Rabab Mohamed Mohamed 1, Ahmed Aboelhasan Eid 2, Atia Gad Anwar 3
Author affiliations:
Objectives: This study compared the performance and safety of the Blockbuster Laryngeal Mask Airway (LMA) and the Baska Mask (BM) in patients undergoing laparoscopic cholecystectomy (LC).
Methodology: In this randomized open-label trial, 140 individuals between the ages of 18 and 60 years, underwent elcetive LC. Patients were chosen at random to receive either the Blockbuster LMA (Group L) or the Baska Mask (Group B).
Results: The groups exhibited comparability in terms of insertion time, number of attempts, and success rate. Group B had a statistically significant reduction in gastric tube insertion time (P = 0.005). Oropharyngeal leak pressure (OLP) was significantly higher in Group B, both just after insertion (P < 0.001) and at 30 min (P = 0.002). Hemodynamic parameters and peak airway pressure (PAP) were insignificantly different between the groups. Postoperative complications (pain, difficulty swallowing, cough, and blood on the device) were insignificantly different between the groups.
Conclusions: The BM exhibited a more effective oropharyngeal seal and facilitated the insertion of the stomach tube in comparison to the Blockbuster LMA, while both devices exhibited comparable insertion characteristics, hemodynamic profiles, and postoperative complications in patients undergoing LC.
Keywords: Laparoscopic cholecystectomy; Blockbuster LMA; Baska Mask; Supraglottic airway devices; Oropharyngeal leak pressure
Citation: Mohamed RM, Eid AA, Anwar AG. Blockbuster LMA versus Baska Mask in patients undergoing laparoscopic cholecystectomy: a randomized clinical trial. Anaesth. pain intensive care 2025;29(2):155-161. DOI: 10.35975/apic.v29i2.2698
Received: July 30, 2024; Reviewed: August 12, 2024; Accepted: August 12, 2024
Laparoscopic cholecystectomy (LC) stands out as one of the most frequently performed laparoscopic operations worldwide and has become increasingly prevalent across numerous surgical disciplines due to the well-established benefits it offers over traditional open procedures.1, 2
While general anesthesia facilitated by endotracheal intubation is routinely employed for LC, this approach is associated with several drawbacks. These include an elevated sympathetic stimulation during the process of intubation, pneumoperitoneum, and extubation, potential instances of unsuccessful intubation, and the potential for oropharyngeal damage during the insertion procedure, compounded by concerns regarding postoperative laryngopharyngeal complications.3
Supraglottic airway devices (SADs) serve in airway management algorithms is of utmost importance, serving as viable alternatives in both anticipated and unanticipated difficult airway situations.4 Compared to endotracheal tubes, SADs typically keep minimal oropharyngeal leak pressure (OLP). Nevertheless, it is important to note that the elevated inspiratory pressures necessary for laparoscopic procedures have the potential to surpass the OLP, hence augmenting the leak fraction and the subsequent hazards of aspiration. Consequently, laparoscopic surgery benefits from the use of second-generation SADs, which provide increased seal pressures and distinct channels for the alimentary and respiratory systems.5
The laryngeal mask airway (LMA) is employed for the purpose of establishing a regular airway during general anesthesia or, on occasion, as a means for tracheal intubation. Newer, improved LMA designs incorporate cuffs that provide higher leaking pressures than classic LMAs, while also allowing for the venting of gastric substances throughout a dedicated drainage conduit. Such modern technologies have the potential to be utilized in a safe manner during anesthesia for procedures that involve elevated peak airway pressures (PAP), for instance LC.6
The the Baska Mask (BM) is one of the 2nd generation SAD that incorporates a non-inflatable cuff that is seamlessly integrated with the air tract, thereby inflating with positive pressure ventilation to improve cuff seal.7
The Blockbuster LMA, a more recent SAD, is touted as an efficient conduit for endotracheal intubation.8 Multiple studies have investigated the efficacy of blind intubation using the Blockbuster LMA.9, 10
This trial was conducted with the objective of comparing the performance and safety profiles of two SADs, the Blockbuster LMA and the BM, in LC.
A randomized clinical trial with an open-label design was undertaken on a sample of 140 individuals, ranging in age from 18 to 60 years, of both genders, with American Society of Anesthesiologists (ASA) physical status I-II, listed for elective LC under general anesthesia. The study took place between December 2023 and April 2024 after obtaining approval from the Ethical Committee of Tanta University Hospitals (approval code: 36264PRS526/2/24) and registration on clinicaltrials.gov (ID: NCT06395922). Written informed consent was procured from all participants or their relatives.
The exclusion criteria where potential challenges in the respiratory system include respiratory distress, impaired kidney function, hiatus hernia, obesity, pregnancy, and the use of rate-controlling medicines, steroids, opioids, or regular antacids.
2.1. Randomization and blindness
In a parallel approach, the cases were randomly assigned using a sequence created by online random generator “www.random.org”. Participants were assigned randomly to two equal groups: Group L got the Blockbuster LMA, while Group B got the BM. The trial was conducted at an open label level due to variations in approaches.
