery time (12.9 ± 3.9 vs. 18.3 ± 4.5 min; P < 0.0010) respectively. Also, the TCI group showed more patient and radiologist satisfaction scores.
Conclusion: Target-controlled infusion achieved more effective sedation for transjugular intrahepatic portosystemic shunt procedure, with less propofol consumption, and less sedation related complications. Target-controlled infusion had better patient and interventional radiologist satisfaction when compared to manually controlled infusion.
Key words: Chronic Liver Disease; Propofol; Target Control Infusion; Transjugular Intrahepatic Portosystemic Shunt Procedure
Citation: Elshafie MA, Salem MA, Ghoniem AM, Abdelrahman AI. Target controlled vs. manually controlled infusion of propofol for sedation during transjugular intrahepatic portosystemic shunt procedure: a randomized controlled trial. Anaesth. pain intensive care 2025;29(3):403-410. DOI: 10.35975/apic.v29i3.2754
Received: January 04, 2025; Revised: March 14, 2025; Accepted: March 29, 2025
Transjugular Intrahepatic Portosystemic Shunt (TIPS) has been used in cirrhotic patients for the management of portal hypertension complications as varices and refractory ascites.1 TIPS has also been used as a potential treatment for Hepatopulmonary Syndrome (HPS).2 The procedure was first described by Josef Rösch and was first used in human patients by Colapinto from the University of Toronto, Canada in 1982.3,4 TIPS is a synthetic stent inserted under radiological guidance within the liver tissue that helps to communicate the inflow of the portal vein with the outflow of the hepatic vein.5
Patients undergoing TIPS are medically complex as a result of the chronic liver disease that cause multisystem physiological disruption. They should receive multidisciplinary preoperative assessment and optimization before undergoing the procedure.6 Complexities of remote site should be considered, where the care administration is in an unfamiliar environment with considering staff and equipment availability. Sedation can be used to avoid the need for general anesthesia, using combinations of short acting sedative agents. The choice of drugs demand consideration of the physiological and pharmacokinetic changes seen in chronic liver disease patients.7
Propofol can be suitable for TIPS anesthesia, due to its pharmacological properties such as rapid onset of action, rapid change of sedation level and early recovery due to its large volume of distribution and a high-clearance rate.8 Also, it has an excellent amnesic effect, and low incidence of nausea and vomiting.9 The aims of sedation are to ensure the safety and well-being of the patient, to minimize the discomfort by providing anxiolysis, amnesia, and analgesia; to ensure that there is behavior and movement control that will allow for the procedure to be completed safely; and to bring the patient safely to discharge.10 The infusion rate should be changed intermittently to maintain the desired level of sedation.11
Target-controlled infusion (TCI) is an intravenous administration system, and is a pharmacokinetic model with a computer-controlled device that allows intravenous anesthetic drugs to be administered to a calculated target plasma concentration, mathematically predicted by a delivery algorithm. It can be enhanced to reduce bias and increase precision by incorporating covariates like age, weight, and sex and utilizing a pharmacokinetic model generated from its own population.12
The TCI-system uses its pharmacokinetic model to calculate the initial loading dose and infusion rate required to reach the desired target concentration.13 The drug passes from the blood or plasma to the central nervous system (CNS), to the effect site, where it exerts its activity.14
The Marsh pharmacokinetic parameters,15 that are incorporated into the Diprifusor TCI system parameters have been proven to provide a stable blood-therapeutic agent concentration for propofol induction and maintenance of anesthesia in patients without organ dysfunction.16
TCI has ability to maintain more consistent plasma concentrations with fewer fluctuations, the smooth process of induction and easily adjustable depth of anesthesia as well as more predictable recovery time.17-20 The aid of SedLine monitoring of the hypnotic component of anesthesia could be beneficial to avoid inadequate lower doses, or excessive administration of anesthetics that may be associated with an increased risk of postoperative neurocognitive disorder.21
We aimed primarily to evaluate the effectiveness of TCI in sedation for TIPS procedure regarding SedLine levels and sedation-related complication, and secondarily to evaluate the recovery time, recovery profile, total propofol consumption, and the patient and interventional radiologist satisfaction levels.
Formal approval was obtained from the ethics and research committee of Faculty of Medicine, Menoufia University, Egypt 5/3/2023 ) and the Institutional Research Board, (IRB) of the National Liver Institute, Menoufia University, Egypt on 1 July 2023, with protocol number 00003413FWA0000227, and registered at the Cochrane South Africa Registry (PACTR202310626983365) on 19 October 2023.This prospective, randomized, controlled trial was conducted at the Interventional Radiology Department, National Liver Institute, Menoufia University, Egypt from 20 October 2023 to 28 July 2024.
2.1. Study Design
The study included 78 patients of both sexes, aged 18 to 60 years, with an ASA-PS II, candidates for TIPS intervention. Patients with uncontrolled cardiovascular, respiratory or renal dysfunction, patients allergic to any used anesthetic agent, morbidly obese with body mass index (BMI) ≥ 40 kg/m2), patients undergoing perioperative significant bleeding or hemodynamic instability (e.g., air embolism), and who refused to participate in the study, were excluded from the study.
Based on previous studies (Laso et al., 2016) who reported that recovery time was significantly shorter in TCI group than MIT group (TCI: 7.48 ± 3.1 vs. manual: 10.3 ± 4.9min) (P =.008), minimum sample size calculated was 34 patients in each group, to be increased to 38 patients in each group for 15% drop-out rate.
After written informed consent, patients were allocated into two equal groups using a random number generator in sealed envelopes technique. The study group experienced anesthesia through the target-controlled infusion pump (TCI group), and the control group was conducted manually by infusion pump (MCI group).
2.2. Anesthetic Management
On arrival to the radiology suite, standard monitors were attached to the patient, two 20-gauge intravenous cannulas were secured, and a nasal cannula with oxygen flowing at 3–5 L/min was applied to each patient. SedLine was applied after skin preparation and disinfection with alcohol and slight rubbing for anesthesia depth monitoring. The four electrodes of the Electrical Cardiometry (EC) were applied after skin sterilization by alcohol swab, (first: approximately 5 cm above left base of the neck; second, on the left base of the neck; third, on the lower left thorax at the level of xiphoid and the fourth on the lower left thorax approximately 5 cm below 3rd electrode at level of anterior axillary line), and the patient’s data was applied. Verification of the correct signal quality was accomplished by visualization of the ECG, the impedance waveform and its first derivative. The patient’s position was carefully checked so that intravenous lines were not occluded.
