Wajida Perveen 1, Yasha Sajjad 2, Umer Ilyas 3, Rimsha Naeem 4
Authors affiliations:
Takayasu Arteritis (TA) affects major arteries in the body and it is a rare vasculitis that causes inflammation and leads to loss of pulse and raised blood pressure. In our case, stroke lead to an accidental diagnosis of TA. Moreover, physical symptoms such as problems with maintaining balance and the muscular strength have never been reported in previous case studies, especially in patients presenting with stroke. A 24-year-old female patient was brought to the emergency room in unconscious state and was diagnosed with right-sided ischemic stroke. On diagnostic imaging, her right common carotid artery and left subclavian artery were found to be more than 90% blocked. She was discharged after three days. Her control over maintaining her balance decreased even more with closed eyes and feet together, on manual perturbation approaches directed from right and left sides. Additionally, her left lower limb had reduced muscular strength than her left upper limb.
There are high chances of experiencing frequent falls and reduced muscular strength in this population group, that could hinder their day-to-day activities.
Keyword: Takayasu Arteritis; Balance Impairments; Muscle; Stroke; Doppler Ultrasound
Citation: Perveen W, Sajjad Y, Ilyas U, Naeem R. Takayasu’s arteritis, discovered in a young lady presenting with stroke; a case report. Anaesth. pain intensive care 2025;29(2):350-353. DOI: 10.35975/apic.v29i2.2728
Received: February 04, 2025; Revised: February 13, 2025; Accepted: February 15, 2025
Takayasu Arteritis (TA) is a systemic illness affecting the main arteries in the body. It’s a rare vasculitis which is of unknown origin and causes inflammation, stenosis, and aneurysms in the pulmonary, coronary, medium and large-sized arteries. Systemic demonstrations include an absence of pulses in the limbs, claudication, ischemic strokes, myocardial infarction, hypertension or loss of blood supply to any organ causing an organ failure.1 It is mostly reported in Asian women in their 20’s and 30’s.2
According to the previous literature, there are two phases that have been identified during the course of this disease: the primary phase includes generalized weakness, fatigue, frequent febrile states, frequent episodes of myalgia and joint aches, and weight loss. Advanced phase represents loss of pulses, raised blood pressure values, blurred visions, headaches, dizziness, transient ischemic attacks and stroke.3
In this context, current study presents a unique case involving a 24-year-old Pakistani female, which deviates from the conventional disease progression. Notably, there is a gap in the existing literature as there is no specific study detailing the physical and functional manifestations of these patients in the weeks following discharge from the hospital. This case report aims to shed light on this unexplored aspect of TA.
The patient was doing chores at home when suddenly she started having headache. Afterward, she lost her balance and fell down due to extreme weakness that she was feeling in both of her lower limbs, but more so in her left lower limb. After some time, she started losing sensations in her left upper limb and later on she felt as if her “left side was not the part of her body anymore”. She experienced jaw deviation towards the right side. She lost consciousness and was brought to the emergency department of a public sector tertiary care teaching hospital during the last week of December 2023. At the time of hospital admission, she was pale, and afebrile, with pulse rate of 122 beats/min on ECG and a blood pressure of 100/60 mmHg. She was revived with the help of medications after a few hours.
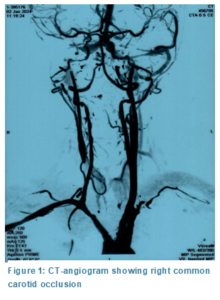
They initially reached a provisional diagnosis of right ischemic stroke. MRI of the brain demonstrated acute ischemic infarct in the right caudate nucleus, lentiform nucleus, and insular cortex. Afterward, she was moved to the neurology ward for work up regarding young age-related stroke. CT-angiogram showed a long segment thrombus extending 5cm cranially from its origin in the right common carotid artery and additionally left subclavian artery also had reduced flow (Figure 1). Carotid Doppler Ultrasound showed more than 90% occlusion in the right common carotid artery extending from its origin up to the carotid bulb. On the other hand, bilateral vertebral arteries, left common carotid artery, internal and external carotid arteries showed normal flow patterns and flow velocities. Her lab reports showed increased levels of cholesterol; triglycerides, low density lipoproteins and very-low density lipoproteins (Table 1).
