Yuka Matsuki1, Koji Hosokawa2*, Ayako Uchino3, Shuko Matsuda4, Kenji Shigemi5
Author affiliations:
Background & objective: Lung atelectasis is a known complication of general anesthesia, and especially in patients undergoing laparoscopic surgical procedures. Respiratory system compliance (Crs) is a measured sign of lung atelectasis in laparoscopic surgery. A protocolized sequential alveolar recruitment maneuver (RM) with positive end-expiratory pressure (PEEP) was compared to a usual management.
Methodology: Patients scheduled for elective laparoscopic radical prostatectomy under extreme Trendelenburg position were randomly allocated to one of the two groups; either PEEP plus alveolar RM in every 30 min (RM group) or PEEP only (PEEP group). The primary outcome was the time-dependent differences in Crs between the groups, that was tested using multivariate analysis of variance (MANOVA).
Results: Between 19 patients in the RM group and 17 patients in the PEEP group, patients’ demography was balanced. The time depended difference in Crs was significantly higher in the RM group than in the non-RM group. Postoperative atelectasis occurred in one patient in the PEEP group, whose Crs was 34 cmH2O/mL at the time of intubation. In the subgroup with initial low Crs (< 60 cmH2O/mL), the time-dependent difference in Crs was significantly higher in the RM group than the PEEP group.
Conclusion: In the subgroup with initial low respiratory system compliance (< 60 cmH2O/mL), the time-dependent difference in respiratory system compliance was significantly higher in the RM group than in the PEEP group, suggesting that the therapeutic target of RM would be initially low respiratory system compliance patients.
Abbreviations: Crs - Respiratory system compliance; RM - recruitment maneuver; PEEP - positive end-expiratory pressure
Keywords: Respiratory System Compliance; Lung Recruitment Maneuver; Lung Mechanics; Atelectasis; Randomized Control Trial
Citation: Matsuki Y, Hosokawa K, Uchino A, Matsuda S, Shigemi K. Sequential alveolar recruitment maneuvers during laparoscopic radical prostatectomy: a pilot randomized control trial. Anaesth. pain intensive care 2024;28(2):329−332; DOI: 10.35975/apic.v28i2.2407
Received: February 16, 2024; Revised: February 16, 2024; Accepted: March 11, 2024
Lung atelectasis is troublesome after Trendelenburg positioned laparoscopic prostatectomy.1-3 Alveolar recruitment maneuvers (RMs) would be plausible to maintain respiratory system compliance (Crs),4 however, no concrete protocol has been established. We compared the changes in Cr and clinical outcomes using protocolized sequential RMs in every 30 min.
This study was conducted with the approval of the ethics committee of the University of Fukui (#20160055) and with patients’ informed consent for study participation. A total of 36 adult patients scheduled for elective laparoscopic radical prostatectomy under general anesthesia (October 2016–March 2018) were enrolled. The patients were randomly allocated to either PEEP (5–8 cmH2O) plus alveolar RM of 30 cmH2O for 20 sec (RM group) or PEEP (5–8 cmH2O) only (PEEP group). In the RM group, the RM was performed at predetermined several time points and every 30 min during pneumoperitoneum. All patients received volume-guaranteed pressure-controlled ventilation with a tidal volume of 6–8 mL/kg (ideal body weight). Crs (basically calculated by tidal volume / peak inspiratory pressure – positive end-expiratory pressure (PEEP)) was displayed on Aisys CS 2 (GE healthcare, Chicago, IL) using manufacture-driven calculations. During the surgery, the patients were placed in the 25‒30° Trendelenburg position. Time-dependent differences between the groups were compared using multivariate analysis of variance (MANOVA) using JMP 16 (SAS, Cary, NC). Post hoc analysis was performed in the subgroup with low and high initial Crs.