Anesthesia induction for patients in the TCI group was done by using TCI pump (Injectomat TIVA Agilia, Fresenius Kabi syringe pump). The initial target of plasma propofol concentration for each patient was set according to the age. It was 4 μg/mL in the patients aged over 50 years, and 5 μg/mL in ≤ 50 years using the Marsh pharmacokinetic model.6 Then the TCI extension line was connected to the patient and infusion started until SedLine target range (25-50) was reached, fentanyl (1-1.5 μg/kg) bolus was given. The induction was planned to be achieved over 10 min, but if any hemodynamic instability was recorded (hypotension, bradycardia or desaturation), induction time was increased to 15 min.
When SedLine reached the targeted values and the patient lost responsiveness, the TIPS procedure started. Local anesthetic drug (lidocaine hydrochloride 1%) was used for the port of entry of the needle in the right internal jugular in all patients. The TIPS procedure is not painful. The extent of procedural pain is limited to the puncture wound in the neck, puncture of the liver capsule and pain during dilation of the Wallstent device.
For maintenance of anesthesia, the target concentration was gradually increased by 0.5 μg/mL, when SedLine reading exceeded the target range to be more than 50, or when BP and HR increased by 20% above the baseline. On the other hand, the target plasma concentration was decreased by 0.5 μg/mL, when SedLine reading decreased below 25, or BP and HR decreased by 20% below the baseline, or SpO2 fell below 92%.
For the MCI group anesthesia was induced with propofol bolus (1 mg/kg) over 10 min, then 170 µg/ kg/min infusion for 10 min using BD Alaris™ CC Plus syringe pump , and then 130 µg/kg/min for another 10 min, while monitoring the SedLine readings to obtain the target range (25-50)..22 When the target level was reached, fentanyl 1-1.5 μg/kg was given and the TIPS procedure started.
Anesthesia was maintained by infusion of propofol 100 µg/kg/min, increasing the rate by 10 µg/kg/min, when SedLine reading exceeded the target range of 50, and also when BP and HR increased by 20% above the baseline. Propofol infusion rate was decreased by (10 µg/kg/min), when SedLine reading decreased below 25 or mean blood pressure and heart rate decreased by 20% below the patient baseline.
The fluid therapy was managed in all patients according to EC readings to keep corrected flow time (FTC) within normal range to maintain the patient on the euvolumic side throughout the procedure. Hypotension was managed by 5 mg of ephedrine intravenously and any other vasopressor doses was recorded if needed.
At the end of the procedure, in the TCI group the target plasma drug concentration was adjusted to be (0 μg/mL). While in the MCI group the propofol infusion was stopped. All patients were allowed to regain consciousness while they were monitored. When SedLine values were above 80, SpO2 above 95% and patients were hemodynamically stable, they were transferred to post-anesthesia care unite (PACU). They were monitored until their modified Aldrete scores were 9-10, then discharged to the ward.
2.3. Measured Data
Hemodynamic parameters (MBP and HR), cardiac output (CO), and SedLine score were measured at; base line (T1), after induction of anesthesia (T2), at time of puncture of liver capsule (T3), time of venography (T4), time of balloon dilatation (T5) and time from the discontinuation of propofol infusion until adequate response to verbal command (recovery time) (T6).
Total propofol consumption, recovery time, procedure time, patient satisfaction score and intervention radiologist satisfaction scores were recorded.
Complications related to the procedure (pneumothorax, arrhythmia and bleeding) and sedation related complications ((hypotension, bradycardia, and hypoxemia) were recorded within the first 24 hours.
2.4. Statistical analysis
Data were collected, tabulated and statistically analyzed using an IBM compatible personal computer with Statistical Package for the Social Sciences (SPSS) version 26. Descriptive statistics e.g. qualitative data were expressed as Number (N), percentage (%), while quantitative data were expressed as mean (x̅), standard deviation (SD) and range (minimum-maximum). Student’s t-test (t) is a test of significance used for comparison of quantitative variables between the two groups of normally distributed data. Repeated measures ANOVA test was used for comparison of quantitative variables between more than two consecutive measures in the same group of normally distributed data. Chi-square test (χ2) was used to study association between qualitative variables. Whenever any of the expected cells were less than five, Fisher’s Exact test was used. Significant test results were quoted as two-tailed probabilities. Significance of the obtained results was judged at the 5% level (P > 0.05).
A total of 78 patients were included in this study. They were divided into 2 groups: TCI group and MCI group; in TCI group one patient was excluded due to failed TIPS procedure, while, in the MCI group another patient was excluded due to conversion to general anesthesia after repeated oxygen desaturation. Finally, 76 patients were analyzed, and equally divided in both groups.
Age, sex, BMI and ASA scores were compared between TCI and MCI groups showing no significant difference between both groups (P > 0.05) as shown in Table 1.
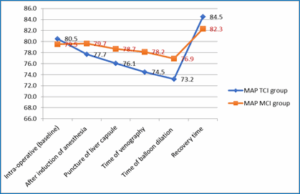
Figure 1: Comparative MAP measurements during TIPS procedure in the studied groups
There was a statistically significant difference between both groups regarding MAP during time of venography and time of balloon dilation while other measurements showed no significant differences
between both groups (Figure 1). Regarding HR there was no significant difference between TCI and MCI groups during different steps of TIPS procedure (Figure 2).
There was a highly significant difference between TCI and MCI groups regarding SedLine at time of venography (40.8 ± 6.3 vs. 46.3 ± 4.2) and the time of balloon dilation (39.5 ± 6.1 vs. 45.1 ± 3.4). Other SedLine comparisons showed no statistically significant differences (Figure 3).
There were no significant differences between TCI and MCI groups regarding recovery score and procedure time (P > 0.05) (Table 2). While there were highly significant differences between the groups regarding total propofol required and recovery time (P < 0.001).
