Tamer Samir Abdelsalam Abdelaziz1, Khaled Abdou2, Marwa Salem3
Author affiliations:
Background & objective: Fascial plane blocks have emerged as one of the main parts in multimodal analgesia after major abdominal surgeries. Quadratus lumborum (QL) and erector spinae plane (ESP) blocks could cover both somatic and visceral pain, and have been extensively used by the anesthesiologists. We compared both of the blocks for effectiveness, ease to perform and safety after total abdominal hysterectomy (TAH).
Methodology: We enrolled 64 female participants undergoing TAH, ASA PS I–III, aged 40-60 y, and BMI 18-40 kg/m2. The patients were randomized equally into either Group QLB, to receive lateral QL block or Group ESPB to receive ESP block (ESPB), under ultrasound guidance, with bupivacaine bilaterally after surgery. Pain severity during rest and on coughing was measured with visual analogue scale (VAS), time to first analgesic request, total meperidine consumption as rescue analgesic, and frequency of PONV through 24 h were recorded.
Results: ESPB lowered the median VAS throughout the first 18 h with a significant difference (P < 0.001) during rest and cough than QLB. Also, ESPB lowered postoperative meperidine consumption more than the QLB group (62.50 ± 22.00 mg) vs (95.31 ± 26.52 mg) respectively with P < 0.001. ESPB prolonged the duration of analgesia over QLB (853.13 ± 50.51 min) vs (812.34 ± 67.53 min) respectively with a P = 0.008. No differences were recorded regarding PONV and hemodynamic parameters.
Conclusion: Erector spinae plane block is more effective, simple, and safe approach to multimodal analgesia after total abdominal hysterectomy than quadratus lumborum block.
Clinical trial registration No.: NCT05541588 on 15/9/2022.
Abbreviations: EOM - External oblique muscle; ESPB - Erector Spinae Plane Block; HR - Heart rate; IOM - Internal oblique muscle; LA - Local anesthetic; MAP - Mean arterial blood pressure; PACU: Post anesthesia care unit; QLB: Quadratus Lumborum Block; QL - Quadratus Lumborum muscle; TAM: transverses abdominus muscle; TAP - Transversus abdominus plane; VAS - Visual Analogue score.
Keywords: Erector spinae plane block; Hysterectomy; Postoperative pain; Quadratus lumborum block.
Citation: Abdelaziz TSA, Abdou K, Salem M. Erector spinae plane block versus quadratus lumborum block for postoperative analgesia after abdominal hysterectomy: a randomized comparative study. Anaesth. pain intensive care 2024;28(2):333−340; DOI: 10.35975/apic.v28i2.2442
Received: December 27, 2023; Revised: January 16, 2024; Accepted: January 18, 2024
Abdominal hysterectomy is a common gynecological procedure in the operating rooms due to various causes.1 The pain originates from the abdominal wall (somatic pain) and internal organs, the visceral pain that is transmitted by the autonomic nervous system, mainly by the sympathetic fibers. Adequate postoperative pain relief prevents multiple morbidity scenarios (such as thromboembolism and infection) through early mobility, fast recovery and prevents development of chronic pain.2
Multimodal analgesia for TAH consists of opioid, non-opioid analgesics, lumbar epidural, and recently fascial plane blocks, which include transversus abdominus plane (TAP) block, quadratus lumborum block (QLB), and erector spinae plane block (ESPB). Although lumbar epidural analgesia is considered the popular modality for gynecological and obstetric pain control, it has been associated with some complications; e.g., hypotension, hypovolemia, motor block, bleeding tendency, high intracranial pressure, and local infection.3
TAP block has limited analgesic efficiency and duration as it provides mainly somatic pain relief, and not the visceral pain relief.4
Quadratus Lumborum (QL) is covered anteriorly with transversalis fascia, and ventral rami of T7-L2 pass in between. There are mainly three types of QLB; QLB-I (lateral), QLB-II (posterior), and QLB-III (anterior or trans-muscular), according to the needle tip position; QLB affects ventral rami of T7 to L2, sympathetic chain, iliohypogastric, and ilioinguinal nerves. The diffusion of anesthetic agent around QL muscle to thoracolumbar paravertebral nerve fibers, is responsible for somatic and visceral pain relief. Perioperative QLB provides intra- and post-operative opioid-free analgesia for abdominal surgeries.5-8
The ESPB is a fascial plane where the anesthetic drug is injected between the ES muscle and the transverse process, the solution spreads up and down in the thoracic area covering T1-T12, with lateral spread to paravertebral and epidural space to block ventral and dorsal rami and provides extended unilateral somatic and visceral block. ESPB is gaining popularity for abdominoplasty, intra-abdominal, gynecological, and obstetric surgeries.9-11
We hypothesized that lateral QLB may be an alternative to ESPB regarding postoperative pain control, so compared both of the blocks for effectiveness, ease to perform and safety after total abdominal hysterectomy.
A prospective, randomized, comparative study started after the approval of the institutional Ethics Committee and registration at ClinicalTrials.gov between 7th July 2022 and 1st January 2023 in the university hospitals. It followed CONSORT guidelines, and all participants signed a written informed consent before the procedure.
Participants undergoing TAH, who fulfilled the inclusion criteria; e.g., ASA I–III, age 40-60 y old, and BMI 18-40 kg/m2, were randomized into the study groups using program‐generated numbers in opaque envelopes with a one-to-one ratio.
Group QLB (n = 32) received lateral quadratus lumborum block (QLB-I) under ultrasound guidance with 20 ml of bupivacaine 0.25% at each side after surgery.
Group ESPB (n = 32) received ESPB under ultrasound guidance with 20 ml of bupivacaine 0.25 % at each side after surgery.
Participants were excluded upon refusal or if they had an allergy to bupivacaine, local infection, coagulopathy, and intellectual disability. The participants, allocating staff, and follow-up residents were blinded. The preoperative assessment and the standard investigations were done for all participants.
