Muhamad Rafiqi Hehsan 1, Suki Ismet 2
Authors affiliations;
Ingestion of foreign bodies is a common emergency in pediatrics, but cases where foreign bodies are found adhered to the tonsils are rare. They require prompt identification and management to avoid dire consequences. This condition can lead to a spectrum of clinical presentations, ranging from asymptomatic passage to respiratory compromise. We present a case report of a 7-year-old girl who complained of persistent odynophagia in the throat region. Before that, she had taken a famous and viral jelly ball, and she only complained of pain and a sharp sensation in her throat after some time. On her initial visit to the otorhinolaryngology (ORL) clinic, nothing was found, but her symptoms persisted. So, the patient was seen again in the ORL clinic. She was planned for an examination under general anesthesia due to her being uncooperative during awake throat examination.
During the examination, a fine, thin wooden splinter, about 1 cm in length, was seen stuck at the posterior inferior pole of the left tonsil. The surgeon easily removed the foreign body without much bleeding. This case report presents a unique presentation and emphasises the need for clinicians to maintain a high index of suspicion for ingestion in pediatric patients presenting with oropharyngeal symptoms. Prompt diagnosis and appropriate management strategies for foreign body cases are crucial to prevent complications such as airway obstruction or perforation.
Abbreviations: FB: foreign body, IV: intravenous, ORL: otorhinolaryngology, TCI: target-controlled infusion
Keywords: Airway; Case Report; Emergency; Foreign Body; Tonsil
Citation: Hehsan MR, Ismet S. A viral jelly ball stick stuck to a child’s tonsil: a case report. Anaesth. pain intensive care 2025;29(6):614-617. DOI: 10.35975/apic.v29i6.xxxx
Received: June 05, 2024; Revised: May 30, 2025; Accepted: May 30, 2025
Foreign bodies (FB) lodged in the oropharynx are a common presentation in emergency departments (59.2%), and most of these patients are less than 12 years of age.1 Depending on the patient's age, the anatomical location of the airway FB will influence the necessity for mechanical ventilation, with a mortality rate of 2.5%.1 While most of the cases involve food particles or other inanimate objects, occasionally, more unusual FB are encountered.1-3 Tonsillar foreign bodies are a rare presentation in clinical practice; an estimated 18.21% of the total cases, based on a recent study.4 While typically associated with accidental ingestion or aspiration of solid objects, the involvement of unusual substances in the tonsils is a rare occurrence. We present a unique case of a viral jelly ball stick adherent to the tonsil, highlighting the diagnostic challenges, management strategies, and the potential complications associated with such cases. This jelly ball is a virally trending junk food in Malaysia among children nowadays [Figure 1].

Figure 1: The picture of the jelly ball that is viral among children
We report the case of a 7-year-old girl with a weight of 21 kg who presented to our ORL clinic with complaints of discomfort and odynophagia in the throat region for five days. The patient reported no significant medical history or recent trauma to the oropharynx. She described the symptoms as a sharp and painful sensation in her throat. One week before the onset of these symptoms, she consumed many viral jelly balls, which are available with wooden sticks. She claimed that a splinter of a wooden stick got stuck in her throat. Therefore, her mother brought her to the ORL clinic for her first visit and claimed that the FB had been removed. She was discharged home with advice to take amoxicillin and clavulanate acid for 1 week; however, her symptoms persisted. The mother brought her child to be seen again at the ORL clinic. There was no recent upper respiratory tract infection, no fever, no signs of respiratory distress, and she could tolerate oral intake. The patient appeared active, with her vital signs within normal limits for her age.
Examination with a flexible nasopharyngoscope, a tiny FB resembling a wooden stick was seen adherent to the left lateral pharynx, with ulceration seen at the left vallecula. However, the physician was unable to remove the FB, because the patient was uncooperative. A neck x-ray was taken, but no FB was seen. She was then admitted to the ward for an examination and the removal of the foreign body under general anesthesia (GA). In the ward, a normal fasting protocol for 6 hours was applied with an intravenous (IV) fluid of 60 mL/hr based on the Holliday-Segar formulation. The antibiotic was continued with inj amoxicillin clavulanate 533 mg (25 mg/kg) TDS IV. Her routine investigations were unremarkable.
