Mohamed AbdelKhalek Mohamed Ali 1, Noha Mohamed Kamar Mohamed 2, Hanaa Mohamed Elgendy 3, Diaa Eldin Shalaby Mohamed AlAwady 4, Hatem Mahmoud Sayed 5
Author affiliations:
Objectives: This research endeavors to pinpoint the variables that foretell failure to wean from mechanical ventilation (MV) among individuals who have experienced cardiac surgery, aiming to mitigate the hazards linked to prolonged stays in the intensive care unit (ICU).
Methodology: The investigation was conducted in the ICU for post-cardiac surgery patients at Ain Shams University Hospital. The study included 80 patients who had undergone cardiac surgery and were subsequently on MV.
Results: Successful extubation was achieved in most patients enrolled in the study. Intraoperative complications were common among participants, with pacemaker wire insertion being the most frequent, followed by ventricular fibrillation. The most frequently performed surgical procedure was coronary artery bypass grafting (CABG), with mitral valve replacement (MVR) being the second most common. Most patients exhibited mild to moderate tracheal secretions. Significant differences were observed between successfully weaned patients and those who failed extubation. Specifically, the failed extubation group demonstrated significantly higher Charlson Comorbidity Index scores, a greater prevalence of chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVS), and significantly lower mean blood pressure (MBP) and PaO2/FiO2 ratios.
Conclusion: The study's results indicate that several independent factors are linked to a higher probability of unsuccessful weaning from MV. These factors include a Sequential Organ Failure Assessment (SOFA) score of 6 or above, a Comorbidity Index exceeding 3, severe tracheal secretions, a respiratory rate to tidal volume ratio (RR/TV) of 57 or higher, and minute ventilation of 13.5 L/min or more.
Abbreviations: ACC: aortic cross-clamp, CABG: coronary artery bypass grafting, COPD: chronic obstructive pulmonary disease, ECC: extracorporeal circulation, MV: mechanical ventilation, MVR: mitral valve replacement
Keywords: Cardiac Surgery; Mechanical Ventilation; Weaning Failure
Citation: Mohamed Ali MAK, Mohamed NMK, Elgendy HM, Mohamed AlAwady DES, Sayed HM. Predictors of weaning failure from mechanical ventilation in post-cardiac surgery patients. Anaesth. pain intensive care 2025;29(2):278-283. DOI: 10.35975/apic.v29i2.2716
Received: February 04, 2025; Revised: February 13, 2025; Accepted: February 15, 2025
Cardiac surgery, due to its intricate nature, significantly disrupts the body's homeostatic mechanisms, placing patients in a vulnerable state. Consequently, meticulous postoperative management within an intensive care setting is crucial for optimal recovery.1 While many patients achieve sufficient hemodynamic stability and consciousness to permit early removal of ventilatory support upon admission to the ICU, others require a prolonged period of mechanical ventilation (MV), leading to increased healthcare costs and a higher probability of complications.2 Determining the appropriate time to discontinue ventilator support necessitates not just astute clinical judgment but also consideration of various predictive factors that can inform the decision-making process.3
Following cardiac surgery, individuals typically regain the capacity for spontaneous breathing upon emergence from anesthesia; thus, the specific ventilation mode employed should have minimal bearing on extubation decisions.4 MV is believed to facilitate the normalization of cardiovascular and other physiological functions following the substantial disturbances caused by cardiopulmonary bypass. Nevertheless, a growing emphasis on cost-effective surgical practices and advancements in anesthetic techniques has fostered a movement towards earlier discontinuation of respiratory support provided after cardiac surgery.5
Despite these advancements, ICU physicians often face challenges in accurately predicting the duration of MV required for individual patients. Currently, no single clinical test or scoring system has demonstrated the ability to reliably classify participants who will necessitate prolonged ventilation, which can result in extended ICU stays and potentially unnecessary interventions like tracheostomy.6 To guide weaning from post-cardiac surgery MV, clinicians routinely assess respiratory mechanics and oxygenation parameters. These include analysis of arterial blood gases and evaluation of ventilator indices such as minute ventilation, respiratory rate, tidal volume, and vital capacity.7
Previous studies have shown that elements like older age, the existence of multiple comorbidities, extended periods of extracorporeal circulation, compromised cardiac function, and reduced cardiac output can hinder successful weaning from MV in patients undergoing cardiac surgery. Moreover, prolonged ventilation has been associated with postoperative hemodynamic instability and neurological complications.8
We studied various factors, including hemodynamic and ventilatory parameters, which might lead to prolonged weaning period in patients on mechanical ventilation.