In the operating room, standard monitoring was connected and balanced general anesthesia was administered. After surgery and before extubation, the patient was positioned laterally on her side, and under strict aseptic conditions, ultrasound guided lateral QLB or ESPB was served.
Lateral QLB
A linear probe was placed horizontally over the flanks at the mid-axillary line to identify three parallel muscles; external oblique muscle (EOM), internal oblique muscle (IOM), and transverses abdominus muscle (TAM). Then the probe was slid backwards until TAM aponeurosis; This is an ultrasound hyperechogenic sign where the QL extends posteriorly and to the inside. U/S needle 22G (80-100 mm) directed antero-posteriorly by the ‘in-plane’ technique through the muscles to the hyperechogenic sign without TAM penetration. The needle tip was placed lateral to QL, then after negative aspiration and hydro-dissection (separation of QL from fascia) with 5 ml of normal saline NS, a 20 ml bupivacaine 0.25% was given on each side.12
ESPB
A linear probe was placed longitudinally at T10 spinous process level and then slid outward till the transverse process (TP) was under the ES muscles; U/S needle 22G (80-100 mm) directed caudally by the ‘in-plane’ technique until it contacted the TP, then after negative aspiration and hydro-dissection (separation of ES muscles from the TP) with 5 ml of normal saline, a 20 ml bupivacaine 0.25% was given on each side.13
The participants were transferred to PACU after extubation and after regaining consciousness, where they were connected to standard monitoring. The sensory dermatomal block was assessed by pinprick test and failed blocks were excluded. Pain intensity was recorded during rest and on coughing using the visual analogue scale (VAS) after full recovery. After follow-up, participants were discharged with a modified Aldrete recovery score > 9.
In the ward, paracetamol was infused every 8 h regularly, and VAS score recorded at 2, 6, 12, 18, and 24 h during rest and on coughing. While IV meperidine 0.5 mg/kg was given if VAS score remained ≥ 4; inj. granisetron 1 mg was given for PONV (maximum to 3 mg per day).
The primary outcome was the pain scores during rest at 18 h postoperatively assessed by VAS. The secondary outcome were; pain scores during rest and on coughing through the first 24 h, total duration of analgesia, 24-h meperidine consumption and the frequency of PONV during 24 h.
PASS 11 software was used for sample size calculation and after reviewing Mohamed A. Ghanem et al. (2021)14 results, 32 participants in each group - a total of 64 cases - achieved a power of 80% comparing the mean pain score during rest at 18 h to detect the effect size ≥ 0.8 by independent samples t-test and 0.05 significance level; The sample was inflated by 20% to compensate for the dropouts.
Statistical Package for Social Science (SPSS) version 27.0. was used to analyze the study data, the normally distributed continuous variables are presented as mean ± standard deviation (SD), and the abnormally distributed continuous variables are presented as median and inter-quartile range, while the categorical variables are presented as numbers and percentages. Continuous data were analyzed by the student t-test for normally distributed and Mann–Whitney test for abnormally distributed data. Categorical data were analyzed by the chi-square test. A 95% confidence interval (95% CI) was used with the conduction of all tests and the margin of error accepted was set to 5%. So, a P < 0.05 was significant.
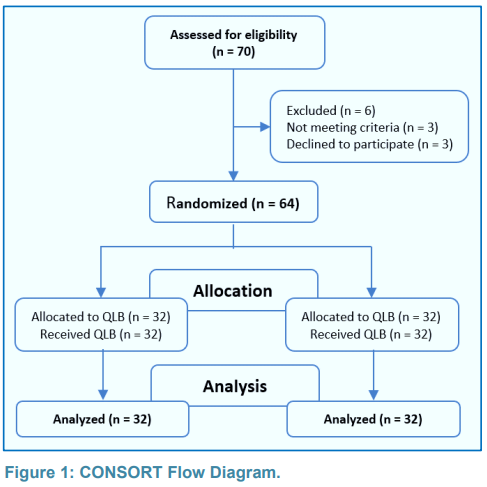
Seventy participants were screened with six exclusions (3 didn’t fulfil the criteria and 3 refused). The 64 participants were randomized into two equal groups and their data were analyzed at the end of the study (Figure 1).
No differences regarding demographic data (age, BMI, ASA), operative time, and hemodynamic parameters (HR and MAP) were found between groups with P > 0.05 (Table 1).
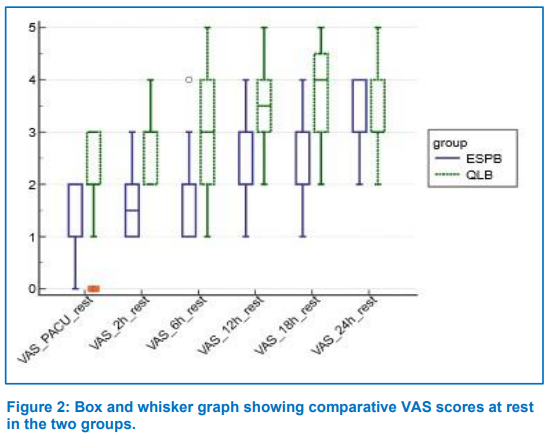
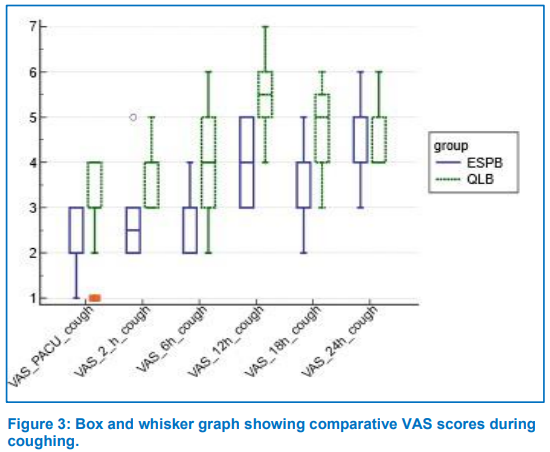
The results showed significant differences in VAS scores during rest (Figure 2) and with cough (Figure 3) at 0, 2, 6, 12, 18 h with lower values in the ESPB group (P < 0.001) (Table 3); Moreover, the duration of analgesia in ESPB group was longer than QLB group (853.13 ± 50.51 vs 812.34 ± 67.53 min respectively) (P = 0.008) and post-operative meperidine consumption was lower in ESPB group than QLB group (62.50 ± 22.00 vs 95.31 ± 26.52 mg respectively) (P < 0.001) (Table 2).
