Mohamed Saleh1, Mohammed Saeed Abd Elaziz2, Eman Rafat Sonbol3, Aya Hisham Moussa4
Authors' affiliations:
Background & objective: Peripheral nerve blocks are efficient options for pain management in breast operations. Following modified radical mastectomy, the application of serratus anterior plane block has been shown to be very successful at controlling pain and minimizing narcotic usage. To increase the peripheral nerve block's duration and strength, numerous adjuvants to local anesthetics have been employed. We compared the effectiveness of neostigmine with ketamine as analgesic adjuvants to local anesthetic in US-guided serratus anterior plane block in patients undergoing modified radical mastectomy.
Methodology: A randomized, prospective, double-blinded comparative study, performed at Ain-Shams University Hospitals on 75 adult females aged 30-65 y, who were planned for a modified radical mastectomy and received serratus anterior plane block immediately after the procedure. Patients were randomly divided into 3 groups, 25 patients per group. Group BK: received 1 ml (50 mg) ketamine added to 20 ml of bupivacaine 0.25%. Group BN: received 1 ml (0.5 mg) neostigmine added to 20 ml of bupivacaine 0.25% and Group BS: received 1 ml normal saline added to 20 ml of bupivacaine 0.25%. The primary outcome was the total amount of nalbuphine consumed in a 24-h period. The secondary outcomes were the patient's hemodynamics, pain scores, and time to first rescue analgesia request.
Results: Total 24 h nalbuphine consumption was statistically significantly varying between the study groups (P < 0.001); the highest consumption of nalbuphine was in Group BS. As regards numeric pain scale at 2 h and 6 h postoperative there was significant statistical difference among Group BS with each of Group BK and Group BN (P = 0.001, P < 0.001 respectively). At 12 h and 24 h postoperative the difference was significant between all study groups. As regards requesting rescue analgesia there was significant variance among Group BS and each of Group1 and Group BN with no significant variance among Group BK and Group BN.
Conclusion: In serratus anterior plane block, adding 50 mg ketamine to bupivacaine decrease 24 h nalbuphine consumption and numeric pain scale, adding 0.5 mg neostigmine to bupivacaine has lower rate of requesting rescue analgesia following ketamine.
Trial Registry: NCT05802979.
Keywords: serratus anterior, ketamine, neostigmine, ultrasound, analgesia, modified radical mastectomy.
Citation: Saleh M, Saeed M, Rafat E, Hisham A. Comparative analgesic efficacy of ketamine versus neostigmine as adjuvants to bupivacaine during ultrasound-guided serratus anterior plane block in modified radical mastectomy. Anaesth. pain intensive care 2024;28(2):315−323; DOI: 10.35975/apic.v28i2.2440
Received: December 18, 2023; Revised: February 08, 2024; Accepted: (February 13, 2024
Modified radical mastectomy is a frequent surgical technique for patients with breast cancer; and it comes with a high risk of severe acute postoperative pain and limited shoulder mobility, which can cause delays in hospital discharge.1 For early mobilization and long-term wellbeing of these patients, adequate pain management after surgery is essential. Intravenous opioids are frequently used to treat acute pain following mastectomy. Adverse effects associated with the use of opioids include lethargy, nausea, vomiting, and respiratory depression.2
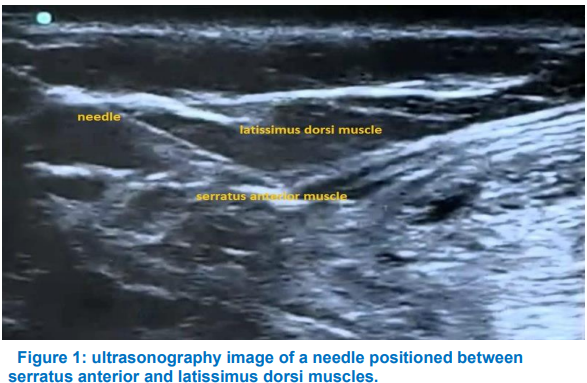
For breast surgery, thoracic epidural analgesia and paravertebral blocks have been considered the gold standards.3,4 But both methods come with serious side effects, including pneumothorax and complete spinal anesthesia.5 Since ultrasonography has been used in anesthetic treatment, a number of interfacial plane blocks have been described. For breast procedures, novel interfacial plane blocks include pectoral nerve blocks (PECS) and serratus anterior plane block (SAPB) can give analgesia.6 During the US-guided SAPB, a local anesthetic (LA) is injected into the compartment bounded by the latissimus dorsi and serratus anterior muscles. Lateral cutaneous branches of the intercostal nerves, thoracodorsal, intercostobrachial, and long thoracic nerves (T3–T9) are all anesthetized by SAPB. Analgesia for lateral thoracic wall and breast surgeries is provided by SAPB.7 Several medications have been utilized as adjuvants to LA through SAPB, such as dexamethasone, nalbuphine, and dexmedetomidine. They allow a decreased postoperative opioid consumption and an improved analgesic profile.8
Ketamine binds to N-methyl-D-aspartate receptors in a non-competitive manner. Premedication, sedation, induction, and maintenance of general anesthesia are among its uses. There have been reports of ketamine's analgesic and central, regional, and local effects.9 Ketamine reduces the amount of morphine consumed over the course of a 24-hour period, lessens postoperative pain intensity for up to 48 h, and postpones the need for rescue analgesic therapy.10,11 The anticholinesterase drug neostigmine raises the levels of acetylcholine at cholinergic synapses. Relying on a spinal cholinergic interneuron, spinal neostigmine appears to activate descending pain inhibitory systems, potentially aggravating a cholinergic tonus that is already activated postoperatively,12 and appears to be very effective in reducing somatic pain. Its analgesic effectiveness as a LA adjuvant in peripheral nerve blocks or interstitial plane blocks, however, is still unknown.13 The purpose of this research was to compare the analgesic effectiveness of ketamine and neostigmine as adjuvants to LA in cases undergoing modified radical mastectomy using ultrasound guidance for SAPB.
1.2. Objectives of study
The primary outcome was defined as the amount of nalbuphine consumed within the first day following surgery. Secondary outcomes included the patient's hemodynamics, pain scores, medication side effects, and the time for the first request for rescue analgesia.
A written informed consent was obtained from 75 adult females, ages 30 to 65, who were undergoing modified radical mastectomy under general anesthesia with Physical Status I, II In accordance with the American Association of Anesthesiologists (ASA) score. The research was performed at Ain-shams University Hospitals with approval from the Ethical Committee of Scientific Research (FMASU MD 209/2022) and prospectively registered at ClinicalTrials.gov (NCT05802979). The study excluded patients who had not agreed to participate, were ASAIII or higher, had a history of drug allergies, a history of coagulation disorders, a history of psychiatric illness, a history of seizures, a history of cardiac arrhythmias (tachycardia or bradycardia), or a history of elevated intracranial tension.
A statistician who was blind to the study's purpose created computer-targeted random number tables from which cases were randomly divided to 3 equal groups of twenty-five each. Patients in Group BK were given ketamine plus bupivacaine, while those in Group BN were given bupivacaine plus neostigmine. Patients in Group BS were given bupivacaine along with normal saline.