This prospective observational study was conducted in the post-cardiac surgery ICU at Ain Shams University Hospital, Cairo, Egypt, for 24 months. Informed written consent was obtained from every patient. It included patients who had elective open-heart surgery, were admitted to the ICU, and required general anesthesia with invasive MV. Patients were divided into two groups based on ventilator dependence duration: Group 1 included 73 patients (91.3%) ventilated for less than 48 hours, and Group 2 had seven patients (8.8%) ventilated for more than 48 hours. A total of 80 patients were recruited using a convenient sampling method.
Inclusion criteria were patients aged 18 years or older of both sexes, while exclusion criteria were death within 24 hours post-surgery and pregnancy. The study obtained ethical approval from the institutional ethical committee.
Data collection involved a comprehensive evaluation of preoperative, intraoperative, and postoperative stages. Upon ICU admission, hemodynamic parameters heart rate, mean arterial pressure (MAP), and central venous pressure (CVP) were registered. MV parameters recorded included ventilation mode, plateau pressure, positive end-expiratory pressure (PEEP), respiratory rate, fraction of inspired oxygen (FiO2), oxygen saturation (SpO2), tidal volume, minute volume, rapid shallow breathing index, and maximal inspiratory pressure. Arterial blood gas analysis and hemoglobin levels were measured upon ICU admission and every six hours during the first 24 hours post-surgery.
Patient data were coded, entered into Microsoft Excel, and analyzed using SPSS version 21.0. Qualitative variables were presented as numbers and percentages, and continuous quantitative variables as mean ± standard deviation (SD). Statistical analysis included the Chi-square test for qualitative variable associations and the t-test for quantitative group comparisons, with significance set at P < 0.05 and high significance at P < 0.001.
The patients' ages in this research varied from 30 to 73 (55.475 ± 8.732) years. Most of them were males compared to female (76.3% vs 23.7%). Among all of the patients 30% were smokers. The mean BMI was 30.807 ± 6.618 kg/m2, ranging from 18.6 to 45.5 kg/m2 (Table 1).
Most of our patients (91.3%) could be extubated within the first 48 hours. However, 8.8% (n=7) had difficulties with extubation. Four of them required re-ventilation with invasive MV mode, and 3 required re-ventilation with noninvasive CPAP mode. One patient needed tracheostomy, and one out of the 80 did not survive (Table 2).
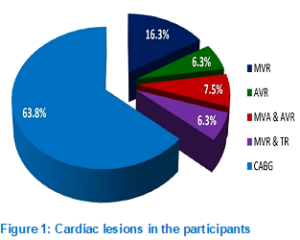
Out of the 80 patients, 63.8% of the patients needed CABG, whereas 16.3% had MVR. Left ventricular EF% varied between 35% and 72%, as shown by echocardiography (Table 3 & Figure 1).
There were statistically insignificant differences between the extracorporeal circulation (ECC) time and aortic cross-clamp (ACC) time of in between weaned or failed-to-wean patients (Table 4).
The SOFA score was significantly greater in patients who could not be successfully weaned off ventilation than those who were weaned off (Table 5). The results demonstrated that compared to weaned off patients, those who failed to be weaned had significantly greater RR/TV ratio, minute volume, maximum inspiratory pressure, and significantly lower PaO2/ FiO2 (Table 6).
A failed extubation can be predicted with an accuracy of 85.7% and a specificity of 84.9% when the cutoff value is 57 RR/TV, 98.6%, and 72.6%, respectively, when the cut-off value is 13.5 MV, 85.7%, and -23 MIP, and 6 SOFA score, according to the Table 7.
To forecast successful extubation, the cutoff values for PO2 are 121 or higher (97.3% sensitivity, 71.4% specificity), 218 or higher (89. % sensitivity, 71.4% specificity), and 72 or higher (98.6% sensitivity, 71.4% specificity) (Table 7).
The present study enrolled 80 patients aged between 30 and 73 years, with a mean age of 55.475 ± 8.732 years. The cohort consisted predominantly of males (76.3%), while females accounted for 23.8%, and 30% of participants were smokers. The average BMI was 30.807 ± 6.618, ranging from 18.6 to 45.5. Successful extubation within the first 48 hours was achieved in 91.3% of patients, whereas 8.8% experienced extubation failure. Among the latter, four required noninvasive CPAP, three needed invasive MV, one underwent tracheostomy, and one patient died. The mortality rates were notably elevated in the group that experienced failed extubation, as opposed to those who were successfully weaned from MV. Nevertheless, no statistically significant disparities were identified between these two groups in terms of age, sex, body mass index (BMI), or smoking status.