There were no statistical differences between groups regarding PONV (Table 2) and no cases of organ injury or local anesthetic toxicity were recorded throughout the study.
We compared the efficacy of lateral QLB with ESPB on post-abdominal hysterectomy pain severity during rest and on movement (coughing), and found a reduction in the VAS scores up to 18 h in ESPB group with lower narcotic consumption at 24 h in comparison to QLB group. The differences in analgesic duration between ESPB and QLB were not clinically significant (853.13 ± 50.51 vs 812.34 ± 67.53 min respectively). Also, no difference regarding PONV, and no cases of any injury or local anesthetic toxicity were recorded.
TAH is a common daily procedure in the operating room.1 The pain originates from the abdominal wall (somatic pain) and internal organs [visceral pain that is transmitted by the autonomic nervous system mainly sympathetic fibers]; Multi-modal analgesia protocols involve ultrasound-guided fascial plane blocks (as transversus abdominus, quadratus lumborum, and erector spinae) to provide opioid-sparing analgesia.3 Postoperative pain relief prevents multiple morbidity scenarios (such as thromboembolism and infection) through early mobility and fast recovery.2
The ESPB is a fascial plane where the anesthetic drug is injected between the ES muscle and the transverse process, the solution extends up and down in the thoracic area covering T1-T12, with lateral spread to paravertebral and epidural space to block ventral and dorsal rami and provides extended unilateral somatic and visceral block.9,10 ESPB at the T10 level could block pain sensation from T5 till L2,15 and cover the visceral sensation of the uterus (T11-T12).16 So, we chose the level of T10 block for this study.
ESPB is gaining popularity for abdominoplasty, intra-abdominal, gynecological, and obstetric surgeries,9-11 and many studies showed sufficient analgesic effect and lower opioid consumption with ESPB in many surgeries as bariatric surgeries, laparotomy, nephrectomy, hernia repair, hysterectomy, and laparoscopy.11,17-21 During the first postoperative 24 h the ESPB lowered the consumption of rescue analgesic compared to QLB.
Ghanem and his colleagues compared the analgesic effects of QLB III and ESPB in colorectal cancer surgeries and found that ESPB lowered pain scores during rest and cough and reduced total narcotic consumption with no differences in the time of first analgesic request, in agreement with our result. Although pain severity was high in QLB than our results but still it was statistically significant, mostly due to dermatomal coverage and excessive surgical manipulation of viscera in colorectal surgery compared with hysterectomy.14
Abd Ellatif and Abdelnaby conducted a controlled trial and found that the QLB III is as efficient as ESPB in providing analgesia and decreasing perioperative opioid consumption after nephrectomy.22 The large skin incisions and muscle cutting cause 75% of postoperative pain (somatic pain) that are fully blocked by ESPB and QLB.23 The same findings were reported by Jiang and his colleagues who compared ESPB and QLB III against control in laparoscopic hysterectomy.24 The different results might be due to less surgical manipulation in laparoscopy and the different QLB techniques.
The diffusion of anesthetic agent around QL muscle to thoracolumbar paravertebral nerve fibers is responsible for somatic and visceral pain relief.25 Perioperative QLB provides intra- and post-operative opioid-free analgesia for abdominal surgeries.5-8 After reviewing the previous literature regarding QLB for abdominal surgeries, no sufficient evidence at the time prefers a specific QL technique over the others for specific surgery.5,8,26,27 So, lateral QLB technique was preferred in this study, being a simple, easy, and fast approach. Additionally, it could be accessed in supine position.
Many trials compared the different techniques of QL against TAP block or control group for intra and postoperative pain, analgesic duration, and narcotic consumption after abdominal, gynecological, and obstetric procedures, where QLB showed better pain control, longer duration of analgesia, and less narcotic requirements, partially in line with our results as median VAS scores were ≤ 4 at all-time points during rest and till 6 h on coughing. 28-31 Moreover, the first analgesic requested was at 812.34 ± 67.53 min. Also, a comparative study between QLB and paravertebral block for radical cystectomy showed similar analgesic effects with no differences in opioid consumption.32 Krohg et al. and Mieszkowski et al. compared lateral QLB against the control group following cesarean section and reported lower pain scores including somatic and visceral pain, less narcotic consumption, and longer analgesia.26,27
Finally, after reviewing the previous literature regarding ESPB and QLB for abdominal surgeries, ESPB showed reduction of pain scores, delayed time to first analgesic request, and lower narcotic consumption regardless of the surgery, while QLB showed different results even with the same technique.
Our study includes the lack of a controlled group, the small sample size, and the lack of optimal local anesthetic volume. Further studies are required to determine the proper spread of LA in live participants, not a cadaver, for QLB techniques and the best technique for each procedure.
The results of our prospective, randomized, comparative study show that erector spinae plane block is an effective, simple, and safe approach to multimodal analgesia after total abdominal hysterectomy.
7. Ethical issues
Written informed consent for participation and publication was obtained from all participants.
8. Availability of data
All numerical data generated during the course of this study is available upon reasonable request.
9. Conflict of interest
The authors declare that no potential conflict of interest relevant to this article was reported. The study was conducted using institutional resources.
10. Authors' contribution
TA: data analysis, results interpretation, writing discussion, preparing manuscript, and journal submission.