Anesthetic management continued intraoperatively. She was pre-oxygenated with 8 L/min of 100% oxygen for 3 to 5 min prior to intubation. After checking the patency of IV access, target-controlled infusion (TCI) of propofol (pharmacokinetic model Kataria) was started at 4 µg/mL, then increasing to 6 µg/mL till loss of consciousness, and remifentanil (pharmacokinetic model mass rate) starting from 0.3 µg/kg/min and increasing to 0.5 µg/kg/min. Prior to intubation, the rocuronium 25 mg (1.2 mg/kg) was given IV. She was intubated with a PVC endotracheal tube with an internal diameter (ID) of 5 mm and anchored at 15 cm. After intubation, dexamethasone 2 mg was administered for postoperative nausea and vomiting (PONV) prophylaxis.
The surgical intervention by the ORL team started by inserting the rigid bronchoscope. FB was a very thin piece of a wooden stick at the postero-inferior pole of the left tonsil [Figure 2]. The foreign body, which measured about 1 cm in length, was firmly stuck to the left tonsillar crypt and was removed (Figures 3, 4). Upon further inspection, there was only minimal slough at the base of the tongue. The operation lasted for about an hour. Hemodynamically, the patient remained stable and had no episodes of desaturation. The anesthesia was reversed by neostigmine 0.8 mg combined with atropine 0.4 mg after the completion of the procedure. Postoperatively, the patient was observed in the recovery bay, and vital signs were charted. Her systolic blood pressure (SBP) remained 90–100 mmHg, diastolic blood pressure (DBP) at 60–70 mmHg, the heart rate between 80 and 110 beats/min, and the oxygen saturation (SpO2) remained 99% with oxygen 5 L/min. There was no episode of desaturation before transfer back to the pediatric ORL ward. Postoperative recovery was uneventful, with an immediate relief of symptoms. The next day, the patient was discharged home with oral analgesics and advised to maintain good oral hygiene.
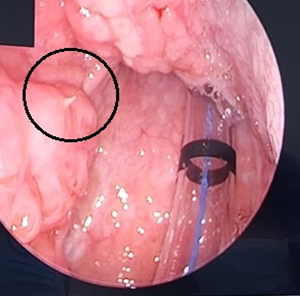
Figure 2: A fine, thin wooden splinter at the posterior inferior pole of the left tonsil (black circle).
Ingestion of foreign bodies among the pediatric population is common, and the highest number of patients have been less than 2 years of age.1,5 The types of foreign bodies vary between different countries and geographic locations, which may be likely due to diverse sociocultural and dietary factors. In the United States, coins are the most frequently swallowed foreign body that requires intervention; in other nations, food-related foreign bodies, such as fish bones, are more common.1,5 The symptoms of foreign body ingestion vary from gastrointestinal symptoms such as abdominal pain and vomiting to respiratory symptoms like coughing and stridor.5 There are three stages to the typical signs and symptoms of aspirating a FB; a history of choking episodes in the early stages, followed by paroxysms of coughing, gagging, and episodes of airway distress ranging from mild to severe airway obstruction.3 The asymptomatic interval is the second stage, while the complication symptoms characterize the third stage. Unfortunately, the chronological three phases were not observed in this case. This patient's main complaint was odynophagia, as she described the symptoms as a sharp and painful sensation in her throat. Therefore, this vague symptom led the treating physician to miss such a case.
