Sara Magdy Abdelrahman Elkfafi 1, Mahmoud Abdelaziz Ahmed Ghallab 2, Hazem Mohamed Fawzy 3, Ghada Mohamed Samir 4, Reham Mustafa Hashim 5
Author affiliations:
Background & objective: Total knee arthroplasty (TKA) causes postoperative discomfort hindering recovery. Effective analgesia aids early rehabilitation and reduces falls. We compare the effectiveness of the conjunction of ACB + IPACK blocks versus GNB + IPACK blocks in providing postoperative pain relief and early recovery following TKA.
Methodology: 40 participants were randomly allocated to two comparable sets received either combined ACB by 10 mL bupivacaine 0.25% and IPACK block by 20 mL of bupivacaine 0.25% or combined GNB using a total of 15 mL bupivacaine 0.25% and IPACK block using 20 mL of bupivacaine 0.25%. Time to first rescue analgesic dose, postoperative pain using NRS, total nalbuphine consumption, and risk of falls using Timed Up and Go (TUG) test on the consecutive two days after surgery were evaluated.
Results: The GNB+IPACK group experienced a delayed time to the first rescue analgesic dose, lower total nalbuphine intake, reduced pain scores, earlier mobilization and decreased fall risk on the first and second postoperative days compared to the ACB+IPACK group with significant P-values.
Conclusion: Combined GNB + IPACK blocks provided superior analgesia, reduced opioid consumption, better motor sparing, earlier ambulation, and decreased falls compared to ACB+IPACK blocks in postoperative TKA patients.
Abbreviations: IPACK: the space between the popliteal artery and the posterior capsule of the knee
Keywords: Adductor Canal Block; Analgesia; Genicular Nerve Block; IPACK; Regional anesthesia; Total Knee Arthroplasty; Opioids
Citation: Abdelrahman Elkfafi SM, Ahmed Ghallab MA, Fawzy HM, Samir GM, Hashim RM. Combined adductor canal block and infiltration in the space between popliteal artery and posterior capsule of the knee block (IPACK) versus combined genicular nerve block and IPACK in total knee arthroplasty. Anaesth. pain intensive care 2025;29(2):261-269. DOI: 10.35975/apic.v29i2.2714
Received: July 30, 2024; Reviewed: October 26, 2024; Accepted: February 04, 2025
Total Knee Arthroplasty (TKA) ranks among the frequently conducted orthopedic surgeries, with a projected six-fold rise in TKA cases globally over the next decade due to aging populations.1 The rise in the number of TKAs performed globally has brought about a stronger focus on effective discomfort relief and quicker recuperation during the immediate postoperative period. As a result, various strategies for managing postoperative pain have emerged, with peripheral nerve blocks gaining significant popularity.2
Optimal postoperative knee pain management is essential not just for Patient's satisfaction and contentment, nevertheless for improving mobility, active recuperation and healthcare facilities release. multidimensional analgesia and motor-sparing interventions are becoming widely utilized for promoting early physical activity and enhanced agility.3 Studies have shown that using analgesic strategies like peripheral nerve blocks, achieved via local anesthetic infiltration, can enhance recuperation from surgery and physical performance, reducing the demand for opioids and other pain relievers.4
The Adductor Canal Block (ACB) promotes sensory coverage limited to the anteromedial knee,5 and significantly reduces pain and opioid usage with modest impact on quadriceps function.6 However, while ACB offers pain relief to the peripatellar and intra-articular regions of the knee, it doesn't alleviate moderate to severe posterior knee discomfort.7
There's growing interest in local anesthetic infiltration in the space between the popliteal artery and the posterior capsule of the knee (IPACK) approach.8 This technique influences the terminal branches of the genicular nerves and the popliteal plexus, innervating the knee joint's posterior capsule while preserving the core trunks of the tibial and common peroneal nerves.9 The IPACK block offers intriguing ultrasound-guided, motor-sparing hind knee discomfort relief with a low risk of neurovascular involvement.10
The Genicular Nerve Block (GNB) has lately surfaced as an innovative approach for eliminating postoperative knee discomfort in TKA, covering the anterior knee capsule, as well as the medial and superolateral knee areas.11 GNB is focused on the main innervating branches of the knee; e.g., superomedial, inferomedial, and superolateral genicular nerves,12 and it is known for its motor-sparing effect, aiding early postoperative ambulation, improving pain scores, and facilitating quicker discharge.10 With improved imaging techniques there has been an ever-increasing interest in regional techniques.
Study objectives
Current literature lacks comparisons of combined ACB and IPACK blocks versus combined GNB and IPACK blocks for analgesia in TKA. Therefore, this study aimed to compare these combinations, evaluating their effectiveness in providing superior analgesia, minimizing motor weakness, improving postoperative pain scores, enhancing ambulation, and reducing opioid consumption. The primary outcome was the assessment of time to the first rescue analgesic dose, assessed using the NRS for pain. The secondary outcomes were assessment of the net postoperative opioid (nalbuphine) intake in the first 48 hours, hemodynamic changes (MAP and HR) in the early postoperative period till 48 hours postoperatively, The time to first mobilization was reported in hours; risk of falls was assessed by using Timed Up and Go (TUG) test, duration of hospitalization, as well as the frequency of advert events and any adverse effect of nerve blocks were noted.
This randomized prospective comparative study took place at Ain Shams University Hospitals from November 2022 to November 2023, approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 285 / 2022) and registered with Pan African Clinical Trial Registry, identifier: PACTR202305870625335. Written informed consent was obtained from all participants.
Forty patients scheduled to undergo elective, unilateral primary TKA, were examined for eligibility as follows: American Society of Anaesthesiologists (ASA) physical status I–III, aged 18 - 80 years, from both sexes and with BMI ≤ 40 kg/m2. Patient refusal, patients with coagulopathy and bleeding disorders, infection at the injection site, history of established intolerance to local anesthetics, bilateral TKA or previous surgery on the same knee, chronic use of gabapentin/pregabalin, history of arrhythmia, seizures or sepsis constituted exclusion criteria
Patients were assessed preoperatively through their medical history, clinical examination, laboratory test reports; e.g., complete blood count, coagulation profile, kidney function tests, liver profile and serum electrolytes. On arrival at the operation theatre, conventional monitoring in the form of blood pressure, and pulse oximeter were connected. Intravenous access was established using an 18-gauge iv cannula.
Every patient was given midazolam 0.03 mg/kg IV, granisetron 1 mg IV and antibiotic prophylaxis according to the hospital protocol before surgery. Spinal anesthesia was conducted using 15 mg (3 mL) hyperbaric bupivacaine 0.5% in the sitting position at L3-4 or L4-5 intervertebral space by a 25 G spinal needle. The level of spinal anesthesia was assessed, then the block procedure proceeded under complete aseptic conditions.