2.1. Sample size
A sample size of at least 75 cases (25 per group) was required when using the PASS 11 program to calculate sample size. Power was set at 80%, alpha error was set at 5%, and the effect size variance among the groups concerning the total amount of analgesic consumption following surgery within a day postoperative and after 10% adjustment for dropout rate was equal to 0.4.
2.2. Study procedures
Pre-operative Settings: A comprehensive preoperative evaluation of each patient was conducted, encompassing a history taking session, a clinical examination, and standard laboratory tests such as complete blood count, BT, PTT, PT, AST, ALT, urea, creatinine, and viral markers. After informing the patients about the procedure, their consent was obtained. The use of the Numeric Pain Scale (NPS) to score the intensity of pain was explained to each patient.14 ranging from zero (no pain) to ten (the worst pain)
The study medications were prepared as;
Group BK: 0.25% bupivacaine 20 ml plus ketamine 01 ml (50 mg)
Group BN: 0.25% bupivacaine 20 ml plus neostigmine 01 ml (0.5 mg)
Group BS: 0.25% bupivacaine 20 ml plus 01 ml normal saline
2.2.1. Intraoperative settings:
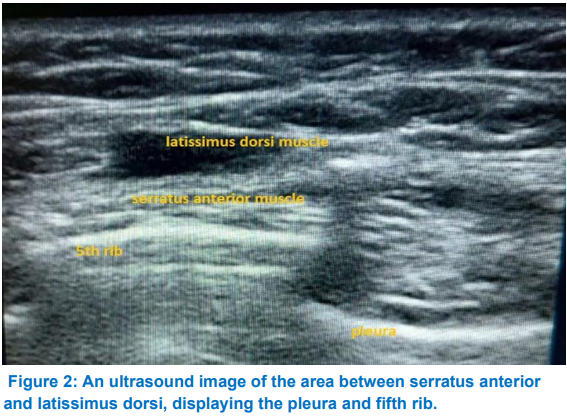
On arrival of the cases to the operating room a 20-gauge iv access was inserted at the contralateral side of the surgery. Heart rate, non-invasive blood pressure, ECG and pulse oximetry (SpO2) were monitored during the perioperative period. Induction of general anesthesia was performed using propofol 2 mg/kg IV, fentanyl 1 µg/kg IV and atracurium 0.5 mg/kg IV. After surgery, the patient was placed on his side, with the surgical side facing up and the arm abducted. SonoSiteTM, Inc., Bothell, WA 98021, USA, provided the linear US transducer (6–13 MHz). The fifth rib level was the location of the probe in the transverse plane of the midaxillary line. There was a visual representation of the ribs, pleural line, and latissimus dorsi and serratus anterior muscles above it. After applying 3 ml of 2% lidocaine topically to the affected area, a regional block needle (22-G, 50-mm Stimuplex A, B Braun, Melsung, Germany) was inserted into the skin at a 45-degree angle and 4 cm of depth toward the fifth rib.
Following aspiration, the study solution was injected according to the group.
2.2.2. Post-operative settings:
Patients were transferred to PACU, and were discharged when a modified Aldrete score was greater than 9.15 The patients were then moved to the ward and given an 8-hr regimen of acetaminophen 1 gram IV.
At 0, 1, 2, 6, 12, and 24 h following surgery, the heart rate, mean arterial pressure, and NPS score were noted. Intravenous boluses of 5 mg of nalbuphine were administered, whenever the NPS score was greater than 4; repeated every hour, if required, for a maximum of 16 h. Measuring the total amount of nalbuphine consumed in a day was the primary outcome. the time to first request for rescue analgesia (nalbuphine), pain scores and patient hemodynamics and any side effects of drugs were the secondary outcomes.
2.3. Statistical analysis
All data were recorded, tabulated, analyzed, and statistically compared between groups to identify any significant differences between them. The statistical package for social sciences (IBM SPSS) software version 28.0, IBM Corp., Chicago, USA, 2021, was used to edit, code, tabulate, and analyze the data according to the type of data.
ANOVA test was used to compare quantitative data that had undergone normality testing with the Shapiro-Wilk test, and had been described as mean ± SD (standard deviation) along with the range's minimum and maximum values. For variables with small expected numbers, the Fisher's Exact test and the Chi square test were used to compare qualitative data that is expressed as a number and percentage. Comparing the frequency of requesting rescue analgesia was done using the log rank test. Post hoc comparisons employ the Bonferroni test. A P < 0.050 was regarded as significant.
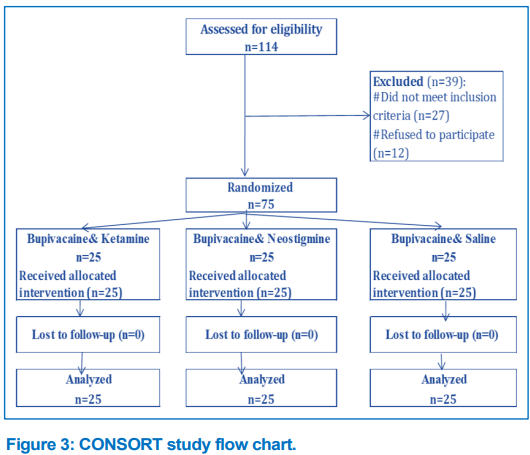
modified radical mastectomy at Ain Shams University Hospitals. Out of the 114 participants, 12 patients refused to take part in the study, and 27 did not meet the inclusion criteria. This left 75 cases, 25 of whom were placed in each of three groups, and they were all statistically analyzed (Figure 3). As demonstrated in Table 1, there was no statistically significant variance (P > 0.05) among any of the study groups in the demographic data and surgical characteristics, such as age, BMI, ASA physical status, and the duration of operation.
Groups BK and BS did not differ significantly in terms of postoperative heart rate; however, Group BN showed significant differences at 1 and 2 h after surgery (P = 0.001 and < 0.001, respectively, Table 2). Notably, only 3 patients in Group BN experienced postoperative bradycardia (P = 0.102, Table 5), which was treated with intravenous 0.5 mg atropine and did not recur during a day after operation. Regarding the mean arterial pressure following surgery, there was no significant variation was observed amongst all the study groups (P > 0.05, Table 2). There was a significant statistical variance among Group BS and each of Groups BK and BN, but no variances were noticed between Groups BK and BN.