She was wheelchair bound for 24 hours. She started walking with the help of her attendants after 24 hours and experienced a fall during the first 3 days of her stay at the hospital. After 3 days, she was discharged from the hospital and was completely fine to walk on her own. Her sensations were intact at the time of discharge but some motor symptoms were still there.
She visited physical therapy department at CMH Lahore Medical College after three weeks of the incident. Institutional Ethical Committee Letter has been waived off as the patient presented here is one of the authors. Following findings on manual muscle testing (MMT)4 were noted (Table 1):
Furthermore, patient was unable to stand on toes and heels without support representing significant weakness in intrinsic foot muscles, planter-flexors and dorsiflexors. Modified Ashworth Scale,5, 6 mostly recorded +1 or above grades representing slight spasticity on the left side. It means at the end ranges there was a feeling of rising resistance (slight increase in tone) that the therapist felt in limbs of the subject while performing passive range of motions on left side joints.
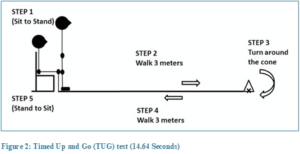
Finger to therapist’s finger and therapist’s finger-nose coordination test7 (Figure 2) was not successfully executed by the patient when performed diagonally. However, finger to her own finger test was successfully demonstrated by the patient. Additionally, left heel to shin test was not properly done by the patient. She took 14.64 seconds to complete Time Up and Go (TUG) test (Figure 2); which is slightly greater than the normal value (13.5 seconds for risk of fall, <10 seconds=normal) as per her age reflecting a risk of fall. 8, 9
Manual perturbations5, 10 were given to the patient to assess balance under the following conditions:
a) Patient stood with eyes opened and feet together:
c) Patient with eyes closed and feet shoulder width apart:
In a detailed interview, the patient stated that she had been experiencing blurry visions and dizziness at random times since the past one month before this hospital admission. A long time ago, she had experienced a complete black out for few minutes but did not lose her memory or consciousness. She linked it to fasting. Occasionally, she had pain in her right arm and she had no radial and brachial pulses bilaterally since the past two years. She also reported history of stroke in her paternal uncle.
Currently, she is on lipid lowering drugs and anti-platelet therapy.
Current study documents a case report of a young female in her mid-20s, who presented with right ischemic stroke and left side hemi paralysis. On different scans, her right common carotid artery showed long and extending thrombus that caused ischemia in right side of her brain effecting lentiform nucleus, caudate nucleus and insular cortex. She was discharged after three days and this incident led to the diagnosis of an uncommon vascular condition known as Takayasu Arteritis. It is unprecedented that this patient presented with ischemic stroke. Usually it is always accompanied by transient ischemic attacks, episodes of fever and weight loss. In this case report, a detailed musculoskeletal and balance related assessment was done three weeks post-hospital stay. Her lower limb showed more loss in strength than her upper limb and she had increased risk of balance impairment.
S Ahmed et al. reported a case of a 22-year-old female presenting with low backache, calf muscle cramps, fatigue, syncopal episodes and fever that used to spike in the morning. She had increased platelet count and her blood pressure was 160/87 mmHg. Her CT scan findings reported diffuse thickening of abdominal and thoracic aorta as well as stenosis of left common carotid artery and left subclavian artery.11 On the other hand, our patient presented with the ischemic stroke and she never had generalized symptoms regarding phase-1 of this disease. Her blood pressure was also lower than the normal and her platelet count was normal.
Another case of a 23 years old patient was reported by Syed et al. in 2024, who developed dropping of facial muscles and lost her consciousness for one day. She developed seizures when anti-platelet therapy was given to her in the emergency room. On CT angiogram, it was found that both common carotid arteries, brachiocephalic and right subclavian arteries had significant stenosis. On MRI, middle cerebral artery showed hemorrhagic lesions. Patient stayed at hospital for several weeks.12 In the present study, patient recovered after 3 days and went home, but she had persistent balance and strength related issues even weeks after her discharge. It can be derived from this that number of arteries involved and the type of stroke determines the prognosis of this disease.