A computer-generated random numbers table was utilized to randomly assign patients into two equal groups, with group allocation disguised in sealed opaque envelopes, each containing 20 patients as follows:
Group I received ACB + IPACK block. ACB was achieved by 10 mL bupivacaine 0.25% and IPACK block by 20 mL bupivacaine 0.25%. Group II received GNB plus IPACK block. GNB was achieved by a total of 15 mL of bupivacaine 0.25% in equal increments at multiple sites (5 mL for each genicular nerve) and IPACK block by 20 mL of bupivacaine 0.25%.
2.1. Group I (ACB+IPACK)
Following spinal anesthesia, patients were positioned supine. An ultrasound-guided ACB was conducted at the mid-thigh level, lateral to the femoral artery and deep to the sartorius muscle, with a high-frequency linear ultrasound transducer (10-12 Hz; Sono-Site Turbo; SonoSite Inc., Bothell, WA), as described by Manickam in 2009.13 Following a negative aspiration, 10 mL of bupivacaine 0.25% was injected under sterile circumstances.
Once the knee was flexed, the US transducer was mounted into the popliteal region to locate the popliteal artery, then it was shifted distally from the division of the common peroneal and tibial nerves, progressing towards the popliteal crease until the tibial nerve was visible superficial to the popliteal vessels. The transducer was then positioned at the junction of the femoral condyles with the femoral shaft. The popliteal artery, tibial and peroneal nerves were viewed and the space between the femur and popliteal artery was identified. A 20-gauge × 100 mm needle was inserted into the IPACK area with a lateral to medial in-plane approach. In sterile conditions, 20 mL of bupivacaine 0.25% was injected incrementally as the needle was gradually pulled out to the distal point of the lateral condyle of the femur. 11
2.2. Group II (GNB+IPACK)
Following spinal anesthesia, patients were positioned supine. An ultrasound-guided GNB was conducted by placing the ultrasound transducer parallel to the femur shaft and identifying the epicondyle. The superolateral, superomedial, and inferomedial genicular arteries, which follow similar routes as their respective genicular nerves, were located near the periosteal zones. A 20-gauge, 100 mm needle was placed in-plane with the ultrasound probe in the long-axis view. Following verification of the needle's tip alignment next to a genicular artery, a total of 15 mL of bupivacaine 0.25% was injected in equal increments at multiple sites around the superior lateral, superior medial, and inferior medial genicular nerves. This technique was outlined by Qudsi-Sinclair et al. in 2017.14 Next, the IPACK block was conducted. After flexing the knee, the transducer was positioned into the popliteal region, as previously described in the (ACB+IPACK) group.
2.3. Outcome assessments
After surgery, patients were evaluated immediately at 0 hour (PACU), and at 2, 4, 8, 12, 24, and 48 hours for post-operative pain using NRS and the hemodynamic parameters, e.g., HR and MAP. All patients received acetaminophen 1 gm IV every 6 hours, 4 doses) as a component of multimodal analgesia. Discomfort following surgery was measured at time of examination or at any time the patient complained of pain by using NRS. NRS > 3 was managed by administration of nalbuphine 5 mg IV as rescue analgesia, repeated till NRS score was ≤ 3 (with maximum dose of 10 mg nalbuphine at a time). Total nalbuphine consumption was recorded. Ambulation onset and side effects of nerve blocks were observed such as (allergic reactions, infections, hematomas or nerve injuries through sensory evaluation of the dermatomal distribution of the targeted nerve by assessing pain, temperature and light touch) and were reported over the initial 48 hours following surgery.
2.4. Statistical Analysis
The sample size was determined using NCSS PASS 11.0 and based on a study conducted by Et et al., 2022. Group sample sizes of 20 patients in group I and 20 patients in group II achieve 81% power to detect a difference of -48.6 between the null hypothesis that both groups means are 160.0 and the alternative hypothesis that the mean of group II is 208.6 with the estimated group standard deviations of 49.7 and 44.5 and with a significance level (alpha) of 0.05000 using a two-sided two-sample t-test. The sample size was inflated by 10.0% to account for the attrition problem in prospective studies.
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 27.0. Quantitative data are represented as mean ± SD or median (IQR) as stated. Qualitative data are presented as frequencies and percentages. The following experiments were conducted: Independent-samples t-test of significance was used to compare two means, the Chi-square (X2) test of significance to compare proportions of two qualitative parameters, and the Mann Whitney U test for two-group comparisons in non-parametric data. The confidence interval was set at 95%, and the acceptable margin of error was 5%. Thus, P < 0.05 was considered significant.
We preliminary contacted 50 individuals, however, 5 patients failed to fulfil the eligibility criteria, 2 patients sought treatment other than TKA and 3 patients disapproved to engage. Hence, 40 TKA patients were enrolled.
Demographic statistics (age, gender, ASA, and BMI) were comparable between the two groups, and no statistically significant difference was found among them (P > 0.05) as demonstrated in Table 1.
At several intervals, group hemodynamic data MAP and HR were comparable, and There were no statistically significant distinctions between them except in HR at 4 hours with P < 0.05 as shown in Table 2. This difference can be justified by the sustained pain relief impact of GNB+ IPACK blocks over the pain relief impact of ACB + IPACK blocks swiftly after surgery.
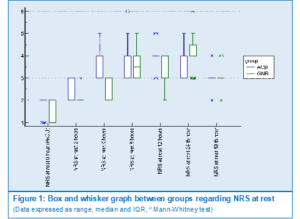
Groups were compared regarding pain evaluation using NRS at various rest intervals, and a statistically significant difference was seen among groups at 2, 4, 12, and 24 hours, however this difference was only clinically meaningful at 4 hours after surgery (Figure 1).
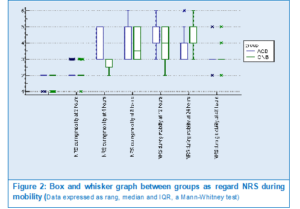
Groups were compared regarding pain assessment using NRS at several intervals during mobility and there was statistically significant difference between groups at 4 hours after surgery (Figure 2).
Both Groups were compared regarding 1st time of rescue analgesia and GNB+IPACK group showed delayed need for rescue analgesia compared to ACB+IPACK group with statistically significant difference of P < 0.001. Both sides were contrasted based on total nalbuphine consumption in the initial consecutive two days after surgery and showed higher nalbuphine consumption in ACB+IPACK group with statistically significant difference of P < 0.05 as displayed in Table 3.
The two groups were compared in terms of first mobilization time in hours and there was a statistically significant difference between them as GNB+IPACK group showed earlier onset of mobilization with P < 0.05. Also, both parties were compared concerning risk of fall using TUG test on 1st and 2nd postoperative days that showed less risk of falling in group GNB+IPACK with P < 0.05 indicating better motor sparing effect of the GNB+IPACK blocks than ACB+IPACK blocks as presented in Table 4.
Groups were compared for the duration of hospital stay in days and blocks’ complications of both groups and revealed no statistically significant distinction as illustrated in Table 5.