Before surgery, history taking, clinical examination, and routine laboratory investigations were conducted. Standard monitors (pulse oximetry, temperature probe, noninvasive blood pressure, 5- lead ECG, and capnography) were applied in the operating theater.
2.2. Procedures
The assigned airway device was prepared according to manufacturer guidelines, with the cuff deflated, shaped if applicable, and the dorsal/external surface lubricated. Premedication comprising midazolam 0.02 mg/kg, glycopyrrolate 0.2 mg, and fentanyl 2 μg/kg was administered. After preoxygenation, induction was done with propofol 1-2.5 mg/kg, atracuruium 0.5 mg/kg to facilitate device placement.
In Group L, the LMA was inserted using the recommended technique, with the patient's head in the sniffing position. The appropriate size was selected based on body weight (size 3 for 30-50 kg, size 4 for 50-70 kg). In Group B, the BM was inserted by opening the mouth, avoiding the tongue, and negotiating the palatopharyngeal curve using the hand-tab.
The time from handling the device until confirmation of correct placement by auscultation was recorded. A lubricated 16 Fr gastric tube was passed through the drain tube, with correct placement confirmed by air injection and epigastric auscultation.
Anesthesia was maintained with 50% oxygen, isoflurane 1-1.5%, and boluses of atracuruium 0.1 mg/kg. Pneumoperitoneum was established manually at 12-15 mmHg using a Veress needle. At the end of surgery, neuromuscular blockade was reversed, and the device was removed upon the patient's ability to open their mouth on command.
Heart rate (HR), mean arterial blood pressure (MAP), and PAP were measured before induction, 1min, 3min, 5min, and 10min after induction between both groups.
The primary outcome was the OLP, measured 30 min after device insertion by closing the expiratory valveat 5 L/min gas flow until equilibrium (maximum 40 cmH2O). Secondary outcomes included OLP immediately after device insertion, device insertion time, successful gastric tube placement, PAP at different time points, and complications.
2.3. Sample size calculation
The sample size calculation was done by G*Power 3.1.9.2 (Universitat Kiel, Germany). The mean ± SD of OLP at 30 min after insertion, the primary outcome was 33.54 ± 5.1 in group L and 36.32 ± 5.8 in group B according to a previous study.3 The sample size was based on 0.509 effect size, 95% confidence limit, 80% power of the study, group ratio 1:1 and eight cases were added to each group to overcome dropout. Therefore, 70 patients were recruited for each group.
2.4. Statistical analysis
Statistical analysis was conducted utilizing IBM SPSS version 27 (IBM©, Chicago, IL, USA). Assessment of normality in the data distribution was executed through the Shapiro-Wilks test alongside the examination of histograms. For quantitative parametric data, descriptive statistics including mean and standard deviation were employed, with subsequent analysis performed using the unpaired Student t-test. Quantitative non-parametric data were presented as the median and interquartile range (IQR), followed by analysis via the Mann-Whitney test. The qualitative variables were presented in terms of frequency and percentage (%), and their analysis was carried out utilizing either the Chi-square test or Fisher's exact test, as deemed appropriate. A two-tailed P-value < 0.05 was deemed indicative of statistical significance.
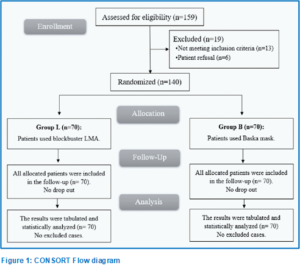
A total of 159 patients underwent initial eligibility assessment. Among them, 13 individuals did not meet the predefined criteria, while six decided not to participate. Subsequently, the remaining patients were randomly assigned to two groups, each comprising 70 patients. Following allocation, all patients were diligently monitored throughout the study period and subjected to comprehensive statistical analysis (Figure 2).
Demographic data and comorbidities were insignificantly different between both groups (Table 1).
The device insertion time, number of attempts, and success rate of insertion at the first attempt were statistically insignificant between both groups. The gastric tube insertion time was significantly lower in Group B compared to Group L (P = 0.005) (Table 2).
HR, MAP and PAP were insignificantly different before induction, then at 1, 3, 5, and 10 min after induction between both groups (Figure 3).
The OLP was statistically higher in Group B than Group L just after insertion with P < 0.001, and at 30 min after insertion with P = 0.002 (Table 3).
The incidences of postoperative complications, including pain in the throat, difficulty in swallowing, cough, and blood on the device, were statistically insignificant between the two groups. Change of voice and aspiration didn’t occur in any patient in both groups (Table 4).
Numerous studies have explored the LMAs performance in general anesthesia, like BM in LC.3-5, 7, 11, 12 and Blockbuster LMA in LC,13 and for elective surgeries.10, 14
The key findings in our trial suggest that while both airway devices exhibited comparable insertion times, number of attempts, and success rates without statistically significant differences between groups, the BM group exhibited a considerably shorter gastric tube insertion time in comparison to the Blockbuster LMA group (P = 0.005). This indicates a potential advantage of the BM over the Blockbuster LMA with regard to the simplicity of stomach conduit implantation. Regarding insertion characteristics, our results align with previous studies reporting similar outcomes for the BM for LC,3-5, 11 and Blockbuster LMA for LC,13 and surgical settings.10, 14 These findings collectively suggest that both devices offer reliable and efficient insertion characteristics, which is crucial for effective airway management during general anesthesia.