According to American College of Rheumatology (ACR) 2022 criteria for classifying Takayasu Arteritis has been revised with the following points: claudication, presence of arterial bruit, decreased pulse in upper limbs, > 20 mmHg blood pressure difference in both arms, involvement of more than one arteries, paired arteries, female gender, angina, involvement of abdominal aorta, renal or mesenteric vessels, and carotid artery tenderness or reduced pulse.13 The female patient in the current study scored > 5. ACR classification does not include type of stroke, physical manifestations and hyperlipidemia as major scoring contributors.
In contrast to the present study, none of the previously reported cases of TA shed light on physical and balance related manifestations. The current study stresses the need to rule out TA in patients presenting with stroke for better management plans. There are chances that during the interview, patient might have experienced recall biased due to neurological involvement and additionally, advanced equipment for assessing balance such as double belt treadmill was not used to get clear picture about balance related issues in this population. Additionally, it is recommended that long term interventions containing strength training and balance related therapies be explored for optimizing recovery and improving activities of daily living.
Stroke can be the first clinical manifestation of patients with Takayasu arteritis. Patients have more decreased control over maintaining their balance with closed eyes and feet together on manual perturbation approaches directed from right and left sides. There are higher chances of experiencing falls and reduced muscular strengths that can hinder day to day activities in this population group. Moreover, hyperlipidemia can add insult to the injury in this group. CT-angiogram may be conducted in young patients presenting with stroke in order to rule out Takayasu arteritis.
5. Conflict of interest
No conflict of interest to declare.
6. Authors contribution
All authors took part in the interview of the patient, literature search and preparation of the manuscript.
Authors affiliations:
- Wajida Perveen, Department of Physical Therapy, School of Allied Health Sciences, CMH Lahore Medical College, Lahore, Pakistan; E-mail: wjda_noor@yahoo.com, {ORCID:0000-0002-4833-0928}
- Yasha Sajjad, Department of Physical Therapy, School of Allied Health Sciences, CMH Lahore Medical College, Lahore, Pakistan; E-mail: yashasajjad68@gmail.com, {ORCID:0000-0001-6084-3761}
- Umer Ilyas, Department of Physical Therapy, School of Allied Health Sciences, CMH Lahore Medical College, Lahore, Pakistan; E-mail: umerilyas158@yahoo.com, ORCID:0000-0002-2011-3024}
- Rimsha Naeem, DPT student, University of Lahore, Lahore Pakistan; drramsha1999@gmail.com, {ORCID:0009-0001-4226-6371}
ABSTRACT
Takayasu Arteritis (TA) affects major arteries in the body and it is a rare vasculitis that causes inflammation and leads to loss of pulse and raised blood pressure. In our case, stroke lead to an accidental diagnosis of TA. Moreover, physical symptoms such as problems with maintaining balance and the muscular strength have never been reported in previous case studies, especially in patients presenting with stroke. A 24-year-old female patient was brought to the emergency room in unconscious state and was diagnosed with right-sided ischemic stroke. On diagnostic imaging, her right common carotid artery and left subclavian artery were found to be more than 90% blocked. She was discharged after three days. Her control over maintaining her balance decreased even more with closed eyes and feet together, on manual perturbation approaches directed from right and left sides. Additionally, her left lower limb had reduced muscular strength than her left upper limb.
There are high chances of experiencing frequent falls and reduced muscular strength in this population group, that could hinder their day-to-day activities.