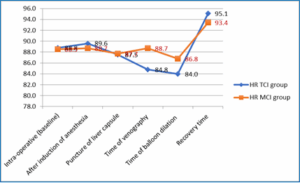
Figure 2: Comparative HR measurements during TIPS procedure in the studied groups
There was highly significant difference between both groups regarding patient satisfaction and radiologist satisfaction (P < 0.001) (Table 3). In patient satisfaction ‘completely comfortable’ category in TCI and MCI groups was 47% and 7.9% respectively, while in the ‘slight discomfort’ and ‘painful’ categories were (13.2% vs. 36%) and (0% vs. 15.8%) respectively. As shown in Table 4 there was no statistically significant difference between TCI and MCI groups regarding Procedure complications (P > 0.05). While there was significant difference between TCI and MCI groups regarding complications (P < 0.05).
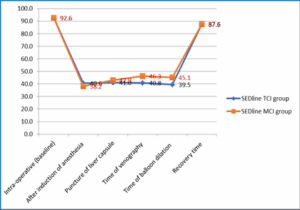
Figure 3: Comparative SEDline measurements during TIPS procedure in the studied groups
Anesthetic management for TIPS patients was a critical aspect of the procedural care, as the patient was medically complex with multisystem physiological disruption with the superadded complexities of remote site anesthesia. TCI systems have been recently established, allowing for easier adjustment of anesthesia depth while enhancing cardiovascular and respiratory stability. The aid of SedLine monitoring the hypnotic component to guide anesthetic management is crucial.
In the present study, we recorded intraoperative hemodynamic changes comparing the use of TCI pumps versus MCI. We found that employing the TCI system led to several significant advantages including more stable hemodynamic parameters during critical procedural stages, improved sedation
management, and faster post-procedural recovery time.
Earlier, Naser Yeganeh et al. studied the TCI with propofol
and remifentanil compared with MCI anesthesia in mastoidectomy surgeries.23 They concluded that TCI-based anesthesia achieved better hemodynamic stability through the stages, better recovery profile, decreased drug costs of anesthetics and more satisfaction of surgeons about surgical field condition, as compared to the MCI. Also, Wang et al. compared the sedation quality and safety of TCI and MCI of propofol during colonoscopy procedures. Their results showed that the TCI group demonstrated more stable hemodynamic status, with higher lowest MAP and lower highest MAP compared to the MCI group. Furthermore, patients in the TCI group experienced earlier recovery.24
In our study, we assessed the consumed propofol dose and recovery time between the TCI and manual groups, and found that there were highly significant less total propofol consumption in the TCI group and consequently shorter recovery times when compared to the manual group. Triem JG et al. compared optimated-target-controlled-infusion (OTCI) and manually-controlled infusion (MCI) technique in nasal sinus surgery. They found propofol consumption was similar within the first 60 min for both groups; thereafter, significantly less propofol usage in the OTCI group than the MCI group.25
Sahu et al. compared manual infusion versus TCI of propofol in total intravenous anesthesia (TIVA) during endoscopic retrograde cholangio-pancreatography (ERCP) procedures. Their results showed that the TCI group had significantly shorter recovery times compared to the TIVA group.26
On the other hand, Hsieh M-L et al. studied a comparison of the TCI and the MCI of propofol anesthesia during electroconvulsive therapy (ECT) found that the TCI group used higher doses of propofol, and longer procedural and recovery time.27 Such potential inferiority in efficacy in the TCI group might be explained by short procedure time and higher doses of propofol used for induction and so longer recovery time.
In terms of SedLine measurements, our study revealed significant differences between both of the groups with higher readings in the MCI group in time of venography and at the time of balloon dilation, which was affecting the quality of sedation compared to TCI. Similarly, Arslan G, et al. found that ‘The Observer’s Assessment of Alertness and Sedation’ (OAAS) scales during surgery were lower in the TCI group overall, while the bispectral index score (BIS) in the TCI group was significantly lower at significant times in comparison to the MCI group.11
Our results identified differences in sedation related complications between both groups. TCI group was associated with fewer complication in the form of delayed recovery, desaturation and hypotension. In the MCI group, the most common adverse event was oxygen desaturation below 90% occurring in 23.7% of patients, and hypotension in 10.5% of patients, and one patient was excluded due to repeated desaturation and converted to general anesthesia.
Similarly, Cuiabano et al., aimed to compare the safety and efficacy of TCI versus intermittent bolus administration of propofol for sedation during colonoscopy procedures. They proved that agitation was more common in the intermittent bolus group.28 Guzzo et al. assessed the safety and efficacy of propofol TCI for sedation during gastrointestinal endoscopic procedures performed by the anesthesiologists. The most common adverse event was oxygen desaturation below 95%, occurring in 22.35% of patients. Other adverse events included need of vasoactive drug administration (19.2%), hypotension (12.64%), and oxygen desaturation below 90% (9.92%). Only 0.5% of patients required advanced airway management.29
In our study patient satisfaction, and interventional radiologist satisfaction scores were highly significantly superior in TCI group. Similarly, Wang et al., showed that the endoscopist's satisfaction score was significantly higher in the TCI group compared to the MCI group. However, patient satisfaction scores were similar between the two groups.24 On the contrary, Gülten Arslan et al. reported that the surgeon’s satisfaction was in TCI group was higher.11,12 This may be because all patients underwent spinal anesthesia, so they felt no pain.
One of the limitations of our study was the relatively small sample size and it was a single center study. Additionally, our study focused exclusively on intraoperative variables and short-term outcomes, lacking long-term follow-up data to assess the sustained benefits of TCI over manual infusion techniques.
TCI achieved effective sedation for TIPS procedure, with less propofol consumption, and less sedation related complications. TCI had superior patient and interventional radiologist satisfaction when compared to MCI.
7. Data availability
The numerical data generated during this research is available with the authors and can be provided on request.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
ME: Concept, data analysis, literature search, revised and approved the manuscript
MS: Revised and approved the manuscript
AG: Data collection, data analysis and manuscript writing
AA: Designed the study protocol, manuscript editing, revised and approved the manuscript.