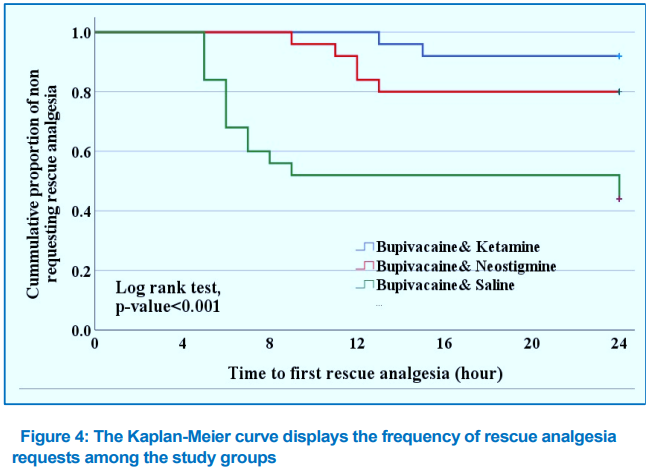
Group BS had the highest NPS, followed by Group BN, and Group BK had the lowest NPS score. This comparison of all study groups was made at 2 h and 6 h postoperatively (P = 0.001 and < 0.001, respectively, (Table 3). Significant statistical differences existed between all study groups at 12 h and 24 h postoperatively. The incidence of request for rescue analgesia varied, with Group BS requesting it more frequently (56%),
Group BN less frequently (20%), and Group BK least frequently (8%). Table 4 and Figure 4 show that there was a significant variance among Group BS and each of Groups 1 and 2, but not between Groups 1 and 2. Between all the study groups, there were statistically significant variances in total 24-h nalbuphine consumption (P < 0.001, Table 4). Group BS had the highest consumption (18.8 ± 2.3), followed by Group BN (13.1 ± 2.7) and Group BK (7.5 ± 3.5).
The study groups exhibited statistically significant variances in the time to 1st rescue analgesia request. Group BS had the shortest time, at 6.3 ± 1.3 h, followed by Group BN at 11.4 ± 1.5 h, and Group BK at 14.0 ± 1.4 h. Table 4 shows that the differences were significant. There was a non-significant statistical variance in post-surgery nausea and vomiting among the study groups (P = 0.687, Table 5), with Group BK experiencing it least frequently.
Significant acute postoperative pain is frequently experienced after breast cancer surgeries, requiring a multimodal analgesia regimen that includes regional analgesia. Analgesia for breast and lateral thoracic wall surgeries is provided by SAPB.7 Our study's findings demonstrated that while adding 0.5 mg neostigmine to bupivacaine decreased rate of requesting rescue analgesia, adding 50 mg of ketamine to bupivacaine in SAPB decreased consumption of nalbuphine over a 24-h period and reduced NPS scores. A popular anesthetic with strong local effects on peripheral nerves is ketamine. Ketamine's local action is most likely brought about by voltage-gated sodium channel blockage.16 Ketamine's action on N-methyl-D-aspartate antagonistic inhibition eliminates the noxious stimulation of peripheral afferent neurons.17 Furthermore, nitric oxide synthase is directly inhibited by ketamine, which likely accounts for some of its analgesic effects.18 The research performed by Elnoamany et al.19 examined the influence of ketamine as an adjuvant to bupivacaine in C-arm guided thoracic paravertebral block for patients undergoing modified radical mastectomy. The findings indicated that the addition of 0.5 mg/kg ketamine to 20 ml of 0.25% bupivacaine reduced total amount of analgesic consumption and delayed period to request rescue analgesia, which is consistent with our findings. Additionally, our results aligned with the research conducted by Othman et al.20, which examined the analgesic effectiveness of combining 1 mg/kg ketamine with 30 ml of 0.25% bupivacaine in US-guided modified pectoral block cases undergoing modified radical mastectomy. The results indicated that ketamine increased the duration before patients requested rescue analgesia and decreased the overall amount of morphine consumed. When Ashry et al.21 added 250 mg of magnesium sulfate and 2 mg/kg of ketamine to 25 ml of 2% lidocaine for US-guided supraclavicular brachial plexus block during upper limb surgeries, they observed that the duration of analgesia was extended by both drugs. Also, they discovered that ketamine was a more effective adjuvant than magnesium sulfate because it required less analgesic medication after surgery. In patients undergoing abdominal hysterectomy, Mohamed et al.22 examined the effects of wound infiltration with 2 mg/kg ketamine added to 40 ml of 0.25% bupivacaine versus 2 µg/kg dexmedetomidine added to 40 ml of 0.25% bupivacaine. They found that patients delayed requesting rescue analgesia and that the postoperative stress response was attenuated, especially with ketamine. In contrast to our findings, Omar et al.23 examined the analgesic effectiveness of tramadol 1.5 mg/kg added to 0.5% bupivacaine versus ketamine 0.5 mg/kg added to 0.5% bupivacaine in paravertebral block for breast operations and discovered no differences in the analgesic duration and 24-hour opioid consumption. Additionally, research by Hefni et al.24 compared the analgesic effect of adding 1 mg/kg ketamine versus 1 µg/kg dexmedetomidine to 32 ml of 0.25% bupivacaine in pecsII block in patients undergoing breast surgery. Their findings revealed different pain scores between study groups, and both ketamine and dexmedetomidine significantly extended the time to 1st analgesic request, with dexmedetomidine offering more successful postoperative pain management than ketamine.
Neostigmine works by preventing the neurotransmitter acetylcholine from being broken down.25 The descending control of afferent nociceptive stimuli is improved by neostigmine's inhibition of acetylcholine degradation, according to recent research. This new method offers a way to increase desired analgesia with minimal dose-related side effects.26 In US guided supraclavicular brachial plexus block procedures for the forearm, Hassanin et al.27 examined the impact of adding 0.5 mg neostigmine to 25 ml of 0.5% bupivacaine versus 25 ml of 0.5% bupivacaine and 1 ml of normal saline. Their findings, which were comparable to ours, showed that the neostigmine group required more time to request their first analgesia. Shakya et al.28 also performed a comparative study for patients undergoing total abdominal hysterectomy between intrathecal 5 µg neostigmine added to 3 ml of 0.5% bupivacaine and intrathecal 25 µg fentanyl added to 3 ml of 0.5% bupivacaine. They found that the low dose of intrathecal neostigmine added to bupivacaine provides postoperative analgesia with fewer side effects. As per our findings, Arafa et al.29 evaluated the analgesic efficacy of intraperitoneal 500 µg neostigmine combined with 50 ml of 0.25% bupivacaine versus 50 ml of 0.25% bupivacaine alone on postoperative pain in laparoscopic cholecystectomy. They discovered that neostigmine intraperitoneally increased the duration of postoperative analgesia and decreased the need for analgesic medications. Neostigmine, on the other hand, did not extend the duration of analgesia in children undergoing urethroplasty when Bhardwaj et al.30 added it to caudal bupivacaine at doses of 2, 3, or 4 µg/kg. According to McCartney et al.31, there was neither anesthetic nor analgesic impact when 1 mg of neostigmine was combined with 0.5% lidocaine during intravenous regional anesthesia.
As regards bradycardia 3 patients only developed postoperative bradycardia in Group BN, that was managed by 0.5 mg atropine IV, it may be due to systemic absorption of neostigmine. Kumari Vasantha and Madhusudhana32 compared the efficacy of intrathecal 0.5% bupivacaine versus 50 µg neostigmine added to 0.5% bupivacaine on postoperative pain management in patients undergoing lower abdominal and lower limb operations and found that one patient developed bradycardia in the neostigmine group that was treated with intravenous atropine 0.6 mg.
In our research, all groups did not significantly differ in terms of postoperative nausea and vomiting and it was clinically non-significant and self-limited. Hood et al.33 studied intrathecal neostigmine in doses of 100-200 µg and observed protracted nausea and vomiting.