KA: study conception, design, data collection, data analysis, results interpretation, and writing discussion.
MS: study conception, design, data collection, and writing discussion.
The manuscript and results were reviewed and approved by all authors.
Author affiliations:
- Tamer Samir Abdelsalam Abdelaziz, MD, Lecturer of Anesthesia and Intensive Care, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: drtasamir@hotmail.com; ORCID: {0000-0002-6964-1418}
- Khaled Abdou, MD, Lecturer of Anesthesia and Intensive Care, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: khaledabdou@med.asu.edu.eg; ORCID: {0000-0001-9777-080X}
- Marwa Salem, MD, Lecturer of Anesthesia and Intensive Care, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: Marwamostafa@med.asu.edu.eg; ORCID: {0000-0002-1223-5670}
ABSTRACT
Background & objective: Fascial plane blocks have emerged as one of the main parts in multimodal analgesia after major abdominal surgeries. Quadratus lumborum (QL) and erector spinae plane (ESP) blocks could cover both somatic and visceral pain, and have been extensively used by the anesthesiologists. We compared both of the blocks for effectiveness, ease to perform and safety after total abdominal hysterectomy (TAH).
Methodology: We enrolled 64 female participants undergoing TAH, ASA PS I–III, aged 40-60 y, and BMI 18-40 kg/m2. The patients were randomized equally into either Group QLB, to receive lateral QL block or Group ESPB to receive ESP block (ESPB), under ultrasound guidance, with bupivacaine bilaterally after surgery. Pain severity during rest and on coughing was measured with visual analogue scale (VAS), time to first analgesic request, total meperidine consumption as rescue analgesic, and frequency of PONV through 24 h were recorded.
Results: ESPB lowered the median VAS throughout the first 18 h with a significant difference (P < 0.001) during rest and cough than QLB. Also, ESPB lowered postoperative meperidine consumption more than the QLB group (62.50 ± 22.00 mg) vs (95.31 ± 26.52 mg) respectively with P < 0.001. ESPB prolonged the duration of analgesia over QLB (853.13 ± 50.51 min) vs (812.34 ± 67.53 min) respectively with a P = 0.008. No differences were recorded regarding PONV and hemodynamic parameters.
Conclusion: Erector spinae plane block is more effective, simple, and safe approach to multimodal analgesia after total abdominal hysterectomy than quadratus lumborum block.
Clinical trial registration No.: NCT05541588 on 15/9/2022.
Abbreviations: EOM - External oblique muscle; ESPB - Erector Spinae Plane Block; HR - Heart rate; IOM - Internal oblique muscle; LA - Local anesthetic; MAP - Mean arterial blood pressure; PACU: Post anesthesia care unit; QLB: Quadratus Lumborum Block; QL - Quadratus Lumborum muscle; TAM: transverses abdominus muscle; TAP - Transversus abdominus plane; VAS - Visual Analogue score.
Keywords: Erector spinae plane block; Hysterectomy; Postoperative pain; Quadratus lumborum block.
Citation: Abdelaziz TSA, Abdou K, Salem M. Erector spinae plane block versus quadratus lumborum block for postoperative analgesia after abdominal hysterectomy: a randomized comparative study. Anaesth. pain intensive care 2024;28(2):333−340; DOI: 10.35975/apic.v28i2.2442
Received: December 27, 2023; Revised: January 16, 2024; Accepted: January 18, 2024
1. INTRODUCTION
Abdominal hysterectomy is a common gynecological procedure in the operating rooms due to various causes.1 The pain originates from the abdominal wall (somatic pain) and internal organs, the visceral pain that is transmitted by the autonomic nervous system, mainly by the sympathetic fibers. Adequate postoperative pain relief prevents multiple morbidity scenarios (such as thromboembolism and infection) through early mobility, fast recovery and prevents development of chronic pain.2
Multimodal analgesia for TAH consists of opioid, non-opioid analgesics, lumbar epidural, and recently fascial plane blocks, which include transversus abdominus plane (TAP) block, quadratus lumborum block (QLB), and erector spinae plane block (ESPB). Although lumbar epidural analgesia is considered the popular modality for gynecological and obstetric pain control, it has been associated with some complications; e.g., hypotension, hypovolemia, motor block, bleeding tendency, high intracranial pressure, and local infection.3
TAP block has limited analgesic efficiency and duration as it provides mainly somatic pain relief, and not the visceral pain relief.4
Quadratus Lumborum (QL) is covered anteriorly with transversalis fascia, and ventral rami of T7-L2 pass in between. There are mainly three types of QLB; QLB-I (lateral), QLB-II (posterior), and QLB-III (anterior or trans-muscular), according to the needle tip position; QLB affects ventral rami of T7 to L2, sympathetic chain, iliohypogastric, and ilioinguinal nerves. The diffusion of anesthetic agent around QL muscle to thoracolumbar paravertebral nerve fibers, is responsible for somatic and visceral pain relief. Perioperative QLB provides intra- and post-operative opioid-free analgesia for abdominal surgeries.5-8
The ESPB is a fascial plane where the anesthetic drug is injected between the ES muscle and the transverse process, the solution spreads up and down in the thoracic area covering T1-T12, with lateral spread to paravertebral and epidural space to block ventral and dorsal rami and provides extended unilateral somatic and visceral block. ESPB is gaining popularity for abdominoplasty, intra-abdominal, gynecological, and obstetric surgeries.9-11
We hypothesized that lateral QLB may be an alternative to ESPB regarding postoperative pain control, so compared both of the blocks for effectiveness, ease to perform and safety after total abdominal hysterectomy.
2. METHODOLOGY
A prospective, randomized, comparative study started after the approval of the institutional Ethics Committee and registration at ClinicalTrials.gov between 7th July 2022 and 1st January 2023 in the university hospitals. It followed CONSORT guidelines, and all participants signed a written informed consent before the procedure.