Author affiliation:
- Minatallah Ali Elshafie, Department of Anesthesia, National Liver Institute, Menoufia University, Shebin Elkom City, Egypt; Email: menna80mas@gmail.com; ORCID: {0000-0002-4752-7913}
- Mohammed Abdelrahman Salem, Department of Anesthesiology, Intensive Care & Pain Management, Faculty of Medicine, Menoufia University, Egypt; E-mail: msalem700@gmail.com; ORCID: {0009-0004-7236-4206}
- Asmaa Morsy Ghoniem, Department of Anesthesia, National Liver Institute, Menoufia University, Shebin Elkom City, Egypt; Email: New.start5550@gmail.com; ORCID: {0009-0006-9736-109X}
- Amal Ismail Abdelrahman, Department of Anesthesiology, Intensive Care & Pain Management, Faculty of Medicine, Menoufia University, Egypt; Email: aml.ismaeel.12@med.menofia.edu.eg
ABSTRACT
Background & objective: Transjugular intrahepatic portosystemic shunt (TIPS) is used to form a tract between the portal and the hepatic veins, with a metallic stent bridged through the hepatic parenchyma for patients who have chronic liver disease causing multisystem physiological disruption. The purpose of this study was to compare the quality of sedation in the radiology suit during TIPS procedure with propofol using target-controlled infusion (TCI) versus manual infusion.
Methodology: This prospective study enrolled 78 ASA II patients, scheduled for TIPS procedure, who were randomly allocated into two equal groups; TCI group to have sedation with propofol guided with TCI system, and MCI group (manual infusion group) received propofol manually. We aimed primarily to study the effectiveness of TCI in sedation for TIPS procedure regarding SedLine levels and sedation-related complications, while the secondary outcomes were to evaluate the amount of total propofol consumption, the recovery time, with recording the patient and interventional radiologist satisfaction.
Results: There were statistically highly significant higher SedLine readings in the MCI group at times of venography and balloon dilation compared to TCI group respectively (P < 0.001). The TCI group showed more stable hemodynamics when compared to MCI group. While there was highly significant lower result in the TCI than MCI group regarding propofol dose (589.6 ± 174.9 vs. 711.6 ± 53.3 mg) and Recovery time (12.9 ± 3.9 vs. 18.3 ± 4.5 min; P < 0.0010) respectively. Also, the TCI group showed more patient and radiologist satisfaction scores.
Conclusion: Target-controlled infusion achieved more effective sedation for transjugular intrahepatic portosystemic shunt procedure, with less propofol consumption, and less sedation related complications. Target-controlled infusion had better patient and interventional radiologist satisfaction when compared to manually controlled infusion.
Key words: Chronic Liver Disease; Propofol; Target Control Infusion; Transjugular Intrahepatic Portosystemic Shunt Procedure
Citation: Elshafie MA, Salem MA, Ghoniem AM, Abdelrahman AI. Target controlled vs. manually controlled infusion of propofol for sedation during transjugular intrahepatic portosystemic shunt procedure: a randomized controlled trial. Anaesth. pain intensive care 2025;29(3):403-410. DOI: 10.35975/apic.v29i3.2754
Received: January 04, 2025; Revised: March 14, 2025; Accepted: March 29, 2025
1. INTRODUCTION
Transjugular Intrahepatic Portosystemic Shunt (TIPS) has been used in cirrhotic patients for the management of portal hypertension complications as varices and refractory ascites.1 TIPS has also been used as a potential treatment for Hepatopulmonary Syndrome (HPS).2 The procedure was first described by Josef Rösch and was first used in human patients by Colapinto from the University of Toronto, Canada in 1982.3,4 TIPS is a synthetic stent inserted under radiological guidance within the liver tissue that helps to communicate the inflow of the portal vein with the outflow of the hepatic vein.5
Patients undergoing TIPS are medically complex as a result of the chronic liver disease that cause multisystem physiological disruption. They should receive multidisciplinary preoperative assessment and optimization before undergoing the procedure.6 Complexities of remote site should be considered, where the care administration is in an unfamiliar environment with considering staff and equipment availability. Sedation can be used to avoid the need for general anesthesia, using combinations of short acting sedative agents. The choice of drugs demand consideration of the physiological and pharmacokinetic changes seen in chronic liver disease patients.7
Propofol can be suitable for TIPS anesthesia, due to its pharmacological properties such as rapid onset of action, rapid change of sedation level and early recovery due to its large volume of distribution and a high-clearance rate.8 Also, it has an excellent amnesic effect, and low incidence of nausea and vomiting.9 The aims of sedation are to ensure the safety and well-being of the patient, to minimize the discomfort by providing anxiolysis, amnesia, and analgesia; to ensure that there is behavior and movement control that will allow for the procedure to be completed safely; and to bring the patient safely to discharge.10 The infusion rate should be changed intermittently to maintain the desired level of sedation.11
Target-controlled infusion (TCI) is an intravenous administration system, and is a pharmacokinetic model with a computer-controlled device that allows intravenous anesthetic drugs to be administered to a calculated target plasma concentration, mathematically predicted by a delivery algorithm. It can be enhanced to reduce bias and increase precision by incorporating covariates like age, weight, and sex and utilizing a pharmacokinetic model generated from its own population.12
The TCI-system uses its pharmacokinetic model to calculate the initial loading dose and infusion rate required to reach the desired target concentration.13 The drug passes from the blood or plasma to the central nervous system (CNS), to the effect site, where it exerts its activity.14
The Marsh pharmacokinetic parameters,15 that are incorporated into the Diprifusor TCI system parameters have been proven to provide a stable blood-therapeutic agent concentration for propofol induction and maintenance of anesthesia in patients without organ dysfunction.16
TCI has ability to maintain more consistent plasma concentrations with fewer fluctuations, the smooth process of induction and easily adjustable depth of anesthesia as well as more predictable recovery time.17-20 The aid of SedLine monitoring of the hypnotic component of anesthesia could be beneficial to avoid inadequate lower doses, or excessive administration of anesthetics that may be associated with an increased risk of postoperative neurocognitive disorder.21
We aimed primarily to evaluate the effectiveness of TCI in sedation for TIPS procedure regarding SedLine levels and sedation-related complication, and secondarily to evaluate the recovery time, recovery profile, total propofol consumption, and the patient and interventional radiologist satisfaction levels.
2. METHODOLOGY
Formal approval was obtained from the ethics and research committee of Faculty of Medicine, Menoufia University, Egypt 5/3/2023 ) and the Institutional Research Board, (IRB) of the National Liver Institute, Menoufia University, Egypt on 1 July 2023, with protocol number 00003413FWA0000227, and registered at the Cochrane South Africa Registry (PACTR202310626983365) on 19 October 2023.This prospective, randomized, controlled trial was conducted at the Interventional Radiology Department, National Liver Institute, Menoufia University, Egypt from 20 October 2023 to 28 July 2024.