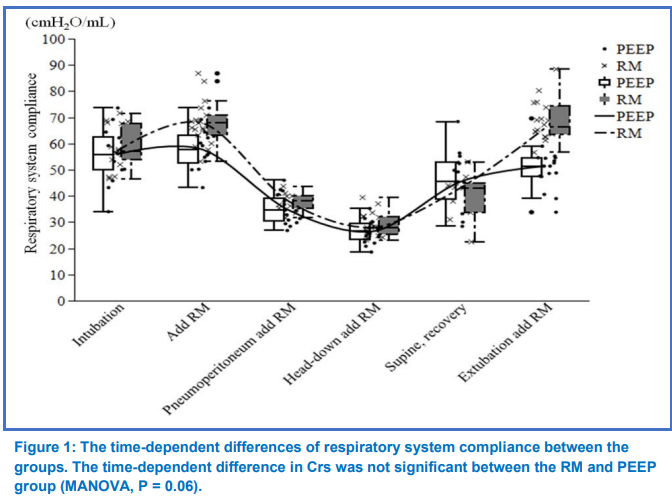
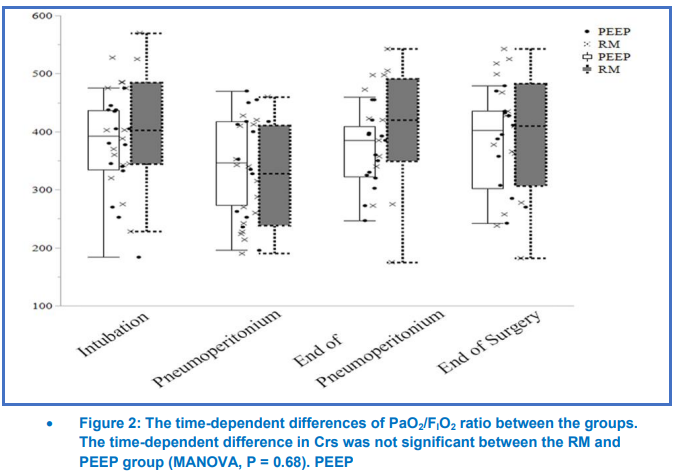
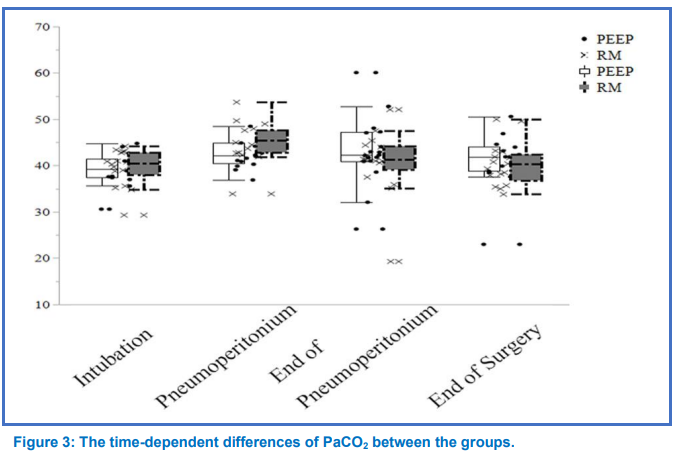
Between 19 patients in the RM group and 17 patients in the PEEP group, no significant differences in patients’ demography (Table 1). At several measured points, the mean of Crs were higher in the RM group than in the PEEP group. However, the time-dependent difference in Crs or gas exchanges were not significant (Figures 1-3).
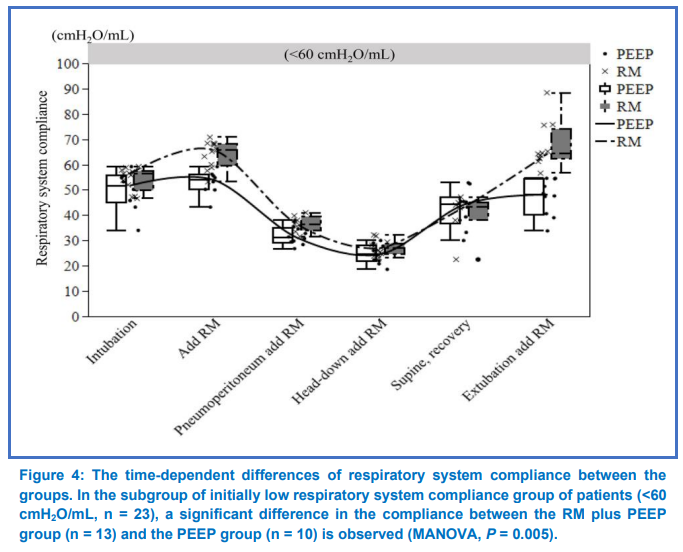
Postoperative atelectasis occurred in one patient in the PEEP group who had a low Crs (34 cmH2O/mL) at intubation and as low as 34 cmH2O/mL before extubation. On post hoc analysis, in the subgroup with initial low Crs at intubation (Crs < 60 cmH2O/mL; the RM group, n = 13; the PEEP group, n = 10), the time-dependent difference in Crs was significantly higher in the RM group than in the PEEP group (Figure 4, P = 0.005).