In this study, the BM demonstrated a significantly lower gastric tube insertion time compared to Blockbuster LMA (P = 0.005). These findings are consistent with previous reports by Sharma et al. and Chaudhary et al., who observed a shorter insertion time for for the BM compared to the I-gel device in LC surgeries. 3,4

This study found no significant changes in HR, MAP, or PAP before and after induction between the two groups, which aligns with the outcomes of Sharma et al. Conversely, Tosh et al. and Gain et al. reported notable rises in HR as well as MAP (p < 0.005) during and after insertion of BM compared to other airway devices like the I-gel and LMA Supreme in LC surgeries.3,5,7
Our study found that the OLP with the BM was significantly higher than the Blockbuster LMA both immediately after insertion (31.34 ± 5.35 cmH2O vs 28.61 ± 3.49 cmH2O, P < 0.001) and 30 min after insertion (37.41 ± 5.47 cmH2O vs 34.9 ± 3.88 cmH2O, P = 0.002) in LC surgeries. This indicates that the BM exhibited superior oropharyngeal leaking compared to the Blockbuster LMA. These findings are consistent with several other recent studies evaluating OLP performance of the BM compared to other SADs in similar surgical contexts. Chaudhary et al. reported significantly higher OLP with the BM versus the I-gel at insertion (P = 0.02) and 30 min after insertion (P = 0.001) in LC. 4 Mahajan et al. documented OLP of 29.25 ± 1.42 cmH2O at insertion and 33.47 ± 1.34 cmH2O at 30 min with the BM in this surgery type. 11 Sharma et al. found the BM had higher OLP than both the I-gel and LMA-Supreme at insertion (31.61 ± 4.3 cmH2O vs 28.27 ± 3.4 cmH2O and 29.42 ± 3.9 cmH2O respectively, P = 0.005) during LC. 3 Most recently, Gain et al. also reported higher OLP with the BM versus I-gel at insertion (30 cmH2O vs 25 cmH2O) in these surgeries.7 The consistent findings across multiple studies, including our own, provide strong evidence that the BM achieves higher OLP compared to other SADs like the I-gel, and LMA-Supreme when used for LC procedures. Higher OLP is clinically desirable as it enables the delivery of higher ventilation pressures while minimizing air leak and risk of aspiration.15 However, our findings contradict Beleña et al., who observed no significant differences in OLP (around 28 and 29 cmH2O, P = 0.61) between the BM and LMA-Supreme groups in LC. 12
In our study evaluating postoperative complications between the Blockbuster LMA and BM groups in LC, we found no statistically significant differences. Throat pain occurred in 24.29% Blockbuster LMA cases and 15.71% BM cases (P = 0.205). Dysphagia was seen in 4.29% LMA cases and 1.43% BM cases. Cough was reported in 2.86% Blockbuster LMA cases and 7.14% BM cases. Blood on the device was seen in 5.71% Blockbuster LMA cases and 2.86% BM cases.
These findings align with several previous studies. Chaudhary et al.4 reported throat pain in 8% BM cases (P = 0.9), with no dysphagia or coughing in either group (P = 0.99). Beleña et al. found coughing in 2.5% cases with BM groups, and blood on the mask in 10% LMA-supreme cases and 12.5% BM cases (P = 0.9).12 Sharma et al. noted no significant differences (p>0.05) among the BM, I-gel, and LMA-supreme groups for throat pain (16.6%, 23.3%, 30% cases), cough (10%, 3.3%, 6.6%), or blood on the device (3.3%, 13.3%, 3.3%).3
While some studies showed higher complication rates with certain devices in general anesthesia cases for elective surgeries, such as Endigeri et al.10 reporting higher sore throat (53.3% vs 10%, P = 0.003), nausea, vomiting (20% vs 6.6%, P = 0.12), and blood staining (20% vs 3.3%, P = 0.04) with Fastrach LMA compared to Blockbuster LMA, our data specific to LC suggests the Blockbuster LMA and BM have comparable safety profiles. Gain et al. also found rare cough cases (10.71% endotracheal tube (ET), 3.57% I-gel, 3.57% BM) and blood staining (10.71% ET, 7.14% I-gel, 3.57% BM) across ET, I-gel, and BM groups in LC, with no significant differences noted.7 Modi et al. demonstrated a higher postoperative sore throat incidence with Fastrach LMA versus Blockbuster LMA at 2 hours (58% vs 34%, P < 0.05) and 4 hours (44% vs 22%, P < 0.05) in general anesthesia for elective surgeries, though not immediately postoperatively.14
The study had several limitations that should be acknowledged. Firstly, the sample size, although calculated based on previous studies, may not be sufficient to detect differences in adverse events. Secondly, the investigation was carried out exclusively at a single center, perhaps constraining the applicability of the results to different healthcare environments or patient populations. Additionally, the study focused on a specific surgical procedure, LC, and the results may not be directly applicable to other types of surgeries or clinical scenarios. Furthermore, the study did not assess long-term outcomes or patient-reported outcomes, such as postoperative quality of life or recovery time, which could provide valuable insights into the overall impact of these airway management strategies.
