Indriasari1, Ezra Oktaliansah2, Rikda Irham Munazat3
Author affiliations:
Background and Objectives: Nearly three-quarters of the patients with COVID-19 received antibiotic therapy despite the bacterial coinfection being only less than 10% in many studies and ranging from 8-22% in ICU patients. The use of broad-spectrum antibiotics in COVID-19 patients has not been proven effective. Overuse of antibiotics may be associated with side effects and antibiotic resistance. The purpose of this study was to determine the antibiotic rationality in COVID-19 patients in the ICU of Dr. Hasan Sadikin Hospital, Bandung, Indonesia.
Methodology: This descriptive, retrospective cohort study was carried out by analyzing medical records of COVID-19 patients admitted in the ICU of Dr. Hasan Sadikin Hospital from January-June 2021.
Results: There were 138 patients who met the inclusion criteria. A total of 126 (91.3%) patients received antibiotics. A total of 12 (8.7%) severe/critical patients did not receive antibiotics and 79 (62.70%) received inappropriate antibiotic duration. Inappropriate regimen was found in 59 patients (74.68%) with COVID-19 without HAP/VAP and 15 patients (31.92%) with HAP/VAP. The primary issue identified was the inappropriate regimen of antibiotics, Gyssens category 4a.
Conclusion: This study concludes that 23.02% patients used rational empirical antibiotics and 45.98% used rational definitive antibiotics in COVID-19 patients in the ICU at RSUP Dr. Hasan Sadikin Bandung during January-June 2021.
Abbreviations: ACE- Angiotensin Converting Enzyme; ICU- Intensive Care Unit; HAI- Hospital-Associated Infections; HAP- Hospital-Acquired Pneumonia; IDSA- Infectious Diseases Society of America VAP- Ventilator-Associated Pneumonia
Key words: Antibiotics; Antimicrobial Resistance; COVID-19; Intensive Care Units; Prescribing Pattern
Citation: Indriasari, Oktaliansah E, Munazat RI. Rationality of antibiotic use in COVID-19 patients in the ICU of Dr. Hasan Sadikin General Hospital Bandung; a cohort study. Anaesth. pain intensive care 2024;28(1):115−125.
DOI: 10.35975/apic.v28i1.2384
Received: November 20, 2023; Reviewed: December 03, 2023; Accepted: December 26, 2023
COVID-19 was officially designated as a pandemic in March 2020, resulting from the SARS-CoV-2 virus, which gains access to human cells by means of the spike protein interacting with the angiotensin-converting enzyme 2 (ACE-2) receptor. The management strategy for mild and moderate cases of COVID-19 primarily encompass home care and self-isolation. However, 14% of severe cases and 5% of critical cases necessitate hospitalization and admission to the intensive care unit (ICU).1
COVID-19 patients undergoing treatment in the ICU are susceptible to hospital-acquired infections due to invasive interventions, such as mechanical ventilation, central venous catheters, and Foley catheters, which can elevate the risk of hospital-associated infections (HAI). Nearly three-quarters of COVID-19 patients receive irrational antibiotic therapy, despite the prevalence of bacterial coinfections being as low as <10% in some studies and ranging from 8-22% among ICU patients.2,3
The Indonesian COVID-19 guidelines recommend empiric antibiotic therapy for severe and critical cases of COVID-19 and do not recommend its use in mild to moderate cases unless there is suspicion of bacterial infection. The choice and duration of empiric antibiotic therapy align with community-acquired pneumonia treatment guidelines. For patients with Ventilator-Associated Pneumonia (VAP) or Hospital-Acquired Pneumonia (HAP), the choice of empiric antibiotics follows established guidelines for HAP/VAP inpatient cases.4,5
Evaluating the use of definitive antibiotics in COVID-19 pneumonia patients is crucial to reduce drug toxicity and antimicrobial resistance. Microbiological culture results should be obtained before administering definitive antibiotics, and therapy should be adjusted based on culture results. Blood and sputum cultures are performed on patients to identify the causative microorganisms of the infection and serve as a reference for prescribing the appropriate definitive antibiotics. Sputum culture is a straightforward method that can be used to detect respiratory pathogens associated with COVID-19 pneumonia.3,6
During COVID-19 pandemic, the establishment of the COVID ICU is a recent development, and there is currently a paucity of comprehensive data concerning microbial patterns derived from the results of microorganism cultures within the COVID ICU. The administration of antibiotics in the COVID ICU at Dr. Hasan Sadikin General Hospital Bandung adheres to the guidelines set forth by the Ministry of Health for the management of COVID-19. As a result, the author aims to gain a deeper understanding of the rationale of antibiotic administration, guided by the established protocols. This investigation focuses on evaluating the appropriateness of indications, the selection of antibiotic regimens, duration of treatment, the chosen method of administration, dosing intervals, and the dosages employed in the care of COVID-19 patients within the COVID ICU at Dr. Hasan Sadikin General Hospital.