Out outcomes matching Sanson et al.,9 which included 205 patients (73% male, 27% female) with mean ages of 66.8 ± 10.0 years for males and 69.5 ± 11.3 years for females. Like our results, they found no significant differences in age or sex between weaned and failed extubation patients. Additionally, Lara et al. corroborated our observation that the group experiencing failed extubation exhibited a significantly higher mortality rate.10
Intraoperative complications were observed in 67.5% of the patients, with pacemaker wire placement being the most common at 36.25%, followed by ventricular fibrillation at 27.5% and bradycardia at 5%. The most frequently performed surgical procedure was CABG, accounting for 63.8% of cases, while MVR was performed in 16.3% of patients. Echocardiography revealed LVEF ranging from 35% to 72%, and the MBP was 85.037 ± 9.914 mmHg, with a range of 56 to 103 mmHg. Sanson et al.[9] CABG was also reported as the most frequent procedure (51%), followed by valvular lesions (26%), and it was noted that the volume of tracheal secretions was markedly elevated in the group that experienced failed extubation. Conversely, Lara et al. reported no significant difference in LVEF between patients who were successfully weaned and those who failed to wean.10
In our study, extracorporeal circulation (ECC) times ranged from 50 to 300 min (mean: 122.925 ± 44.891), and aortic cross-clamp (ACC) times ranged from 30 to 200 minutes (mean: 78.225 ± 28.236). No significant differences in ECC or ACC times were observed between weaned and failed patients, consistent with the findings of Sanson et al.9
The SOFA score in our cohort ranged from 3 to 8 (median: 5), and the FOUR score ranged from 2 to 13 (median: 13). Failed extubation patients had significantly higher SOFA scores. Blood product transfusions were administered to 90% of patients, with packed RBCs (80.1%), fresh frozen plasma (57.5%), and platelets (7.5%) being the most common. No significant differences in transfusion rates were found between weaned and failed patients. In contrast, Sanson et al. reported higher creatinine and lower albumin levels in failed extubation patients, which may be attributed to differing comorbidities.9
Lara et al. found no significant difference in PO2 levels between weaned and failed patients, whereas Yazdanian et al. observed lower preoperative PaO2 levels in reintubated patients compared to controls.10,11
ROC curve analysis revealed that specific cutoff values for RR/TV (≥ 57), MV (≥ 13.5), MIP (≥ -23), and SOFA (≥ 6.5) were predictive of extubation failure, with sensitivities ranging from 85.7% to 98.6% and specificities from 72.6% to 98.6%. For successful extubation, cutoff values for PO2 (≥ 121), PaO2/ FiO2 (≥ 218), and MBP (≥ 72) demonstrated sensitivity of 97.3%, 89%, and 98.6%, respectively, with a specificity of 71.4% for all. The analysis using binary logistic regression identified several independent factors associated with weaning failure, including a SOFA score of 6 or above, a Comorbidity Index exceeding 3, the presence of severe tracheal secretions, an RR/TV of 57 or greater, and minute ventilation of 13.5 L/min or higher.
El-Beheidy et al. indicated that the RSBI showed a significant difference between the groups that experienced successful weaning and those that failed to wean, with a cutoff value of ≥3.5 breaths/min/ml/kg predicting weaning failure with 100% sensitivity and 75% specificity.12 Totonchi et al. found that preoperative, intraoperative, and postoperative variables, including gender, blood transfusion, chronic kidney disease, chronic COPD, duration of the operation, endocarditis, inotrope dependency, postoperative bleeding, time on cardiopulmonary bypass (pump time), and type of surgery.13
The study's limitations included the fact that the sample size was relatively small. The study was conducted in a single center and did not compare our findings with other local anesthetics and different doses and concentrations.
However, the failed extubation group exhibited significantly higher Charlson Comorbidity Index scores and a greater prevalence of COPD and CVS compared to the successfully weaned group. Conversely, MBP and the PO2/ FiO2 ratio were notably reduced in the group that experienced failed extubation. Given the results, it is reasonable to conclude that a SOFA score of 6 or higher, a Comorbidity Index more significant than 3, severe tracheal secretions, an RR/TV ratio of 57 or higher, and minute ventilation of 13.5 L/min or more are independent predictors of unsuccessful weaning from MV.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Funding
The study utilized the hospital resources only.