In the current study we assessed the pain relief efficacy of combined GNB+IPACK block compared to combined ACB+IPACK blocks in TKA in the context of time to the first rescue analgesia, total nalbuphine consumption, 1st mobilization time, risk of fall using TUG test, postoperative pain assessment using NRS score in the first two days postoperatively, length of hospital stays and complications of blocks. This randomized prospective comparative study demonstrated that GNB+IPACK group exhibited delayed need for the 1st rescue analgesic dose compared to ACB+IPACK group as well as less cumulative opioid needs. Additionally, the 1st mobilization time in GNB+IPACK group preceded that of ACB+IPACK group with decreased risk of falling in 1st and 2nd days postoperatively and reduced pain scores in the initial postoperative phase.
This study findings analysis pointed out that GNB+IPACK group displayed more substantial analgesic effectiveness and sought delayed and lesser dosages of rescue analgesia within the first 48 hours after surgery in conformity with the insights of Zeng et al. who conducted a case report of a 62-year-old female whom was scheduled for left-sided total knee arthroplasty under general anesthesia received combined GNB+IPACK blocks, reported that combining GNB with IPACK can deliver pain relief to both the front and back of the knee joint and this combination extends the duration of postoperative pain relief and supports early rehabilitation exercises for patients undergoing TKA.15
Similarly, Akesen et al. comparing GNB to IPACK in pain relief after TKR stated that IPACK and GNB have shown superiority to ACB and sciatic nerve block due to their more extensive analgesic area coverage and minimal motor nerve involvement and that ACB only provides pain relief to the anterior and medial parts of the knee joint, failing to address posterior pain.16 Additionally, both ACB and sciatic nerve blocks negatively impact muscle functions as they involve the motor branches of the tibial and peroneal nerves, hence, impairing mobility.
Moreover, a study by Dundar et al. that compared GNB to IPACK in primary TKA concluded that both GNB and IPACK blocks had a considerably favorable effect on postoperative pain levels within the first day after TKA.17 Compared to IPACK, GNB reduced opioid intake swiftly after surgery as well as encouraging improved mobility. This is consistent with our findings that the combined GNB+IPACK group provided better motor sparing effect, decreased risk of falling and lesser nalbuphine consumption compared to combined ACB+IPACK.
This study showed also the need for higher nalbuphine consumption in ACB+IPACK group than GNB+IPACK group, having statistically significant difference of P < 0.05. Those findings were consistent with Elliot et al, as their study showed that ACB+IPACK group did not have lower Visual Analogue Score (VAS) compared to the (femoral nerve block) FNB+IPACK group, and that ACB+IPACK group displayed slightly higher opioid needs and intake.18 Nonetheless, during the first 48 hours after surgery, ACB+IPACK group showed significantly longer walking distances and a greater hospital release frequency.
Our results align with Kukreja et al., in a study contrasted the combination of GNB to ACB in TKA versus ACB alone, this combination led to improved pain scores and reduced opioid intake during the early recovery stage, which in turn enhanced mobility.19 Also, patients who received genicular nerve blocks demonstrated a significantly greater ambulation distance on the first day following surgery. Kukreja et al. stated that for primary TKA patients, the average oral morphine equivalents intake was decreased across all documented times in the trial with the six- to twelve-hour period showing a trend towards significance and this short-term advantage of adding GNB can be attributed to factors such as the low volume of local anesthetic (LA) used, the injection site, anatomical variance, block approach, uneven spread of LA, or the dispersion of LA upon surgical incision and tissue axis disruption.
Another study by Tayfun et al., IPACK and periarticular block were compared to ACB alone after TKA, found no significant difference in TUG test and range of motion between IPACK and periarticular block groups. Both blocks pursue the genicular branches of the knee, without impacting the quadriceps or calf muscles.20
Contrary to the current study, Sujatha et al. conducted a study to compare the analgesic effectiveness of ultrasound guided GNB with ACB in patients undergoing arthroscopic anterior cruciate ligament restoration (ACLR).21 The study included 38 adults undergoing arthroscopic ACLR, with 19 patients in GNB group receiving US-guided GNB and 19 patients in ACB group receiving US-guided ACB. The results concluded that US-guided GNB has analgesic benefits equivalent to US-guided ACB for patients having arthroscopic ACLR, as both groups had similar NRS ratings and postoperative opioid requirements. Sujatha et al. also stated that although the average time required for initial rescue analgesia was longer in GNB group compared to ACB group, this difference was statistically insignificant. The study's findings show that neither ACB nor GNB can deliver effective pain relief to knee joints. This contrast to our results could be attributed to the different types of operations between the two studies as TKA involves two main components: an upper part that replaces the end of the femur and a lower portion that replaces the end of the tibia. Surgeons make a large incision to access the entire joint, while most ACL surgery uses a minimally invasive approach, with very small incisions. Hence TKA involves more tissue destruction.
A network meta-analysis of 30 RCT on different nerve blocks for patients underwent TKA by Wang et al. stated that to accomplish complete and optimal postoperative pain control IPACK is frequently employed with other peripheral nerve block techniques such as ACB, GNB, and ONB (obturator nerve block), among others.22 This coupled technique guarantees complete pain relief benefits across the whole knee joint region. By utilizing these mergers, this approach can lead to more efficient postoperative pain relief, encourages earlier rehabilitation exercises, reduces opioid consumption, reduces the likelihood of complications following surgery, and ultimately enhances the overall recuperation quality and patient contentment. It also concluded that continuous nerve blocks extended analgesic advantages, lowering postoperative pain threshold and facilitating early rehabilitation attempts. Therefore, they should be prioritized over single shot blocks whenever applicable. Continuous peripheral nerve blocks may be preferred to single-shot blocks in patients undergoing TKA based on results related to postoperative pain, function, adverse events, oral morphine equivalents, and perioperative indicators.
In the current study, both groups were evaluated in terms of the duration of hospital stay and block complications, and no statistically significant difference was found. No complications were reported in either group within the first 48 hours after surgery. However, a study by Chan et al. reported foot drop in two out of 411 participants who underwent an IPACK block at 30 min and 2 hours. 23 Zheng et al., comparing (Femoral-sciatic nerve blocks) FNB-SNB with ACB-IPACK, reported that 6.6% of patients in the IPACK group had foot drop which contrasts with our findings where no block complications were spotted between the two groups after 48 hours. 24 Kampitak et al., when comparing Continuous Adductor Canal Block (CACB) in combination with local anesthetic infiltration (LAI) and IPACK or tibial nerve block (TNB), also revealed that common peroneal nerve (CPN) involvement caused foot drop and a greater likelihood of tripping. 25
First, the sample size was quite small. Second, single-shot blocks offered just a short period of analgesia, with smaller volumes leading to rebound pain after 8-10 hours. Third, the study made no distinction between varus and valgus knees, rendering it challenging to analyze postoperative clinical outcomes in both scenarios individually.
Further randomized controlled research trials are necessary to assess and juxtapose the pain relief effects of GNB, ACB, and femoral triangle block in combination with the IPACK block for TKA. Moreover, further investigation into the ideal dosage and concentration of local anesthetics is essential to offer credible guidelines.