Both the Blockbuster LMA and Baska mask offer reliable insertion characteristics and comparable safety profiles in laparoscopic cholecystectomy. The Baska mask demonstrated superior oropharyngeal leak pressure and ease of gastric tube insertion. These advantages may be attributed to the unique design features of the Baska mask, potentially making it a favorable choice for airway management in laparoscopic procedures.
7. Data availability
Numerical data generated during this research is available with the authors and can be provided on a reasonable request.
8. Funding
The study utilized institutional resources only. No industry or donor funding was needed.
9. Conflict of interest
The authors declare no conflict of interest.
10. Ethical and approval consideration
Permission was taken from all patients and health control to fill in the information required and they were assured regarding the confidentiality of their responses. The aim of the study was explained and only those who agreed to participate were included in the study (Ref Letter 3/7/107 in 18/01/2022).
11. Author contribution
M. M. developed the original idea and the protocol, abstracted and analyzed data, wrote the manuscript, and is a guarantor. A. G. A. and A. A. E. contributed to the development of the protocol, abstracted data, and prepared the manuscript.
Author affiliations:
- Rabab Mohamed Mohamed, Department of Anesthesiology, Surgical Intensive Care & Pain Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; Email: rabmoh_30@outlook.com
- Ahmed Aboelhasan Eid, Department of Anesthesiology, Surgical Intensive Care & Pain Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; Email: boelhasan82@gmail.com
- Atia Gad Anwar, Department of Anesthesiology, Surgical Intensive Care & Pain Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; Email: atteiagad@gmail.com
ABSTRACT
Objectives: This study compared the performance and safety of the Blockbuster Laryngeal Mask Airway (LMA) and the Baska Mask (BM) in patients undergoing laparoscopic cholecystectomy (LC).
Methodology: In this randomized open-label trial, 140 individuals between the ages of 18 and 60 years, underwent elcetive LC. Patients were chosen at random to receive either the Blockbuster LMA (Group L) or the Baska Mask (Group B).
Results: The groups exhibited comparability in terms of insertion time, number of attempts, and success rate. Group B had a statistically significant reduction in gastric tube insertion time (P = 0.005). Oropharyngeal leak pressure (OLP) was significantly higher in Group B, both just after insertion (P < 0.001) and at 30 min (P = 0.002). Hemodynamic parameters and peak airway pressure (PAP) were insignificantly different between the groups. Postoperative complications (pain, difficulty swallowing, cough, and blood on the device) were insignificantly different between the groups.
Conclusions: The BM exhibited a more effective oropharyngeal seal and facilitated the insertion of the stomach tube in comparison to the Blockbuster LMA, while both devices exhibited comparable insertion characteristics, hemodynamic profiles, and postoperative complications in patients undergoing LC.
Keywords: Laparoscopic cholecystectomy; Blockbuster LMA; Baska Mask; Supraglottic airway devices; Oropharyngeal leak pressure
Citation: Mohamed RM, Eid AA, Anwar AG. Blockbuster LMA versus Baska Mask in patients undergoing laparoscopic cholecystectomy: a randomized clinical trial. Anaesth. pain intensive care 2025;29(2):155-161. DOI: 10.35975/apic.v29i2.2698
Received: July 30, 2024; Reviewed: August 12, 2024; Accepted: August 12, 2024
1. INTRODUCTION
Laparoscopic cholecystectomy (LC) stands out as one of the most frequently performed laparoscopic operations worldwide and has become increasingly prevalent across numerous surgical disciplines due to the well-established benefits it offers over traditional open procedures.1, 2
While general anesthesia facilitated by endotracheal intubation is routinely employed for LC, this approach is associated with several drawbacks. These include an elevated sympathetic stimulation during the process of intubation, pneumoperitoneum, and extubation, potential instances of unsuccessful intubation, and the potential for oropharyngeal damage during the insertion procedure, compounded by concerns regarding postoperative laryngopharyngeal complications.3
Supraglottic airway devices (SADs) serve in airway management algorithms is of utmost importance, serving as viable alternatives in both anticipated and unanticipated difficult airway situations.4 Compared to endotracheal tubes, SADs typically keep minimal oropharyngeal leak pressure (OLP). Nevertheless, it is important to note that the elevated inspiratory pressures necessary for laparoscopic procedures have the potential to surpass the OLP, hence augmenting the leak fraction and the subsequent hazards of aspiration. Consequently, laparoscopic surgery benefits from the use of second-generation SADs, which provide increased seal pressures and distinct channels for the alimentary and respiratory systems.5
The laryngeal mask airway (LMA) is employed for the purpose of establishing a regular airway during general anesthesia or, on occasion, as a means for tracheal intubation. Newer, improved LMA designs incorporate cuffs that provide higher leaking pressures than classic LMAs, while also allowing for the venting of gastric substances throughout a dedicated drainage conduit. Such modern technologies have the potential to be utilized in a safe manner during anesthesia for procedures that involve elevated peak airway pressures (PAP), for instance LC.6
The the Baska Mask (BM) is one of the 2nd generation SAD that incorporates a non-inflatable cuff that is seamlessly integrated with the air tract, thereby inflating with positive pressure ventilation to improve cuff seal.7
The Blockbuster LMA, a more recent SAD, is touted as an efficient conduit for endotracheal intubation.8 Multiple studies have investigated the efficacy of blind intubation using the Blockbuster LMA.9, 10
This trial was conducted with the objective of comparing the performance and safety profiles of two SADs, the Blockbuster LMA and the BM, in LC.