Keyword: Takayasu Arteritis; Balance Impairments; Muscle; Stroke; Doppler Ultrasound
Citation: Perveen W, Sajjad Y, Ilyas U, Naeem R. Takayasu’s arteritis, discovered in a young lady presenting with stroke; a case report. Anaesth. pain intensive care 2025;29(2):350-353. DOI: 10.35975/apic.v29i2.2728
Received: February 04, 2025; Revised: February 13, 2025; Accepted: February 15, 2025
1. INTRODUCTION
Takayasu Arteritis (TA) is a systemic illness affecting the main arteries in the body. It’s a rare vasculitis which is of unknown origin and causes inflammation, stenosis, and aneurysms in the pulmonary, coronary, medium and large-sized arteries. Systemic demonstrations include an absence of pulses in the limbs, claudication, ischemic strokes, myocardial infarction, hypertension or loss of blood supply to any organ causing an organ failure.1 It is mostly reported in Asian women in their 20’s and 30’s.2
According to the previous literature, there are two phases that have been identified during the course of this disease: the primary phase includes generalized weakness, fatigue, frequent febrile states, frequent episodes of myalgia and joint aches, and weight loss. Advanced phase represents loss of pulses, raised blood pressure values, blurred visions, headaches, dizziness, transient ischemic attacks and stroke.3
In this context, current study presents a unique case involving a 24-year-old Pakistani female, which deviates from the conventional disease progression. Notably, there is a gap in the existing literature as there is no specific study detailing the physical and functional manifestations of these patients in the weeks following discharge from the hospital. This case report aims to shed light on this unexplored aspect of TA.
2. CASE REPORT
The patient was doing chores at home when suddenly she started having headache. Afterward, she lost her balance and fell down due to extreme weakness that she was feeling in both of her lower limbs, but more so in her left lower limb. After some time, she started losing sensations in her left upper limb and later on she felt as if her “left side was not the part of her body anymore”. She experienced jaw deviation towards the right side. She lost consciousness and was brought to the emergency department of a public sector tertiary care teaching hospital during the last week of December 2023. At the time of hospital admission, she was pale, and afebrile, with pulse rate of 122 beats/min on ECG and a blood pressure of 100/60 mmHg. She was revived with the help of medications after a few hours.
They initially reached a provisional diagnosis of right ischemic stroke. MRI of the brain demonstrated acute ischemic infarct in the right caudate nucleus, lentiform nucleus, and insular cortex. Afterward, she was moved to the neurology ward for work up regarding young age-related stroke. CT-angiogram showed a long segment thrombus extending 5cm cranially from its origin in the right common carotid artery and additionally left subclavian artery also had reduced flow (Figure 1). Carotid Doppler Ultrasound showed more than 90% occlusion in the right common carotid artery extending from its origin up to the carotid bulb. On the other hand, bilateral vertebral arteries, left common carotid artery, internal and external carotid arteries showed normal flow patterns and flow velocities. Her lab reports showed increased levels of cholesterol; triglycerides, low density lipoproteins and very-low density lipoproteins (Table 1).
She was wheelchair bound for 24 hours. She started walking with the help of her attendants after 24 hours and experienced a fall during the first 3 days of her stay at the hospital. After 3 days, she was discharged from the hospital and was completely fine to walk on her own. Her sensations were intact at the time of discharge but some motor symptoms were still there.
She visited physical therapy department at CMH Lahore Medical College after three weeks of the incident. Institutional Ethical Committee Letter has been waived off as the patient presented here is one of the authors. Following findings on manual muscle testing (MMT)4 were noted (Table 1):
| Table 1: Recorded Manual Muscle Testing Grades for muscle strength | |
| Muscles | Grades |
| Left side grip muscles | -4 |
| Left side shoulder and elbow muscles | 4 |
| Left lower limb | 3 |
| Right lower limb | 4 |
Furthermore, patient was unable to stand on toes and heels without support representing significant weakness in intrinsic foot muscles, planter-flexors and dorsiflexors. Modified Ashworth Scale,5, 6 mostly recorded +1 or above grades representing slight spasticity on the left side. It means at the end ranges there was a feeling of rising resistance (slight increase in tone) that the therapist felt in limbs of the subject while performing passive range of motions on left side joints.