Combined GNB + IPACK blocks offered superior analgesia during the early postoperative period, reduced overall opioid consumption, and provided better motor sparing. This allowed for earlier ambulation and a reduced risk of falling in postoperative TKA patients compared to the combined adductor canal block + IPACK blocks.
8. Data availability
The numerical data generated during this research is available with the authors.
9. Conflict of interest
The authors declare that there are no conflicts of interest
10. Ethical issues
The participants and their caregivers (if any) were provided with written and verbal information about the purpose and content of the study. After agreeing to participate in the study, they were asked to sign a registration form for confirmation. All the information regarding the research subjects was confidential
The study was approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 285 / 2022) and registered with Pan African Clinical Trial Registry, identifier: PACTR202305870625335. The procedures used in this study adhered to the tenets of the Declaration of Helsinki.
11. Authors’ contribution
SAME: Conduction of the study work.
MAAG: Manuscript editing.
HMF, RMH: Literature search.
GMS: Statistical analysis and review.
Author affiliations:
- Sara Magdy Abdelrahman Elkfafi, Assistant Lecturer, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams, University, Cairo, Egypt; Email: Saraelkafafi@med.asu.edu.eg, {ORCID:0009-0004-4512-3853}
- Mahmoud Abdelaziz Ahmed Ghallab, Professor, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams, University, Cairo, Egypt; Email: mghallab62@gmail.com
- Hazem Mohamed Fawzy, Professor, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams, University, Cairo, Egypt; Email: hazemmfawzi@yahoo.com
- Ghada Mohamed Samir, Professor, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams, University, Cairo, Egypt; Email: ghada.samir@med.asu.edu.eg, {ORCID:0000-0001-6136-9846}
- Reham Mustafa Hashim, Associate Professor, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams, University, Cairo, Egypt; Email: Dr_reham80@yahoo.com, {ORCID:0000-0003-2423-0014
ABSTRACT
Background & objective: Total knee arthroplasty (TKA) causes postoperative discomfort hindering recovery. Effective analgesia aids early rehabilitation and reduces falls. We compare the effectiveness of the conjunction of ACB + IPACK blocks versus GNB + IPACK blocks in providing postoperative pain relief and early recovery following TKA.
Methodology: 40 participants were randomly allocated to two comparable sets received either combined ACB by 10 mL bupivacaine 0.25% and IPACK block by 20 mL of bupivacaine 0.25% or combined GNB using a total of 15 mL bupivacaine 0.25% and IPACK block using 20 mL of bupivacaine 0.25%. Time to first rescue analgesic dose, postoperative pain using NRS, total nalbuphine consumption, and risk of falls using Timed Up and Go (TUG) test on the consecutive two days after surgery were evaluated.
Results: The GNB+IPACK group experienced a delayed time to the first rescue analgesic dose, lower total nalbuphine intake, reduced pain scores, earlier mobilization and decreased fall risk on the first and second postoperative days compared to the ACB+IPACK group with significant P-values.
Conclusion: Combined GNB + IPACK blocks provided superior analgesia, reduced opioid consumption, better motor sparing, earlier ambulation, and decreased falls compared to ACB+IPACK blocks in postoperative TKA patients.
Abbreviations: IPACK: the space between the popliteal artery and the posterior capsule of the knee
Keywords: Adductor Canal Block; Analgesia; Genicular Nerve Block; IPACK; Regional anesthesia; Total Knee Arthroplasty; Opioids
Citation: Abdelrahman Elkfafi SM, Ahmed Ghallab MA, Fawzy HM, Samir GM, Hashim RM. Combined adductor canal block and infiltration in the space between popliteal artery and posterior capsule of the knee block (IPACK) versus combined genicular nerve block and IPACK in total knee arthroplasty. Anaesth. pain intensive care 2025;29(2):261-269. DOI: 10.35975/apic.v29i2.2714
Received: July 30, 2024; Reviewed: October 26, 2024; Accepted: February 04, 2025
1. INTRODUCTION
Total Knee Arthroplasty (TKA) ranks among the frequently conducted orthopedic surgeries, with a projected six-fold rise in TKA cases globally over the next decade due to aging populations.1 The rise in the number of TKAs performed globally has brought about a stronger focus on effective discomfort relief and quicker recuperation during the immediate postoperative period. As a result, various strategies for managing postoperative pain have emerged, with peripheral nerve blocks gaining significant popularity.2
Optimal postoperative knee pain management is essential not just for Patient's satisfaction and contentment, nevertheless for improving mobility, active recuperation and healthcare facilities release. multidimensional analgesia and motor-sparing interventions are becoming widely utilized for promoting early physical activity and enhanced agility.3 Studies have shown that using analgesic strategies like peripheral nerve blocks, achieved via local anesthetic infiltration, can enhance recuperation from surgery and physical performance, reducing the demand for opioids and other pain relievers.4
The Adductor Canal Block (ACB) promotes sensory coverage limited to the anteromedial knee,5 and significantly reduces pain and opioid usage with modest impact on quadriceps function.6 However, while ACB offers pain relief to the peripatellar and intra-articular regions of the knee, it doesn't alleviate moderate to severe posterior knee discomfort.7
There's growing interest in local anesthetic infiltration in the space between the popliteal artery and the posterior capsule of the knee (IPACK) approach.8 This technique influences the terminal branches of the genicular nerves and the popliteal plexus, innervating the knee joint's posterior capsule while preserving the core trunks of the tibial and common peroneal nerves.9 The IPACK block offers intriguing ultrasound-guided, motor-sparing hind knee discomfort relief with a low risk of neurovascular involvement.10
The Genicular Nerve Block (GNB) has lately surfaced as an innovative approach for eliminating postoperative knee discomfort in TKA, covering the anterior knee capsule, as well as the medial and superolateral knee areas.11 GNB is focused on the main innervating branches of the knee; e.g., superomedial, inferomedial, and superolateral genicular nerves,12 and it is known for its motor-sparing effect, aiding early postoperative ambulation, improving pain scores, and facilitating quicker discharge.10 With improved imaging techniques there has been an ever-increasing interest in regional techniques.
Study objectives
Current literature lacks comparisons of combined ACB and IPACK blocks versus combined GNB and IPACK blocks for analgesia in TKA. Therefore, this study aimed to compare these combinations, evaluating their effectiveness in providing superior analgesia, minimizing motor weakness, improving postoperative pain scores, enhancing ambulation, and reducing opioid consumption. The primary outcome was the assessment of time to the first rescue analgesic dose, assessed using the NRS for pain. The secondary outcomes were assessment of the net postoperative opioid (nalbuphine) intake in the first 48 hours, hemodynamic changes (MAP and HR) in the early postoperative period till 48 hours postoperatively, The time to first mobilization was reported in hours; risk of falls was assessed by using Timed Up and Go (TUG) test, duration of hospitalization, as well as the frequency of advert events and any adverse effect of nerve blocks were noted.