In the present study, a catheter was not inserted to enable long-term postoperative pain relief. Large-scale research is also necessary to determine the best injection techniques for a superficial or deep serratus anterior plane block, and the duration of analgesia with and without adjuvants and usage of different doses of ketamine and neostigmine in order to enhance the post-operative analgesia. Rather than during coughing or movement, we measured the pain on numerical pain rating scale at rest following surgery. The ultrasonic view's resolution and clearance were impacted by the postoperative edema in the surgical field, which also distorted the anatomy.
In cases undergoing modified radical mastectomy, ketamine added to bupivacaine in serratus anterior plane block reduces the pain scores on the numeric pain rating scale as well as 24-hour nalbuphine consumption; neostigmine added to bupivacaine decreases the rate of requesting rescue analgesia
7. Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
8. Ethical issues
This study was approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 209/2022) and registered retrospectively with ClinicalTrials.gov Registry, identifier: (NCT05802979). Written informed consent was obtained from all patients.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
MS, manuscript editing
MSA, literature search
ERS, conduction of the study work
AHM, statistical analysis and review
Authors' affiliations:
- Mohamed Saleh, MD, Assistant Professor of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: drsalehm2002@hotmail.com; ORCID ID: https://orcid.org/0000-0001-9856-918X
- Mohammed Saeed Abd Elaziz, MD, Professor of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: mohdsaeed47@yahoo.com
- Eman Rafat Sonbol, MSc, Assistant Lecturer of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: emanrafat119@gmail.com; ORCID ID: https://orcid.org/0009-0003-5097-9552
- Aya Hisham Moussa, MD, Lecturer of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: Ayahisham@med.asu.edu.eg; ORCID ID: https://orcid.org/0000-0003-4680-2204
ABSTRACT
Background & objective: Peripheral nerve blocks are efficient options for pain management in breast operations. Following modified radical mastectomy, the application of serratus anterior plane block has been shown to be very successful at controlling pain and minimizing narcotic usage. To increase the peripheral nerve block's duration and strength, numerous adjuvants to local anesthetics have been employed. We compared the effectiveness of neostigmine with ketamine as analgesic adjuvants to local anesthetic in US-guided serratus anterior plane block in patients undergoing modified radical mastectomy.
Methodology: A randomized, prospective, double-blinded comparative study, performed at Ain-Shams University Hospitals on 75 adult females aged 30-65 y, who were planned for a modified radical mastectomy and received serratus anterior plane block immediately after the procedure. Patients were randomly divided into 3 groups, 25 patients per group. Group BK: received 1 ml (50 mg) ketamine added to 20 ml of bupivacaine 0.25%. Group BN: received 1 ml (0.5 mg) neostigmine added to 20 ml of bupivacaine 0.25% and Group BS: received 1 ml normal saline added to 20 ml of bupivacaine 0.25%. The primary outcome was the total amount of nalbuphine consumed in a 24-h period. The secondary outcomes were the patient's hemodynamics, pain scores, and time to first rescue analgesia request.
Results: Total 24 h nalbuphine consumption was statistically significantly varying between the study groups (P < 0.001); the highest consumption of nalbuphine was in Group BS. As regards numeric pain scale at 2 h and 6 h postoperative there was significant statistical difference among Group BS with each of Group BK and Group BN (P = 0.001, P < 0.001 respectively). At 12 h and 24 h postoperative the difference was significant between all study groups. As regards requesting rescue analgesia there was significant variance among Group BS and each of Group1 and Group BN with no significant variance among Group BK and Group BN.
Conclusion: In serratus anterior plane block, adding 50 mg ketamine to bupivacaine decrease 24 h nalbuphine consumption and numeric pain scale, adding 0.5 mg neostigmine to bupivacaine has lower rate of requesting rescue analgesia following ketamine.
Trial Registry: NCT05802979.
Keywords: serratus anterior, ketamine, neostigmine, ultrasound, analgesia, modified radical mastectomy.
Citation: Saleh M, Saeed M, Rafat E, Hisham A. Comparative analgesic efficacy of ketamine versus neostigmine as adjuvants to bupivacaine during ultrasound-guided serratus anterior plane block in modified radical mastectomy. Anaesth. pain intensive care 2024;28(2):315−323; DOI: 10.35975/apic.v28i2.2440
Received: December 18, 2023; Revised: February 08, 2024; Accepted: (February 13, 2024
1. INTRODUCTION
Modified radical mastectomy is a frequent surgical technique for patients with breast cancer; and it comes with a high risk of severe acute postoperative pain and limited shoulder mobility, which can cause delays in hospital discharge.1 For early mobilization and long-term wellbeing of these patients, adequate pain management after surgery is essential. Intravenous opioids are frequently used to treat acute pain following mastectomy. Adverse effects associated with the use of opioids include lethargy, nausea, vomiting, and respiratory depression.2
For breast surgery, thoracic epidural analgesia and paravertebral blocks have been considered the gold standards.3,4 But both methods come with serious side effects, including pneumothorax and complete spinal anesthesia.5 Since ultrasonography has been used in anesthetic treatment, a number of interfacial plane blocks have been described. For breast procedures, novel interfacial plane blocks include pectoral nerve blocks (PECS) and serratus anterior plane block (SAPB) can give analgesia.6 During the US-guided SAPB, a local anesthetic (LA) is injected into the compartment bounded by the latissimus dorsi and serratus anterior muscles. Lateral cutaneous branches of the intercostal nerves, thoracodorsal, intercostobrachial, and long thoracic nerves (T3–T9) are all anesthetized by SAPB. Analgesia for lateral thoracic wall and breast surgeries is provided by SAPB.7 Several medications have been utilized as adjuvants to LA through SAPB, such as dexamethasone, nalbuphine, and dexmedetomidine. They allow a decreased postoperative opioid consumption and an improved analgesic profile.8
Ketamine binds to N-methyl-D-aspartate receptors in a non-competitive manner. Premedication, sedation, induction, and maintenance of general anesthesia are among its uses. There have been reports of ketamine's analgesic and central, regional, and local effects.9 Ketamine reduces the amount of morphine consumed over the course of a 24-hour period, lessens postoperative pain intensity for up to 48 h, and postpones the need for rescue analgesic therapy.10,11 The anticholinesterase drug neostigmine raises the levels of acetylcholine at cholinergic synapses. Relying on a spinal cholinergic interneuron, spinal neostigmine appears to activate descending pain inhibitory systems, potentially aggravating a cholinergic tonus that is already activated postoperatively,12 and appears to be very effective in reducing somatic pain. Its analgesic effectiveness as a LA adjuvant in peripheral nerve blocks or interstitial plane blocks, however, is still unknown.13 The purpose of this research was to compare the analgesic effectiveness of ketamine and neostigmine as adjuvants to LA in cases undergoing modified radical mastectomy using ultrasound guidance for SAPB.
1.2. Objectives of study
The primary outcome was defined as the amount of nalbuphine consumed within the first day following surgery. Secondary outcomes included the patient's hemodynamics, pain scores, medication side effects, and the time for the first request for rescue analgesia.