An immediate evaluation of the airway is necessary in cases of suspected FB ingestion. The majority of FB ingestions are often removed in outpatient clinics.1 However, in this case, the symptoms of odynophagia persisted, despite an ORL clinic visit. The ingested FB can be identified visually or endoscopically.1 Plain x-ray imaging is the first modality of choice due to its ability to detect most of FB rapidly, cost-effectively, and with minimal radiation exposure.6
As the radiological x-ray findings were negative, she then proceeded with flexible nasopharyngoscopy under GA was subsequently performed, and the FB was confirmed and seen at the posterior inferior pole of the left tonsil. Most commonly, the ingested FB are removed endoscopically, especially those lodged in the oesophagus.5 FB lodged in the airways is linked to significant morbidity, and prompt detection and removal is crucial as certain FB may erode through the GI tract and cause complications, if the object perforates or migrates.3, 5 Complications associated with tonsillar foreign bodies include secondary infection, abscess formation, and airway compromise, emphasizing the importance of prompt diagnosis and intervention.1-3
We used total intravenous anesthesia (TIVA) during the procedure, because it is the anesthesia method of choice recommended, especially for bronchoscopy cases.7, 8 In an ideal situation, bispectral index (BIS) monitoring would be the best monitoring during the TIVA method for patients at risk for intraoperative awareness, with the goal being to achieve a BIS index between 40 and 60.7, 8 However, due to the short duration of the procedure, it would not be cost-effective to apply BIS monitoring in this case. There is a synergistic interaction between propofol and opioids; therefore, we used propofol and remifentanil as drugs of choice for TIVA.8 Opioids reduce the volume of propofol required for achieving unconsciousness and, more specifically, to obtund movement and the hemodynamic reaction to unpleasant stimuli.7, 8 Propofol is a short-acting intravenous hypnotic drug with fast onset, a short half-life, and a high body clearance, providing rapid recovery from anesthesia.7 Remifentanil is a potent, short-acting narcotic that offers profound analgesia, suppresses airway reflexes, and has a minimal impact on cognitive function.7
Communication between the multidisciplinary team, including the ORL team and the anesthesiologists, is essential before the procedure to establish the plan of action.5 Most FB extractions are being performed under GA.1,2,5 The endotracheal intubation was performed to prevent aspiration and protect the airway from FB. In this case, the neuromuscular blocking agent was given so that the patient could relax for an easy removal of FB to minimize the complications. Some anesthetists prefer spontaneous ventilation to the controlled ventilation technique.7, 8 We used controlled ventilation to improve oxygenation and overcome the increase in airway resistance during the bronchoscopy. However, a recent meta-analysis does not show a preference for either spontaneous or controlled ventilation, although there is a lower incidence of laryngospasm when controlled ventilation is used.9
In conclusion, healthcare providers should maintain a high index of suspicion for an unusual FB in patients presenting with oropharyngeal discomfort. Prompt recognition, thorough investigation, diagnosis, and tailored management are essential for achieving optimal outcomes in such cases. Vigilance in history-taking and clinical examination, coupled with appropriate imaging and bronchoscopy techniques, is essential. Good and effective communication between the multidisciplinary team would also help in managing the case and ensuring safety.
5. Conflict of interest
All authors declare that there was no conflict of interest.
6. Ethical considerations
The study complied with the contemporary ethical guidelines for dealing with such patients and publishing reports based on their disease and the management. Written informed consent was obtained from the father of the child.
7. Acknowledgement
Special thanks to Universiti Sains Malaysia for the financial assistance through Short Term Grant R501-LR-RND002-0000000333-0000
8. Authors’ contribution
MRH: Literature review, manuscript writing
SI: Conducted the case, final approval of manuscript
Authors affiliations;
- Muhamad Rafiqi Hehsan, Department of Anesthesiology & Critical Care, School of Medical Sciences, Health Campus, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia / Faculty of Medicine, Universiti Sultan Zainal Abidin, Medical Campus, Jalan Sultan Mahmud, 20400 Kuala Terengganu, Terengganu Darul Iman, Malaysia; Email: muhamad_rafiqi@yahoo.com
- Suki Ismet, Department of Anesthesiology & Critical Care, School of Medical Sciences, Health Campus, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia; Email: sukiismet@usm.my
ABSTRACT
Ingestion of foreign bodies is a common emergency in pediatrics, but cases where foreign bodies are found adhered to the tonsils are rare. They require prompt identification and management to avoid dire consequences. This condition can lead to a spectrum of clinical presentations, ranging from asymptomatic passage to respiratory compromise. We present a case report of a 7-year-old girl who complained of persistent odynophagia in the throat region. Before that, she had taken a famous and viral jelly ball, and she only complained of pain and a sharp sensation in her throat after some time. On her initial visit to the otorhinolaryngology (ORL) clinic, nothing was found, but her symptoms persisted. So, the patient was seen again in the ORL clinic. She was planned for an examination under general anesthesia due to her being uncooperative during awake throat examination.