Finger to therapist’s finger and therapist’s finger-nose coordination test7 (Figure 2) was not successfully executed by the patient when performed diagonally. However, finger to her own finger test was successfully demonstrated by the patient. Additionally, left heel to shin test was not properly done by the patient. She took 14.64 seconds to complete Time Up and Go (TUG) test (Figure 2); which is slightly greater than the normal value (13.5 seconds for risk of fall, <10 seconds=normal) as per her age reflecting a risk of fall. 8, 9
Manual perturbations5, 10 were given to the patient to assess balance under the following conditions:
a) Patient stood with eyes opened and feet together:
- If push was given from front side, patient used ankle strategy to stabilize herself.
- If she was pushed from back and left side, she used hip strategy and took one step to stabilize herself.
- If a perturbation was added from the right side, then she took more than one step to prevent herself from falling.
c) Patient with eyes closed and feet shoulder width apart:
- Front side perturbation: Same as with open eyes.
- Back and left sides’ perturbation: Used hip strategy and took more than one step.
- Right side approach: Took several steps to avoid falling.
- Patient took several steps to prevent her from falling if perturbations were given from front, back and left sides.
- Patient was unable to maintain her balance even after taking several steps and was saved by the therapist when from right side perturbation was given.
In a detailed interview, the patient stated that she had been experiencing blurry visions and dizziness at random times since the past one month before this hospital admission. A long time ago, she had experienced a complete black out for few minutes but did not lose her memory or consciousness. She linked it to fasting. Occasionally, she had pain in her right arm and she had no radial and brachial pulses bilaterally since the past two years. She also reported history of stroke in her paternal uncle.
Currently, she is on lipid lowering drugs and anti-platelet therapy.
3. DISCUSSION
Current study documents a case report of a young female in her mid-20s, who presented with right ischemic stroke and left side hemi paralysis. On different scans, her right common carotid artery showed long and extending thrombus that caused ischemia in right side of her brain effecting lentiform nucleus, caudate nucleus and insular cortex. She was discharged after three days and this incident led to the diagnosis of an uncommon vascular condition known as Takayasu Arteritis. It is unprecedented that this patient presented with ischemic stroke. Usually it is always accompanied by transient ischemic attacks, episodes of fever and weight loss. In this case report, a detailed musculoskeletal and balance related assessment was done three weeks post-hospital stay. Her lower limb showed more loss in strength than her upper limb and she had increased risk of balance impairment.
S Ahmed et al. reported a case of a 22-year-old female presenting with low backache, calf muscle cramps, fatigue, syncopal episodes and fever that used to spike in the morning. She had increased platelet count and her blood pressure was 160/87 mmHg. Her CT scan findings reported diffuse thickening of abdominal and thoracic aorta as well as stenosis of left common carotid artery and left subclavian artery.11 On the other hand, our patient presented with the ischemic stroke and she never had generalized symptoms regarding phase-1 of this disease. Her blood pressure was also lower than the normal and her platelet count was normal.
Another case of a 23 years old patient was reported by Syed et al. in 2024, who developed dropping of facial muscles and lost her consciousness for one day. She developed seizures when anti-platelet therapy was given to her in the emergency room. On CT angiogram, it was found that both common carotid arteries, brachiocephalic and right subclavian arteries had significant stenosis. On MRI, middle cerebral artery showed hemorrhagic lesions. Patient stayed at hospital for several weeks.12 In the present study, patient recovered after 3 days and went home, but she had persistent balance and strength related issues even weeks after her discharge. It can be derived from this that number of arteries involved and the type of stroke determines the prognosis of this disease.
According to American College of Rheumatology (ACR) 2022 criteria for classifying Takayasu Arteritis has been revised with the following points: claudication, presence of arterial bruit, decreased pulse in upper limbs, > 20 mmHg blood pressure difference in both arms, involvement of more than one arteries, paired arteries, female gender, angina, involvement of abdominal aorta, renal or mesenteric vessels, and carotid artery tenderness or reduced pulse.13 The female patient in the current study scored > 5. ACR classification does not include type of stroke, physical manifestations and hyperlipidemia as major scoring contributors.