2. METHODOLOGY
A randomized clinical trial with an open-label design was undertaken on a sample of 140 individuals, ranging in age from 18 to 60 years, of both genders, with American Society of Anesthesiologists (ASA) physical status I-II, listed for elective LC under general anesthesia. The study took place between December 2023 and April 2024 after obtaining approval from the Ethical Committee of Tanta University Hospitals (approval code: 36264PRS526/2/24) and registration on clinicaltrials.gov (ID: NCT06395922). Written informed consent was procured from all participants or their relatives.
The exclusion criteria where potential challenges in the respiratory system include respiratory distress, impaired kidney function, hiatus hernia, obesity, pregnancy, and the use of rate-controlling medicines, steroids, opioids, or regular antacids.
2.1. Randomization and blindness
In a parallel approach, the cases were randomly assigned using a sequence created by online random generator “www.random.org”. Participants were assigned randomly to two equal groups: Group L got the Blockbuster LMA, while Group B got the BM. The trial was conducted at an open label level due to variations in approaches.
Before surgery, history taking, clinical examination, and routine laboratory investigations were conducted. Standard monitors (pulse oximetry, temperature probe, noninvasive blood pressure, 5- lead ECG, and capnography) were applied in the operating theater.
2.2. Procedures
The assigned airway device was prepared according to manufacturer guidelines, with the cuff deflated, shaped if applicable, and the dorsal/external surface lubricated. Premedication comprising midazolam 0.02 mg/kg, glycopyrrolate 0.2 mg, and fentanyl 2 μg/kg was administered. After preoxygenation, induction was done with propofol 1-2.5 mg/kg, atracuruium 0.5 mg/kg to facilitate device placement.
In Group L, the LMA was inserted using the recommended technique, with the patient's head in the sniffing position. The appropriate size was selected based on body weight (size 3 for 30-50 kg, size 4 for 50-70 kg). In Group B, the BM was inserted by opening the mouth, avoiding the tongue, and negotiating the palatopharyngeal curve using the hand-tab.
The time from handling the device until confirmation of correct placement by auscultation was recorded. A lubricated 16 Fr gastric tube was passed through the drain tube, with correct placement confirmed by air injection and epigastric auscultation.
Anesthesia was maintained with 50% oxygen, isoflurane 1-1.5%, and boluses of atracuruium 0.1 mg/kg. Pneumoperitoneum was established manually at 12-15 mmHg using a Veress needle. At the end of surgery, neuromuscular blockade was reversed, and the device was removed upon the patient's ability to open their mouth on command.
Heart rate (HR), mean arterial blood pressure (MAP), and PAP were measured before induction, 1min, 3min, 5min, and 10min after induction between both groups.
The primary outcome was the OLP, measured 30 min after device insertion by closing the expiratory valveat 5 L/min gas flow until equilibrium (maximum 40 cmH2O). Secondary outcomes included OLP immediately after device insertion, device insertion time, successful gastric tube placement, PAP at different time points, and complications.
2.3. Sample size calculation
The sample size calculation was done by G*Power 3.1.9.2 (Universitat Kiel, Germany). The mean ± SD of OLP at 30 min after insertion, the primary outcome was 33.54 ± 5.1 in group L and 36.32 ± 5.8 in group B according to a previous study.3 The sample size was based on 0.509 effect size, 95% confidence limit, 80% power of the study, group ratio 1:1 and eight cases were added to each group to overcome dropout. Therefore, 70 patients were recruited for each group.
2.4. Statistical analysis
Statistical analysis was conducted utilizing IBM SPSS version 27 (IBM©, Chicago, IL, USA). Assessment of normality in the data distribution was executed through the Shapiro-Wilks test alongside the examination of histograms. For quantitative parametric data, descriptive statistics including mean and standard deviation were employed, with subsequent analysis performed using the unpaired Student t-test. Quantitative non-parametric data were presented as the median and interquartile range (IQR), followed by analysis via the Mann-Whitney test. The qualitative variables were presented in terms of frequency and percentage (%), and their analysis was carried out utilizing either the Chi-square test or Fisher's exact test, as deemed appropriate. A two-tailed P-value < 0.05 was deemed indicative of statistical significance.