2. METHODOLOGY
A written informed consent was obtained from 75 adult females, ages 30 to 65, who were undergoing modified radical mastectomy under general anesthesia with Physical Status I, II In accordance with the American Association of Anesthesiologists (ASA) score. The research was performed at Ain-shams University Hospitals with approval from the Ethical Committee of Scientific Research (FMASU MD 209/2022) and prospectively registered at ClinicalTrials.gov (NCT05802979). The study excluded patients who had not agreed to participate, were ASAIII or higher, had a history of drug allergies, a history of coagulation disorders, a history of psychiatric illness, a history of seizures, a history of cardiac arrhythmias (tachycardia or bradycardia), or a history of elevated intracranial tension.
A statistician who was blind to the study's purpose created computer-targeted random number tables from which cases were randomly divided to 3 equal groups of twenty-five each. Patients in Group BK were given ketamine plus bupivacaine, while those in Group BN were given bupivacaine plus neostigmine. Patients in Group BS were given bupivacaine along with normal saline.
2.1. Sample size
A sample size of at least 75 cases (25 per group) was required when using the PASS 11 program to calculate sample size. Power was set at 80%, alpha error was set at 5%, and the effect size variance among the groups concerning the total amount of analgesic consumption following surgery within a day postoperative and after 10% adjustment for dropout rate was equal to 0.4.
2.2. Study procedures
Pre-operative Settings: A comprehensive preoperative evaluation of each patient was conducted, encompassing a history taking session, a clinical examination, and standard laboratory tests such as complete blood count, BT, PTT, PT, AST, ALT, urea, creatinine, and viral markers. After informing the patients about the procedure, their consent was obtained. The use of the Numeric Pain Scale (NPS) to score the intensity of pain was explained to each patient.14 ranging from zero (no pain) to ten (the worst pain)
The study medications were prepared as;
Group BK: 0.25% bupivacaine 20 ml plus ketamine 01 ml (50 mg)
Group BN: 0.25% bupivacaine 20 ml plus neostigmine 01 ml (0.5 mg)
Group BS: 0.25% bupivacaine 20 ml plus 01 ml normal saline
2.2.1. Intraoperative settings:
On arrival of the cases to the operating room a 20-gauge iv access was inserted at the contralateral side of the surgery. Heart rate, non-invasive blood pressure, ECG and pulse oximetry (SpO2) were monitored during the perioperative period. Induction of general anesthesia was performed using propofol 2 mg/kg IV, fentanyl 1 µg/kg IV and atracurium 0.5 mg/kg IV. After surgery, the patient was placed on his side, with the surgical side facing up and the arm abducted. SonoSiteTM, Inc., Bothell, WA 98021, USA, provided the linear US transducer (6–13 MHz). The fifth rib level was the location of the probe in the transverse plane of the midaxillary line. There was a visual representation of the ribs, pleural line, and latissimus dorsi and serratus anterior muscles above it. After applying 3 ml of 2% lidocaine topically to the affected area, a regional block needle (22-G, 50-mm Stimuplex A, B Braun, Melsung, Germany) was inserted into the skin at a 45-degree angle and 4 cm of depth toward the fifth rib.
Following aspiration, the study solution was injected according to the group.
2.2.2. Post-operative settings:
Patients were transferred to PACU, and were discharged when a modified Aldrete score was greater than 9.15 The patients were then moved to the ward and given an 8-hr regimen of acetaminophen 1 gram IV.
At 0, 1, 2, 6, 12, and 24 h following surgery, the heart rate, mean arterial pressure, and NPS score were noted. Intravenous boluses of 5 mg of nalbuphine were administered, whenever the NPS score was greater than 4; repeated every hour, if required, for a maximum of 16 h. Measuring the total amount of nalbuphine consumed in a day was the primary outcome. the time to first request for rescue analgesia (nalbuphine), pain scores and patient hemodynamics and any side effects of drugs were the secondary outcomes.
| Table 1: Demographic data and operation characteristics among the study groups | |||||
|
Variables |
Group BK
(n = 25) |
Group BN
(n = 25) |
Group BS
(n = 25) |
p-value | |
| Age (y) | 50.3 ± 9.6 | 52.2 ± 8.8 | 52.6 ± 9.3 | ^0.643 | |
| BMI (kg/m2) | 29.5 ± 2.4 | 30.6 ± 2.3 | 30.3 ± 2.0 | ^0.244 | |
| ASA | I | 2 (8.0) | 4 (16.0) | 3 (12.0) | §0.903 |
| II | 23 (92.0) | 21 (84.0) | 22 (88.0) | ||
| Operation duration (min) | 123.6 ± 4.1 | 125.2 ± 4.4 | 125.1 ± 4.1 | ^0.353 | |
| The data are shown as number and (%) or mean ± SD;. P <0.05 considered as significant
ASA: American Society of Anesthesiologists. BMI: Body Mass Index. ^ANOVA test. §Fisher’s Exact test. |
|||||
2.3. Statistical analysis
All data were recorded, tabulated, analyzed, and statistically compared between groups to identify any significant differences between them. The statistical package for social sciences (IBM SPSS) software version 28.0, IBM Corp., Chicago, USA, 2021, was used to edit, code, tabulate, and analyze the data according to the type of data.
ANOVA test was used to compare quantitative data that had undergone normality testing with the Shapiro-Wilk test, and had been described as mean ± SD (standard deviation) along with the range's minimum and maximum values. For variables with small expected numbers, the Fisher's Exact test and the Chi square test were used to compare qualitative data that is expressed as a number and percentage. Comparing the frequency of requesting rescue analgesia was done using the log rank test. Post hoc comparisons employ the Bonferroni test. A P < 0.050 was regarded as significant.
3. RESULTS
modified radical mastectomy at Ain Shams University Hospitals. Out of the 114 participants, 12 patients refused to take part in the study, and 27 did not meet the inclusion criteria. This left 75 cases, 25 of whom were placed in each of three groups, and they were all statistically analyzed (Figure 3). As demonstrated in Table 1, there was no statistically significant variance (P > 0.05) among any of the study groups in the demographic data and surgical characteristics, such as age, BMI, ASA physical status, and the duration of operation.