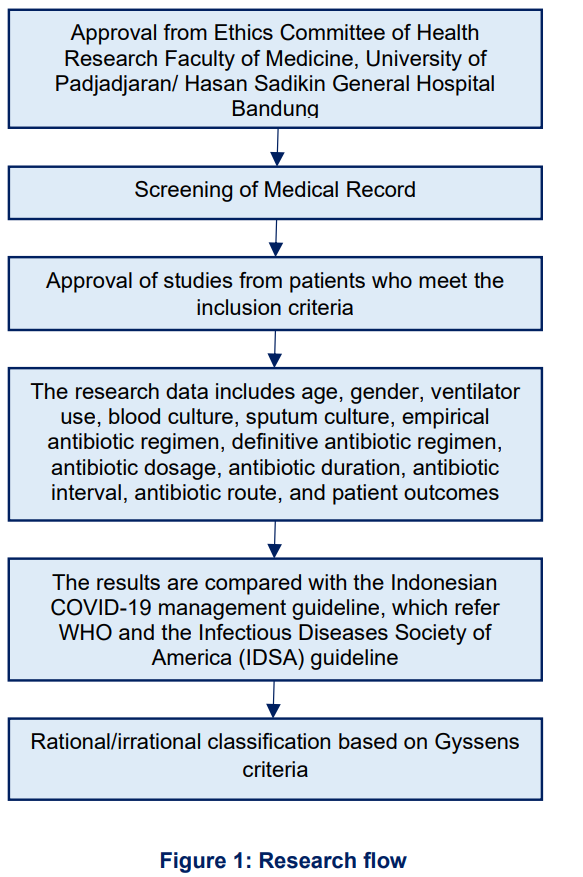
This study is an observational descriptive study. The study subjects include all severe or critical COVID-19 patients treated in the COVID ICU at Dr. Hasan Sadikin General Hospital Bandung from January to June 2021 who meet the inclusion criteria, are over 18 years old, and have been diagnosed with COVID-19 based on PCR swab results. Exclusion criteria for this study are incomplete medical records.
This research has been approved with research permit number DP.04.03/X2.2.1/4065/2023 and ethical permit number LB.02.01/X.6.5/40/2023 from the institutional Ethics Committee. This research was conducted retrospectively on the medical records of COVID-19 patients treated in the ICU at RSUP Dr. Hasan Sadikin Bandung from January to June 2021. Subsequently, research data was collected from patient medical records, including gender, age, ventilator use, COVID-19 severity, case criteria with or without HAP/VAP, empiric antibiotic regimen, definitive antibiotic regimen, antibiotic duration, antibiotic dosage, antibiotic interval, antibiotic route, blood culture results, sputum culture results, and patient outcomes.