| Table 1: Demographic data and comorbidities of the studied groups | ||||
| Parameter | Group L (n=70) |
Group B (n=70) |
P value | |
| Age (y) | 41.6 ± 11.67 | 43.21 ± 10.23 | 0.386 | |
| Gender | Male | 33 (47.14) | 27 (38.57) | 0.306 |
| Female | 37 (52.86) | 43 (61.43) | ||
| Weight (kg) | 68.67 ± 7.11 | 66.46 ± 7.22 | 0.070 | |
| Height | 167.66 ± 6.86 | 166.5 ± 7.26 | 0.334 | |
| BMI (kg/m2) | 24.57 ± 3.38 | 24.06 ± 3 | 0.350 | |
| ASA physical status | I | 52 (74.29) | 50 (71.43) | 0.704 |
| II | 18 (25.71) | 20 (28.57) | ||
| Hypertension | 24 (34.29) | 20 (28.57) | 0.466 | |
| DM | 18 (25.71) | 15 (21.43) | 0.550 | |
| Smoking | 22 (31.43) | 20 (28.57) | 0.712 | |
| Data are presented as mean ± SD or frequency (%). BMI: Body mass index, ASA: American Society of Anesthesiologists, DM: Diabetes mellitus | ||||
| Table 2: Insertion parameters of laryngeal mask airway of the studied groups | ||||
| Variable | Group L (n=70) |
Group B (n=70) |
P value | |
| Device insertion time (s) | 15.01 ± 6.04 | 14.06 ± 5.66 | 0.335 | |
| Gastric tube insertion time
(sec) |
10.87 ± 4.31 | 9.21 ± 2.25 | 0.005* | |
| Number of attempts | 1 | 64 (91.43) | 66 (94.29) | 0.744 |
| 2 | 6 (8.57) | 4 (5.71) | ||
| Success rate of insertion at the first attempt |
62 (88.57) | 66 (94.29) | 0.366 | |
| Data are presented as mean ± SD or frequency (%). *Significant as P ≤ 0.05 | ||||
| Table 3: Oropharyngeal leak pressure (OLP) of the studied groups | |||
| Parameter | Group L (n=70) |
Group B (n=70) |
P value |
| OLP just after insertion | 28.61 ± 3.49 | 31.34 ± 5.35 | < 0.001* |
| OLP 30 min after insertion | 34.9 ± 3.88 | 37.41 ± 5.47 | 0.002* |
| Data are presented as median (IQR) *: Significant when P value ≤0.05. | |||
3. RESULTS
A total of 159 patients underwent initial eligibility assessment. Among them, 13 individuals did not meet the predefined criteria, while six decided not to participate. Subsequently, the remaining patients were randomly assigned to two groups, each comprising 70 patients. Following allocation, all patients were diligently monitored throughout the study period and subjected to comprehensive statistical analysis (Figure 2).
Demographic data and comorbidities were insignificantly different between both groups (Table 1).
The device insertion time, number of attempts, and success rate of insertion at the first attempt were statistically insignificant between both groups. The gastric tube insertion time was significantly lower in Group B compared to Group L (P = 0.005) (Table 2).
HR, MAP and PAP were insignificantly different before induction, then at 1, 3, 5, and 10 min after induction between both groups (Figure 3).
The OLP was statistically higher in Group B than Group L just after insertion with P < 0.001, and at 30 min after insertion with P = 0.002 (Table 3).
The incidences of postoperative complications, including pain in the throat, difficulty in swallowing, cough, and blood on the device, were statistically insignificant between the two groups. Change of voice and aspiration didn’t occur in any patient in both groups (Table 4).
4. DISCUSSION
Numerous studies have explored the LMAs performance in general anesthesia, like BM in LC.3-5, 7, 11, 12 and Blockbuster LMA in LC,13 and for elective surgeries.10, 14
The key findings in our trial suggest that while both airway devices exhibited comparable insertion times, number of attempts, and success rates without statistically significant differences between groups, the BM group exhibited a considerably shorter gastric tube insertion time in comparison to the Blockbuster LMA group (P = 0.005). This indicates a potential advantage of the BM over the Blockbuster LMA with regard to the simplicity of stomach conduit implantation. Regarding insertion characteristics, our results align with previous studies reporting similar outcomes for the BM for LC,3-5, 11 and Blockbuster LMA for LC,13 and surgical settings.10, 14 These findings collectively suggest that both devices offer reliable and efficient insertion characteristics, which is crucial for effective airway management during general anesthesia.