During the examination, a fine, thin wooden splinter, about 1 cm in length, was seen stuck at the posterior inferior pole of the left tonsil. The surgeon easily removed the foreign body without much bleeding. This case report presents a unique presentation and emphasises the need for clinicians to maintain a high index of suspicion for ingestion in pediatric patients presenting with oropharyngeal symptoms. Prompt diagnosis and appropriate management strategies for foreign body cases are crucial to prevent complications such as airway obstruction or perforation.
Abbreviations: FB: foreign body, IV: intravenous, ORL: otorhinolaryngology, TCI: target-controlled infusion
Keywords: Airway; Case Report; Emergency; Foreign Body; Tonsil
Citation: Hehsan MR, Ismet S. A viral jelly ball stick stuck to a child’s tonsil: a case report. Anaesth. pain intensive care 2025;29(6):614-617. DOI: 10.35975/apic.v29i6.xxxx
Received: June 05, 2024; Revised: May 30, 2025; Accepted: May 30, 2025
1. INTRODUCTION
Foreign bodies (FB) lodged in the oropharynx are a common presentation in emergency departments (59.2%), and most of these patients are less than 12 years of age.1 Depending on the patient's age, the anatomical location of the airway FB will influence the necessity for mechanical ventilation, with a mortality rate of 2.5%.1 While most of the cases involve food particles or other inanimate objects, occasionally, more unusual FB are encountered.1-3 Tonsillar foreign bodies are a rare presentation in clinical practice; an estimated 18.21% of the total cases, based on a recent study.4 While typically associated with accidental ingestion or aspiration of solid objects, the involvement of unusual substances in the tonsils is a rare occurrence. We present a unique case of a viral jelly ball stick adherent to the tonsil, highlighting the diagnostic challenges, management strategies, and the potential complications associated with such cases. This jelly ball is a virally trending junk food in Malaysia among children nowadays [Figure 1].
Figure 1: The picture of the jelly ball that is viral among children
2. CASE REPORT
We report the case of a 7-year-old girl with a weight of 21 kg who presented to our ORL clinic with complaints of discomfort and odynophagia in the throat region for five days. The patient reported no significant medical history or recent trauma to the oropharynx. She described the symptoms as a sharp and painful sensation in her throat. One week before the onset of these symptoms, she consumed many viral jelly balls, which are available with wooden sticks. She claimed that a splinter of a wooden stick got stuck in her throat. Therefore, her mother brought her to the ORL clinic for her first visit and claimed that the FB had been removed. She was discharged home with advice to take amoxicillin and clavulanate acid for 1 week; however, her symptoms persisted. The mother brought her child to be seen again at the ORL clinic. There was no recent upper respiratory tract infection, no fever, no signs of respiratory distress, and she could tolerate oral intake. The patient appeared active, with her vital signs within normal limits for her age.
Examination with a flexible nasopharyngoscope, a tiny FB resembling a wooden stick was seen adherent to the left lateral pharynx, with ulceration seen at the left vallecula. However, the physician was unable to remove the FB, because the patient was uncooperative. A neck x-ray was taken, but no FB was seen. She was then admitted to the ward for an examination and the removal of the foreign body under general anesthesia (GA). In the ward, a normal fasting protocol for 6 hours was applied with an intravenous (IV) fluid of 60 mL/hr based on the Holliday-Segar formulation. The antibiotic was continued with inj amoxicillin clavulanate 533 mg (25 mg/kg) TDS IV. Her routine investigations were unremarkable.
Anesthetic management continued intraoperatively. She was pre-oxygenated with 8 L/min of 100% oxygen for 3 to 5 min prior to intubation. After checking the patency of IV access, target-controlled infusion (TCI) of propofol (pharmacokinetic model Kataria) was started at 4 µg/mL, then increasing to 6 µg/mL till loss of consciousness, and remifentanil (pharmacokinetic model mass rate) starting from 0.3 µg/kg/min and increasing to 0.5 µg/kg/min. Prior to intubation, the rocuronium 25 mg (1.2 mg/kg) was given IV. She was intubated with a PVC endotracheal tube with an internal diameter (ID) of 5 mm and anchored at 15 cm. After intubation, dexamethasone 2 mg was administered for postoperative nausea and vomiting (PONV) prophylaxis.