In contrast to the present study, none of the previously reported cases of TA shed light on physical and balance related manifestations. The current study stresses the need to rule out TA in patients presenting with stroke for better management plans. There are chances that during the interview, patient might have experienced recall biased due to neurological involvement and additionally, advanced equipment for assessing balance such as double belt treadmill was not used to get clear picture about balance related issues in this population. Additionally, it is recommended that long term interventions containing strength training and balance related therapies be explored for optimizing recovery and improving activities of daily living.
4. CONCLUSION
Stroke can be the first clinical manifestation of patients with Takayasu arteritis. Patients have more decreased control over maintaining their balance with closed eyes and feet together on manual perturbation approaches directed from right and left sides. There are higher chances of experiencing falls and reduced muscular strengths that can hinder day to day activities in this population group. Moreover, hyperlipidemia can add insult to the injury in this group. CT-angiogram may be conducted in young patients presenting with stroke in order to rule out Takayasu arteritis.
5. Conflict of interest
No conflict of interest to declare.
6. Authors contribution
All authors took part in the interview of the patient, literature search and preparation of the manuscript.
7. REFERENCES
- Watanabe R, Berry GJ, Liang DH, Goronzy JJ, Weyand CM. Pathogenesis of Giant Cell Arteritis and Takayasu Arteritis-Similarities and Differences. Curr Rheumatol Rep. 20206;22(10):68. [PubMed] DOI: 10.1007/s11926-020-00948-x
- Gudbrandsson B, Molberg Ø, Garen T, Palm Ø. Prevalence, incidence, and disease characteristics of Takayasu arteritis by ethnic background: data from a large, population‐based cohort resident in southern Norway. Arthritis Care Res. 2017;69(2):278-85. [PubMed] DOI: 10.1002/acr.22931
- Keser G, Aksu K, Direskeneli H. Takayasu arteritis: an update. Turk J Med Sci. 2018 Aug 16;48(4):681-697. [PubMed] DOI: 10.3906/sag-1804-136
- System MMTG. Manual Muscle Testing Grading System. Available from: http://www.scottsevinsky.com/pt/mmt.html
- Unger J, Chan K, Scovil CY, Craven BC, Mansfield A, Masani K, et al. Intensive balance training for adults with incomplete spinal cord injuries: protocol for an assessor-blinded randomized clinical trial. Phys Ther. 2019;99(4):420-7. [PubMed] DOI: 10.1093/ptj/pzy153
- Harb A, Kishner S. Modified Ashworth Scale. 2023 May 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. [PubMed]
- Kottke F. From reflex to skill: the training of coordination. Arch Phys Med Rehabil. 1980;61(12):551-61. [PubMed]
- Sears B. Timed Up and Go (TUG) Test: An Overview Simple test used to estimate the risk of falls; 2023. Available from: https://www.verywellhealth.com/the-timed-up-and-go-test-2696072
- Bell TR. Timed Get Up and Go Implementation to Improve Falls Assessment. 2020. Available from: http://hdl.handle.net/10342/8488
- McCrum C, Bhatt TS, Gerards MH, Karamanidis K, Rogers MW, Lord SR, et al. Perturbation-based balance training: Principles, mechanisms and implementation in clinical practice. Front Sports Act Living. 2022;4:1015394. [PubMed] DOI: 10.3389/fspor.2022.1015394
- Ahmad S, Khan MSA, Bahadori P, Khan A, Ahmad W, Ilyas M, et al. Pakistani Origin Takayasu Arteritis: A Case Report with a Brief Review from Asymptomatic Presentation Till Diagnosis and Clinical Management. DOI: 10.11648/j.ccr.20230704.15
- Syed ER, Salih N, Ullah H, Wahab A, Ali MY, Ayub M, et al. Takayasu's Arteritis: An Uncommon Cause of Hemorrhagic Stroke in Young Individuals. Cureus. 2024;16(1). [PubMed] DOI: 10.7759/cureus.52301
- Grayson PC, Ponte C, Suppiah R, Robson JC, Gribbons KB, Judge A, et al. 2022 American College of Rheumatology/EULAR classification criteria for Takayasu arteritis. Arthritis Rheumatol. 2022;74(12):1872-80. [PubMed] DOI: 10.1002/art.42324