Groups BK and BS did not differ significantly in terms of postoperative heart rate; however, Group BN showed significant differences at 1 and 2 h after surgery (P = 0.001 and < 0.001, respectively, Table 2). Notably, only 3 patients in Group BN experienced postoperative bradycardia (P = 0.102, Table 5), which was treated with intravenous 0.5 mg atropine and did not recur during a day after operation. Regarding the mean arterial pressure following surgery, there was no significant variation was observed amongst all the study groups (P > 0.05, Table 2). There was a significant statistical variance among Group BS and each of Groups BK and BN, but no variances were noticed between Groups BK and BN.
| Table 2: Heart Rate and Mean Arterial Pressure in Comparison of the Study Groups | ||||
| Postoperative time | Group BK
(n = 25) |
Group BN
(n = 25) |
Group BS
(n = 25) |
^P-value |
| Heart rate (beat/min) | ||||
| Hour-0 | 78.1 ± 2.4 | 77.2 ± 3.3 | 77.0 ± 4.1 | 0.450 |
| Hour-1 | 77.4 ± 2.6a | 71.7 ± 8.4 b | 76.7 ± 4.1 a | 0.001* |
| Hour-2 | 76.6 ± 3.4 a | 72.3 ± 3.8 b | 75.5 ± 4.1 a | ^< 0.001* |
| Hour-6 | 76.5 ± 4.3 | 74.9 ± 3.0 | 75.5 ± 3.5 | 0.298 |
| Hour-12 | 76.7 ± 4.3 | 75.2 ± 2.8 | 75.3 ± 4.0 | 0.295 |
| Hour-24 | 76.0 ± 4.1 | 75.2 ± 3.3 | 75.6 ± 4.1 | 0.745 |
| Mean Arterial Pressure (mmHg) | ||||
| Hour-0 | 81.7 ± 1.7 | 81.8 ± 1.8 | 82.4 ± 2.8 | 0.462 |
| Hour-1 | 81.7 ± 1.7 | 81.2 ± 2.1 | 81.8 ± 2.7 | 0.581 |
| Hour-2 | 81.2 ± 1.8 | 80.5 ± 1.8 | 81.4 ± 3.0 | 0.350 |
| Hour-6 | 80.3 ± 1.5 | 80.2 ± 1.7 | 81.0 ± 3.4 | 0.400 |
| Hour-12 | 80.1 ± 1.6 | 79.7 ± 1.7 | 81.0 ± 3.2 | 0.130 |
| Hour-24 | 79.6 ± 1.3 | 79.8 ± 1.4 | 80.5 ± 3.2 | 0.285 |
| The data are shown as number and (%) or mean ± SD.^ANOVA test. *Significant. The post hoc Bonferroni test revealed that homogenous groups shared the same symbol, "a,b." | ||||
| Table 3: Comparative NPS scores in the study groups | ||||||
| Postoperative time | Group BK
(n = 25) |
Group BN
(n = 25) |
Group BS
(n = 25) |
^P-value | ||
| Hour-0 | 0.5 ± 0.5 | 0.5 ± 0.5 | 0.5 ± 0.5 | 0.950 | ||
| Hour-1 | 1.0 ± 0.5 | 1.2 ± 0.6 | 1.3 ± 0.6 | 0.132 | ||
| Hour-2 | 1.4 ± 0.5 a | 1.6 ± 0.6 a | 2.0 ± 0.5 b | ^0.001* | ||
| Hour-6 | 1.8 ± 0.5 a | 2.0 ± 0.8 a | 2.6 ± 0.8 b | ^<0.001* | ||
| Hour-12 | 2.1 ± 0.8 a | 2.7 ± 0.9 b | 3.3 ± 0.7 c | ^<0.001* | ||
| Hour-24 | 1.4 ± 0.5 a | 2.2 ± 0.5 b | 2.9 ± 0.9 c | ^<0.001* | ||
| The data shown as number (%) or mean ± SD.^ANOVA test. *Significant. The post hoc Bonferroni test revealed that homogenous groups shared the same symbol, "a,b." | ||||||
| Table 4: Rescue analgesia between the study groups | ||||
| Variables | Group BK
(n = 25) |
Group BN
(n = 25) |
Group BS
(n = 25) |
P-value |
| Rescue analgesia | 2 (8.0) a | 5 (20.0) a | 14 (56.0) b | #< 0.001* |
| Total 24-h nalbuphine (mg) | 7.5 ± 3.5 a | 13.0 ± 2.7 b | 18.8 ± 2.3 c | ^< 0.001* |
| Time to first request for analgesic (h) | 14.0 ± 1.4 a | 11.4 ± 1.5 b | 6.3 ± 1.3 c | ^< 0.001* |
| The data shown as number (%) or mean ± SD.^ANOVA test. *P-value significant. According to the post hoc Bonferroni test, homogeneous groups shared the same symbol "a, b, c". #Chi square test. | ||||
Group BS had the highest NPS, followed by Group BN, and Group BK had the lowest NPS score. This comparison of all study groups was made at 2 h and 6 h postoperatively (P = 0.001 and < 0.001, respectively, (Table 3). Significant statistical differences existed between all study groups at 12 h and 24 h postoperatively. The incidence of request for rescue analgesia varied, with Group BS requesting it more frequently (56%),
| Table 5. adverse effects of the drugs among the study groups | ||||
| Variables | Group BK
(N = 25) |
Group BN
(N = 25) |
Group BS
(N = 25) |
p-value |
| Bradycardia | 0 (0.0) | 3 (12.0) | 0 (0.0) | §0.102 |
| Nausea and vomiting | 1 (4.0) | 3 (12.0) | 3 (12.0) | §0.687 |
| The data are shown as number (%). §Fisher’s Exact test. | ||||
Group BN less frequently (20%), and Group BK least frequently (8%). Table 4 and Figure 4 show that there was a significant variance among Group BS and each of Groups 1 and 2, but not between Groups 1 and 2. Between all the study groups, there were statistically significant variances in total 24-h nalbuphine consumption (P < 0.001, Table 4). Group BS had the highest consumption (18.8 ± 2.3), followed by Group BN (13.1 ± 2.7) and Group BK (7.5 ± 3.5).
The study groups exhibited statistically significant variances in the time to 1st rescue analgesia request. Group BS had the shortest time, at 6.3 ± 1.3 h, followed by Group BN at 11.4 ± 1.5 h, and Group BK at 14.0 ± 1.4 h. Table 4 shows that the differences were significant. There was a non-significant statistical variance in post-surgery nausea and vomiting among the study groups (P = 0.687, Table 5), with Group BK experiencing it least frequently.