Participants undergoing TAH, who fulfilled the inclusion criteria; e.g., ASA I–III, age 40-60 y old, and BMI 18-40 kg/m2, were randomized into the study groups using program‐generated numbers in opaque envelopes with a one-to-one ratio.
Group QLB (n = 32) received lateral quadratus lumborum block (QLB-I) under ultrasound guidance with 20 ml of bupivacaine 0.25% at each side after surgery.
Group ESPB (n = 32) received ESPB under ultrasound guidance with 20 ml of bupivacaine 0.25 % at each side after surgery.
Participants were excluded upon refusal or if they had an allergy to bupivacaine, local infection, coagulopathy, and intellectual disability. The participants, allocating staff, and follow-up residents were blinded. The preoperative assessment and the standard investigations were done for all participants.
In the operating room, standard monitoring was connected and balanced general anesthesia was administered. After surgery and before extubation, the patient was positioned laterally on her side, and under strict aseptic conditions, ultrasound guided lateral QLB or ESPB was served.
Lateral QLB
A linear probe was placed horizontally over the flanks at the mid-axillary line to identify three parallel muscles; external oblique muscle (EOM), internal oblique muscle (IOM), and transverses abdominus muscle (TAM). Then the probe was slid backwards until TAM aponeurosis; This is an ultrasound hyperechogenic sign where the QL extends posteriorly and to the inside. U/S needle 22G (80-100 mm) directed antero-posteriorly by the ‘in-plane’ technique through the muscles to the hyperechogenic sign without TAM penetration. The needle tip was placed lateral to QL, then after negative aspiration and hydro-dissection (separation of QL from fascia) with 5 ml of normal saline NS, a 20 ml bupivacaine 0.25% was given on each side.12
ESPB
A linear probe was placed longitudinally at T10 spinous process level and then slid outward till the transverse process (TP) was under the ES muscles; U/S needle 22G (80-100 mm) directed caudally by the ‘in-plane’ technique until it contacted the TP, then after negative aspiration and hydro-dissection (separation of ES muscles from the TP) with 5 ml of normal saline, a 20 ml bupivacaine 0.25% was given on each side.13
The participants were transferred to PACU after extubation and after regaining consciousness, where they were connected to standard monitoring. The sensory dermatomal block was assessed by pinprick test and failed blocks were excluded. Pain intensity was recorded during rest and on coughing using the visual analogue scale (VAS) after full recovery. After follow-up, participants were discharged with a modified Aldrete recovery score > 9.
In the ward, paracetamol was infused every 8 h regularly, and VAS score recorded at 2, 6, 12, 18, and 24 h during rest and on coughing. While IV meperidine 0.5 mg/kg was given if VAS score remained ≥ 4; inj. granisetron 1 mg was given for PONV (maximum to 3 mg per day).
The primary outcome was the pain scores during rest at 18 h postoperatively assessed by VAS. The secondary outcome were; pain scores during rest and on coughing through the first 24 h, total duration of analgesia, 24-h meperidine consumption and the frequency of PONV during 24 h.
PASS 11 software was used for sample size calculation and after reviewing Mohamed A. Ghanem et al. (2021)14 results, 32 participants in each group - a total of 64 cases - achieved a power of 80% comparing the mean pain score during rest at 18 h to detect the effect size ≥ 0.8 by independent samples t-test and 0.05 significance level; The sample was inflated by 20% to compensate for the dropouts.
Statistical Package for Social Science (SPSS) version 27.0. was used to analyze the study data, the normally distributed continuous variables are presented as mean ± standard deviation (SD), and the abnormally distributed continuous variables are presented as median and inter-quartile range, while the categorical variables are presented as numbers and percentages. Continuous data were analyzed by the student t-test for normally distributed and Mann–Whitney test for abnormally distributed data. Categorical data were analyzed by the chi-square test. A 95% confidence interval (95% CI) was used with the conduction of all tests and the margin of error accepted was set to 5%. So, a P < 0.05 was significant.
3. RESULTS
Seventy participants were screened with six exclusions (3 didn’t fulfil the criteria and 3 refused). The 64 participants were randomized into two equal groups and their data were analyzed at the end of the study (Figure 1).
No differences regarding demographic data (age, BMI, ASA), operative time, and hemodynamic parameters (HR and MAP) were found between groups with P > 0.05 (Table 1).
