Furqan Moein Auda 1, Athraa Rehman 2
Author affiliations:
Background & objective: Atherosclerosis is a condition where fat deposits cause blood arteries to stiffen and become hard instead of flexible. Many factors cause arterial stiffness, including hyperlipidemia, hypertension, hyperglycemia. In the current study, we attempted to shed light on the effect of chronic high cortisol and its relationship to early predictive indicators of atherosclerosis.
Methodology: This was a case-control study which included 60 Patient and 30 control are participated in this study. Their ages ranged between 45-70 y, all patients diagnosed with vascular diseases by ultrasound and diagnostic catheterization. Samples were taken in the morning when they were fasting, and it taken from the Open-Heart Institute, Al-Sadr Teaching Hospital, Najaf, Iraq.
Results: The study showed that patients with atherosclerosis suffer from increase in the level of cortisol, in addition to a significant increase in the concentration of midkine, cholesterol, low-density lipoprotein and atherogenic index. On the other hand, the study revealed a notable drop in the amounts of high-density lipoprotein in patients compared to the control group. Finally, we can conclude from this study that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoprotein remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis.
Conclusions: From this study it be can concluded that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoprotein remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis. Abbreviations: MDK - midkine; HDL - high density lipoprotein; LDL - low density lipoprotein; VSMC - vascular smooth muscle cells; NO - nitric oxide; TG - triglyceride; BMI - body mass index Keywords: Atherosclerosis, cortisol resistance, midkine and atherogenic index.
Citation: Auda FM, Rehman A. Evaluation of midkine, cortisol, and other biochemical indicators in patients with atherosclerosis. Anaesth. pain intensive care 2025;29(1):40-46. DOI: 10.35975/apic.v28i6.2661
Received: June 03, 2024; Reviewed: June 16, 2024; Accepted: December 29, 2025
Atherosclerosis is a condition that forms gradually in blood vessels due to oxidized fat buildup on the artery's surface, although its symptoms don't always show up right away.1 There are many causes of plaque formation, including hypercholesterolemia, hypertriglyceridemia levels, hypertension, smoking, and diabetes.2 Cholesterol and triglycerides are hydrophobic and cannot move into the blood except by binding to special transporters,3 its surface is water-loving protein and the core is hydrophobic and loaded with fats such as LDL Which transports fats to cells and HDL that transports fats to the liver.4 Oxidation of LDL is caused by an increase in either internal or external oxidation agents, and elevated levels of oxidized low-density lipoprotein (oxLDL) in the blood are an essential indicator of arteriosclerosis.5,6 oxLDL blocks the action of nitric oxide a vital vasodilator, and stimulates the immune response, including recruitment of monocytes and their differentiation into phagocytosis and the formation of foam cells,7 migration and proliferation of vascular smooth muscle cells (VSMC).8 The integrity of the endothelium barrier and the retention of atherogenic LDL are impacted by the decreased expression of endothelial NO synthase and superoxide dismutase, which are in charge of preserving an effective barrier and lowering oxidative stress, respectively.9 Monocytes convert into Macrophage cells, which phagocytose and uptake oxidized lipids. They then become foam cells and, ultimately, fatty lines on the blood vessel wall.10 In addition, there are many parameters that development of atherosclerosis such as stress hormones, Cortisol a cyclic organic hormone that is the basic substance for synthesis is cholesterol. It is secreted from the adrenal gland as a result of exposure to stress.11 Following a stressful event, the pituitary gland secretes adrenocorticotropic hormone, which acts as a catalyst to produce the hormone cortisol, which increases low-density lipoprotein receptors. and boost the activity of cholesterol desmolase, the rate-limiting step in the manufacture of cortisol that transforms cholesterol to pregnenolone.12 Research indicates that prolonged stress might elevate cortisol levels, which in turn can worsen lipid hyperglycemia—a major risk factor for atherosclerosis.13 Cortisol raises blood sugar by breaking down protein in the muscles and converting them into amino acids, which the liver converts with glycerol in the process of gluconeogenesis into sugar. Also it raises blood sugar by breakdown of glycogen by glycogenolysis and converting it into sugar.14 Chronic or persistent high blood sugar leads to its conversion into lipid and storage in adipocytes. If the fat cells are full, it leads to its accumulation in the blood, which is considered an important risk factor for atherosclerosis.15 Also one of the early indicators of atherosclerosis is Midkine (MDK) is a member of the protein family that binds carbohydrates and functions as a cytokine or growth factor.16 As seen in Figure 1. MDK levels have a positive correlation with LDL-C and total cholesterol; midkine stimulates lipid accumulation in macrophages. An early stage of atherogenesis called foam cell development might result from lipid buildup in macrophages.17
The main objective of the study was to evaluate serum midkine and cortisol as specific biomarkers for early diagnosis of atherosclerosis.
This is a case-control study which included sixty patients with atherosclerosis and thirty control are participated in this study. Their ages ranged between 45-70 y, all patients diagnosed with vascular diseases by ultrasound and diagnostic catheterization. Samples were taken in the morning when they were fasting, and it taken from the Al-Sadr Medical City's Open-Heart Center is located in AL-Najaf Al-Ashraf, Iraq. Patients were evaluated through a complete medical history to explore the presence of other diseases related to vascular disease which may influence this study. healthy people were chosen to serve as the control group because their age ranges were similar to the patients’. All these people were not smokers and did not suffer from vascular diseases, kidney disease, inflammation and thyroid disease.