2.1. Study Design
The study included 78 patients of both sexes, aged 18 to 60 years, with an ASA-PS II, candidates for TIPS intervention. Patients with uncontrolled cardiovascular, respiratory or renal dysfunction, patients allergic to any used anesthetic agent, morbidly obese with body mass index (BMI) ≥ 40 kg/m2), patients undergoing perioperative significant bleeding or hemodynamic instability (e.g., air embolism), and who refused to participate in the study, were excluded from the study.
Based on previous studies (Laso et al., 2016) who reported that recovery time was significantly shorter in TCI group than MIT group (TCI: 7.48 ± 3.1 vs. manual: 10.3 ± 4.9min) (P =.008), minimum sample size calculated was 34 patients in each group, to be increased to 38 patients in each group for 15% drop-out rate.
After written informed consent, patients were allocated into two equal groups using a random number generator in sealed envelopes technique. The study group experienced anesthesia through the target-controlled infusion pump (TCI group), and the control group was conducted manually by infusion pump (MCI group).
2.2. Anesthetic Management
On arrival to the radiology suite, standard monitors were attached to the patient, two 20-gauge intravenous cannulas were secured, and a nasal cannula with oxygen flowing at 3–5 L/min was applied to each patient. SedLine was applied after skin preparation and disinfection with alcohol and slight rubbing for anesthesia depth monitoring. The four electrodes of the Electrical Cardiometry (EC) were applied after skin sterilization by alcohol swab, (first: approximately 5 cm above left base of the neck; second, on the left base of the neck; third, on the lower left thorax at the level of xiphoid and the fourth on the lower left thorax approximately 5 cm below 3rd electrode at level of anterior axillary line), and the patient’s data was applied. Verification of the correct signal quality was accomplished by visualization of the ECG, the impedance waveform and its first derivative. The patient’s position was carefully checked so that intravenous lines were not occluded.
Anesthesia induction for patients in the TCI group was done by using TCI pump (Injectomat TIVA Agilia, Fresenius Kabi syringe pump). The initial target of plasma propofol concentration for each patient was set according to the age. It was 4 μg/mL in the patients aged over 50 years, and 5 μg/mL in ≤ 50 years using the Marsh pharmacokinetic model.6 Then the TCI extension line was connected to the patient and infusion started until SedLine target range (25-50) was reached, fentanyl (1-1.5 μg/kg) bolus was given. The induction was planned to be achieved over 10 min, but if any hemodynamic instability was recorded (hypotension, bradycardia or desaturation), induction time was increased to 15 min.
When SedLine reached the targeted values and the patient lost responsiveness, the TIPS procedure started. Local anesthetic drug (lidocaine hydrochloride 1%) was used for the port of entry of the needle in the right internal jugular in all patients. The TIPS procedure is not painful. The extent of procedural pain is limited to the puncture wound in the neck, puncture of the liver capsule and pain during dilation of the Wallstent device.
For maintenance of anesthesia, the target concentration was gradually increased by 0.5 μg/mL, when SedLine reading exceeded the target range to be more than 50, or when BP and HR increased by 20% above the baseline. On the other hand, the target plasma concentration was decreased by 0.5 μg/mL, when SedLine reading decreased below 25, or BP and HR decreased by 20% below the baseline, or SpO2 fell below 92%.
For the MCI group anesthesia was induced with propofol bolus (1 mg/kg) over 10 min, then 170 µg/ kg/min infusion for 10 min using BD Alaris™ CC Plus syringe pump , and then 130 µg/kg/min for another 10 min, while monitoring the SedLine readings to obtain the target range (25-50)..22 When the target level was reached, fentanyl 1-1.5 μg/kg was given and the TIPS procedure started.
Anesthesia was maintained by infusion of propofol 100 µg/kg/min, increasing the rate by 10 µg/kg/min, when SedLine reading exceeded the target range of 50, and also when BP and HR increased by 20% above the baseline. Propofol infusion rate was decreased by (10 µg/kg/min), when SedLine reading decreased below 25 or mean blood pressure and heart rate decreased by 20% below the patient baseline.
The fluid therapy was managed in all patients according to EC readings to keep corrected flow time (FTC) within normal range to maintain the patient on the euvolumic side throughout the procedure. Hypotension was managed by 5 mg of ephedrine intravenously and any other vasopressor doses was recorded if needed.
At the end of the procedure, in the TCI group the target plasma drug concentration was adjusted to be (0 μg/mL). While in the MCI group the propofol infusion was stopped. All patients were allowed to regain consciousness while they were monitored. When SedLine values were above 80, SpO2 above 95% and patients were hemodynamically stable, they were transferred to post-anesthesia care unite (PACU). They were monitored until their modified Aldrete scores were 9-10, then discharged to the ward.
2.3. Measured Data
Hemodynamic parameters (MBP and HR), cardiac output (CO), and SedLine score were measured at; base line (T1), after induction of anesthesia (T2), at time of puncture of liver capsule (T3), time of venography (T4), time of balloon dilatation (T5) and time from the discontinuation of propofol infusion until adequate response to verbal command (recovery time) (T6).
Total propofol consumption, recovery time, procedure time, patient satisfaction score and intervention radiologist satisfaction scores were recorded.
Complications related to the procedure (pneumothorax, arrhythmia and bleeding) and sedation related complications ((hypotension, bradycardia, and hypoxemia) were recorded within the first 24 hours.
2.4. Statistical analysis
Data were collected, tabulated and statistically analyzed using an IBM compatible personal computer with Statistical Package for the Social Sciences (SPSS) version 26. Descriptive statistics e.g. qualitative data were expressed as Number (N), percentage (%), while quantitative data were expressed as mean (x̅), standard deviation (SD) and range (minimum-maximum). Student’s t-test (t) is a test of significance used for comparison of quantitative variables between the two groups of normally distributed data. Repeated measures ANOVA test was used for comparison of quantitative variables between more than two consecutive measures in the same group of normally distributed data. Chi-square test (χ2) was used to study association between qualitative variables. Whenever any of the expected cells were less than five, Fisher’s Exact test was used. Significant test results were quoted as two-tailed probabilities. Significance of the obtained results was judged at the 5% level (P > 0.05).