| Table 1: Comparative demographic data and the procedure time | |||||
| Parameter | Group ESPB
(n = 32) |
Group QLB
(n = 32) |
t/x2 | P value | |
| Age (y) | 54.47 ± 7.45 | 54.22 ± 6.74 | 0.14 t | 0.89 | |
| BMI (kg/m2) | 36.73 ± 5.49 | 37.87 ± 6.57 | 0.75 t | 0.45 | |
| ASA | I II |
17 (53.1%) 15 (46.9%) |
16 (50%) 16 (50%) |
0.06 X2 | 0.8 |
| Procedure time (min) | 12.13 ± 2.00 | 12.00 ± 1.98 | 0.25 t | 0.8 | |
| Data expressed as mean ± SD or n (%); t = student’s t test, x2 = chi-square test; P < 0.05 considered as significant | |||||
| Table 2: Comparative hemodynamic data and narcotic use in two groups | ||||
| Recording Time | Group ESPB
(n = 32) |
Group QLB
(n = 32) |
t/x2 | P value |
| MAP (mmHg) | ||||
| · PACU | 89.06 ± 6.02 | 87.94 ± 4.89 | 0.82 t | 0.41 |
| · 2 h | 91.41 ± 5.85 | 90.72 ± 5.12 | 0.50 t | 0.62 |
| · 6 h | 92.03 ± 4.90 | 91.06 ± 4.67 | 0.81 t | 0.42 |
| · 12 h | 90.31 ± 6.59 | 90.75 ± 5.09 | 0.30 t | 0.77 |
| · 18 h | 91.25 ± 7.30 | 90.06 ± 5.85 | 0.72 t | 0.48 |
| · 24 h | 91.25 ± 6.09 | 88.47 ± 5.26 | 1.96 t | 0.06 |
| HR (beat / min) | ||||
| · PACU) | 72.66 ± 7.83 | 74.34 ± 8.94 | -0.80t | 0.42 |
| · 2 h | 76.81 ± 8.28 | 75.31 ± 7.99 | 0.74 t | 0.46 |
| · 6 h | 76.47 ± 8.34 | 76.19 ± 8.01 | 0.14 t | 0.89 |
| · 12 h | 74.53 ± 8.28 | 75.13 ± 7.83 | -0.30t | 0.77 |
| · 18 h | 75.38 ± 8.83 | 75.97 ± 7.35 | 0.29 t | 0.77 |
| · 24 h | 75.88 ± 7.71 | 75.72 ± 7.81 | 0.08 t | 0.94 |
| Time to 1st rescue analgesia (min) | 853.13 ± 50.51 | 812.34 ± 67.53 | 2.7 t | 0.008* |
| Postop narcotic (mg) | 62.50 ± 22.00 | 95.31 ± 26.52 | 5.39 t | <0.001* |
| PONV | 5 (15.6%) | 10 (31.2%) | 2.1 X2 | 0.14 |
| Data expressed as mean ± SD or n (%); t = student’s t test, x2 = chi-square test, *= P of significant difference, h=hours, min= minute, PONV=postoperative nausea and vomiting. | ||||
| Table 3: Comparative postoperative VAS scores at rest and cough. | ||||
| Recording time | ESPB
(n=32) |
QLB
(n=32) |
z | P value |
| VAS at rest | ||||
| PACU | 1 (1-2) | 2 (2-3) | 4.1 | < 0.001* |
| 2 h | 1.5 (1-2) | 3 (2-3) | 5.9 | < 0.001* |
| 6 h | 2 (1-2) | 3 (2-4) | 5.02 | < 0.001* |
| 12 h | 2 (2-3) | 3.5 (3-4) | 5.07 | < 0.001* |
| 18 h | 3 (2-3) | 4 (3-4.5) | 4.56 | < 0.001* |
| 24 h | 3 (3-4) | 3 (3-4) | 1.2 | 0.22 |
| VAS at cough | ||||
| PACU | 2 (2-3) | 3 (3-4) | 4.1 | < 0.001* |
| 2 h | 2.5 (2-3) | 4 (3-4) | 5.8 | < 0.001* |
| 6 h | 3 (2-3) | 4 (3-5) | 5.3 | < 0.001* |
| 12 h | 4 (3-5) | 5.5 (5-6) | 5.35 | < 0.001* |
| 18 h | 4 (3-4) | 5 (4-5.5) | 4.2 | < 0.001* |
| 24 h | 4 (4-5) | 4 (4-5) | 1.4 | 0.17 |
| Data expressed as range, median and inter quartile range (IQR),
z= Mann-Whitney test, * P < 0.05 is significant |
||||
The results showed significant differences in VAS scores during rest (Figure 2) and with cough (Figure 3) at 0, 2, 6, 12, 18 h with lower values in the ESPB group (P < 0.001) (Table 3); Moreover, the duration of analgesia in ESPB group was longer than QLB group (853.13 ± 50.51 vs 812.34 ± 67.53 min respectively) (P = 0.008) and post-operative meperidine consumption was lower in ESPB group than QLB group (62.50 ± 22.00 vs 95.31 ± 26.52 mg respectively) (P < 0.001) (Table 2).
There were no statistical differences between groups regarding PONV (Table 2) and no cases of organ injury or local anesthetic toxicity were recorded throughout the study.
4. DISCUSSION
We compared the efficacy of lateral QLB with ESPB on post-abdominal hysterectomy pain severity during rest and on movement (coughing), and found a reduction in the VAS scores up to 18 h in ESPB group with lower narcotic consumption at 24 h in comparison to QLB group. The differences in analgesic duration between ESPB and QLB were not clinically significant (853.13 ± 50.51 vs 812.34 ± 67.53 min respectively). Also, no difference regarding PONV, and no cases of any injury or local anesthetic toxicity were recorded.
TAH is a common daily procedure in the operating room.1 The pain originates from the abdominal wall (somatic pain) and internal organs [visceral pain that is transmitted by the autonomic nervous system mainly sympathetic fibers]; Multi-modal analgesia protocols involve ultrasound-guided fascial plane blocks (as transversus abdominus, quadratus lumborum, and erector spinae) to provide opioid-sparing analgesia.3 Postoperative pain relief prevents multiple morbidity scenarios (such as thromboembolism and infection) through early mobility and fast recovery.2
The ESPB is a fascial plane where the anesthetic drug is injected between the ES muscle and the transverse process, the solution extends up and down in the thoracic area covering T1-T12, with lateral spread to paravertebral and epidural space to block ventral and dorsal rami and provides extended unilateral somatic and visceral block.9,10 ESPB at the T10 level could block pain sensation from T5 till L2,15 and cover the visceral sensation of the uterus (T11-T12).16 So, we chose the level of T10 block for this study.
ESPB is gaining popularity for abdominoplasty, intra-abdominal, gynecological, and obstetric surgeries,9-11 and many studies showed sufficient analgesic effect and lower opioid consumption with ESPB in many surgeries as bariatric surgeries, laparotomy, nephrectomy, hernia repair, hysterectomy, and laparoscopy.11,17-21 During the first postoperative 24 h the ESPB lowered the consumption of rescue analgesic compared to QLB.