9. Conflict of interest
The authors declare that there was no conflict of interests.
10. Authors’ contribution
All authors took part in the study and preparation of the manuscript.
Author affiliations:
- Mohamed AbdelKhalek Mohamed Ali, Professor of Anesthesiology, Intensive Care Medicine and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt. Email: mmabdelkhalek99@gmail.com
- Noha Mohamed Kamar Mohamed, Professor of Anesthesiology, Intensive Care Medicine and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt. Email: nmelsharnoby@gmail.com
- Hanaa Mohamed Elgendy, Professor of Anesthesiology, Intensive Care Medicine and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt. Email: hanaelgendy84@gmail.com
- Diaa Eldin Shalaby Mohamed AlAwady, lecturer of Anesthesiology, Intensive Care Medicine and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt. Email: diaelawady@gmail.com
- Hatem Mahmoud Sayed, MD Anesthesiology, Intensive Care Medicine and Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt. Email: dr.hatem123@gmail.com
ABSTRACT
Objectives: This research endeavors to pinpoint the variables that foretell failure to wean from mechanical ventilation (MV) among individuals who have experienced cardiac surgery, aiming to mitigate the hazards linked to prolonged stays in the intensive care unit (ICU).
Methodology: The investigation was conducted in the ICU for post-cardiac surgery patients at Ain Shams University Hospital. The study included 80 patients who had undergone cardiac surgery and were subsequently on MV.
Results: Successful extubation was achieved in most patients enrolled in the study. Intraoperative complications were common among participants, with pacemaker wire insertion being the most frequent, followed by ventricular fibrillation. The most frequently performed surgical procedure was coronary artery bypass grafting (CABG), with mitral valve replacement (MVR) being the second most common. Most patients exhibited mild to moderate tracheal secretions. Significant differences were observed between successfully weaned patients and those who failed extubation. Specifically, the failed extubation group demonstrated significantly higher Charlson Comorbidity Index scores, a greater prevalence of chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVS), and significantly lower mean blood pressure (MBP) and PaO2/FiO2 ratios.
Conclusion: The study's results indicate that several independent factors are linked to a higher probability of unsuccessful weaning from MV. These factors include a Sequential Organ Failure Assessment (SOFA) score of 6 or above, a Comorbidity Index exceeding 3, severe tracheal secretions, a respiratory rate to tidal volume ratio (RR/TV) of 57 or higher, and minute ventilation of 13.5 L/min or more.
Abbreviations: ACC: aortic cross-clamp, CABG: coronary artery bypass grafting, COPD: chronic obstructive pulmonary disease, ECC: extracorporeal circulation, MV: mechanical ventilation, MVR: mitral valve replacement
Keywords: Cardiac Surgery; Mechanical Ventilation; Weaning Failure
Citation: Mohamed Ali MAK, Mohamed NMK, Elgendy HM, Mohamed AlAwady DES, Sayed HM. Predictors of weaning failure from mechanical ventilation in post-cardiac surgery patients. Anaesth. pain intensive care 2025;29(2):278-283. DOI: 10.35975/apic.v29i2.2716
Received: February 04, 2025; Revised: February 13, 2025; Accepted: February 15, 2025
1. INTRODUCTION
Cardiac surgery, due to its intricate nature, significantly disrupts the body's homeostatic mechanisms, placing patients in a vulnerable state. Consequently, meticulous postoperative management within an intensive care setting is crucial for optimal recovery.1 While many patients achieve sufficient hemodynamic stability and consciousness to permit early removal of ventilatory support upon admission to the ICU, others require a prolonged period of mechanical ventilation (MV), leading to increased healthcare costs and a higher probability of complications.2 Determining the appropriate time to discontinue ventilator support necessitates not just astute clinical judgment but also consideration of various predictive factors that can inform the decision-making process.3
Following cardiac surgery, individuals typically regain the capacity for spontaneous breathing upon emergence from anesthesia; thus, the specific ventilation mode employed should have minimal bearing on extubation decisions.4 MV is believed to facilitate the normalization of cardiovascular and other physiological functions following the substantial disturbances caused by cardiopulmonary bypass. Nevertheless, a growing emphasis on cost-effective surgical practices and advancements in anesthetic techniques has fostered a movement towards earlier discontinuation of respiratory support provided after cardiac surgery.5
Despite these advancements, ICU physicians often face challenges in accurately predicting the duration of MV required for individual patients. Currently, no single clinical test or scoring system has demonstrated the ability to reliably classify participants who will necessitate prolonged ventilation, which can result in extended ICU stays and potentially unnecessary interventions like tracheostomy.6 To guide weaning from post-cardiac surgery MV, clinicians routinely assess respiratory mechanics and oxygenation parameters. These include analysis of arterial blood gases and evaluation of ventilator indices such as minute ventilation, respiratory rate, tidal volume, and vital capacity.7
Previous studies have shown that elements like older age, the existence of multiple comorbidities, extended periods of extracorporeal circulation, compromised cardiac function, and reduced cardiac output can hinder successful weaning from MV in patients undergoing cardiac surgery. Moreover, prolonged ventilation has been associated with postoperative hemodynamic instability and neurological complications.8
We studied various factors, including hemodynamic and ventilatory parameters, which might lead to prolonged weaning period in patients on mechanical ventilation.