2. METHODOLOGY
This randomized prospective comparative study took place at Ain Shams University Hospitals from November 2022 to November 2023, approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 285 / 2022) and registered with Pan African Clinical Trial Registry, identifier: PACTR202305870625335. Written informed consent was obtained from all participants.
Forty patients scheduled to undergo elective, unilateral primary TKA, were examined for eligibility as follows: American Society of Anaesthesiologists (ASA) physical status I–III, aged 18 - 80 years, from both sexes and with BMI ≤ 40 kg/m2. Patient refusal, patients with coagulopathy and bleeding disorders, infection at the injection site, history of established intolerance to local anesthetics, bilateral TKA or previous surgery on the same knee, chronic use of gabapentin/pregabalin, history of arrhythmia, seizures or sepsis constituted exclusion criteria
Patients were assessed preoperatively through their medical history, clinical examination, laboratory test reports; e.g., complete blood count, coagulation profile, kidney function tests, liver profile and serum electrolytes. On arrival at the operation theatre, conventional monitoring in the form of blood pressure, and pulse oximeter were connected. Intravenous access was established using an 18-gauge iv cannula.
Every patient was given midazolam 0.03 mg/kg IV, granisetron 1 mg IV and antibiotic prophylaxis according to the hospital protocol before surgery. Spinal anesthesia was conducted using 15 mg (3 mL) hyperbaric bupivacaine 0.5% in the sitting position at L3-4 or L4-5 intervertebral space by a 25 G spinal needle. The level of spinal anesthesia was assessed, then the block procedure proceeded under complete aseptic conditions.
A computer-generated random numbers table was utilized to randomly assign patients into two equal groups, with group allocation disguised in sealed opaque envelopes, each containing 20 patients as follows:
Group I received ACB + IPACK block. ACB was achieved by 10 mL bupivacaine 0.25% and IPACK block by 20 mL bupivacaine 0.25%. Group II received GNB plus IPACK block. GNB was achieved by a total of 15 mL of bupivacaine 0.25% in equal increments at multiple sites (5 mL for each genicular nerve) and IPACK block by 20 mL of bupivacaine 0.25%.
2.1. Group I (ACB+IPACK)
Following spinal anesthesia, patients were positioned supine. An ultrasound-guided ACB was conducted at the mid-thigh level, lateral to the femoral artery and deep to the sartorius muscle, with a high-frequency linear ultrasound transducer (10-12 Hz; Sono-Site Turbo; SonoSite Inc., Bothell, WA), as described by Manickam in 2009.13 Following a negative aspiration, 10 mL of bupivacaine 0.25% was injected under sterile circumstances.
Once the knee was flexed, the US transducer was mounted into the popliteal region to locate the popliteal artery, then it was shifted distally from the division of the common peroneal and tibial nerves, progressing towards the popliteal crease until the tibial nerve was visible superficial to the popliteal vessels. The transducer was then positioned at the junction of the femoral condyles with the femoral shaft. The popliteal artery, tibial and peroneal nerves were viewed and the space between the femur and popliteal artery was identified. A 20-gauge × 100 mm needle was inserted into the IPACK area with a lateral to medial in-plane approach. In sterile conditions, 20 mL of bupivacaine 0.25% was injected incrementally as the needle was gradually pulled out to the distal point of the lateral condyle of the femur. 11
2.2. Group II (GNB+IPACK)
Following spinal anesthesia, patients were positioned supine. An ultrasound-guided GNB was conducted by placing the ultrasound transducer parallel to the femur shaft and identifying the epicondyle. The superolateral, superomedial, and inferomedial genicular arteries, which follow similar routes as their respective genicular nerves, were located near the periosteal zones. A 20-gauge, 100 mm needle was placed in-plane with the ultrasound probe in the long-axis view. Following verification of the needle's tip alignment next to a genicular artery, a total of 15 mL of bupivacaine 0.25% was injected in equal increments at multiple sites around the superior lateral, superior medial, and inferior medial genicular nerves. This technique was outlined by Qudsi-Sinclair et al. in 2017.14 Next, the IPACK block was conducted. After flexing the knee, the transducer was positioned into the popliteal region, as previously described in the (ACB+IPACK) group.
2.3. Outcome assessments
After surgery, patients were evaluated immediately at 0 hour (PACU), and at 2, 4, 8, 12, 24, and 48 hours for post-operative pain using NRS and the hemodynamic parameters, e.g., HR and MAP. All patients received acetaminophen 1 gm IV every 6 hours, 4 doses) as a component of multimodal analgesia. Discomfort following surgery was measured at time of examination or at any time the patient complained of pain by using NRS. NRS > 3 was managed by administration of nalbuphine 5 mg IV as rescue analgesia, repeated till NRS score was ≤ 3 (with maximum dose of 10 mg nalbuphine at a time). Total nalbuphine consumption was recorded. Ambulation onset and side effects of nerve blocks were observed such as (allergic reactions, infections, hematomas or nerve injuries through sensory evaluation of the dermatomal distribution of the targeted nerve by assessing pain, temperature and light touch) and were reported over the initial 48 hours following surgery.
2.4. Statistical Analysis
The sample size was determined using NCSS PASS 11.0 and based on a study conducted by Et et al., 2022. Group sample sizes of 20 patients in group I and 20 patients in group II achieve 81% power to detect a difference of -48.6 between the null hypothesis that both groups means are 160.0 and the alternative hypothesis that the mean of group II is 208.6 with the estimated group standard deviations of 49.7 and 44.5 and with a significance level (alpha) of 0.05000 using a two-sided two-sample t-test. The sample size was inflated by 10.0% to account for the attrition problem in prospective studies.
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 27.0. Quantitative data are represented as mean ± SD or median (IQR) as stated. Qualitative data are presented as frequencies and percentages. The following experiments were conducted: Independent-samples t-test of significance was used to compare two means, the Chi-square (X2) test of significance to compare proportions of two qualitative parameters, and the Mann Whitney U test for two-group comparisons in non-parametric data. The confidence interval was set at 95%, and the acceptable margin of error was 5%. Thus, P < 0.05 was considered significant.
| Table 1: Comparing groups based on demographic data. | ||||
| Parameter | Group ACB+IPACK
(n=20) |
Group GNB+IPACK
(n=20) |
P-value | |
| Age (years) | 59.4 ± 16.5 | 63.85 ± 14.3 | 0.368 t | |
| BMI | 28.35 ± 4.3 | 28.45 ± 3.9 | 0.939 t | |
| Gender | Male | 11 (55) 9 (45) |
11 (55) 9 (45) |
1 x2 |
| Female | ||||
| ASA | I | 9 (45) 9 (45) 2 (10) |
10 (50) 10 (50) 0 (0) |
0.349 x2 |
| II | ||||
| III | ||||
| Data expressed as mean ± SD, or n (%); t = student t test, X2 = chi square | ||||
3. RESULTS
We preliminary contacted 50 individuals, however, 5 patients failed to fulfil the eligibility criteria, 2 patients sought treatment other than TKA and 3 patients disapproved to engage. Hence, 40 TKA patients were enrolled.