A previous report showed that intraoperative Crs and the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2 ratio) increased more in the RM group than in the control group,5 however that was controversial.6 The discrepancies were thought to be differences in the method or timing of RM. The RM method in the present study involved vital capacity maneuvers that applied a continuous, fixed, high pressure in every 30 min. We did not identify the optimal RM method, however, the initially low Crs group showed high recruit-ability. While RM would not be appropriate for all patients, for laparoscopic surgery in the Trendelenburg position, RM can cause concerns with respect to hemodynamics.7 Moreover, prostatectomy has a risk of bleeding responsible for pelvic vascular network, although recently the bleeding is normally minimized since of using laparoscopy. The future studies would find the patients group which benefit from intraoperative Crs management.
Several limitations were noted. First, this study was a small single-center study. Second, because of a relatively long time to enrolled patients, practices may have changed. Third, the effects of patient factors, including obesity or pulmonary function, were not considered. Fourth, perioperative outcomes were not fully examined.
The present pilot study showed that the time-course of respiratory system compliance values similarly maintained in 30-min interval RM group compared with normal PEEP group. Additionally, in the subgroup with initial low respiratory system compliance (< 60 cmH2O/mL), the time-dependent difference in respiratory system compliance was significantly higher in the RM group than in the PEEP group, suggesting that the therapeutic target of RM would be initially low compliance patients.
7. Data availability
The datasets generated and/or analyzed during the current study are not publicly available to avoid unintended use, but are available from the corresponding author on reasonable request.
8. Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
9. Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
10. Authors' contributions:
YM: Formal analysis, visualization, and writing-original draft.
KH: Conceptualization, methodology, formal analysis, visualization, validation, and writing- reviewing and editing.
AU: validation, and writing- reviewing and editing.
SM: visualization, and writing- reviewing and editing.
KS: Supervision, and writing- reviewing and editing.
11. Registration No.
UMIN CTR, UMIN000053311
Author affiliations:
- Yuka Matsuki, Department of Anesthesiology & Reanimatology, Faculty of Medical Sciences, University of Fukui, Fukui, Japan; E-mail: ymatsuki@u-fukui.ac.jp
- Koji Hosokawa, Department of Anesthesiology & Reanimatology, Faculty of Medical Sciences, University of Fukui, Fukui, Japan; E-mail: khosok@u-fukui.ac.jp
- Ayako Uchino, Department of Anesthesiology & Reanimatology, Faculty of Medical Sciences, University of Fukui / Sugita Genpaku Memorial Obama Municipal Hospital, Fukui, Japan; E-mail: okuno.aya2@gmail.com
- Shuko Matsuda, Department of Anesthesiology & Reanimatology, Faculty of Medical Sciences, University of Fukui, Fukui, Japan; E-mail: matshu@u-fukui.ac.jp
- Kenji Shigemi, Department of Anesthesiology & Reanimatology, Faculty of Medical Sciences, University of Fukui, Fukui, Japan; E-mail: kshigemi@u-fukui.ac.jp
ABSTRACT
Background & objective: Lung atelectasis is a known complication of general anesthesia, and especially in patients undergoing laparoscopic surgical procedures. Respiratory system compliance (Crs) is a measured sign of lung atelectasis in laparoscopic surgery. A protocolized sequential alveolar recruitment maneuver (RM) with positive end-expiratory pressure (PEEP) was compared to a usual management.
Methodology: Patients scheduled for elective laparoscopic radical prostatectomy under extreme Trendelenburg position were randomly allocated to one of the two groups; either PEEP plus alveolar RM in every 30 min (RM group) or PEEP only (PEEP group). The primary outcome was the time-dependent differences in Crs between the groups, that was tested using multivariate analysis of variance (MANOVA).