2.1. Blood sample collection
Five milliliters of venous blood samples were drawn using a disposable needle and plastic syringes from each patient and control subjects without a tourniquet, in the morning who had fasted for 10 hours. Samples were transferred into a gel tube these samples were separated by a centrifuge at 3000 rpm for 15 min.
2.2. Serum level of cytokine and hormone
The serum levels of cortisol and midkine were measured enzymatically using the ELISA technique using ELISA kit from the PARS Biochem Company (China).
2.3. Serum level of lipid profile
Cholesterol, triglyceride and high-density lipoprotein (HDL) were determined by the spectrophotometer method using a unique kit from the Spinreact firm for each parameter (Spanish). Low density lipoprotein, very low-density lipoprotein and atherogenic index were measured mathematically.
2.4. Statistical analysis
The statistical analysis of the current study was completed using the SPSS Model 26 program, to determine the mean ± standard deviation and p-value, Excel 2016 18 was used, whereas the sensitivity of the assessed parameters was presented via a receiver operating characteristic (ROC) curve 19.
3.1. Demographic characteristics
Table 1 shows the demographic characteristics of the study population. The mean age of patients with atherosclerosis was 57.26 ± 7.29 y, which was very close to that of the controls (59.93 ± 7.35 y) with no significant difference. Also, the two groups comparable with regard to mean BMI with no significant differences.
3.2. Hormonal and cytokine profile
Table 2 shows the levels of the cortisol and midkine in patients with atherosclerosis compared to the control group, as it shows a significant increase in the levels of cortisol and midkine in patients compared to the control group.
3.3. Lipid profile and atherogenic index
Table 3 shows significant increase (P < 0.05) in total cholesterol and LDL in patients as compared with the control group. In addition, the results show significant decrease in HDL between the two groups, no significant change in TG as compared with the control group.
3.4. Correlation between all variables in atherosclerosis patients
Spearman’s correlation test was used to explore the possible correlation of all parameters in patients and controls. Cortisol displayed a significant positive correlation with all parameters except midkine and HDL. Cortisol showed a significant negative correlation with HDL. On the other hand, midkine appearance positive correlation with VLDL as shown in (Table 4).
3.5. Diagnostic value of Cortisol and Midkine
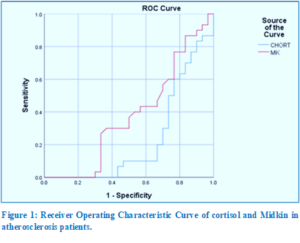
Receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of cortisol and midkine in the context of discrimination between atherosclerosis patients and healthy group. The area under the curve (AUC) of cortisol was 0.769, 95% CI = 0.645-0.893, P = 0.001. The sensitivity and specificity of the test, at cut off value = 80.9, were 71% and 72.4%, respectively.while, The sensitivity and specificity of midkine = 60,56.7 respectively as shown in (Table 5, Figure 1).
The results in the Table 1 indicate that there was no significant difference in age and body mass index (BMI) between patients and controls. While the results in Table 2 indicate a significant increase in cholesterol, low density lipoprotein (LDL), very low density lipoprotein (vLDL), Index I, Index II, Index III results are consistent with many earlier studies, where it was shown that lipid is the important risk factor of atherosclerosis,20 Cholesterol is the most closely linked to heart disease. It is hydrophobic, so it binds to lipoproteins to can travel through the blood, such as (HDL, LDL,VLDL, Chylomicron),21 increase in the level of LDL in the body with the presence of internal or external oxidation factors that lead to its conversion LDL into OXLDL,22 which is deposited on the artery wall, so the immune cells (macrophages) devour it through the process of phagocytosis, which then turns into foam cell and then lead to atherosclerosis such as this studies.23
When good cholesterol is low, the risk of developing atherosclerosis increases due to a defect in the reverse transport of cholesterol and a weak protective role of crystallized good cholesterol in reducing the oxidation of other lipoproteins,24 high bad cholesterol and low good cholesterol are due to a person following an unhealthy lifestyle,25 such as not exercising, smoking,26 or eating large amounts of carbohydrates and starches.27 The study data in Table 2 shows that there was no significant increase in the level of triglycerides (P = 0.837) in patients with atherosclerosis, which may be due to the patients taking lipid-lowering treatments, such as statins. Niacin (nicotinic acid) decreases TG levels by up to 30-40%, or may be due to patients following a healthy diet or intermittent fasting according to the doctor’s instructions to reduce triglycerides, as when fasting, the intestine’s production of chylomicrons (these particles are highly enriched in TG and produced by the intestine) that transport triglycerides decreases.21
The study showed in the Table 2, a significant increase in cortisol levels (P = 0.000). Persistent high cortisol may be caused by cortisol resistance, which leads to other problems such as hypertension and diabetes mellitus or dyslipidemia.28 Excess cortisol may cause hypertension by migrating vascular smooth muscle cells and increasing contractility of endothelial cells with impaired nitric oxide synthesis,29 cause to rise glucose level (by increased gluconeogenesis and insulin resistance) and lead to hyperlipidemia (by increased lipolysis). All of these lead to atherosclerosis and heart disease.30