2. METHODOLOGY
This prospective observational study was conducted in the post-cardiac surgery ICU at Ain Shams University Hospital, Cairo, Egypt, for 24 months. Informed written consent was obtained from every patient. It included patients who had elective open-heart surgery, were admitted to the ICU, and required general anesthesia with invasive MV. Patients were divided into two groups based on ventilator dependence duration: Group 1 included 73 patients (91.3%) ventilated for less than 48 hours, and Group 2 had seven patients (8.8%) ventilated for more than 48 hours. A total of 80 patients were recruited using a convenient sampling method.
Inclusion criteria were patients aged 18 years or older of both sexes, while exclusion criteria were death within 24 hours post-surgery and pregnancy. The study obtained ethical approval from the institutional ethical committee.
Data collection involved a comprehensive evaluation of preoperative, intraoperative, and postoperative stages. Upon ICU admission, hemodynamic parameters heart rate, mean arterial pressure (MAP), and central venous pressure (CVP) were registered. MV parameters recorded included ventilation mode, plateau pressure, positive end-expiratory pressure (PEEP), respiratory rate, fraction of inspired oxygen (FiO2), oxygen saturation (SpO2), tidal volume, minute volume, rapid shallow breathing index, and maximal inspiratory pressure. Arterial blood gas analysis and hemoglobin levels were measured upon ICU admission and every six hours during the first 24 hours post-surgery.
Patient data were coded, entered into Microsoft Excel, and analyzed using SPSS version 21.0. Qualitative variables were presented as numbers and percentages, and continuous quantitative variables as mean ± standard deviation (SD). Statistical analysis included the Chi-square test for qualitative variable associations and the t-test for quantitative group comparisons, with significance set at P < 0.05 and high significance at P < 0.001.
3. RESULTS
The patients' ages in this research varied from 30 to 73 (55.475 ± 8.732) years. Most of them were males compared to female (76.3% vs 23.7%). Among all of the patients 30% were smokers. The mean BMI was 30.807 ± 6.618 kg/m2, ranging from 18.6 to 45.5 kg/m2 (Table 1).
| Table 1: Descriptive clinical data (n= 80) | ||
| Parameter | Result | |
| Age (years) | Mean ± SD | 55.475 ± 8.732 |
| Median [IQR] | 56 [13] | |
| Range | 30−73 | |
| Gender | Male | 61 (76.3%) |
| Female | 19 (23.8%) | |
| BMI (Kg/m2) | Mean ± SD | 30.807 ± 6.618 |
| Median [IQR] | 29.8 [8.93] | |
| Range | 18.6−45.5 | |
| Smokers | 24 (30%) | |
| Data is presented as Mean ± SD or n (%) | ||
| Table 2: Comprehensive overview of the clinical characteristics of the patients | ||
| Parameter | Result | |
| Outcome
|
Successful extubation in first 48h | 73 (91.3) |
| Failed extubation in first 48h | 7 (8.8) | |
| Next, ventilation needed after 48 h | Non-invasive CPAP | 4 (5) |
| Still on invasive MV | 3 (3.7) | |
| Mortality | Survived | 79 (98.75) |
| Died | 1 (1.25) | |
| Data presented as n (%) | ||
| Table 3: Detailed information on the cardiac status | ||
| Parameter | Result | |
| Type of cardiac lesion | MVR | 13 (16.3) |
| AVR | 5 (6.3) | |
| MVR & AVR | 6 (7.5) | |
| MVR & TR | 5 (6.3) | |
| CABG | 51 (63.8) | |
| LV EF% | Mean ± SD | 56.950 ± 7.475 |
| Median [IQR] | 57 [6.75] | |
| Range | 35 -72 | |
| Data presented as n (%) or Mean ± SD. | ||
| Table 4: Comparative time spent in ECC and ACC compared across groups. | |||
| Time | Weaned (N=73) | Failed (N=7) | p-value |
| ECC time | 119.986 ± 44.129 | 123.571 ± 44.320 | 0.096 |
| ACC time | 77.055 ± 28.331 | 80.429 ± 25.993 | 0.236 |
| Data is presented as Mean ± SD.