4. DISCUSSION
Significant acute postoperative pain is frequently experienced after breast cancer surgeries, requiring a multimodal analgesia regimen that includes regional analgesia. Analgesia for breast and lateral thoracic wall surgeries is provided by SAPB.7 Our study's findings demonstrated that while adding 0.5 mg neostigmine to bupivacaine decreased rate of requesting rescue analgesia, adding 50 mg of ketamine to bupivacaine in SAPB decreased consumption of nalbuphine over a 24-h period and reduced NPS scores. A popular anesthetic with strong local effects on peripheral nerves is ketamine. Ketamine's local action is most likely brought about by voltage-gated sodium channel blockage.16 Ketamine's action on N-methyl-D-aspartate antagonistic inhibition eliminates the noxious stimulation of peripheral afferent neurons.17 Furthermore, nitric oxide synthase is directly inhibited by ketamine, which likely accounts for some of its analgesic effects.18 The research performed by Elnoamany et al.19 examined the influence of ketamine as an adjuvant to bupivacaine in C-arm guided thoracic paravertebral block for patients undergoing modified radical mastectomy. The findings indicated that the addition of 0.5 mg/kg ketamine to 20 ml of 0.25% bupivacaine reduced total amount of analgesic consumption and delayed period to request rescue analgesia, which is consistent with our findings. Additionally, our results aligned with the research conducted by Othman et al.20, which examined the analgesic effectiveness of combining 1 mg/kg ketamine with 30 ml of 0.25% bupivacaine in US-guided modified pectoral block cases undergoing modified radical mastectomy. The results indicated that ketamine increased the duration before patients requested rescue analgesia and decreased the overall amount of morphine consumed. When Ashry et al.21 added 250 mg of magnesium sulfate and 2 mg/kg of ketamine to 25 ml of 2% lidocaine for US-guided supraclavicular brachial plexus block during upper limb surgeries, they observed that the duration of analgesia was extended by both drugs. Also, they discovered that ketamine was a more effective adjuvant than magnesium sulfate because it required less analgesic medication after surgery. In patients undergoing abdominal hysterectomy, Mohamed et al.22 examined the effects of wound infiltration with 2 mg/kg ketamine added to 40 ml of 0.25% bupivacaine versus 2 µg/kg dexmedetomidine added to 40 ml of 0.25% bupivacaine. They found that patients delayed requesting rescue analgesia and that the postoperative stress response was attenuated, especially with ketamine. In contrast to our findings, Omar et al.23 examined the analgesic effectiveness of tramadol 1.5 mg/kg added to 0.5% bupivacaine versus ketamine 0.5 mg/kg added to 0.5% bupivacaine in paravertebral block for breast operations and discovered no differences in the analgesic duration and 24-hour opioid consumption. Additionally, research by Hefni et al.24 compared the analgesic effect of adding 1 mg/kg ketamine versus 1 µg/kg dexmedetomidine to 32 ml of 0.25% bupivacaine in pecsII block in patients undergoing breast surgery. Their findings revealed different pain scores between study groups, and both ketamine and dexmedetomidine significantly extended the time to 1st analgesic request, with dexmedetomidine offering more successful postoperative pain management than ketamine.
Neostigmine works by preventing the neurotransmitter acetylcholine from being broken down.25 The descending control of afferent nociceptive stimuli is improved by neostigmine's inhibition of acetylcholine degradation, according to recent research. This new method offers a way to increase desired analgesia with minimal dose-related side effects.26 In US guided supraclavicular brachial plexus block procedures for the forearm, Hassanin et al.27 examined the impact of adding 0.5 mg neostigmine to 25 ml of 0.5% bupivacaine versus 25 ml of 0.5% bupivacaine and 1 ml of normal saline. Their findings, which were comparable to ours, showed that the neostigmine group required more time to request their first analgesia. Shakya et al.28 also performed a comparative study for patients undergoing total abdominal hysterectomy between intrathecal 5 µg neostigmine added to 3 ml of 0.5% bupivacaine and intrathecal 25 µg fentanyl added to 3 ml of 0.5% bupivacaine. They found that the low dose of intrathecal neostigmine added to bupivacaine provides postoperative analgesia with fewer side effects. As per our findings, Arafa et al.29 evaluated the analgesic efficacy of intraperitoneal 500 µg neostigmine combined with 50 ml of 0.25% bupivacaine versus 50 ml of 0.25% bupivacaine alone on postoperative pain in laparoscopic cholecystectomy. They discovered that neostigmine intraperitoneally increased the duration of postoperative analgesia and decreased the need for analgesic medications. Neostigmine, on the other hand, did not extend the duration of analgesia in children undergoing urethroplasty when Bhardwaj et al.30 added it to caudal bupivacaine at doses of 2, 3, or 4 µg/kg. According to McCartney et al.31, there was neither anesthetic nor analgesic impact when 1 mg of neostigmine was combined with 0.5% lidocaine during intravenous regional anesthesia.
As regards bradycardia 3 patients only developed postoperative bradycardia in Group BN, that was managed by 0.5 mg atropine IV, it may be due to systemic absorption of neostigmine. Kumari Vasantha and Madhusudhana32 compared the efficacy of intrathecal 0.5% bupivacaine versus 50 µg neostigmine added to 0.5% bupivacaine on postoperative pain management in patients undergoing lower abdominal and lower limb operations and found that one patient developed bradycardia in the neostigmine group that was treated with intravenous atropine 0.6 mg.
In our research, all groups did not significantly differ in terms of postoperative nausea and vomiting and it was clinically non-significant and self-limited. Hood et al.33 studied intrathecal neostigmine in doses of 100-200 µg and observed protracted nausea and vomiting.
5. LIMITATIONS
In the present study, a catheter was not inserted to enable long-term postoperative pain relief. Large-scale research is also necessary to determine the best injection techniques for a superficial or deep serratus anterior plane block, and the duration of analgesia with and without adjuvants and usage of different doses of ketamine and neostigmine in order to enhance the post-operative analgesia. Rather than during coughing or movement, we measured the pain on numerical pain rating scale at rest following surgery. The ultrasonic view's resolution and clearance were impacted by the postoperative edema in the surgical field, which also distorted the anatomy.
6. CONCLUSIONS
In cases undergoing modified radical mastectomy, ketamine added to bupivacaine in serratus anterior plane block reduces the pain scores on the numeric pain rating scale as well as 24-hour nalbuphine consumption; neostigmine added to bupivacaine decreases the rate of requesting rescue analgesia
7. Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
8. Ethical issues
This study was approved by the research ethics committee at the faculty of medicine, Ain Shams University (FMASU MD 209/2022) and registered retrospectively with ClinicalTrials.gov Registry, identifier: (NCT05802979). Written informed consent was obtained from all patients.
9. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
MS, manuscript editing
MSA, literature search
ERS, conduction of the study work
AHM, statistical analysis and review
11. REFERENCES
- Woodworth GE, Ivie RMJ, Nelson SM, Walker CM, Maniker RB. Perioperative Breast Analgesia: A Qualitative Review of Anatomy and Regional Techniques. Reg Anesth Pain Med. 2017;42:609-631. PMID: 28820803 DOI: 1097/AAP.0000000000000641
- Wikler A. Opioid dependence: mechanisms and treatment. New York: Springer Science & Business Media; 2013.