Empiric antibiotic data were then compared to the COVID-19 management guidelines in Indonesia, which refer to the WHO and Infectious Diseases Society of America (IDSA) COVID-19 guidelines. According to the Indonesian COVID-19 guidelines, recommended empiric antibiotics for severe/critical COVID-19 patients are intravenous ceftriaxone 50-100 mg/kg/24 h or intravenous azithromycin 10 mg/kg/24 h for 5 days. The 2016 IDSA guidelines recommend antibiotics for COVID-19 patients with HAP/VAP, including piperacillin-tazobactam, cefepime, ceftazidime, levofloxacin, ciprofloxacin, imipenem, meropenem, aztreonam, amikacin, gentamicin, tobramycin, vancomycin, and linezolid for 7 days. The definitive antibiotic data were analyzed for rationality based on blood and sputum culture results and antibiotic sensitivity. Subsequently, the rationality of the data was categorized based on Gyssens criteria.
This study was conducted on 138 severely or critically ill patients in the COVID ICU at Hasan Sadikin General Hospital, Bandung, during the period of January to June 2021.
The characteristics of severe and critical COVID-19 patients in the COVID-19 Intensive Care Unit at Hasan Sadikin Hospital in Bandung can be seen in Table 1. The average age is 55.9 years, with a minimum age of 18 and a maximum of 87 years. A total of 68 patients used a ventilator (49.3%).
The indication for antibiotic administration in COVID-19 patients in the COVID-19 Intensive Care Unit at Hasan Sadikin Hospital in Bandung revealed that out of 126 patients receiving antibiotics, 56 (40.58%) received antibiotics for severe COVID-19 and 70 (50.72%) for critical cases (51.70%). Meanwhile, 10 (7.25%) severe cases and 2 (1.45%) critical cases did not receive antibiotics (Table 2). Based on Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP) criteria, 10 (7.25%) were diagnosed with HAP, and 37 were diagnosed with VAP (26.81%) According to Table 3 which illustrates the duration of antibiotic use, there were 4 patients (5.06%) without Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) who received medication for the appropriate 5 days duration and 9 patients (19.15%) with HAP/VAP who received treatment for the appropriate 7 days duration (Table 3).
Cultures were conducted for 87 patients, including 55 blood cultures only, 23 sputum cultures only, and 9 patients underwent both examinations. Among the 30 patients receiving antibiotics based on blood culture results, 14 patients (21.88%) continued with empirical antibiotics, 12 patients (18.75%) were discontinued upon receiving antibiotics due to the absence of microorganisms, and in 4 patients (6.25%) antibiotic was changed based on the culture results. Among the 19 patients receiving antibiotics based on sputum culture results, 9 patients (25%) continued with the same empirical antibiotics, and 10 patients (31.25%) received different antibiotics than the empirical regimen.
All patients (100%) received antibiotics through the appropriate intravenous route according to guidelines.
Table 4 describes the appropriate empirical antibiotic regimen in patients without HAP/VAP was found in 20 (25.32%) patients. A total of 59 (74.68%) patients received an inappropriate regimen, with levofloxacin being the most commonly administered antibiotic, followed by the combination of ceftriaxone and levofloxacin. No instance of inaccurate dosages and intervals of medications was identified. Within the cohort of COVID-19 patients afflicted with HAP/VAP, a total of 32 individuals (68.08%) received an appropriate therapeutic regimen, primarily comprising meropenem and levofloxacin. Nonetheless, it is noteworthy that one patient (2.13%) was prescribed piperacillin with a dosage deemed inappropriate. A total of 64 patients underwent blood culture, and 32 patients underwent sputum culture. The most common result in blood culture was the absence of microorganisms (60.9%), while Acinetobacter baumannii was found in 46.38% of sputum cultures (Table 5).
The categorization of the rationality of empirical and definitive antibiotic use based on the Gyssens criteria can be observed in Table 8. Patients receiving rational antibiotics were identified in 29 cases (23.02%) for empirical antibiotics and 40 cases (45.98%) for definitive antibiotics. The most common Gyssens category for empirical antibiotics was category IVA, indicating the presence of another more effective regimen in 50 patients (39.68%), and category V, signifying inappropriate indications in 29 patients (33.33%).