3. RESULTS
A total of 78 patients were included in this study. They were divided into 2 groups: TCI group and MCI group; in TCI group one patient was excluded due to failed TIPS procedure, while, in the MCI group another patient was excluded due to conversion to general anesthesia after repeated oxygen desaturation. Finally, 76 patients were analyzed, and equally divided in both groups.
Age, sex, BMI and ASA scores were compared between TCI and MCI groups showing no significant difference between both groups (P > 0.05) as shown in Table 1.
| Table 1: Comparative demographic data of both groups | ||||
| Parameter | TCI group (N=38) |
MCI group (N=38) |
P-value | |
| Age (years) | Mean ± SD | 32.9 ± 10.9 | 34.5 ± 9.4 | 0.488 t |
| Range | 18-55 | 18-55 | ||
| BMI (kg/m2): | Mean ± SD | 25.7 ± 3.2 | 26.7 ± 2.5 | 0.136 t |
| Range | 20-35 | 21-30 | ||
| Gender | Male | 14 (36.8) | 17 (44.7) | 0.484 χ2 |
| Female | 24 (63.2) | 21 (55.3) | ||
| ASA | II | 38 (100.0) | 38 (100.0) | - |
| Data presented as Mean ± SD, Range or n (%)
P < 0.05 considered significant; t: student t test, χ2: Chi-square test |
||||
Figure 1: Comparative MAP measurements during TIPS procedure in the studied groups
There was a statistically significant difference between both groups regarding MAP during time of venography and time of balloon dilation while other measurements showed no significant differences
between both groups (Figure 1). Regarding HR there was no significant difference between TCI and MCI groups during different steps of TIPS procedure (Figure 2).
There was a highly significant difference between TCI and MCI groups regarding SedLine at time of venography (40.8 ± 6.3 vs. 46.3 ± 4.2) and the time of balloon dilation (39.5 ± 6.1 vs. 45.1 ± 3.4). Other SedLine comparisons showed no statistically significant differences (Figure 3).
There were no significant differences between TCI and MCI groups regarding recovery score and procedure time (P > 0.05) (Table 2). While there were highly significant differences between the groups regarding total propofol required and recovery time (P < 0.001).
| Table 2: Comparative total propofol consumption, recovery time, recovery score, and total time of the procedure | ||||
| Variables | TCI group
(N=38) |
MCI group (N=38) |
(t) | P-value |
| Propofol dose (mg) | 589.6 ± 174.9 (400-1305) | 711.6 ± 53.3 (550-780) | 4.11 | < 0.001** |
| Recovery time (min) | 12.9 ± 3.9 (3-20) | 18.3 ± 4.5 (10-26) | 5.53 | < 0.001** |
| Recovery score | 9.2 ± 0.4 (9-10) | 9.3 ± 0.5 (9-10) | 1.38 | 0.173 |
| Procedure time (min) | 70.9 ± 15.8 (37-110) | 76.3 ± 13.2 (45-105) | 1.63 | 0.109 |
| Data presented as Mean ± SD (Range); **: P < 0.001 considered as highly significant; t: Student’s t test | ||||
Figure 2: Comparative HR measurements during TIPS procedure in the studied groups
There was highly significant difference between both groups regarding patient satisfaction and radiologist satisfaction (P < 0.001) (Table 3). In patient satisfaction ‘completely comfortable’ category in TCI and MCI groups was 47% and 7.9% respectively, while in the ‘slight discomfort’ and ‘painful’ categories were (13.2% vs. 36%) and (0% vs. 15.8%) respectively. As shown in Table 4 there was no statistically significant difference between TCI and MCI groups regarding Procedure complications (P > 0.05). While there was significant difference between TCI and MCI groups regarding complications (P < 0.05).
Figure 3: Comparative SEDline measurements during TIPS procedure in the studied groups
| Table 3: Comparative patient satisfaction, and interventional radiologist satisfaction scores | ||||
| Parameter | TCI group
(N=38) |
MCI group (N=38) |
Chi square test (χ2) | P-value |
| Patient satisfaction score: | ||||
| Completely comfortable | 18 (47.4) | 3 (7.9) | 22.31 | < 0.0018**
|
| Quite comfortable | 13 (34.2) | 13 (34.2) | ||
| Slight comfortable | 2 (5.3) | 1 (2.6) | ||
| Slight discomfort | 5 (13.2) | 14 (36.8) | ||
| Painful | 0 | 6 (15.8) | ||
| Very painful | 0 | 1 (2.6) | ||
| Radiologist satisfaction score: | ||||
| Very bad | 0 | 3 (7.9) | 33.76 | < 0.001**
|
| Bad | 0 | 12 (31.6) | ||
| Moderate | 4 (10.5) | 12 (31.6) | ||
| Good | 16 (42.1) | 9 (23.7) | ||
| Very good | 18 (47.4) | 2 (5.3) | ||
| **: highly significant, (P < 0.001) considered as highly significant; *: significant; (P < 0.05) considered as significant
Data presented as n (%) |
||||
| Table 4: Comparative anesthetic and procedural complications | |||||
| Complications | TCI group (N=38) |
MCI group (N=38) |
Chi square test (χ2) | P-value | |
| Anesthetic complications: | Delayed recovery | - | 2 (5.3) | 16.05 | 0.003*
|
| Desaturation | - | 9 (23.7) | |||
| Hypotension | 2 (5.3) | 4 (10.5) | |||
| Hypotension and delayed recovery |
- | 1 (2.6) | |||
| Non | 36 (94.7) | 22 (57.9) | |||
| Procedural complications: | Arrhythmia | 5 (13.2) | 3 (7.9) | FE
0.56 |
0.711 |
| Non | 33 (86.8) | 35 (92.1) | |||
| Data presented as n (%); FE: Fischer’s Exact test; *: P < 0.05 considered as significant; Data presented as n (%) | |||||
4. DISCUSSION
Anesthetic management for TIPS patients was a critical aspect of the procedural care, as the patient was medically complex with multisystem physiological disruption with the superadded complexities of remote site anesthesia. TCI systems have been recently established, allowing for easier adjustment of anesthesia depth while enhancing cardiovascular and respiratory stability. The aid of SedLine monitoring the hypnotic component to guide anesthetic management is crucial.