Results: Between 19 patients in the RM group and 17 patients in the PEEP group, patients’ demography was balanced. The time depended difference in Crs was significantly higher in the RM group than in the non-RM group. Postoperative atelectasis occurred in one patient in the PEEP group, whose Crs was 34 cmH2O/mL at the time of intubation. In the subgroup with initial low Crs (< 60 cmH2O/mL), the time-dependent difference in Crs was significantly higher in the RM group than the PEEP group.
Conclusion: In the subgroup with initial low respiratory system compliance (< 60 cmH2O/mL), the time-dependent difference in respiratory system compliance was significantly higher in the RM group than in the PEEP group, suggesting that the therapeutic target of RM would be initially low respiratory system compliance patients.
Abbreviations: Crs - Respiratory system compliance; RM - recruitment maneuver; PEEP - positive end-expiratory pressure
Keywords: Respiratory System Compliance; Lung Recruitment Maneuver; Lung Mechanics; Atelectasis; Randomized Control Trial
Citation: Matsuki Y, Hosokawa K, Uchino A, Matsuda S, Shigemi K. Sequential alveolar recruitment maneuvers during laparoscopic radical prostatectomy: a pilot randomized control trial. Anaesth. pain intensive care 2024;28(2):329−332; DOI: 10.35975/apic.v28i2.2407
Received: February 16, 2024; Revised: February 16, 2024; Accepted: March 11, 2024
1. INTRODUCTION
Lung atelectasis is troublesome after Trendelenburg positioned laparoscopic prostatectomy.1-3 Alveolar recruitment maneuvers (RMs) would be plausible to maintain respiratory system compliance (Crs),4 however, no concrete protocol has been established. We compared the changes in Cr and clinical outcomes using protocolized sequential RMs in every 30 min.
2. METHODOLOGY
This study was conducted with the approval of the ethics committee of the University of Fukui (#20160055) and with patients’ informed consent for study participation. A total of 36 adult patients scheduled for elective laparoscopic radical prostatectomy under general anesthesia (October 2016–March 2018) were enrolled. The patients were randomly allocated to either PEEP (5–8 cmH2O) plus alveolar RM of 30 cmH2O for 20 sec (RM group) or PEEP (5–8 cmH2O) only (PEEP group). In the RM group, the RM was performed at predetermined several time points and every 30 min during pneumoperitoneum. All patients received volume-guaranteed pressure-controlled ventilation with a tidal volume of 6–8 mL/kg (ideal body weight). Crs (basically calculated by tidal volume / peak inspiratory pressure – positive end-expiratory pressure (PEEP)) was displayed on Aisys CS 2 (GE healthcare, Chicago, IL) using manufacture-driven calculations. During the surgery, the patients were placed in the 25‒30° Trendelenburg position. Time-dependent differences between the groups were compared using multivariate analysis of variance (MANOVA) using JMP 16 (SAS, Cary, NC). Post hoc analysis was performed in the subgroup with low and high initial Crs.
3. RESULTS
Between 19 patients in the RM group and 17 patients in the PEEP group, no significant differences in patients’ demography (Table 1). At several measured points, the mean of Crs were higher in the RM group than in the PEEP group. However, the time-dependent difference in Crs or gas exchanges were not significant (Figures 1-3).
Postoperative atelectasis occurred in one patient in the PEEP group who had a low Crs (34 cmH2O/mL) at intubation and as low as 34 cmH2O/mL before extubation. On post hoc analysis, in the subgroup with initial low Crs at intubation (Crs < 60 cmH2O/mL; the RM group, n = 13; the PEEP group, n = 10), the time-dependent difference in Crs was significantly higher in the RM group than in the PEEP group (Figure 4, P = 0.005).
4. DISCUSSION
A previous report showed that intraoperative Crs and the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2 ratio) increased more in the RM group than in the control group,5 however that was controversial.6 The discrepancies were thought to be differences in the method or timing of RM. The RM method in the present study involved vital capacity maneuvers that applied a continuous, fixed, high pressure in every 30 min. We did not identify the optimal RM method, however, the initially low Crs group showed high recruit-ability. While RM would not be appropriate for all patients, for laparoscopic surgery in the Trendelenburg position, RM can cause concerns with respect to hemodynamics.7 Moreover, prostatectomy has a risk of bleeding responsible for pelvic vascular network, although recently the bleeding is normally minimized since of using laparoscopy. The future studies would find the patients group which benefit from intraoperative Crs management.