In the ICU, nosocomial infections are observed in up to 30% of patients, representing an incidence 5-10 times higher than in non-ICU patients. Antibiotic use in the ICU is, therefore ten times higher than in traditional inpatient settings. The ICU, characterized by a substantial infectious disease burden, exhibits the highest antibiotic consumption, accounting for an estimated 71% of patients receiving antibiotics. Nonetheless, around one-third of antibiotic prescriptions in the ICU are considered inappropriate. Antibiotic prescription rates were higher in adults aged 18-39 and 40-64 compared to younger age groups. The presence of comorbidities was positively correlated with an increased rate of antibiotic prescription. These findings were consistent with the outcomes of the present study, where the mean patient age is 56.49 years, aligning with the prevalence of severe and critical cases. Notably, empirical antibiotics were administered to only 126 patients (91.3%) with severe and critical COVID-19 treated in the ICU in this study. Studies conducted in the United States have documented a relationship between antibiotic use and prolonged hospital stay, particularly in ICU patients requiring mechanical ventilation.2,3,7
In this study, antibiotics were administered based on indications in 56 patients (40.58%) with severe COVID-19 and 70 patients (50.72%) with critical COVID-19. A study conducted in Sierra Leone found a significantly higher prevalence of antibiotic use in patients with mild, moderate, and severe COVID-19 compared to asymptomatic patients. The prevalence of antibiotic use was higher in older patients compared to younger ones.8
The recommended antibiotic regimen for COVID-19 in Indonesia is ceftriaxone and azithromycin for cases without HAP/VAP. Ceftriaxone was the most commonly used antibiotic in patients without HAP/VAP (24.05%). This aligns with a literature review of 19 studies on antibiotic use in COVID-19 patients, which found that fluoroquinolones were the most commonly used antibiotics in 56.8% of patients, followed by ceftriaxone in 39.5% of patients, and azithromycin in 29.1% of patients. Only 2 patients were found to be using carbapenems. Duration of antibiotic administration ranged from 3 to 17 days, with a median of 5 days. A total of 59 patients (74.68%) without HAP/VAP did not receive antibiotic regimens according to guidelines. Additionally, 24 patients (30.38%) received a combination of ceftriaxone and levofloxacin.
The selection of empirical antibiotics for VAP/HAP is guided by the microbiological and resistance patterns specific to each hospital. According to the 2016 IDSA guidelines, recommended antibiotics for cases of HAP/VAP include piperacillin-tazobactam, cefepime, ceftazidime, levofloxacin, ciprofloxacin, meropenem, imipenem, aztreonam, and vancomycin.5 In patients with HAP/VAP in this study, meropenem emerged as the predominant antibiotic, administered to 10 patients (21.28%). A total of 15 (31.92%) patients received antibiotic regimens that did not adhere to the guidelines, with 5 (10.64%) patients receiving a combination of levofloxacin and ceftriaxone, and another 5 patients (10.64%) receiving a combination of amikacin and tigecycline.
A total of 79 (62.70%) patients were prescribed antibiotics with duration that did not align with the recommended guidelines. Among them, 45 (35.71%) patients received antibiotics for a duration shorter than recommendation, resulting in 32 (25.39%) of them recovered, 3 (2.38%) passed away during 5 days of treatment, and 10 (7.94%) with an unknown cause for discontinuation.
This study identified prolonged antibiotic use beyond guideline recommendations in 68 (53.97%) patients Within these cases, 34 (26.98%) were awaiting culture results, 11 (8.73%) demonstrated resistance to the prescribed empirical antibiotics, 20 (15.87%) continued antibiotic treatment despite the absence of microorganisms in culture results, and 3 (2.38%) patients had an unknown reason for continuation of antibiotics. The 34 patients awaiting culture results were classified into the category of appropriate treatment duration, consisting of 16 patients without HAP/VAP and 18 patients with HAP/VAP.