The results in Table 2 refers to increase concentration of MDK (P = 0.028) in patients with atherosclerosis as compared with the control group (P = 0.029). These results agree with many other studies that have shown MDK is a marker that has been illustrated to exacerbate atherosclerosis via a variety of methods.31 MDK promote lipid accumulation in macrophages by inhibiting ATP binding cassette transporter A1 (ABCA1) which has roles in arterial narrowing through enhancing the cholesterol's out flow. ABCA1 transport cholesterol and phospholipids from macrophages to apolipoproteins that have less lipid including apolipoprotein A-I (APOA-I) and apoE, that lead form high-density lipoprotein (HDL).32 Also it stimulates VSMC to migration and conversion to foam cell, when endothelial injury, VSMCs can migrate from the media to the intima where they proliferate, resulting in neointima formation and atherosclerosis development.33 It is known as spontaneous cell death and is important in the development of tissue growth and maintenance of homeostasis within multicellular organisms, it can occur in three major effector cell types including macrophages, vascular smooth muscle and endothelial cell.34 Another important role for midkine that induced vascular inflammation that plays a central role in the pathogenesis of atherosclerosis. During atherogenesis, monocytes roll to bind with arterial wall and then transmigrate across endothelial cell a monolayer into subendothelial space for conversion into macrophages.35 Hypertension is a major cause of cerebral vascular diseases. MDK levels have positive correlation with hypertension. MDK effect in the hypertension by regulation of the renin angiotensin aldosterone system, MDK can upregulate angiotensin-converting enzyme (ACE) expression, leading to increased levels of angiotensin II, a potent vasoconstrictor that can contribute to hypertension.36
A high level of cortisol in the blood is linked to an increase in sugar, which generates the basic substance for the synthesis of cholesterol. Also, there is a relationship between cortisol and LDL, Index I, Index II, Index III, and TG, which are positive risk factors for atherosclerosis, and this is clear evidence of a relationship of high cortisol in the development of atherosclerosis by increasing the accumulation of harmful fats on the arterial walls.37 While this study shows the significant negative relationship between cortisol and good cholesterol HDL that transports lipids to the liver. MDK also shows posotive correlation with lipid profile, because it works to retain cholesterol in macrophages, and an inverse relationship with HDL due to reducing ATP binding cassette transporter A1 (ABCA1). On the other hand, the results show irregular relation between MDK and cortsol in atherosclerosis patients, The mechanism of action of each of MDK and cortisol in the development of atherosclerosis differs, and we may need other studies to prove this relationship.38
ROC curves of the analysis are plotted in Figure 2. The coordinates of ROC results and the cut-off of the concentration that produce the best sensitivities and specificities are presented in Table 4. Serum cortisol showed a sensitivity of 71 % and specificity of 76.7%, which represents the best diagnostic ability followed by MDK.
From this study it be can be concluded that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoproteins remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Faculty of Medicine, Open-Heart Institute, Al-Sadr Teaching Hospital, Najaf, Iraq.
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
Both authors took equal part in the conduct of the study and in the preparation of this manuscript.
Author affiliations:
- Furqan Moein Auda, Chemistry Department, College of Science, University of Kufa, Al Najaf, Iraq; Email: furqan.chmala@uokufa.edu.iq
- Athraa Rehman, Chemistry Department, College of Science, University of Kufa, Al Najaf, Iraq; Email: azraar.alzalemi@student.uokufa.edu.iq
ABSTRACT
Background & objective: Atherosclerosis is a condition where fat deposits cause blood arteries to stiffen and become hard instead of flexible. Many factors cause arterial stiffness, including hyperlipidemia, hypertension, hyperglycemia. In the current study, we attempted to shed light on the effect of chronic high cortisol and its relationship to early predictive indicators of atherosclerosis.
Methodology: This was a case-control study which included 60 Patient and 30 control are participated in this study. Their ages ranged between 45-70 y, all patients diagnosed with vascular diseases by ultrasound and diagnostic catheterization. Samples were taken in the morning when they were fasting, and it taken from the Open-Heart Institute, Al-Sadr Teaching Hospital, Najaf, Iraq.
Results: The study showed that patients with atherosclerosis suffer from increase in the level of cortisol, in addition to a significant increase in the concentration of midkine, cholesterol, low-density lipoprotein and atherogenic index. On the other hand, the study revealed a notable drop in the amounts of high-density lipoprotein in patients compared to the control group. Finally, we can conclude from this study that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoprotein remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis.
Conclusions: From this study it be can concluded that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoprotein remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis. Abbreviations: MDK - midkine; HDL - high density lipoprotein; LDL - low density lipoprotein; VSMC - vascular smooth muscle cells; NO - nitric oxide; TG - triglyceride; BMI - body mass index Keywords: Atherosclerosis, cortisol resistance, midkine and atherogenic index.