Demographic statistics (age, gender, ASA, and BMI) were comparable between the two groups, and no statistically significant difference was found among them (P > 0.05) as demonstrated in Table 1.
| Table (2): Comparison of groups' postoperative hemodynamic data. | ||||
| Parameter | Time | Group ACB+IPACK
(n=20) |
Group GNB+IPACK
(n=20) |
P-value t |
| MAP | Baseline | 86.9 ± 9.0 | 87.95 ± 10.2 | 0.7314 |
| 0 hours (PACU) | 83.9 ± 7.7 | 83.65 ± 6.9 | 0.9143 | |
| 2 hours | 84.4 ± 7.3 | 85.05 ± 6.1 | 0.7608 | |
| 4 hours | 91.5 ± 9.2 | 86.9 ± 4.9 | 0.0553 | |
| 8 hours | 95.65 ± 11.0 | 98.4 ± 9.9 | 0.4118 | |
| 12 hours | 99.25 ± 7.8 | 97.65 ± 10.4 | 0.5857 | |
| 24 hours | 89.3 ± 9.3 | 92.75 ± 7.2 | 0.1968 | |
| 48 hours | 87.65 ± 8.4 | 89.7 ± 7.8 | 0.4286 | |
| HR | Baseline | 75.5 ± 3.9 | 77.15 ± 4.8 | 0.2436 |
| 0 hours (PACU) | 71.45 ± 3.5 | 71.6 ± 5.0 | 0.9129 | |
| 2 hours | 73.8 ± 4.0 | 73.2 ± 5.3 | 0.691 | |
| 4 hours | 81.45 ± 5.7 | 75.3 ± 3.7 | 0.0003 | |
| 8 hours | 84.05 ± 4.8 | 85 ± 4.8 | 0.5364 | |
| 12 hours | 87.05 ± 4.9 | 85.55 ± 6.1 | 0.396 | |
| 24 hours | 85.65 ± 5.8 | 87.65 ± 5.9 | 0.2869 | |
| 48 hours | 79.4 ± 4.6 | 78.35 ± 5.4 | 0.5131 | |
| Data expressed as mean ± SD, t = student t test; P < 0.05 considered as significant | ||||
At several intervals, group hemodynamic data MAP and HR were comparable, and There were no statistically significant distinctions between them except in HR at 4 hours with P < 0.05 as shown in Table 2. This difference can be justified by the sustained pain relief impact of GNB+ IPACK blocks over the pain relief impact of ACB + IPACK blocks swiftly after surgery.
Groups were compared regarding pain evaluation using NRS at various rest intervals, and a statistically significant difference was seen among groups at 2, 4, 12, and 24 hours, however this difference was only clinically meaningful at 4 hours after surgery (Figure 1).
Groups were compared regarding pain assessment using NRS at several intervals during mobility and there was statistically significant difference between groups at 4 hours after surgery (Figure 2).
Both Groups were compared regarding 1st time of rescue analgesia and GNB+IPACK group showed delayed need for rescue analgesia compared to ACB+IPACK group with statistically significant difference of P < 0.001. Both sides were contrasted based on total nalbuphine consumption in the initial consecutive two days after surgery and showed higher nalbuphine consumption in ACB+IPACK group with statistically significant difference of P < 0.05 as displayed in Table 3.
The two groups were compared in terms of first mobilization time in hours and there was a statistically significant difference between them as GNB+IPACK group showed earlier onset of mobilization with P < 0.05. Also, both parties were compared concerning risk of fall using TUG test on 1st and 2nd postoperative days that showed less risk of falling in group GNB+IPACK with P < 0.05 indicating better motor sparing effect of the GNB+IPACK blocks than ACB+IPACK blocks as presented in Table 4.
| Table 3: Comparison of groups based on the first time of rescue analgesia and total Nalbuphine dosage | |||
| Variable | Group ACB+IPACK
(n=20) |
Group GNB+IPACK
(n=20) |
P-value |
| Time to rescue analgesia (min) | 312 ± 69.1 | 534 ± 84.6 | <0.001 t |
| Total nalbuphine used as rescue analgesia (mg) | 11.95 ± 3.9 | 8.6 ± 2.3 | 0.002 t |
| Data expressed as mean ± SD, or n (%); t = student t test, X2 = chi square; P < 0.05 considered as significant | |||
| Table 4: Comparison of groups for first mobilization time in hours and TUG test on the first and second postoperative days | |||
| Variable | Group ACB+IPACK (n=20) | Group GNB+IPACK
(n=20) |
P-value t |
| First mobilization (hours) | 14.85 ± 3.3 | 11.4 ± 2.2 | 0.0004 |
| TUG 1st Day (sec) | 13.55 ± 3.0 | 10.2 ± 0.8 | <0.001 |
| TUG 2nd Day (sec) | 9.1 ± 1.4 | 8.3 ± 0.9 | 0.04 |
| Data expressed as mean ± SD, t = student t test; P < 0.05 considered as significant | |||
| Table 5: Comparison across groups in terms of hospital stay and complications | |||||||
| Variable | Group ACB +IPACK | Group GNB+IPACK |
P-value a |
||||
| Range | Median | IQR | Range | Median | IQR | ||
| Hospital Stay (Days) | 2−3 | 2 | 2−3 | 2−3 | 2 | 2−2.5 | 0.496 |
| Complications | No complications were detected from the blocks | ||||||
| Data expressed as rang, median and IQR, a Mann−Whitney test; P < 0.05 considered as significant | |||||||
Groups were compared for the duration of hospital stay in days and blocks’ complications of both groups and revealed no statistically significant distinction as illustrated in Table 5.
4. DISCUSSION
In the current study we assessed the pain relief efficacy of combined GNB+IPACK block compared to combined ACB+IPACK blocks in TKA in the context of time to the first rescue analgesia, total nalbuphine consumption, 1st mobilization time, risk of fall using TUG test, postoperative pain assessment using NRS score in the first two days postoperatively, length of hospital stays and complications of blocks. This randomized prospective comparative study demonstrated that GNB+IPACK group exhibited delayed need for the 1st rescue analgesic dose compared to ACB+IPACK group as well as less cumulative opioid needs. Additionally, the 1st mobilization time in GNB+IPACK group preceded that of ACB+IPACK group with decreased risk of falling in 1st and 2nd days postoperatively and reduced pain scores in the initial postoperative phase.
This study findings analysis pointed out that GNB+IPACK group displayed more substantial analgesic effectiveness and sought delayed and lesser dosages of rescue analgesia within the first 48 hours after surgery in conformity with the insights of Zeng et al. who conducted a case report of a 62-year-old female whom was scheduled for left-sided total knee arthroplasty under general anesthesia received combined GNB+IPACK blocks, reported that combining GNB with IPACK can deliver pain relief to both the front and back of the knee joint and this combination extends the duration of postoperative pain relief and supports early rehabilitation exercises for patients undergoing TKA.15
Similarly, Akesen et al. comparing GNB to IPACK in pain relief after TKR stated that IPACK and GNB have shown superiority to ACB and sciatic nerve block due to their more extensive analgesic area coverage and minimal motor nerve involvement and that ACB only provides pain relief to the anterior and medial parts of the knee joint, failing to address posterior pain.16 Additionally, both ACB and sciatic nerve blocks negatively impact muscle functions as they involve the motor branches of the tibial and peroneal nerves, hence, impairing mobility.