Ghanem and his colleagues compared the analgesic effects of QLB III and ESPB in colorectal cancer surgeries and found that ESPB lowered pain scores during rest and cough and reduced total narcotic consumption with no differences in the time of first analgesic request, in agreement with our result. Although pain severity was high in QLB than our results but still it was statistically significant, mostly due to dermatomal coverage and excessive surgical manipulation of viscera in colorectal surgery compared with hysterectomy.14
Abd Ellatif and Abdelnaby conducted a controlled trial and found that the QLB III is as efficient as ESPB in providing analgesia and decreasing perioperative opioid consumption after nephrectomy.22 The large skin incisions and muscle cutting cause 75% of postoperative pain (somatic pain) that are fully blocked by ESPB and QLB.23 The same findings were reported by Jiang and his colleagues who compared ESPB and QLB III against control in laparoscopic hysterectomy.24 The different results might be due to less surgical manipulation in laparoscopy and the different QLB techniques.
The diffusion of anesthetic agent around QL muscle to thoracolumbar paravertebral nerve fibers is responsible for somatic and visceral pain relief.25 Perioperative QLB provides intra- and post-operative opioid-free analgesia for abdominal surgeries.5-8 After reviewing the previous literature regarding QLB for abdominal surgeries, no sufficient evidence at the time prefers a specific QL technique over the others for specific surgery.5,8,26,27 So, lateral QLB technique was preferred in this study, being a simple, easy, and fast approach. Additionally, it could be accessed in supine position.
Many trials compared the different techniques of QL against TAP block or control group for intra and postoperative pain, analgesic duration, and narcotic consumption after abdominal, gynecological, and obstetric procedures, where QLB showed better pain control, longer duration of analgesia, and less narcotic requirements, partially in line with our results as median VAS scores were ≤ 4 at all-time points during rest and till 6 h on coughing. 28-31 Moreover, the first analgesic requested was at 812.34 ± 67.53 min. Also, a comparative study between QLB and paravertebral block for radical cystectomy showed similar analgesic effects with no differences in opioid consumption.32 Krohg et al. and Mieszkowski et al. compared lateral QLB against the control group following cesarean section and reported lower pain scores including somatic and visceral pain, less narcotic consumption, and longer analgesia.26,27
Finally, after reviewing the previous literature regarding ESPB and QLB for abdominal surgeries, ESPB showed reduction of pain scores, delayed time to first analgesic request, and lower narcotic consumption regardless of the surgery, while QLB showed different results even with the same technique.
5. LIMITATIONS
Our study includes the lack of a controlled group, the small sample size, and the lack of optimal local anesthetic volume. Further studies are required to determine the proper spread of LA in live participants, not a cadaver, for QLB techniques and the best technique for each procedure.
6. CONCLUSION
The results of our prospective, randomized, comparative study show that erector spinae plane block is an effective, simple, and safe approach to multimodal analgesia after total abdominal hysterectomy.
7. Ethical issues
Written informed consent for participation and publication was obtained from all participants.
8. Availability of data
All numerical data generated during the course of this study is available upon reasonable request.
9. Conflict of interest
The authors declare that no potential conflict of interest relevant to this article was reported. The study was conducted using institutional resources.
10. Authors' contribution
TA: data analysis, results interpretation, writing discussion, preparing manuscript, and journal submission.
KA: study conception, design, data collection, data analysis, results interpretation, and writing discussion.
MS: study conception, design, data collection, and writing discussion.
The manuscript and results were reviewed and approved by all authors.
11. REFERENCES
- Cohen SL, Vitonis AF, Einarsson JI. Updated hysterectomy surveillance and factors associated with minimally invasive hysterectomy. JSLS. 2014 Jul;18(3):e2014.00096. PMID: 25392662 DOI: 4293/JSLS.2014.00096
- Kehlet H. Manipulation of the metabolic response in clinical practice. World J Surg. 2000;24(6):690–695. PMID: 10773121 DOI: 1007/s002689910111
- Moraca RJ, Sheldon DG, Thirlby RC. The role of epidural anesthesia and analgesia in surgical practice. Ann Surg. 2003;238(5):663–673. PMID: 14578727 DOI: 1097/01.sla.0000094300.36689.ad
- Baeriswyl M, Kirkham KR, Kern C, Albrecht E. The analgesic efficacy of ultrasound guided transversus abdominis plane block in adult patients: a meta-analysis. Anesth Analg. 2015;121:1640–1654. PMID: 26397443 DOI: 1213/ANE.0000000000000967
- Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus lumborum block: anatomical concepts, mechanisms, and techniques. Anesthesiology. 2019 Feb;130(2):322-35. PMID: 30688787 DOI: 1097/ALN.0000000000002524
- Kadam VR. Ultrasound-guided quadratus lumborum block as a postoperative analgesic technique for laparotomy. J Anaesthesiol Clin Pharmacol. 2013 Oct;29(4):550-2. PMID: 24249997 DOI: 4103/0970-9185.119148
- Onwochei DN, Børglum J, Pawa A. Abdominal wall blocks for intra-abdominal surgery. BJA Educ. 2018;18(10):317-322. PMID: 33456796 DOI: 1016/j.bjae.2018.07.002
- Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: A randomised controlled trial. Eur J Anaesthesiol. 2015 Nov;32(11):812-8.PMID: 26225500 DOI: 1097/EJA.0000000000000299