Citation: Auda FM, Rehman A. Evaluation of midkine, cortisol, and other biochemical indicators in patients with atherosclerosis. Anaesth. pain intensive care 2025;29(1):40-46. DOI: 10.35975/apic.v28i6.2661
Received: June 03, 2024; Reviewed: June 16, 2024; Accepted: December 29, 2025
1. INTRODUCTION
Atherosclerosis is a condition that forms gradually in blood vessels due to oxidized fat buildup on the artery's surface, although its symptoms don't always show up right away.1 There are many causes of plaque formation, including hypercholesterolemia, hypertriglyceridemia levels, hypertension, smoking, and diabetes.2 Cholesterol and triglycerides are hydrophobic and cannot move into the blood except by binding to special transporters,3 its surface is water-loving protein and the core is hydrophobic and loaded with fats such as LDL Which transports fats to cells and HDL that transports fats to the liver.4 Oxidation of LDL is caused by an increase in either internal or external oxidation agents, and elevated levels of oxidized low-density lipoprotein (oxLDL) in the blood are an essential indicator of arteriosclerosis.5,6 oxLDL blocks the action of nitric oxide a vital vasodilator, and stimulates the immune response, including recruitment of monocytes and their differentiation into phagocytosis and the formation of foam cells,7 migration and proliferation of vascular smooth muscle cells (VSMC).8 The integrity of the endothelium barrier and the retention of atherogenic LDL are impacted by the decreased expression of endothelial NO synthase and superoxide dismutase, which are in charge of preserving an effective barrier and lowering oxidative stress, respectively.9 Monocytes convert into Macrophage cells, which phagocytose and uptake oxidized lipids. They then become foam cells and, ultimately, fatty lines on the blood vessel wall.10 In addition, there are many parameters that development of atherosclerosis such as stress hormones, Cortisol a cyclic organic hormone that is the basic substance for synthesis is cholesterol. It is secreted from the adrenal gland as a result of exposure to stress.11 Following a stressful event, the pituitary gland secretes adrenocorticotropic hormone, which acts as a catalyst to produce the hormone cortisol, which increases low-density lipoprotein receptors. and boost the activity of cholesterol desmolase, the rate-limiting step in the manufacture of cortisol that transforms cholesterol to pregnenolone.12 Research indicates that prolonged stress might elevate cortisol levels, which in turn can worsen lipid hyperglycemia—a major risk factor for atherosclerosis.13 Cortisol raises blood sugar by breaking down protein in the muscles and converting them into amino acids, which the liver converts with glycerol in the process of gluconeogenesis into sugar. Also it raises blood sugar by breakdown of glycogen by glycogenolysis and converting it into sugar.14 Chronic or persistent high blood sugar leads to its conversion into lipid and storage in adipocytes. If the fat cells are full, it leads to its accumulation in the blood, which is considered an important risk factor for atherosclerosis.15 Also one of the early indicators of atherosclerosis is Midkine (MDK) is a member of the protein family that binds carbohydrates and functions as a cytokine or growth factor.16 As seen in Figure 1. MDK levels have a positive correlation with LDL-C and total cholesterol; midkine stimulates lipid accumulation in macrophages. An early stage of atherogenesis called foam cell development might result from lipid buildup in macrophages.17
The main objective of the study was to evaluate serum midkine and cortisol as specific biomarkers for early diagnosis of atherosclerosis.
2. METHODOLOGY
This is a case-control study which included sixty patients with atherosclerosis and thirty control are participated in this study. Their ages ranged between 45-70 y, all patients diagnosed with vascular diseases by ultrasound and diagnostic catheterization. Samples were taken in the morning when they were fasting, and it taken from the Al-Sadr Medical City's Open-Heart Center is located in AL-Najaf Al-Ashraf, Iraq. Patients were evaluated through a complete medical history to explore the presence of other diseases related to vascular disease which may influence this study. healthy people were chosen to serve as the control group because their age ranges were similar to the patients’. All these people were not smokers and did not suffer from vascular diseases, kidney disease, inflammation and thyroid disease.
2.1. Blood sample collection
Five milliliters of venous blood samples were drawn using a disposable needle and plastic syringes from each patient and control subjects without a tourniquet, in the morning who had fasted for 10 hours. Samples were transferred into a gel tube these samples were separated by a centrifuge at 3000 rpm for 15 min.
2.2. Serum level of cytokine and hormone
The serum levels of cortisol and midkine were measured enzymatically using the ELISA technique using ELISA kit from the PARS Biochem Company (China).
2.3. Serum level of lipid profile
Cholesterol, triglyceride and high-density lipoprotein (HDL) were determined by the spectrophotometer method using a unique kit from the Spinreact firm for each parameter (Spanish). Low density lipoprotein, very low-density lipoprotein and atherogenic index were measured mathematically.
2.4. Statistical analysis
The statistical analysis of the current study was completed using the SPSS Model 26 program, to determine the mean ± standard deviation and p-value, Excel 2016 18 was used, whereas the sensitivity of the assessed parameters was presented via a receiver operating characteristic (ROC) curve 19.
3. RESULTS
3.1. Demographic characteristics
Table 1 shows the demographic characteristics of the study population. The mean age of patients with atherosclerosis was 57.26 ± 7.29 y, which was very close to that of the controls (59.93 ± 7.35 y) with no significant difference. Also, the two groups comparable with regard to mean BMI with no significant differences.
3.2. Hormonal and cytokine profile
Table 2 shows the levels of the cortisol and midkine in patients with atherosclerosis compared to the control group, as it shows a significant increase in the levels of cortisol and midkine in patients compared to the control group.
3.3. Lipid profile and atherogenic index
Table 3 shows significant increase (P < 0.05) in total cholesterol and LDL in patients as compared with the control group. In addition, the results show significant decrease in HDL between the two groups, no significant change in TG as compared with the control group.
3.4. Correlation between all variables in atherosclerosis patients
Spearman’s correlation test was used to explore the possible correlation of all parameters in patients and controls. Cortisol displayed a significant positive correlation with all parameters except midkine and HDL. Cortisol showed a significant negative correlation with HDL. On the other hand, midkine appearance positive correlation with VLDL as shown in (Table 4).