Moreover, a study by Dundar et al. that compared GNB to IPACK in primary TKA concluded that both GNB and IPACK blocks had a considerably favorable effect on postoperative pain levels within the first day after TKA.17 Compared to IPACK, GNB reduced opioid intake swiftly after surgery as well as encouraging improved mobility. This is consistent with our findings that the combined GNB+IPACK group provided better motor sparing effect, decreased risk of falling and lesser nalbuphine consumption compared to combined ACB+IPACK.
This study showed also the need for higher nalbuphine consumption in ACB+IPACK group than GNB+IPACK group, having statistically significant difference of P < 0.05. Those findings were consistent with Elliot et al, as their study showed that ACB+IPACK group did not have lower Visual Analogue Score (VAS) compared to the (femoral nerve block) FNB+IPACK group, and that ACB+IPACK group displayed slightly higher opioid needs and intake.18 Nonetheless, during the first 48 hours after surgery, ACB+IPACK group showed significantly longer walking distances and a greater hospital release frequency.
Our results align with Kukreja et al., in a study contrasted the combination of GNB to ACB in TKA versus ACB alone, this combination led to improved pain scores and reduced opioid intake during the early recovery stage, which in turn enhanced mobility.19 Also, patients who received genicular nerve blocks demonstrated a significantly greater ambulation distance on the first day following surgery. Kukreja et al. stated that for primary TKA patients, the average oral morphine equivalents intake was decreased across all documented times in the trial with the six- to twelve-hour period showing a trend towards significance and this short-term advantage of adding GNB can be attributed to factors such as the low volume of local anesthetic (LA) used, the injection site, anatomical variance, block approach, uneven spread of LA, or the dispersion of LA upon surgical incision and tissue axis disruption.
Another study by Tayfun et al., IPACK and periarticular block were compared to ACB alone after TKA, found no significant difference in TUG test and range of motion between IPACK and periarticular block groups. Both blocks pursue the genicular branches of the knee, without impacting the quadriceps or calf muscles.20
Contrary to the current study, Sujatha et al. conducted a study to compare the analgesic effectiveness of ultrasound guided GNB with ACB in patients undergoing arthroscopic anterior cruciate ligament restoration (ACLR).21 The study included 38 adults undergoing arthroscopic ACLR, with 19 patients in GNB group receiving US-guided GNB and 19 patients in ACB group receiving US-guided ACB. The results concluded that US-guided GNB has analgesic benefits equivalent to US-guided ACB for patients having arthroscopic ACLR, as both groups had similar NRS ratings and postoperative opioid requirements. Sujatha et al. also stated that although the average time required for initial rescue analgesia was longer in GNB group compared to ACB group, this difference was statistically insignificant. The study's findings show that neither ACB nor GNB can deliver effective pain relief to knee joints. This contrast to our results could be attributed to the different types of operations between the two studies as TKA involves two main components: an upper part that replaces the end of the femur and a lower portion that replaces the end of the tibia. Surgeons make a large incision to access the entire joint, while most ACL surgery uses a minimally invasive approach, with very small incisions. Hence TKA involves more tissue destruction.
A network meta-analysis of 30 RCT on different nerve blocks for patients underwent TKA by Wang et al. stated that to accomplish complete and optimal postoperative pain control IPACK is frequently employed with other peripheral nerve block techniques such as ACB, GNB, and ONB (obturator nerve block), among others.22 This coupled technique guarantees complete pain relief benefits across the whole knee joint region. By utilizing these mergers, this approach can lead to more efficient postoperative pain relief, encourages earlier rehabilitation exercises, reduces opioid consumption, reduces the likelihood of complications following surgery, and ultimately enhances the overall recuperation quality and patient contentment. It also concluded that continuous nerve blocks extended analgesic advantages, lowering postoperative pain threshold and facilitating early rehabilitation attempts. Therefore, they should be prioritized over single shot blocks whenever applicable. Continuous peripheral nerve blocks may be preferred to single-shot blocks in patients undergoing TKA based on results related to postoperative pain, function, adverse events, oral morphine equivalents, and perioperative indicators.
In the current study, both groups were evaluated in terms of the duration of hospital stay and block complications, and no statistically significant difference was found. No complications were reported in either group within the first 48 hours after surgery. However, a study by Chan et al. reported foot drop in two out of 411 participants who underwent an IPACK block at 30 min and 2 hours. 23 Zheng et al., comparing (Femoral-sciatic nerve blocks) FNB-SNB with ACB-IPACK, reported that 6.6% of patients in the IPACK group had foot drop which contrasts with our findings where no block complications were spotted between the two groups after 48 hours. 24 Kampitak et al., when comparing Continuous Adductor Canal Block (CACB) in combination with local anesthetic infiltration (LAI) and IPACK or tibial nerve block (TNB), also revealed that common peroneal nerve (CPN) involvement caused foot drop and a greater likelihood of tripping. 25
5. LIMITATIONS
First, the sample size was quite small. Second, single-shot blocks offered just a short period of analgesia, with smaller volumes leading to rebound pain after 8-10 hours. Third, the study made no distinction between varus and valgus knees, rendering it challenging to analyze postoperative clinical outcomes in both scenarios individually.
6. Future scope
Further randomized controlled research trials are necessary to assess and juxtapose the pain relief effects of GNB, ACB, and femoral triangle block in combination with the IPACK block for TKA. Moreover, further investigation into the ideal dosage and concentration of local anesthetics is essential to offer credible guidelines.
7. CONCLUSION
Combined GNB + IPACK blocks offered superior analgesia during the early postoperative period, reduced overall opioid consumption, and provided better motor sparing. This allowed for earlier ambulation and a reduced risk of falling in postoperative TKA patients compared to the combined adductor canal block + IPACK blocks.
8. Data availability
The numerical data generated during this research is available with the authors.
9. Conflict of interest
The authors declare that there are no conflicts of interest
10. Ethical issues
The participants and their caregivers (if any) were provided with written and verbal information about the purpose and content of the study. After agreeing to participate in the study, they were asked to sign a registration form for confirmation. All the information regarding the research subjects was confidential
The study was approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 285 / 2022) and registered with Pan African Clinical Trial Registry, identifier: PACTR202305870625335. The procedures used in this study adhered to the tenets of the Declaration of Helsinki.
11. Authors’ contribution
SAME: Conduction of the study work.
MAAG: Manuscript editing.
HMF, RMH: Literature search.
GMS: Statistical analysis and review.