- Schwartzmann A, Peng P, Maciel MA, Forero M. Mechanism of the erector spinae plane block: insights from a magnetic resonance imaging study. Can J Anaesth. 2018 Oct;65(10):1165-6. PMID: 30076575 DOI: 1007/s12630-018-1187-y
- Aponte A, Sala-Blanch X, Prats-Galino A, Masdeu J, Moreno LA, Sermeus LA. Anatomical evaluation of the extent of spread in the erector spinae plane block: a cadaveric study. Can J Anaesth. 2019 Aug;66(8):886-93. PMID: 30076575 DOI: 1007/s12630-018-1187-y
- Hamed MA, Goda AS, Basiony MM, Fargaly OS, Abdelhady MA. Erector spinae plane block for postoperative analgesia in patients undergoing total abdominal hysterectomy: a randomised controlled study original study. J Pain Res. 2019;12:1393-1398. PMID: 31118757 DOI: 2147/JPR.S196501
- Akerman M, Pejčić N, Veličković I. A Review of the Quadratus Lumborum Block and ERAS. Front Med (Lausanne). 2018;5:44. PMID: 29536008 DOI: 3389/fmed.2018.00044
- Zengin SU, Ergun MO, Gunal O. Effect of ultrasound-guided erector spinae plane block on postoperative pain and intraoperative opioid consumption in bariatric surgery. Obes Surg. 2021;31(12):5176-82. PMID: 34449029 DOI: 1007/s11695-021-05681-7
- Mohamed A. Ghanem, Amer A. Attieh, Ahmed M. Mohasseb, May E. Badr. A randomised comparative study of analgesic effect of erector spinae plane block versus quadratus lumborum block for open colorectal cancer surgeries. Egypt J Anaesth. 2021;37(1):483-490. DOI: 1080/11101849.2021.1984735
- Frassanito L, Zanfini BA, Catarci S, Sonnino C, Giuri PP, Draisci G. Erector spinae plane block for postoperative analgesia after total laparoscopic hysterectomy: case series and review of the literature. Eur Rev Med Pharmacol Sci. 2020;24:3892–7. PMID: 32329864 DOI: 26355/eurrev_202004_20855
- Singh N, Rao PB, Elayat A. Ultrasound-guided anterior and posterior quadratus lumborum block for analgesia after laparoscopic hysterectomy. Pain Manag. 2021;11:5–8. PMID: 33073711 DOI: 2217/pmt-2020-0008
- Luis-Navarro JC, Seda-Guzmán M, Luis-Moreno C, Chin KJ. Erector spinae plane block in abdominal surgery: Case series. Indian J Anaesth. 2018;62:549-54. PMID: 30078859 DOI: 4103/ija.IJA_57_18
- Kim D, Kim JM, Choi GS, Heo G, Kim GS, Jeong JS. Ultrasoundguided erector spinae plane block for postoperative analgesia in laparoscopic liver resection: a prospective, randomised controlled, patient and observer-blinded study. Eur J Anaesthesiol. 2021;38(2):S106-12. PMID: 33653982 DOI: 1097/EJA.0000000000001475
- Kim S, Bang S, Kwon W. Intermittent erector spinae plane block as a part of multimodal analgesia after open nephrectomy. Chin Med J (Engl). 2019;132(12):1507–1508. PMID: 31205117 DOI: 1097/CM9.0000000000000269
- Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of preoperative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72:452-60. PMID: 28188621 DOI: 1111/anae.13814
- Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: A Report of 3 cases. Reg Anesth Pain Med. 2017;42:372 6. PMID: 28272292 DOI: 1097/AAP.0000000000000581
- Abd Ellatif SE, Abdelnaby SM. Ultrasound guided erector spinae plane block versus quadratus lumborum block for postoperative analgesia in patient undergoing open nephrectomy: a randomised controlled study. Egypt J Anaesth. 2021 Jan 1;37(1):123-34. DOI: 1080/11101849.2021.1894661
- Niraj G, Tariq Z. Continuous erector spinae plane (ESP) analgesia in different open abdominal surgical procedures: a case series. J Anesth Surg. 2018;5(1):57–60. [FreeFullText]
- Jiang W, Wang M, Wang X, Jin S, Zhang M, Zhang L, et al. Effects of Erector Spinae Plane Block and Transmuscular Quadratus Lumborum Block on Postoperative Opioid Consumption in Total Laparoscopic Hysterectomy: A Randomised Controlled Clinical Trial. Pain Ther. 2023;12:811–824. PMID: 37052813 DOI: 1007/s40122-023-00505-1
- Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG, et al. Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. 2011;66:1023–30. PMID: 21851346 DOI: 10.1111/j.1365-2044.2011.06855.x
- Krohg A, Ullensvang K, Rosseland LA, Langesæter E, Sauter AR. The analgesic effect of ultrasound-guided quadratus lumborum block after cesarean delivery: A randomised clinical trial. Anesth Analg. 2018;126:559–65. PMID: 29135590 DOI: 1213/ANE.0000000000002648
- Mieszkowski MM, Mayzner-Zawadzka E, Tuyakov B, Mieszkowska M, Żukowski M, Waśniewski T, et al. Evaluation of the effectiveness of the quadratus lumborum block type I using ropivacaine in postoperative analgesia after a cesarean section: A controlled clinical study. Ginekol Pol. 2018;89:89–96. PMID: 29512813 DOI: 5603/GP.a2018.0015
- Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: A randomised controlled trial. Reg Anesth Pain Med. 2016;41:757–62 PMID: 27755488 DOI: 1097/AAP.0000000000000495
- Alansary AM, Kamaly AM, Abdel Hamid HS, Aboelanean YM, Ezzat AW. Ultrasound-guided quadratus lumborum block versus transversus abdominis plane block in patients undergoing total abdominal hysterectomy. Ain-Shams J Anesthesiol. 2022;14(22). DOI: 1186/s42077-022-00224-3
- Yousef NK. Quadratus Lumborum Block versus Transversus Abdominis Plane Block in Patients Undergoing Total Abdominal Hysterectomy: A Randomised Prospective Controlled Trial. Anesth Essays Res. 2018;12(3):742-747. PMID: 30283187 DOI: 4103/aer.AER_108_18
- Fargaly OS, Boules ML, Hamed MA, Aleem Abbas MA, Shawky MA. Lateral Quadratus Lumborum Block versus Transversus Abdominis Plane Block in Laparoscopic Surgery: A Randomized Controlled Study. Anesthesiol Res Pract. 2022 Mar 28;2022:9201795. PMID: 35386840 DOI: 1155/2022/9201795
- Lee AJ, Yabes JG, Hale N, Hrebinko RL, Gingrich JR, Maranchie JK, et al. The comparative effectiveness of quadratus lumborum blocks and paravertebral blocks in radical cystectomy patients. Can J Urol. 2018 Apr;25(2):9255-9261 PMID: 29680003