3.5. Diagnostic value of Cortisol and Midkine
Receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of cortisol and midkine in the context of discrimination between atherosclerosis patients and healthy group. The area under the curve (AUC) of cortisol was 0.769, 95% CI = 0.645-0.893, P = 0.001. The sensitivity and specificity of the test, at cut off value = 80.9, were 71% and 72.4%, respectively.while, The sensitivity and specificity of midkine = 60,56.7 respectively as shown in (Table 5, Figure 1).
| Table 1: Comparative demographic data of the study population | |||
| Variables | Control Group
(n = 30) |
Patients Group
(n = 60) |
Sig |
| Age (y) | 59.93 ± 7.35 | 57.26 ± 7.29 | 0.164 |
| BMI (kg/m2) | 30.55 ± 3.26 | 29.41 ± 3.55 | 0.202 |
| Data presented as Mean ± SD | |||
| Table 2: Comparative hormonal and cytokine profile in two groups | |||
| Variables | Control Group
(n = 30) |
Patients Group
(n = 60) |
Sig |
| Cortisol | 69.35 ± 16.94 | 101.82 ± 43.08 | < 0.0001 |
| MK | 164.69 ± 35.69 | 198.40 ± 73.51 | 0.028 |
| Data presented as Median (Range); P < 0.05 considered as significant | |||
| Table 3: Lipid profile in patients and controls | |||
| Variables | Control Group
(n = 30) |
Patients Group
(n = 60) |
Sig |
| TG (mg/dL) | 169.93 ± 64.39 | 166.31 ± 70.91 | 0.837 |
| HDL (mg/dL) | 66.60 ± 27.63 | 29.23 ± 11.43 | 0.000 |
| CHO (mg/dL) | 155.03 ± 37.04 | 226.88 ± 63.26 | 0.000 |
| LDL (mg/dL) | 114.89 ± 33.61 | 165.71 ± 65.69 | 0.000 |
| VLDL (mg/dL) | 34.49 ± 12.61 | 48.02 ± 16.38 | 0.001 |
| Index I | 2.91 ± 1.87 | 11.11 ± 10.98 | 0.000 |
| Index II | 2.20 ± 1.735 | 8.67 ± 10.06 | 0.001 |
| Index III | 3.26 ± 2.493 | 8.32 ± 10.37 | 0.012 |
| Data presented as mean ± SD; P < 0.05 was considered as significant | |||
4. DISCUSSION
The results in the Table 1 indicate that there was no significant difference in age and body mass index (BMI) between patients and controls. While the results in Table 2 indicate a significant increase in cholesterol, low density lipoprotein (LDL), very low density lipoprotein (vLDL), Index I, Index II, Index III results are consistent with many earlier studies, where it was shown that lipid is the important risk factor of atherosclerosis,20 Cholesterol is the most closely linked to heart disease. It is hydrophobic, so it binds to lipoproteins to can travel through the blood, such as (HDL, LDL,VLDL, Chylomicron),21 increase in the level of LDL in the body with the presence of internal or external oxidation factors that lead to its conversion LDL into OXLDL,22 which is deposited on the artery wall, so the immune cells (macrophages) devour it through the process of phagocytosis, which then turns into foam cell and then lead to atherosclerosis such as this studies.23
| Table 4: Spearman’s correlation of variables in atherosclerosis patients | |||||||||||
| Variables | TG | HDL | CHO | LDL | VLDL | IndexI | IndexII | IndexIII | CHORT | MDK | |
| TG | Pearson Correlation | 1 | -.467** | .471** | .429* | .252 | .681** | .647** | .729** | .762** | .242 |
| Sig. | .009 | .009 | .018 | .179 | .000 | .000 | .000 | .000 | .198 | ||
| HDL | Pearson Correlation | -.467** | 1 | -.729** | -.777** | -.165 | -.762** | -.723** | -.623** | -.544** | -.156 |
| Sig. | .0090 | .0000 | .0000 | .3830 | .0000 | .0000 | .0000 | .0020 | .4110 | ||
| CHO | Pearson Correlation | .471** | -.729** | 1 | .945** | .109 | .626** | .578** | .464** | .508** | .249 |
| Sig | .009 | .000 | .000 | .565 | .000 | .001 | .010 | .004 | .185 | ||
| LDL | Pearson Correlation | .429* | -.777** | .945** | 1 | .102 | .689** | .671** | .535** | .418* | .230 |
| Sig. | .0180 | .0000 | .0000 | .5930 | .0000 | .0000 | .0020 | .0220 | .2210 | ||
| VLDL | Pearson Correlation | .252 | -.165 | .109 | .102 | 1 | .462* | .447* | .517** | .552** | .355 |
| Sig. | .1790 | .3830 | .5650 | .5930 | .0100 | .0130 | .0030 | .0020 | .0540 | ||
| Index I | Pearson Correlation | .681** | -.762** | .626** | .689** | .462* | 1 | .992** | .966** | .679** | .268 |
| Sig. | .0000 | .0000 | .0000 | .0000 | .0100 | .0000 | .0000 | .0000 | .1530 | ||
| Index II | Pearson Correlation | .647** | -.723** | .578** | .671** | .447* | .992** | 1 | .971** | .634** | .264 |
| Sig. | .000 | .000 | .001 | .000 | .013 | .000 | .000 | .000 | .159 | ||
| Index III | Pearson Correlation | .729** | -.623** | .464** | .535** | .517** | .966** | .971** | 1 | .693** | .269 |
| Sig. | .000 | .000 | .010 | .002 | .003 | .000 | .000 | .000 | .150 | ||
| Cortisol | Pearson Correlation | .762** | -.544** | .508** | .418* | .552** | .679** | .634** | .693** | 1 | .276 |
| Sig. | .0000 | .0020 | .0040 | .0220 | .0020 | .0000 | .0000 | 0.000 | .1390 | ||
| MDK | Pearson Correlation | .242 | -.156 | .249 | .230 | .355 | .268 | .264 | .269 | .276 | 1 |
| Sig. | .1980 | .4110 | .1850 | .2210 | 0.054 | .1530 | 0.159 | .1500 | .1390 | ||
| * Correlation is significant at the 0.05 level; ** Correlation is significant at the 0.01 level | |||||||||||
| Table 5: Receiver operating characteristic analysis of cortisol and midkine as diagnostic markers for atherosclerosis | ||||||
| Item | Cut off | Sensitivity | Specificity | AUC | 95% CI of AUC | P Value |