The surgical intervention by the ORL team started by inserting the rigid bronchoscope. FB was a very thin piece of a wooden stick at the postero-inferior pole of the left tonsil [Figure 2]. The foreign body, which measured about 1 cm in length, was firmly stuck to the left tonsillar crypt and was removed (Figures 3, 4). Upon further inspection, there was only minimal slough at the base of the tongue. The operation lasted for about an hour. Hemodynamically, the patient remained stable and had no episodes of desaturation. The anesthesia was reversed by neostigmine 0.8 mg combined with atropine 0.4 mg after the completion of the procedure. Postoperatively, the patient was observed in the recovery bay, and vital signs were charted. Her systolic blood pressure (SBP) remained 90–100 mmHg, diastolic blood pressure (DBP) at 60–70 mmHg, the heart rate between 80 and 110 beats/min, and the oxygen saturation (SpO2) remained 99% with oxygen 5 L/min. There was no episode of desaturation before transfer back to the pediatric ORL ward. Postoperative recovery was uneventful, with an immediate relief of symptoms. The next day, the patient was discharged home with oral analgesics and advised to maintain good oral hygiene.
Figure 2: A fine, thin wooden splinter at the posterior inferior pole of the left tonsil (black circle).
3. DISCUSSION
Ingestion of foreign bodies among the pediatric population is common, and the highest number of patients have been less than 2 years of age.1,5 The types of foreign bodies vary between different countries and geographic locations, which may be likely due to diverse sociocultural and dietary factors. In the United States, coins are the most frequently swallowed foreign body that requires intervention; in other nations, food-related foreign bodies, such as fish bones, are more common.1,5 The symptoms of foreign body ingestion vary from gastrointestinal symptoms such as abdominal pain and vomiting to respiratory symptoms like coughing and stridor.5 There are three stages to the typical signs and symptoms of aspirating a FB; a history of choking episodes in the early stages, followed by paroxysms of coughing, gagging, and episodes of airway distress ranging from mild to severe airway obstruction.3 The asymptomatic interval is the second stage, while the complication symptoms characterize the third stage. Unfortunately, the chronological three phases were not observed in this case. This patient's main complaint was odynophagia, as she described the symptoms as a sharp and painful sensation in her throat. Therefore, this vague symptom led the treating physician to miss such a case.
An immediate evaluation of the airway is necessary in cases of suspected FB ingestion. The majority of FB ingestions are often removed in outpatient clinics.1 However, in this case, the symptoms of odynophagia persisted, despite an ORL clinic visit. The ingested FB can be identified visually or endoscopically.1 Plain x-ray imaging is the first modality of choice due to its ability to detect most of FB rapidly, cost-effectively, and with minimal radiation exposure.6
As the radiological x-ray findings were negative, she then proceeded with flexible nasopharyngoscopy under GA was subsequently performed, and the FB was confirmed and seen at the posterior inferior pole of the left tonsil. Most commonly, the ingested FB are removed endoscopically, especially those lodged in the oesophagus.5 FB lodged in the airways is linked to significant morbidity, and prompt detection and removal is crucial as certain FB may erode through the GI tract and cause complications, if the object perforates or migrates.3, 5 Complications associated with tonsillar foreign bodies include secondary infection, abscess formation, and airway compromise, emphasizing the importance of prompt diagnosis and intervention.1-3
We used total intravenous anesthesia (TIVA) during the procedure, because it is the anesthesia method of choice recommended, especially for bronchoscopy cases.7, 8 In an ideal situation, bispectral index (BIS) monitoring would be the best monitoring during the TIVA method for patients at risk for intraoperative awareness, with the goal being to achieve a BIS index between 40 and 60.7, 8 However, due to the short duration of the procedure, it would not be cost-effective to apply BIS monitoring in this case. There is a synergistic interaction between propofol and opioids; therefore, we used propofol and remifentanil as drugs of choice for TIVA.8 Opioids reduce the volume of propofol required for achieving unconsciousness and, more specifically, to obtund movement and the hemodynamic reaction to unpleasant stimuli.7, 8 Propofol is a short-acting intravenous hypnotic drug with fast onset, a short half-life, and a high body clearance, providing rapid recovery from anesthesia.7 Remifentanil is a potent, short-acting narcotic that offers profound analgesia, suppresses airway reflexes, and has a minimal impact on cognitive function.7
Communication between the multidisciplinary team, including the ORL team and the anesthesiologists, is essential before the procedure to establish the plan of action.5 Most FB extractions are being performed under GA.1,2,5 The endotracheal intubation was performed to prevent aspiration and protect the airway from FB. In this case, the neuromuscular blocking agent was given so that the patient could relax for an easy removal of FB to minimize the complications. Some anesthetists prefer spontaneous ventilation to the controlled ventilation technique.7, 8 We used controlled ventilation to improve oxygenation and overcome the increase in airway resistance during the bronchoscopy. However, a recent meta-analysis does not show a preference for either spontaneous or controlled ventilation, although there is a lower incidence of laryngospasm when controlled ventilation is used.9
4. CONCLUSION
In conclusion, healthcare providers should maintain a high index of suspicion for an unusual FB in patients presenting with oropharyngeal discomfort. Prompt recognition, thorough investigation, diagnosis, and tailored management are essential for achieving optimal outcomes in such cases. Vigilance in history-taking and clinical examination, coupled with appropriate imaging and bronchoscopy techniques, is essential. Good and effective communication between the multidisciplinary team would also help in managing the case and ensuring safety.