In this study, the BM demonstrated a significantly lower gastric tube insertion time compared to Blockbuster LMA (P = 0.005). These findings are consistent with previous reports by Sharma et al. and Chaudhary et al., who observed a shorter insertion time for for the BM compared to the I-gel device in LC surgeries. 3,4
This study found no significant changes in HR, MAP, or PAP before and after induction between the two groups, which aligns with the outcomes of Sharma et al. Conversely, Tosh et al. and Gain et al. reported notable rises in HR as well as MAP (p < 0.005) during and after insertion of BM compared to other airway devices like the I-gel and LMA Supreme in LC surgeries.3,5,7
Our study found that the OLP with the BM was significantly higher than the Blockbuster LMA both immediately after insertion (31.34 ± 5.35 cmH2O vs 28.61 ± 3.49 cmH2O, P < 0.001) and 30 min after insertion (37.41 ± 5.47 cmH2O vs 34.9 ± 3.88 cmH2O, P = 0.002) in LC surgeries. This indicates that the BM exhibited superior oropharyngeal leaking compared to the Blockbuster LMA. These findings are consistent with several other recent studies evaluating OLP performance of the BM compared to other SADs in similar surgical contexts. Chaudhary et al. reported significantly higher OLP with the BM versus the I-gel at insertion (P = 0.02) and 30 min after insertion (P = 0.001) in LC. 4 Mahajan et al. documented OLP of 29.25 ± 1.42 cmH2O at insertion and 33.47 ± 1.34 cmH2O at 30 min with the BM in this surgery type. 11 Sharma et al. found the BM had higher OLP than both the I-gel and LMA-Supreme at insertion (31.61 ± 4.3 cmH2O vs 28.27 ± 3.4 cmH2O and 29.42 ± 3.9 cmH2O respectively, P = 0.005) during LC. 3 Most recently, Gain et al. also reported higher OLP with the BM versus I-gel at insertion (30 cmH2O vs 25 cmH2O) in these surgeries.7 The consistent findings across multiple studies, including our own, provide strong evidence that the BM achieves higher OLP compared to other SADs like the I-gel, and LMA-Supreme when used for LC procedures. Higher OLP is clinically desirable as it enables the delivery of higher ventilation pressures while minimizing air leak and risk of aspiration.15 However, our findings contradict Beleña et al., who observed no significant differences in OLP (around 28 and 29 cmH2O, P = 0.61) between the BM and LMA-Supreme groups in LC. 12
In our study evaluating postoperative complications between the Blockbuster LMA and BM groups in LC, we found no statistically significant differences. Throat pain occurred in 24.29% Blockbuster LMA cases and 15.71% BM cases (P = 0.205). Dysphagia was seen in 4.29% LMA cases and 1.43% BM cases. Cough was reported in 2.86% Blockbuster LMA cases and 7.14% BM cases. Blood on the device was seen in 5.71% Blockbuster LMA cases and 2.86% BM cases.
These findings align with several previous studies. Chaudhary et al.4 reported throat pain in 8% BM cases (P = 0.9), with no dysphagia or coughing in either group (P = 0.99). Beleña et al. found coughing in 2.5% cases with BM groups, and blood on the mask in 10% LMA-supreme cases and 12.5% BM cases (P = 0.9).12 Sharma et al. noted no significant differences (p>0.05) among the BM, I-gel, and LMA-supreme groups for throat pain (16.6%, 23.3%, 30% cases), cough (10%, 3.3%, 6.6%), or blood on the device (3.3%, 13.3%, 3.3%).3
While some studies showed higher complication rates with certain devices in general anesthesia cases for elective surgeries, such as Endigeri et al.10 reporting higher sore throat (53.3% vs 10%, P = 0.003), nausea, vomiting (20% vs 6.6%, P = 0.12), and blood staining (20% vs 3.3%, P = 0.04) with Fastrach LMA compared to Blockbuster LMA, our data specific to LC suggests the Blockbuster LMA and BM have comparable safety profiles. Gain et al. also found rare cough cases (10.71% endotracheal tube (ET), 3.57% I-gel, 3.57% BM) and blood staining (10.71% ET, 7.14% I-gel, 3.57% BM) across ET, I-gel, and BM groups in LC, with no significant differences noted.7 Modi et al. demonstrated a higher postoperative sore throat incidence with Fastrach LMA versus Blockbuster LMA at 2 hours (58% vs 34%, P < 0.05) and 4 hours (44% vs 22%, P < 0.05) in general anesthesia for elective surgeries, though not immediately postoperatively.14
5. LIMITATIONS
The study had several limitations that should be acknowledged. Firstly, the sample size, although calculated based on previous studies, may not be sufficient to detect differences in adverse events. Secondly, the investigation was carried out exclusively at a single center, perhaps constraining the applicability of the results to different healthcare environments or patient populations. Additionally, the study focused on a specific surgical procedure, LC, and the results may not be directly applicable to other types of surgeries or clinical scenarios. Furthermore, the study did not assess long-term outcomes or patient-reported outcomes, such as postoperative quality of life or recovery time, which could provide valuable insights into the overall impact of these airway management strategies.
6. CONCLUSION
Both the Blockbuster LMA and Baska mask offer reliable insertion characteristics and comparable safety profiles in laparoscopic cholecystectomy. The Baska mask demonstrated superior oropharyngeal leak pressure and ease of gastric tube insertion. These advantages may be attributed to the unique design features of the Baska mask, potentially making it a favorable choice for airway management in laparoscopic procedures.
7. Data availability
Numerical data generated during this research is available with the authors and can be provided on a reasonable request.
8. Funding
The study utilized institutional resources only. No industry or donor funding was needed.