| Cortisol | 80.92225 | 71 | 72.4 | 0.769 | 0.645-0.893 | 0.001 |
| MK | 168.23975 | 60. | 56.7 | 0.621 | 0.477-0.765 | 0. 109 |
When good cholesterol is low, the risk of developing atherosclerosis increases due to a defect in the reverse transport of cholesterol and a weak protective role of crystallized good cholesterol in reducing the oxidation of other lipoproteins,24 high bad cholesterol and low good cholesterol are due to a person following an unhealthy lifestyle,25 such as not exercising, smoking,26 or eating large amounts of carbohydrates and starches.27 The study data in Table 2 shows that there was no significant increase in the level of triglycerides (P = 0.837) in patients with atherosclerosis, which may be due to the patients taking lipid-lowering treatments, such as statins. Niacin (nicotinic acid) decreases TG levels by up to 30-40%, or may be due to patients following a healthy diet or intermittent fasting according to the doctor’s instructions to reduce triglycerides, as when fasting, the intestine’s production of chylomicrons (these particles are highly enriched in TG and produced by the intestine) that transport triglycerides decreases.21
The study showed in the Table 2, a significant increase in cortisol levels (P = 0.000). Persistent high cortisol may be caused by cortisol resistance, which leads to other problems such as hypertension and diabetes mellitus or dyslipidemia.28 Excess cortisol may cause hypertension by migrating vascular smooth muscle cells and increasing contractility of endothelial cells with impaired nitric oxide synthesis,29 cause to rise glucose level (by increased gluconeogenesis and insulin resistance) and lead to hyperlipidemia (by increased lipolysis). All of these lead to atherosclerosis and heart disease.30
The results in Table 2 refers to increase concentration of MDK (P = 0.028) in patients with atherosclerosis as compared with the control group (P = 0.029). These results agree with many other studies that have shown MDK is a marker that has been illustrated to exacerbate atherosclerosis via a variety of methods.31 MDK promote lipid accumulation in macrophages by inhibiting ATP binding cassette transporter A1 (ABCA1) which has roles in arterial narrowing through enhancing the cholesterol's out flow. ABCA1 transport cholesterol and phospholipids from macrophages to apolipoproteins that have less lipid including apolipoprotein A-I (APOA-I) and apoE, that lead form high-density lipoprotein (HDL).32 Also it stimulates VSMC to migration and conversion to foam cell, when endothelial injury, VSMCs can migrate from the media to the intima where they proliferate, resulting in neointima formation and atherosclerosis development.33 It is known as spontaneous cell death and is important in the development of tissue growth and maintenance of homeostasis within multicellular organisms, it can occur in three major effector cell types including macrophages, vascular smooth muscle and endothelial cell.34 Another important role for midkine that induced vascular inflammation that plays a central role in the pathogenesis of atherosclerosis. During atherogenesis, monocytes roll to bind with arterial wall and then transmigrate across endothelial cell a monolayer into subendothelial space for conversion into macrophages.35 Hypertension is a major cause of cerebral vascular diseases. MDK levels have positive correlation with hypertension. MDK effect in the hypertension by regulation of the renin angiotensin aldosterone system, MDK can upregulate angiotensin-converting enzyme (ACE) expression, leading to increased levels of angiotensin II, a potent vasoconstrictor that can contribute to hypertension.36
A high level of cortisol in the blood is linked to an increase in sugar, which generates the basic substance for the synthesis of cholesterol. Also, there is a relationship between cortisol and LDL, Index I, Index II, Index III, and TG, which are positive risk factors for atherosclerosis, and this is clear evidence of a relationship of high cortisol in the development of atherosclerosis by increasing the accumulation of harmful fats on the arterial walls.37 While this study shows the significant negative relationship between cortisol and good cholesterol HDL that transports lipids to the liver. MDK also shows posotive correlation with lipid profile, because it works to retain cholesterol in macrophages, and an inverse relationship with HDL due to reducing ATP binding cassette transporter A1 (ABCA1). On the other hand, the results show irregular relation between MDK and cortsol in atherosclerosis patients, The mechanism of action of each of MDK and cortisol in the development of atherosclerosis differs, and we may need other studies to prove this relationship.38
ROC curves of the analysis are plotted in Figure 2. The coordinates of ROC results and the cut-off of the concentration that produce the best sensitivities and specificities are presented in Table 4. Serum cortisol showed a sensitivity of 71 % and specificity of 76.7%, which represents the best diagnostic ability followed by MDK.