12. REFERENCES
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg. 2007;89(4):780–5. [PubMed] DOI: 2106/JBJS.F.00222
- Sankineani SR, Reddy ARC, Eachempati KK, Jangale A, Reddy AV. Comparison of adductor canal block and IPACK block with adductor canal block alone after total knee arthroplasty: a prospective control trial. Eur J Orthop Surg Traumatol. 2018;28(7):1391–5. [PubMed] DOI: 1007/s00590-018-2218-7
- Kopp SL, Børglum J, Buvanendran A, Horlocker TT, Ilfeld BM, Memtsoudis SG, et al. Anesthesia and analgesia practice pathway options for total knee arthroplasty: an evidence-based review. Reg Anesth Pain Med. 2017;42:683–97. [PubMed] DOI: 1097/AAP.0000000000000673
- Morales-Avalos R, Davila-Amar D, Martinez-Avila EC, González JE. Update on post-operative analgesia in total knee replacement. J Anesth Surg Care. 2019;1. [FreeFullText]
- Kuang MJ, Ma JX, Fu L, He WW, Zhao J, Ma XL. Is adductor canal block better than femoral nerve block in primary total knee arthroplasty? A systematic review and meta-analysis. J Arthroplasty. 2017;32:3238–48.e3. [PubMed] DOI: 1016/j.arth.2017.05.015
- Li D, Yang Z, Xie X, Zhao J, Kang P. Adductor canal block provides better performance after total knee arthroplasty compared with femoral nerve block: a systematic review and meta-analysis. Int Orthop. 2016;40:925–33. [PubMed] DOI: 1007/s00264-015-2998-x
- Laoruengthana A, Rattanaprichavej P, Rasamimongkol S, Galassi M. Anterior vs posterior periarticular multimodal drug injections: a randomized controlled trial in simultaneous bilateral total knee arthroplasty. J Arthroplasty. 2017;32(7):2100–4. [PubMed] DOI: 1016/j.arth.2017.02.033
- Govender-Davies S, Davies L, Pillay-Addinall S. A cadaveric study investigating the spread of injectate following an IPACK block in a neonatal sample: a pilot study. Anat Cell Biol. 2024;57(2):229–37. [PubMed] DOI: 5115/acb.23.274
- Tran J, Giron Arango L, Peng P, Sinha SK, Agur A, Chan V. Evaluation of the iPACK block injectate spread: a cadaveric study. Reg Anesth Pain Med. 2019;44(7):689–94. [PubMed] DOI: 1136/rapm-2018-100355
- Kandarian B, Indelli PF, Sinha S, Hunter OO, Wang RR, Kim TE, et al. Implementation of the IPACK block into a multimodal analgesic pathway for total knee replacement. Korean J Anesthesiol. 2019;72(3):238–44. [PubMed] DOI: 4097/kja.d.18.00346
- Kim DH, Beathe JC, Lin Y, YaDeau JT, Maalouf DB, Goytizolo E, et al. Addition of IPACK and adductor canal block to periarticular injection enhances postoperative pain control in total knee arthroplasty. Anesth Analg. 2019;129(2):526–35. [PubMed] DOI: 1213/ANE.0000000000003794
- Kesikburun S, Merkezi R, Yasar E, Kılıç C, Güzelküçük Ü, Yazar F, et al. Cadaveric study accuracy of ultrasound-guided genicular nerve block. Pain Physician. 2015;18(5):E899-904.. [PubMed]
- Manickam B, Perlas A, Duggan E, Brull R, Chan VW, Ramlogan R. Feasibility and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. Reg Anesth Pain Med. 2009;34(6):578–80. [PubMed] DOI: 1097/aap.0b013e3181bfbf84
- Qudsi-Sinclair S, Borrás-Rubio E, Abellan-Guillén JF, Padilla del Rey ML, Ruiz-Merino G. A comparison of genicular nerve treatment using radiofrequency or analgesic block with corticosteroid for pain after total knee arthroplasty. Pain Pract. 2017;17(5):578–88. [PubMed] DOI: 1111/papr.12481
- Zeng Y, Xu Y. Application of genicular nerves block combined with iPACK block in postoperative analgesia of total knee arthroplasty. Asploro J Biomed Clin Case Rep. 2023;6(1):47–9. DOI: 36502/2023/ASJBCCR.6289
- Akesen S, Akesen B, Atıcı T, Gurbet A, Ermutlu C, Özyalçın A. Comparison of genicular nerve block and IPACK block for total knee replacement surgery: a randomized controlled study. Acta Orthop Traumatol Turc. 2021;55(2):134–40. [PubMed] DOI: 5152/j.aott.2021.20187
- Dündar A, Ipek D, Yalvaç M, Kaya Ş. Comparison of IPACK block and genicular nerve block in primary total knee arthroplasty: a prospective randomized trial. Saudi Med J. 2024;45(3):279–87. [PubMed] DOI: 15537/smj.2024.45.3.20230432
- Elliott CE, Myers TJ, Soberon JR. The adductor canal block combined with iPACK improves physical therapy performance and reduces hospital length of stay (Abstract 197). Presented at the 40th annual regional anesthesiology and acute pain medicine meeting (ASRA); 2015.
- Kukreja P, Venter A, Mason L, Kofskey AM, Northern T, Naranje S, et al. Comparison of genicular nerve block in combination with adductor canal block in both primary and revision total knee arthroplasty: a retrospective case series. Cureus. 2021;13(7):e16712. [PubMed] DOI: 7759/cureus.16712
- Et T, Korkusuz M, Basaran B, Yarımoğlu R, Toprak H, Bilge A, et al. Comparison of iPACK and periarticular block with adductor block alone after total knee arthroplasty: a randomized clinical trial. J Anesth. 2022;36(2):276–86. [PubMed] DOI: 1007/s00540-022-03047-6
- Sujatha SSN, Gupta K, Guria S, Chhabra PH. Comparison of genicular nerve block with adductor canal block for postoperative pain management in arthroscopic knee ligament reconstruction: a randomized controlled trial. Indian J Anaesth. 2024;68(5):454–9. [PubMed] DOI: 4103/ija.ija_994_23
- Wang F, Wu J, Wu Y, Han X, Dai H, Chen Q. Different peripheral nerve blocks for total knee arthroplasty: a network meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg. 2024;144(9):4179-4206. [PubMed] DOI: 1007/s00402-024-05507-y
- Chan E, Howle R, Onwochei D, Desai N. IPACK block in knee surgery: a narrative review. Reg Anesth Pain Med. 2021;46:784–805. [PubMed] DOI: 1136/rapm-2021-102681
- Zheng FY, Liu YB, Huang H, Xu S, Ma XJ, Liu YZ, et al. Impact of IPACK combined with adductor canal block under ultrasound guidance on early motor function after total knee arthroplasty. Braz J Anesthesiol. 2022;72(1):110–4. [PubMed] DOI: 1016/j.bjane.2021.04.012
- Kampitak W, Tanavalee A, Ngarmukos S, Tantavisut S. Motor-sparing effect of iPACK block vs tibial nerve block after total knee arthroplasty: a randomized controlled trial. Reg Anesth Pain Med. 2020;45(4):267–76. [PubMed] DOI: 1136/rapm-2019-100895