5. Conflict of interest
All authors declare that there was no conflict of interest.
6. Ethical considerations
The study complied with the contemporary ethical guidelines for dealing with such patients and publishing reports based on their disease and the management. Written informed consent was obtained from the father of the child.
7. Acknowledgement
Special thanks to Universiti Sains Malaysia for the financial assistance through Short Term Grant R501-LR-RND002-0000000333-0000
8. Authors’ contribution
MRH: Literature review, manuscript writing
SI: Conducted the case, final approval of manuscript
9. REFERENCES
- Kwon, B., Choi, Y., Kim, S. K., Hong, S. J., Kim, Y. B., & Hong, S. M. (2022). Ear, Nose, and Throat Foreign Bodies in Children: A Retrospective Study. Children (Basel, Switzerland), 9(1), 63. [PubMed] DOI: 10.3390/children9010063
- Johnson, K., Linnaus, M., & Notrica, D. (2017). Airway foreign bodies in pediatric patients: anatomic location of foreign body affects complications and outcomes. Pediatric surgery international, 33(1), 59–64. [PubMed] DOI: 10.1007/s00383-016-3988-9
- Tan, H. K., Brown, K., McGill, T., Kenna, M. A., Lund, D. P., & Healy, G. B. (2000). Airway foreign bodies (FB): a 10-year review. International journal of pediatric otorhinolaryngology, 56(2), 91–99. [PubMed] DOI: 10.1016/s0165-5876(00)00391-8
- Lin, C., Liu, D., Zhou, H., Zhang, X., Lu, L., & Gao, X. (2020). Clinical diagnosis and treatment of throat foreign bodies under video laryngoscopy. The Journal of international medical research, 48(7), 300060520940494. [PubMed] DOI: 10.1177/0300060520940494
- Conners GP, Mohseni M. Pediatric Foreign Body Ingestion. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430915/
- Campbell EA, Wilbert CD. Foreign Body Imaging. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470294/
- Galway, U.A., Zura, A., Wang, M., Deeby, M., Riter, Q., Li, T., & Ruetzler, K. (2022). Anesthetic considerations for rigid bronchoscopy: A narrative educational review. Trends in Anaesthesia and Critical Care.
- Nimmo, A. F., Absalom, A. R., Bagshaw, O., Biswas, A., Cook, T. M., Costello, A., Grimes, S., Mulvey, D., Shinde, S., Whitehouse, T., & Wiles, M. D. (2019). Guidelines for the safe practice of total intravenous anaesthesia (TIVA): Joint Guidelines from the Association of Anaesthetists and the Society for Intravenous Anaesthesia. Anaesthesia, 74(2), 211–224. [PubMed] DOI: 10.1111/anae.14428
- Liu, Y., Chen, L., & Li, S. (2014). Controlled ventilation or spontaneous respiration in anesthesia for tracheobronchial foreign body removal: a meta-analysis. Paediatric anaesthesia, 24(10), 1023–1030. [PubMed] DOI: 10.1111/pan.12469