5. CONCLUSION
From this study it be can be concluded that patients with atherosclerosis may have cortisol resistance, although patients continue to take treatment, the levels of midkine, cholesterol, and low-density lipoproteins remain high in patients with atherosclerosis. On the other hand, cortisol is considered more sensitive than midkine for diagnosing atherosclerosis.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Faculty of Medicine, Open-Heart Institute, Al-Sadr Teaching Hospital, Najaf, Iraq.
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
Both authors took equal part in the conduct of the study and in the preparation of this manuscript.
10. REFERENCES
- Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524-33. [PubMed] DOI: 1038/s41586-021-03392-8
- Lechner K, von Schacky C, McKenzie AL, Worm N, Nixdorff U, Lechner B, et al. Lifestyle factors and high-risk atherosclerosis: Pathways and mechanisms beyond traditional risk factors. Eur J Prev Cardiol. 2020;27(4):394-406. [PubMed] DOI: 1177/2047487319869400
- Mahdi B, Auda FM, editors. Study the relationship between zinc transporter 8 and others parameters in atherosclerosis patients. AIP Conf Proc. AIP Publishing; 2024.
- Rafieian-Kopaei M, Setorki M, Doudi M, Baradaran A, Nasri H. Atherosclerosis: process, indicators, risk factors and new hopes. Int J Prev Med. 2014;5(8):927. [PubMed]
- Busatto S, Walker SA, Grayson W, Pham A, Tian M, Nesto N, et al. Lipoprotein-based drug delivery. Adv Drug Deliv Rev. 2020;159:377-90. [PubMed] DOI: 1016/j.addr.2020.08.003
- Al-Hakeim HK, Auda FM, Ali BM. Lack of correlation between non-labile iron parameters, total carbonyl and malondialdehyde in major thalassemia. J Clin Biochem Nutr. 2014;55(3):203-6. [PubMed] DOI: 3164/jcbn.14-24
- Auda FM, Ali BM, Al-Andaleb M, Abidali MK, Dhyaa S. Estimation of Hepcidin and Sexual Hormones Levels in Patients with Atherosclerosis in Al-Najaf City/Iraq. Indian J Forensic Med Toxicol. 2021;15(3):16264. DOI: 37506/ijfmt.v15i3.16264
- Zakiev ER, Sukhorukov VN, Melnichenko AA, Sobenin IA, Ivanova EA, Orekhov AN Lipid composition of circulating multiple-modified low density lipoprotein. Lipids Health Dis. 2016;15:134. [PubMed] DOI: 1186/s12944-016-0308-2
- Malekmohammad K, Bezsonov EE, Rafieian-Kopaei M. Role of lipid accumulation and inflammation in atherosclerosis: focus on molecular and cellular mechanisms. Front Cardiovasc Med. 2021;8:707529. [PubMed] DOI: 3389/fcvm.2021.707529
- Maiolino G, Rossitto G, Caielli P, Bisogni V, Rossi GP, Calò LA. The role of oxidized low-density lipoproteins in atherosclerosis: the myths and the facts. Mediators Inflamm. 2013:714653. [PubMed] DOI: 1155/2013/714653
- Risan TZ, Ali BM. Study the Effect of Amphetamine on the Immune System and Liver Function. HIV Nurs. 2023;23(3):896-9.
- Finkielstain GP, Jha S, Merke D. Adrenal disorders. Biochem Mol Basis Pediatr Dis. 2021:267-96. DOI: 1016/B978-0-12-817962-8.00008-1
- Whitworth JA, Williamson PM, Mangos G, Kelly JJ. Cardiovascular consequences of cortisol excess. Vasc Health Risk Manag. 2005;1(4):291-9. [PubMed] DOI: 2147/vhrm.2005.1.4.291
- Ahmed S, Soliman A, De Sanctis V, Alyafie F, Alaaraj N, Hamed N, et al. Defective cortisol secretion in response to spontaneous hypoglycemia but normal cortisol response to ACTH stimulation in neonates with hyperinsulinemic hypoglycemia (HH). Acta Bio Med. 2021;92(2):11396. [PubMed] DOI: 23750/abm.v92i2.11396
- Lamharzi N, Renard CB, Kramer F, et al. Hyperlipidemia in concert with hyperglycemia stimulates the proliferation of macrophages in atherosclerotic lesions: potential role of glucose-oxidized LDL. Diabetes. 2004;53(12):3217-25. [PubMed] DOI: 2337/diabetes.53.12.3217
- Majaj M, Weckbach LT. Midkine—A novel player in cardiovascular diseases. Front Cardiovasc Med. 2022;9:1003104. [PubMed] DOI: 3389/fcvm.2022.1003104
- Zhang ZZ, Wang G, Yin SH, Yu XH. Midkine: A multifaceted driver of atherosclerosis. Clin Chim Acta. 2021;521:251-7. [PubMed] DOI: 1016/j.cca.2021.07.024
- Abbas ZK, Auda FM, Ali BM, Hamzah AA. Study the relationship between Vitamin D, Vitamin D binding protein (VDBP) and Electrolyte with T-score in Osteoporosis and Osteopenia patients in AL-Najaf city/Iraq. [FreeFullText]