In the present study, we recorded intraoperative hemodynamic changes comparing the use of TCI pumps versus MCI. We found that employing the TCI system led to several significant advantages including more stable hemodynamic parameters during critical procedural stages, improved sedation
management, and faster post-procedural recovery time.
| Figure 3: Comparative SEDline measurements during TIPS procedure in the studied groups |
| Figure 2: Comparative HR measurements during TIPS procedure in the studied groups |
and remifentanil compared with MCI anesthesia in mastoidectomy surgeries.23 They concluded that TCI-based anesthesia achieved better hemodynamic stability through the stages, better recovery profile, decreased drug costs of anesthetics and more satisfaction of surgeons about surgical field condition, as compared to the MCI. Also, Wang et al. compared the sedation quality and safety of TCI and MCI of propofol during colonoscopy procedures. Their results showed that the TCI group demonstrated more stable hemodynamic status, with higher lowest MAP and lower highest MAP compared to the MCI group. Furthermore, patients in the TCI group experienced earlier recovery.24
In our study, we assessed the consumed propofol dose and recovery time between the TCI and manual groups, and found that there were highly significant less total propofol consumption in the TCI group and consequently shorter recovery times when compared to the manual group. Triem JG et al. compared optimated-target-controlled-infusion (OTCI) and manually-controlled infusion (MCI) technique in nasal sinus surgery. They found propofol consumption was similar within the first 60 min for both groups; thereafter, significantly less propofol usage in the OTCI group than the MCI group.25
Sahu et al. compared manual infusion versus TCI of propofol in total intravenous anesthesia (TIVA) during endoscopic retrograde cholangio-pancreatography (ERCP) procedures. Their results showed that the TCI group had significantly shorter recovery times compared to the TIVA group.26
On the other hand, Hsieh M-L et al. studied a comparison of the TCI and the MCI of propofol anesthesia during electroconvulsive therapy (ECT) found that the TCI group used higher doses of propofol, and longer procedural and recovery time.27 Such potential inferiority in efficacy in the TCI group might be explained by short procedure time and higher doses of propofol used for induction and so longer recovery time.
In terms of SedLine measurements, our study revealed significant differences between both of the groups with higher readings in the MCI group in time of venography and at the time of balloon dilation, which was affecting the quality of sedation compared to TCI. Similarly, Arslan G, et al. found that ‘The Observer’s Assessment of Alertness and Sedation’ (OAAS) scales during surgery were lower in the TCI group overall, while the bispectral index score (BIS) in the TCI group was significantly lower at significant times in comparison to the MCI group.11
Our results identified differences in sedation related complications between both groups. TCI group was associated with fewer complication in the form of delayed recovery, desaturation and hypotension. In the MCI group, the most common adverse event was oxygen desaturation below 90% occurring in 23.7% of patients, and hypotension in 10.5% of patients, and one patient was excluded due to repeated desaturation and converted to general anesthesia.
Similarly, Cuiabano et al., aimed to compare the safety and efficacy of TCI versus intermittent bolus administration of propofol for sedation during colonoscopy procedures. They proved that agitation was more common in the intermittent bolus group.28 Guzzo et al. assessed the safety and efficacy of propofol TCI for sedation during gastrointestinal endoscopic procedures performed by the anesthesiologists. The most common adverse event was oxygen desaturation below 95%, occurring in 22.35% of patients. Other adverse events included need of vasoactive drug administration (19.2%), hypotension (12.64%), and oxygen desaturation below 90% (9.92%). Only 0.5% of patients required advanced airway management.29
In our study patient satisfaction, and interventional radiologist satisfaction scores were highly significantly superior in TCI group. Similarly, Wang et al., showed that the endoscopist's satisfaction score was significantly higher in the TCI group compared to the MCI group. However, patient satisfaction scores were similar between the two groups.24 On the contrary, Gülten Arslan et al. reported that the surgeon’s satisfaction was in TCI group was higher.11,12 This may be because all patients underwent spinal anesthesia, so they felt no pain.
5. LIMITATIONS
One of the limitations of our study was the relatively small sample size and it was a single center study. Additionally, our study focused exclusively on intraoperative variables and short-term outcomes, lacking long-term follow-up data to assess the sustained benefits of TCI over manual infusion techniques.
6. CONCLUSION
TCI achieved effective sedation for TIPS procedure, with less propofol consumption, and less sedation related complications. TCI had superior patient and interventional radiologist satisfaction when compared to MCI.
7. Data availability
The numerical data generated during this research is available with the authors and can be provided on request.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
ME: Concept, data analysis, literature search, revised and approved the manuscript
MS: Revised and approved the manuscript
AG: Data collection, data analysis and manuscript writing
AA: Designed the study protocol, manuscript editing, revised and approved the manuscript.