ECC: extracorporeal circulation, ACC: aortic cross-clamping |
|||
Most of our patients (91.3%) could be extubated within the first 48 hours. However, 8.8% (n=7) had difficulties with extubation. Four of them required re-ventilation with invasive MV mode, and 3 required re-ventilation with noninvasive CPAP mode. One patient needed tracheostomy, and one out of the 80 did not survive (Table 2).
Out of the 80 patients, 63.8% of the patients needed CABG, whereas 16.3% had MVR. Left ventricular EF% varied between 35% and 72%, as shown by echocardiography (Table 3 & Figure 1).
There were statistically insignificant differences between the extracorporeal circulation (ECC) time and aortic cross-clamp (ACC) time of in between weaned or failed-to-wean patients (Table 4).
The SOFA score was significantly greater in patients who could not be successfully weaned off ventilation than those who were weaned off (Table 5). The results demonstrated that compared to weaned off patients, those who failed to be weaned had significantly greater RR/TV ratio, minute volume, maximum inspiratory pressure, and significantly lower PaO2/ FiO2 (Table 6).
| Table 5: Comparable SOFA score between the groups | ||||
| SOFA score | Weaned (N=73) | Failed (N=7) | p-value | |
| SOFA score | Mean ± SD | 4.657 ± 1.1453 | 7.285 ± 1.112 | <0.0001 |
| Median [IQR] | 5 [2] | 8 [1] | ||
| Range | 3 - 8 | 5 -8 | ||
| Data is presented as Mean ± SD. (SOFA): Sequential Organ Failure Assessment | ||||
| Table 6: Comparison of ventilation parameters of the studied groups | |||
| Ventilation parameters | Weaned (N=73) | Failed (N=7) | P-value |
| RR/TV | 43.493 ± 14.549 | 99.143 ± 31.667 | 0.003 |
| PaO2/ FiO2 | 267.000 ± 48.875 | 183.429 ± 43.003 | 0.001 |
| Minute volume (L/min) | 11.164 ± 2.273 | 15.429 ± 2.573 | 0.004 |
| Max inspiratory pressure (cmH2O) | -27.699 ± 2.277 | -20.143 ± 2.673 | <0.0001 |
| Data is presented as Mean ± SD; RR/TV: respiratory rate to tidal volume ratio | |||
| Table 7: Predicting the result using laboratory investigations and ventilator parameters: sensitivity, specificity, and threshold value | ||||||
| Criteria | Cut off value | Area Under Curve | Sensitivity % | Specificity % | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | |||||
| RR/TV | ≥ 57 | 0.932 | 85.7% | 89% | 0.846 | 1.000 |
| MV | ≥ 13.5 | 0.883 | 85.7% | 84.9% | 0.716 | 1.000 |
| Max inspiratory pressure | ≥ -23 | 0.988 | 85.7% | 98.6% | 0.965 | 1.000 |
| SOFA | ≥ 6 | 0.933 | 85.7% | 72.6% | 0.823 | 1.000 |
| PO2 | ≥121 | 0.865 | 97.3% | 71.4% | 0.658 | 1.000 |
| PaO2/ FiO2 | ≥218 | 0.893 | 89% | 71.4% | 0.770 | 1.000 |
| MBP | ≥72 | 0.871 | 98.6% | 71.4% | 0.701 | 1.000 |
| Data presented as %; (SOFA): Sequential Organ Failure Assessment, MBP: mean blood pressure,
RR/TV: respiratory rate to tidal volume ratio |
||||||
A failed extubation can be predicted with an accuracy of 85.7% and a specificity of 84.9% when the cutoff value is 57 RR/TV, 98.6%, and 72.6%, respectively, when the cut-off value is 13.5 MV, 85.7%, and -23 MIP, and 6 SOFA score, according to the Table 7.
To forecast successful extubation, the cutoff values for PO2 are 121 or higher (97.3% sensitivity, 71.4% specificity), 218 or higher (89. % sensitivity, 71.4% specificity), and 72 or higher (98.6% sensitivity, 71.4% specificity) (Table 7).