- Auda FM, Saleh AA, Ali DS. The frequency of 6 beta-thalassemia mutations in the Iraqi patients from Najaf province. Gene Rep. 2019;17:100516. DOI: 1016/j.genrep.2019.100516
- Jebari-Benslaiman S, Galicia-García U, Larrea-Sebal A, Olaetxea JR, Alloza I, Vandenbroeck K, et al. Pathophysiology of atherosclerosis. Int J Mol Sci. 2022;23(6):3346. [PubMed] DOI: 3390/ijms23063346
- Sekhar MS, Marupuru S, Reddy BS, Kurian , Rao M, Marupuru S. Physiological role of cholesterol in human body. Dietary Sugar Salt Fat Hum Health. 2020:453-81. DOI: 1016/B978-0-12-816918-6.00021-4
- Auda A, Furqan M. Evaluate some biochemical changes associated with chronic renal failure patients undergoing hemodialysis in al najaf al ashraf governorate. Int J Sci Res Publ. 2014;4(11). [FreeFullText]
- Khatana C, Saini NK, Chakrabarti S, Saini V, Sharma A, Saini RV, et al. Mechanistic insights into the oxidized low-density lipoprotein-induced atherosclerosis. Oxid Med Cell Longev. 2020:5245308. [PubMed] DOI: 1155/2020/5245308
- Poznyak AV, Kashirskikh DA, Sukhorukov VN, et al. Cholesterol transport dysfunction and its involvement in atherogenesis. Int J Mol Sci. 2022;23(3):1332. [PubMed] DOI: 3390/ijms23031332
- Risan TZ, Ali BM, editors. Study the effect of amphetamine on neurotransmitter factors in abusers individuals. AIP Conf Proc: AIP Publishing; 2024.
- Ali BM, Moein F, AlAndaleb M, Hussein Z, Abidali MK, Dhyaa S. Study of some factors affecting in myocardial infarction. Ann Rom Soc Cell Biol. 2021;25(6):14454-9. [FreeFullText]
- Acosta S, Johansson A, Drake I. Diet and lifestyle factors and risk of atherosclerotic cardiovascular disease—a prospective cohort study. Nutrients. 2021;13(11):3822. [PubMed] DOI: 3390/nu13113822
- Ali LBM, Alasadi IJB, Zearah SA. Determination of Some Biomarkers that affect in Behaviors of Spectrum Disorder Individuals in Iraq. Indian J Forensic Autism Med Toxicol. 2020;14(2):1681-6. DOI: 37506/ijfmt.v14i2.3175
- Ali BM, Alassadi P, Iqbal J, Zearah SA. Study the effect of antioxidants and oxidative products and their genetic effect on methionine synthase in people with autism spectrum disorder. Int J Res Appl Sci Biotechnol. 2020;6(6). [FreeFullText]
- Ortiz R, Kluwe B, Odei JB, Echouffo Tcheugui JB, Sims M, Kalyani RR, et al. The association of morning serum cortisol with glucose metabolism and diabetes: The Jackson Heart Study. Psychoneuroendocrinology. 2019;25:232-9. [PubMed] DOI: 1016/j.psyneuen.2018.12.237
- Weckbach LT, Preissner KT, Deindl E. The role of midkine in arteriogenesis, involving mechanosensing, endothelial cell proliferation, and vasodilation. Int J Mol Sci. 2018;19(9):2559. [PubMed] DOI: 3390/ijms19092559
- Ou HX, Huang Q, Liu CH, Xiao J, Lv YC, Li X, Lei LP, et al. Midkine inhibits cholesterol efflux by decreasing ATP-binding membrane cassette transport protein A1 via AMPK/mTOR signaling in macrophages. Circ J. 2020;84(2):217-25. [PubMed] DOI: 1253/circj.CJ-19-0430
- T Takemoto Y, Horiba M, Harada M, Sakamoto K, Takeshita K, Murohara T, et al. Midkine promotes atherosclerotic plaque formation through its pro-inflammatory, angiogenic and anti-apoptotic functions in apolipoprotein E-knockout mice. Circ J. 2017;82(1):19-27. [PubMed] DOI: 1253/circj.CJ-17-0043
- Ball RY, Stowers EC, Burton JH, Cary NR, Skepper JN, Mitchinson MJ. Evidence that the death of macrophage foam cells contributes to the lipid core of atheroma. Atherosclerosis. 1995;114(1):45-54. [PubMed] DOI: 1016/0021-9150(94)05463-s
- Shin DH, Jo JY, Kim SH, Choi M, Han C, Choi BK, et al. Midkine is a potential therapeutic target of tumorigenesis, angiogenesis, and metastasis in non-small cell lung cancer. Cancers. 2020;12(9):2402. [PubMed] DOI: 3390/cancers12092402
- Ali BM, Mohammed UJ. The association of atherosclerosis with cortisol and alpha-enolase levels and lipid profile. Anaesth Pain Intensive Care. 2024;28(6):1097-1104. [FreeFullText]
- Fantidis P, Eladio S, Ibrahim T, Tomas P, Antonio CJ, Ramón GJ. Is there a role for cortisol in the accumulation of lipids in the intima a crucial step of atherogenesis? Curr Vasc Pharmacol. 2015;13(5):587-93. [PubMed] DOI: 2174/1570161112666141127163307