9. Conflict of interest
The authors declare no conflict of interest.
10. Ethical and approval consideration
Permission was taken from all patients and health control to fill in the information required and they were assured regarding the confidentiality of their responses. The aim of the study was explained and only those who agreed to participate were included in the study (Ref Letter 3/7/107 in 18/01/2022).
11. Author contribution
M. M. developed the original idea and the protocol, abstracted and analyzed data, wrote the manuscript, and is a guarantor. A. G. A. and A. A. E. contributed to the development of the protocol, abstracted data, and prepared the manuscript.
12. REFERENCES
- Patil Jr M, Gharde P, Reddy K, Nayak K, Patil M. Comparative analysis of laparoscopic versus open procedures in specific general surgical interventions. Cureus. 2024;6(2):e54433. [PubMed] DOI: 7759/cureus.54433
- Kang SH, Park M. Comparison of early postoperative recovery between laryngeal mask airway and endotracheal tube in laparoscopic cholecystectomy: A randomized trial. Medicine. 2019;98:e16022. [PubMed] DOI: 1097/MD.0000000000016022
- Sharma P, Rai S, Tripathi M, Malviya D, Kumari S, Mishra S. Comparison of LMA supreme, i-gel, and baska mask for airway management during laparoscopic cholecystectomy: A prospective randomized comparative study from North India. Anesth Essays Res. 2022;16:42-8. [PubMed] DOI: 4103/aer.aer_23_22
- Chaudhary UK, Mahajan SR, Mahajan M, Sharma C, Sharma M. A comparative analysis of the baska mask versus I-gel for general anesthesia in surgical patients undergoing laparoscopic cholecystectomy. Acta Med Int. 2018;5:69-73. DOI: 4103/ami.ami_41_18
- Tosh P, Kumar RB, Sahay N, Suman S, Bhadani UK. Efficacy of Baska mask as an alternative airway device to endotracheal tube in patients undergoing laparoscopic surgeries under controlled ventilation. J Anaesthesiol Clin Pharmacol. 2021;37:419-24. [PubMed] DOI: 4103/joacp.JOACP_339_19
- Gill RK, Tarat A, Pathak D, Dutta S. Comparative study of two laryngeal mask airways: Proseal laryngeal mask airway and supreme laryngeal mask airway in anesthetized paralyzed adults undergoing elective surgery. Anesth Essays Res. 2017;11:23-7. [PubMed] DOI: 4103/0259-1162.177184
- Gain A, Mallick S, Ghosh S, Swaika S, Mandal US, Choudhury A. Comparison of Baska mask and I-gel with endotracheal tube in laparoscopic cholecystectomy: A randomized controlled study. Asian J Med Sci. 2024;15:14-21. [FreeFullText]
- Pang N, Pan F, Chen R, Zhang B, Yang Z, Guo M, et al. Laryngeal mask airway versus endotracheal intubation as general anesthesia airway managements for atrial fibrillation catheter ablation: A comparative analysis based on propensity score matching. J Interv Card Electrophysiol. 2024;67(6):1377-90. [PubMed] DOI: 1007/s10840-024-01742-w
- Shuai Z, Jing Z, Ye Z, Fang X, Ming T. Application of blind orotracheal intubation via Blockbuster laryngeal mask in patients undergoing general anesthesia. Int J Anesth Resus. 2016;10:917-24.
- Endigeri A, Ganeshnavar A, Varaprasad B, Shivanand Y, Ayyangouda B. Comparison of success rate of BlockBuster® versus Fastrach® LMA as conduit for blind endotracheal intubation: A prospective randomised trial. Indian J Anaesth. 2019;63:988-94. [PubMed] DOI: 4103/ija.IJA_396_19
- Mahajan SR, Mahajan M, Chaudhary U, Kumar S. Evaluation of baska mask performance in laparoscopic cholecystectomy. IOSR J Dent Med Sci. 2018;17:74-8. [FreeFullText]
- Beleña J, Núñez M, Alvarez-Manzanedo R, Fernandez-Lanza V. A prospective randomized controlled trial of the Baska® mask and the LMA Supreme® in patients undergoing laparoscopic cholecystectomy. Acta Anaesth Belg. 2020;71:23-8. DOI: 56126/71.1.04
- Guleria A, Badhan A, Sood P, Singha D, Bhandari S. A comparative study to evaluate the ease of blind tracheal intubation through the I-Gel versus the Blockbuster LMA during general anaesthesia. Eur J Cardiovasc Med. 2023;13(2):422. [FreeFullText]
- Modi K, Pathak R, Kanchanaa S. A study of BlockBuster laryngeal mask airway versus Fastrach/Intubating laryngeal mask airway as a conduit for blind oro-tracheal intubation: A prospective randomized controlled study. Indian J Clin Anaesth. 2022;9:422-7. DOI: 18231/j.ijca.2022.086
- Alexiev V, Salim A, Kevin L, Laffey J. An observational study of the Baska® mask: a novel supraglottic airway. Anaesthesia. 2012;67:640-5. [PubMed] DOI: 1111/j.1365-2044.2012.07140.x