4. DISCUSSION
The present study enrolled 80 patients aged between 30 and 73 years, with a mean age of 55.475 ± 8.732 years. The cohort consisted predominantly of males (76.3%), while females accounted for 23.8%, and 30% of participants were smokers. The average BMI was 30.807 ± 6.618, ranging from 18.6 to 45.5. Successful extubation within the first 48 hours was achieved in 91.3% of patients, whereas 8.8% experienced extubation failure. Among the latter, four required noninvasive CPAP, three needed invasive MV, one underwent tracheostomy, and one patient died. The mortality rates were notably elevated in the group that experienced failed extubation, as opposed to those who were successfully weaned from MV. Nevertheless, no statistically significant disparities were identified between these two groups in terms of age, sex, body mass index (BMI), or smoking status.
Out outcomes matching Sanson et al.,9 which included 205 patients (73% male, 27% female) with mean ages of 66.8 ± 10.0 years for males and 69.5 ± 11.3 years for females. Like our results, they found no significant differences in age or sex between weaned and failed extubation patients. Additionally, Lara et al. corroborated our observation that the group experiencing failed extubation exhibited a significantly higher mortality rate.10
Intraoperative complications were observed in 67.5% of the patients, with pacemaker wire placement being the most common at 36.25%, followed by ventricular fibrillation at 27.5% and bradycardia at 5%. The most frequently performed surgical procedure was CABG, accounting for 63.8% of cases, while MVR was performed in 16.3% of patients. Echocardiography revealed LVEF ranging from 35% to 72%, and the MBP was 85.037 ± 9.914 mmHg, with a range of 56 to 103 mmHg. Sanson et al.[9] CABG was also reported as the most frequent procedure (51%), followed by valvular lesions (26%), and it was noted that the volume of tracheal secretions was markedly elevated in the group that experienced failed extubation. Conversely, Lara et al. reported no significant difference in LVEF between patients who were successfully weaned and those who failed to wean.10
In our study, extracorporeal circulation (ECC) times ranged from 50 to 300 min (mean: 122.925 ± 44.891), and aortic cross-clamp (ACC) times ranged from 30 to 200 minutes (mean: 78.225 ± 28.236). No significant differences in ECC or ACC times were observed between weaned and failed patients, consistent with the findings of Sanson et al.9
The SOFA score in our cohort ranged from 3 to 8 (median: 5), and the FOUR score ranged from 2 to 13 (median: 13). Failed extubation patients had significantly higher SOFA scores. Blood product transfusions were administered to 90% of patients, with packed RBCs (80.1%), fresh frozen plasma (57.5%), and platelets (7.5%) being the most common. No significant differences in transfusion rates were found between weaned and failed patients. In contrast, Sanson et al. reported higher creatinine and lower albumin levels in failed extubation patients, which may be attributed to differing comorbidities.9
Lara et al. found no significant difference in PO2 levels between weaned and failed patients, whereas Yazdanian et al. observed lower preoperative PaO2 levels in reintubated patients compared to controls.10,11
ROC curve analysis revealed that specific cutoff values for RR/TV (≥ 57), MV (≥ 13.5), MIP (≥ -23), and SOFA (≥ 6.5) were predictive of extubation failure, with sensitivities ranging from 85.7% to 98.6% and specificities from 72.6% to 98.6%. For successful extubation, cutoff values for PO2 (≥ 121), PaO2/ FiO2 (≥ 218), and MBP (≥ 72) demonstrated sensitivity of 97.3%, 89%, and 98.6%, respectively, with a specificity of 71.4% for all. The analysis using binary logistic regression identified several independent factors associated with weaning failure, including a SOFA score of 6 or above, a Comorbidity Index exceeding 3, the presence of severe tracheal secretions, an RR/TV of 57 or greater, and minute ventilation of 13.5 L/min or higher.
El-Beheidy et al. indicated that the RSBI showed a significant difference between the groups that experienced successful weaning and those that failed to wean, with a cutoff value of ≥3.5 breaths/min/ml/kg predicting weaning failure with 100% sensitivity and 75% specificity.12 Totonchi et al. found that preoperative, intraoperative, and postoperative variables, including gender, blood transfusion, chronic kidney disease, chronic COPD, duration of the operation, endocarditis, inotrope dependency, postoperative bleeding, time on cardiopulmonary bypass (pump time), and type of surgery.13
5. LIMITATIONS
The study's limitations included the fact that the sample size was relatively small. The study was conducted in a single center and did not compare our findings with other local anesthetics and different doses and concentrations.