5. LIMITATIONS
Several limitations were noted. First, this study was a small single-center study. Second, because of a relatively long time to enrolled patients, practices may have changed. Third, the effects of patient factors, including obesity or pulmonary function, were not considered. Fourth, perioperative outcomes were not fully examined.
| Table 1: Characteristics of patients | |||
| Variables | RM group
(n = 19) |
PEEP group
(n = 17) |
P value |
| Age (y) | 68 ± 4 | 67 ± 7 | 0.595 |
| Height (cm) | 167 ± 6 | 167 ± 6 | 0.970 |
| Weight (kg) | 68 ± 9 | 67 ± 9 | 0.837 |
| Body mass index (kg/m2) | 24 ± 2 | 24 ± 2 | 0.738 |
| Duration of anesthesia (min) | 261 ± 40 | 270 ± 51 | 0.574 |
| Duration of pneumoperitoneum (min) | 165 ± 38 | 174 ± 47 | 0.547 |
| ASA-PS
· 1 · 2 · 3 |
4 (21) 14 (74) 1 (5) |
1 (6) 15 (88) 1 (6) |
0.421 |
| Data presented as mean ± SD, or n (%); P < 0.05 considered as significant | |||
6. CONCLUSIONS
The present pilot study showed that the time-course of respiratory system compliance values similarly maintained in 30-min interval RM group compared with normal PEEP group. Additionally, in the subgroup with initial low respiratory system compliance (< 60 cmH2O/mL), the time-dependent difference in respiratory system compliance was significantly higher in the RM group than in the PEEP group, suggesting that the therapeutic target of RM would be initially low compliance patients.
7. Data availability
The datasets generated and/or analyzed during the current study are not publicly available to avoid unintended use, but are available from the corresponding author on reasonable request.
8. Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
9. Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
10. Authors' contributions:
YM: Formal analysis, visualization, and writing-original draft.
KH: Conceptualization, methodology, formal analysis, visualization, validation, and writing- reviewing and editing.
AU: validation, and writing- reviewing and editing.
SM: visualization, and writing- reviewing and editing.
KS: Supervision, and writing- reviewing and editing.
11. Registration No.
UMIN CTR, UMIN000053311
12. REFERENCES
- Kim MS, Soh S, Kim SY, Song MS, Park JH. Comparisons of pressure-controlled ventilation with volume guarantee and volume-controlled 1:1 equal ratio ventilation on oxygenation and respiratory mechanics during robot-assisted laparoscopic radical prostatectomy: a randomized-controlled trial. Int J Med Sci 2018;15:1522-9. PMID: 30443174 DOI: 7150/ijms.28442
- Lee JM, Lee SK, Rhim CC, Seo KH, Han M, Kim SY, et al. Comparison of volume-controlled, pressure-controlled, and pressure-controlled volume-guaranteed ventilation during robot-assisted laparoscopic gynecologic surgery in the Trendelenburg position. Int J Med Sci 2020;17:2728-34. PMID: 33162800 DOI: 7150/ijms.49253
- Choi EM, Na S, Choi SH, An J, Rha KH, Oh YJ. Comparison of volume-controlled and pressure-controlled ventilation in steep Trendelenburg position for robot-assisted laparoscopic radical prostatectomy. J Clin Anesth 2011;23:183-8. PMID: 21377341 DOI: 1016/j.jclinane.2010.08.006
- Hartland BL, Newell TJ, Damico N. Alveolar recruitment maneuvers under general anesthesia: a systematic review of the literature. Respir Care 2015;60:609-20. PMID: 25425708 DOI: 4187/respcare.03488
- Sprung J, Whalen FX, Comfere T, Bosnjak ZJ, Bajzer Z, Gajic O, et al. Alveolar recruitment and arterial desflurane concentration during bariatric surgery. Anesth Analg 2009;108:120-7. PMID: 19095839 DOI: 1213/ane.0b013e31818db6c7
- Severgnini P, Selmo G, Lanza C, Chiesa A, Frigerio A, Bacuzzi A, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013;118:1307-21. PMID: 23542800 DOI: 1097/ALN.0b013e31829102de