- Lynch EP, Welch KJ, Carabuena JM, Eberlein TJ. Thoracic epidural anesthesia improves outcome after breast surgery. Ann Surg. 1995;222:663. PMID: 7487214 DOI: 1097/00000658-199511000-00009
- Kooij FO, Schlack WS, Preckel B, Hollmann MW. Does regional analgesia for major surgery improve outcome? Focus on epidural analgesia. Anesth Analg. 2014;119:740–744. PMID: 25137006 DOI: 1213/ANE.0000000000000245
- Wahba SS, Kamal SM. Thoracic paravertebral block versus pectoral nerve block for analgesia after breast surgery. Egypt J Anaesth. 2014;30:129–135. DOI: 1016/j.egja.2013.10.006
- Blanco R. The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia. 2011;66:847–848. PMID: 21831090 DOI: 1111/j.1365-2044.2011.06838.x
- Razek AA, AbouAllo MM, El Hamid SA, Margany OM. Ultrasound-guided pectoral nerve blocks versus serratus intercostal plane block in breast surgeries. Res Opin Anesthesia Intensive Care. 2018 Jul 1;5(3):162-169. [FreeFullText]
- Rashwan DAEK, Mohammed AR, Kasem Rashwan SA, Abd El Basset AS, Nafady HA. Efficacy of serratus anterior plane block using bupivacaine/magnesium sulfate versus bupivacaine/nalbuphine for mastectomy: a randomized, double-blinded comparative study. Anesth Pain Med. 2020 June;10(3):e103141. PMID: 32944562 DOI: 5812/aapm.103141
- Haas DA, Harper DG. Ketamine: A review of its pharmacologic properties and use in ambulatory anesthesia. Anesth Prog. 1992;39:61-68. PMID: 1308374
- Burburan SM, Xisto DG, Rocco PR. Anesthetic management in asthma. Minerva Anestesiol. 2007;73:357-365. PMID: 17115010
- Elia N, Tramèr MR. Ketamine and postoperative pain: A quantitative systematic review of randomised trials. Pain. 2005;113:61-70. PMID: 15621365 DOI: 1016/j.pain.2004.09.036
- Krukowski JA, Hood DD, Eisenach JC, Mallak KA, Parker RL. Intrathecal neostigmine for post-cesarean section analgesia: Dose response. Anesth Analg. 1997;84:1269-1275. PMID: 9174305 DOI: 1097/00000539-199706000-00018
- Elbahrawy K, El-Deeb A. The effects of adding neostigmine to supraclavicular brachial plexus block for postoperative analgesia in chronic renal failure patients: a prospective randomized double-blinded study. Res Opin Anesthesia Intensive Care. 2016 Jan 1;3(1):36-41. [FreeFullText]
- Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain. 1993;55:195–203. PMID: 8309709 DOI: 1016/0304-3959(93)90148-I
- Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7(1):89-91. PMID: 7772368 DOI: 1016/0952-8180(94)00001-k
- Ismael AH, Latef AH, Al-Shamari AL. Non-opioid analgesia with regional block: The effect of ketamine as adjuvant with 0.5% bupivacaine in infraclavicular brachial plexus block. Mustansiriya Med J. 2012;11(1):78-84. [FreeFullText]
- Trehan V, Srivastava U, Kumar A, Saxena S, Singh CS, Darolia A. Comparison of two approaches of infraclavicular brachial plexus block for orthopedic surgery below mid-humerus. Indian J Anaesth. 2010;54:210-214. PMID: 20885866 DOI: 4103/0019-5049.65362
- Sleigh J, Harvey M, Voss L, Denny B. Ketamine – More mechanisms of action than just NMDA blockade. Trends Anaesth Crit Care. 2014;4:76‑81. DOI: 1016/j.tacc.2014.03.002
- Elnoamany SA, Elsheikh NA, Amer AF, et al. Role of Ketamine as an Adjuvant to Bupivacaine in C-Arm Guided Thoracic Paravertebral Block Analgesia for Modified Radical Mastectomy. Egypt J Hosp Med. 2018;71(5):3153-3157. [FreeFullText]
- Gamal RM, Bossily SS, Ali AR, Samy SF, Seif NE, Ahmed HI. Serratus anterior plane block versus thoracic epidural block in patients undergoing thoracotomy: a randomized double-blind trial. Anaesth. pain intensive care 2023;27(3):389−395.
DOI: 10.35975/apic.v27i3.2243 - Ashry EM, Awad AA, Elkemary F, et al. Comparative study between magnesium sulfate and ketamine added to lidocaine in ultrasound-guided supraclavicular brachial plexus block in upper limb surgery. Sci J Al-Azhar Med Fac, Girls. 2019;3:407–415.
- Mohamed SA, Sayed DM, El Sherif FA, Abd El-Rahman AM. Effect of local wound infiltration with ketamine versus dexmedetomidine on postoperative pain and stress after abdominal hysterectomy, a randomized trial. Eur J Pain. 2018;22(5):951-960. PMID: 29388288 DOI: 1002/ejp.1181
- Omar AM, Mansour MA, Abdelwahab HH, Aboushanab OH. Role of ketamine and tramadol as adjuncts to bupivacaine 0.5% in paravertebral block for breast surgery. A randomized double-blind study. Egypt J Anaesth. 2011;27(2):101-105. DOI: 1016/j.egja.2011.04.002
- Hefni AF, Eldeek AM, Ismael SA, Shaban AR. Comparing Effect of Adding Ketamine Versus Dexmedetomidine to Bupivacaine in Pecs-II Block on Postoperative Pain Control in Patients Undergoing Breast Surgery. Clin J Pain. 2022;38(9):568-574. PMID: 35777735 DOI: 1097/AJP.0000000000001055
- Naguib M, Yaksh TL. Antinociceptive effects of spinal cholinesterase inhibition and isobolographic analysis of the interaction with mu and alpha 2 receptor systems. Anesthesiology. 1994;80:1338-1348. PMID: 8010479 DOI: 1097/00000542-199406000-00022
- Pandey V, Mohindra BK, Sodhi GS. Comparative evaluation of different doses of intrathecal neostigmine as an adjuvant to bupivacaine for postoperative analgesia. Anesth Essays Res. 2016;10(3):538-545.PMID: 27746548 DOI: 4103/0259-1162.180779
- Hassanin AA, Youssef IA, Mohamed HA, Hanna GA. Effect of adding neostigmine to bupivacaine for ultrasound-guided supraclavicular brachial plexus block in forearm surgeries: a randomized, blinded, controlled study. Egypt J Anaesth. 2023;39(1):32-39. DOI: 1080/11101849.2023.2165890
- Shakya ML, Yadav AS, Dwivedi S. Comparative evaluation of intrathecal neostigmine with intrathecal fentanyl for post-operative pain relief. IJSS. 2016;4(5):168-171. [FreeFullText]
- Arafa MS, Ahmed HM, Elnabawy AB, Kassem SF. The evaluation of the analgesic effect of intraperitoneal bupivacaine versus bupivacaine with neostigmine on postoperative pain in laparoscopic cholecystectomy: a randomized controlled double-blinded study. Ain-Shams J Anesthesiol. 2022;14:92. DOI: 1186/s42077-022-00289-0
- Bhardwaj N, Yaddanapudi S, Ghai B, Wig J. Neostigmine does not prolong the duration of analgesia produced by caudal bupivacaine in children undergoing urethroplasty. J Postgrad Med. 2007;53:161-165. PMID: 17699988 DOI: 4103/0022-3859.33856
- McCartney CJ, Brill S, Rawson R, Sanandaji K, Iagounova A, Chan VW. No anesthetic or analgesic benefit of neostigmine 1 mg added to intravenous regional anesthesia with lidocaine 0.5% for hand surgery. Reg Anesth Pain Med. 2003;28(5):414–417. PMID: 14556131 DOI: 1016/s1098-7339(03)00217-7
- Kumari Vasantha NS, Madhusudhana R. Intrathecal Bupivacaine with Neostigmine and Bupivacaine with Normal Saline for Postoperative Analgesia: A Cost-effective Additive. Anesth Essays Res. 2018;12(2):328-332. PMID: 29962592 DOI: 4103/aer.AER_184_17
- Hood DD, Eisenach JC, Tuttle R. Phase I safety assessment of intrathecal neostigmine methyl sulfate in humans. Anesthesiology. 1995;82:331-343. PMID: 7856891 DOI: 1097/00000542-199502000-00003