REFERENCES
- García-Pagán JC, Saffo S, Mandorfer M, Garcia-Tsao G. Where does TIPS fit in the management of patients with cirrhosis? JHEP Rep. 2020;2(4):100122. PubMed DOI: 1016/j.jhepr.2020.100122
- Paramesh AS, Husain SZ, Shneider B, Guller J, Tokat I, Gondolesi GE, et al. Improvement of hepatopulmonary syndrome after transjugular intrahepatic portasystemic shunting: case report and review of literature. Pediatr Transplant. 2003;7(2):157–62. PubMed DOI: 1034/j.1399-3046.2003.00033.x
- Rösch J, Hanafee W, Snow H, Barenfus M, Gray R. Transjugular intrahepatic portacaval shunt an experimental work. Am J Surg. 1971;121(5):588–92. PubMed DOI: 1016/0002-9610(71)90147-4
- Colapinto R, Stronell R, Birch S, Langer B, Blendis L, Greig P, et al. Creation of an intrahepatic portosystemic shunt with a Grüntzig balloon catheter. Can Med Assoc J. 1982;126(3):267. PubMed
- Patidar KR, Sydnor M, Sanyal AJ. Transjugular intrahepatic portosystemic shunt. Clin Liver Dis. 2014;18(4):853–76. PubMed DOI: 1016/j.cld.2014.07.006
- Yang XY, Zhou ZB, Yang L, Zhou X, Niu LJ, Feng X. Hemodynamic responses during induction: comparison of Marsh and Schnider pharmacokinetic models. Int J Clin Pharmacol Ther. 2015;53(1):32–40. PubMed DOI: 5414/CP202141
- Rahimzadeh P, Safari S, Faiz SHR, Alavian SM. Anesthesia for patients with liver disease. Hepat Mon. 2014;14(7). PubMed DOI: 5812/hepatmon.19881
- Pan JR, Cai J, Zhou SL, Zhu QQ, Huang F, Zhang YH, et al. Pharmacodynamic analysis of target-controlled infusion of propofol in patients with hepatic insufficiency. Biomed Rep. 2016;5(6):693–8. PubMed DOI: 3892/br.2016.786
- Chana A, James M, Veale P. Anaesthesia for transjugular intrahepatic portosystemic shunt insertion. BJA Educ. 2016;16(12):405–9. DOI: 1093/bjaed/mkw022
- Höhener D, Blumenthal S, Borgeat A. Sedation and regional anaesthesia in the adult patient. Br J Anaesth. 2008;100(1):8–16. PubMed DOI: 1093/bja/aem342
- Arslan G, Sezen Ö. Comparison of target controlled infusion and manual infusion of propofol for sedation in spinal anesthesia. Ain Shams J Anesthesiol. 2020;12(1). DOI: 1186/s42077-020-00063-0
- Short T, Lim T, Tam Y. Prospective evaluation of pharmacokinetic model-controlled infusion of propofol in adult patients. Br J Anaesth. 1996;76(2):313–5. PubMed DOI: 1093/bja/76.2.313
- Schraag S, Flaschar J, Georgieff M. Target controlled infusion (TCI)--status and clinical perspectives. Anasth Intensiv Notfall Schmerzther. 2000;35(1):12–20. PubMed DOI: 1055/s-2000-10845
- Absalom A, Mani V, De Smet T, Struys M. Pharmacokinetic models for propofol—defining and illuminating the devil in the detail. Br J Anaesth. 2009;103(1):26–37. PubMed DOI: 1093/bja/aep143
- Marsh B, White M, Morton N, Kenny G. Pharmacokinetic model driven infusion of propofol in children. Br J Anaesth. 1991;67(1):41–8. PubMed DOI: 1093/bja/67.1.41
- Cortínez LI, De la Fuente N, Eleveld DJ, Oliveros A, Crovari F, Sepulveda P, et al. Performance of propofol target-controlled infusion models in the obese: pharmacokinetic and pharmacodynamic analysis. Anesth Analg. 2014;119(2):302–10. PubMed DOI: 1213/ANE.0000000000000317
- Egan TD, Weiskopf RB. Target-controlled drug delivery: progress toward an intravenous “vaporizer” and automated anesthetic administration. Anesthesiology. 2003;99(5):1214–9. PubMed DOI: 1097/00000542-200311000-00031
- Hu LG, Pan JH, Li J, Kang F, Jiang L. Effects of different doses of sufentanil and remifentanil combined with propofol in target-controlled infusion on stress reaction in elderly patients. Exp Ther Med. 2013;5(3):807–12. PubMed DOI: 3892/etm.2013.900
- Derrode N, Lebrun F, Levron JC, Chauvin M, Debaene B. Influence of peroperative opioid on postoperative pain after major abdominal surgery: sufentanil TCI versus remifentanil TCI. A randomized, controlled study. Br J Anaesth. 2003;91(6):842–9. PubMed DOI: 1093/bja/aeg263
- Kreuer S, Biedler A, Larsen R, Altmann S, Wilhelm W. Narcotrend monitoring allows faster emergence and a reduction of drug consumption in propofol–remifentanil anesthesia. Anesthesiology. 2003;99(1):34–41. PubMed DOI: 1097/00000542-200307000-00009
- Obert DP, Schneider F, Schneider G, von Dincklage F, Sepulveda P, García PS, et al. Performance of the SedLine monitor: age dependency and time delay. Anesth Analg. 2023;137(4):887–95. PubMed DOI: 1213/ANE.0000000000006369
- Yeganeh N, Roshani B, Yari M, Almasi A. Target-controlled infusion anesthesia with propofol and remifentanil compared with manually controlled infusion anesthesia in mastoidectomy surgeries. Age (Y). 2010;28:9.79. PubMed
- Yeganeh N, Roshani B, Yari M, Almasi A. Target-controlled infusion anesthesia with propofol and remifentanil compared with manually controlled infusion anesthesia in mastoidectomy surgeries. Middle East J Anaesthesiol. 2010;20(6):785–93. PubMed
- Wang JF, Li B, Yang YG, Fan XH, Li JB, Deng XM. Target-controlled infusion of propofol in training anesthesiology residents in colonoscopy sedation: a prospective randomized crossover trial. Med Sci Monit. 2016;22:206. PubMed DOI: 12659/msm.895295
- Triem J, Röhm K, Boldt J, Piper S. Comparison of a propofol-based anesthesia regimen using optimated-target-controlled-infusion (OTCI) and manually-controlled infusion (MCI) technique. Anasth Intensiv Notfall Schmerzther. 2006;41(3):150–5. PubMed DOI: 1055/s-2005-921199
- Sahu A, Tripathy DK, Gupta B, Talawar P, Gupta R. Recovery time in target controlled infusion versus manual infusion of propofol in total intravenous anaesthesia for endoscopic retrograde cholangio-pancreatography procedure using laryngeal mask airway-gastro: A randomised comparative study. Indian J Anaesth. 2023;67(Suppl 2):S120–5. PubMed DOI: 4103/ija.ija_484_22
- Hsieh ML, Lu YT, Lin CC, Lee CP. Comparison of the target-controlled infusion and the manual infusion of propofol anesthesia during electroconvulsive therapy: an open-label randomized controlled trial. BMC Psychiatry. 2021;21:71. PubMed DOI: 1186/s12888-021-03069-6
- Cuiabano IS, Garbin PM, Módolo NSP, Nascimento P. Safety and efficacy of target-controlled infusion versus intermittent bolus administration of propofol for sedation in colonoscopy: a randomized controlled trial. Braz J Anesthesiol. 2023;73(6):751–7. PubMed DOI: 1016/j.bjane.2022.06.003
- García Guzzo ME, Fernandez MS, Sanchez Novas D, Salgado SS, Terrasa SA, Domenech G, et al. Deep sedation using propofol target-controlled infusion for gastrointestinal endoscopic procedures: a retrospective cohort study. BMC Anesthesiol. 2020;20:195. PubMed DOI: 1186/s12871-020-01103-w