6. CONCLUSION
However, the failed extubation group exhibited significantly higher Charlson Comorbidity Index scores and a greater prevalence of COPD and CVS compared to the successfully weaned group. Conversely, MBP and the PO2/ FiO2 ratio were notably reduced in the group that experienced failed extubation. Given the results, it is reasonable to conclude that a SOFA score of 6 or higher, a Comorbidity Index more significant than 3, severe tracheal secretions, an RR/TV ratio of 57 or higher, and minute ventilation of 13.5 L/min or more are independent predictors of unsuccessful weaning from MV.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Funding
The study utilized the hospital resources only.
9. Conflict of interest
The authors declare that there was no conflict of interests.
10. Authors’ contribution
All authors took part in the study and preparation of the manuscript.
11. REFERENCES
- Alcalde RV, Guaragna JC, Bodanese LC, Castro I, Sussenbach E, Noer R, et al. A high dose of amiodarone in a short-term period reduces the incidence of postoperative atrial fibrillation and atrial flutter. Arq Bras Cardiol. 2006;87:236-40. [PubMed] DOI: 10.1590/s0066-782x2006001600002
- Lellouche F, Mancebo J, Jolliet P, Roeseler J, Schortgen F, Dojat M, et al. A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. Am J Respir Crit Care Med. 2006;174:894-900. [PubMed] DOI: 10.1164/rccm.200511-1780OC
- Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J. 2007;29:1033-56. [PubMed] DOI: 10.1183/09031936.00010206
- Nozawa E, Azeka E, Ignêz ZM, Feltrim Z, Auler Júnior JO. Factors associated with failure of weaning from long-term mechanical ventilation after cardiac surgery. Int Heart J. 2005;46:819-31. [PubMed] DOI: 10.1536/ihj.46.819
- Rady MY, Ryan T. Perioperative predictors of extubation failure and the effect on clinical outcome after cardiac surgery. Crit Care Med. 1999;27:340-7. [PubMed] DOI: 10.1097/00003246-199902000-00041
- Combes A, Luyt CE, Nieszkowska A, Trouillet JL, Gibert C, Chastre J. Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation? Crit Care Med. 2007;35:802-7. [PubMed] DOI: 10.1097/01.CCM.0000256721.60517.B1
- Nozawa E, Kobayashi E, Matsumoto ME, Feltrim MI, Carmona MJ, Auler JJ. Assessment of factors that influence weaning from long-term mechanical ventilation after cardiac surgery. Arq Bras Cardiol. 2003;80:301-10. [PubMed] DOI: 10.1590/s0066-782x2003000300006
- Sulzer CF, Chioléro R, Chassot PG, Mueller XM, Revelly JP. Adaptive support ventilation for fast tracheal extubation after cardiac surgery: a randomized controlled study. Anesthesiology. 2001;95:1339-45. [PubMed] DOI: 10.1097/00000542-200112000-00010
- Sanson G, Sartori M, Dreas L, Ciraolo R, Fabiani A. Predictors of extubation failure after open-chest cardiac surgery based on routinely collected data. The importance of a shared interprofessional clinical assessment. Eur J Cardiovasc Nurs. 2018;17:751-9. [PubMed] DOI: 10.1177/1474515118782103
- Lara TM, Hajjar LA, de Almeida JP, Fukushima JT, Barbas CS, Rodrigues AR, et al. High levels of B-type natriuretic peptide predict weaning failure from mechanical ventilation in adult patients after cardiac surgery. Clinics (Sao Paulo). 2013;68:33-8. [PubMed] DOI: 10.6061/clinics/2013(01)oa05
- Yazdanian F, Azarfarin R, Aghdaii N, Faritous SZ, Motlagh SD, Panahipour A. Cardiac variables as main predictors of endotracheal reintubation rate after cardiac surgery. J Tehran Heart Cent. 2013;8:42-7. [PubMed]
- El-Beheidy RM, Abdulrahman DA, Bayoumi SS, Hassan WAH. Prediction of weaning failure of mechanical ventilation using clinical parameters in picu. Zagazig Uni Med J. 2018;24:386-93. [FreeFullText]
- Totonchi Z, Baazm F, Chitsazan M, Seifi S, Chitsazan M. Predictors of prolonged mechanical ventilation after open heart surgery. J Cardiovasc Thorac Res. 2014;6:211-6. [PubMed] DOI: 10.15171/jcvtr.2014.014