The decision to extend antibiotic treatment beyond the recommended duration is made when the patient's condition has not shown improvement, resistance to the prescribed antibiotics, or the availability of alternative antibiotic option deemed more suitable based on the culture results. Research on patients with bacteremia revealed that 25% of patients received irrational antibiotic prescriptions. Patient comorbidities, the identification of multidrug-resistant microorganisms, non-compliance with guidelines, and errors in clinical assessment influence the administration of rational antibiotic therapy.9
Pneumonia poses challenges for definitive therapy, even in cohort studies with regularly scheduled cultures, where microorganisms are only identified in a subset of cases. Consequently, the majority of antibiotic prescriptions for pneumonia are based on regional microbial trends or syndromic presentations, guideline recommendations, or established prescription practices, rather than targeting the specific infecting organisms. There are three examinations employed to determine the etiology of bacterial pneumonia: respiratory tract cultures, blood cultures, and serum or urine antigen tests. Each testing modality has limitations, including the high rate of oral flora contamination in respiratory tract cultures (low specificity), low positive rates in blood cultures (low sensitivity), and the limited target range of antigenic testing.10
Blood and sputum cultures were conducted in this study to identify the microorganisms causing infections in patients and serve as a reference for prescribing the appropriate definitive antibiotics. A total of 87 patients (69.04%) underwent microbial cultures. Among the 87 patients, 55 (43.65%) had blood cultures only, 23 (18.25%) had sputum cultures only, and 9 (7.14%) had both examinations. Sputum culture was essential for identifying the microorganisms causing pneumonia in this study, but it was only performed on 32 patients. This is attributed to the fact that some patients, comprising 37 individuals (29.4%) recovered with empirical antibiotics, whereas 46 patients (36.5%) died, and the cause remained unidentified in 11 patients (8.7%).
Sputum culture is easily conducted and can be utilized to detect respiratory pathogens associated with COVID-19 pneumonia. A notably high rate of bacterial co-infection and secondary infections was identified in a retrospective study, accounting for 23.3% and 16.95%, respectively. Various studies have reported a widely varying prevalence of bacterial superinfection in COVID-19 patients, ranging from 1% to 50%, which can be attributed to differences in criteria and diagnostic tests. In this study, Pseudomonas aeruginosa emerged as the most commonly identified pathogenic bacterium in sputum samples, followed by Klebsiella pneumoniae and Escherichia coli. This is attributed to the frequent need for mechanical ventilation in critically ill COVID-19 patients in the ICU, combined with prolonged periods of heavy sedation, supine positioning, and muscle relaxant use, all of which can elevate the risk of secondary nosocomial infections, particularly Ventilator-Associated Pneumonia (VAP). Pulmonary microbiome studies have reported an increase in Staphylococcus, Streptococcus, and Enterobacter in patients with COVID-19.11,12
Definitive antibiotics in this case were administered after receiving blood and sputum culture results to determine the appropriate antibiotic for the patient. A total of 30 patients (46.88%) received antibiotics in accordance with blood culture results, and 19 patients (59.37%) received antibiotics based on sputum culture results. Inappropriate antibiotic treatment in 29 patients (33.33%) occurred when antibiotics were administered to patients with fungal and no microorganisms were identified in culture examination. Additionally, 12 patients (12.78%) received inappropriate antibiotic regimens because there was no replacement of the antibiotic regimen that was identified resistant to culture results.
Research in Sierra Leone found that nearly half of all confirmed COVID-19 patients received antibiotics. Approximately six out of ten suspected COVID-19 patients were prescribed antibiotics without proper indication according to WHO guidelines and national case management protocols. Besides the misuse of antibiotics among COVID-19 patients, researchers could draw conclusions about the importance of relevant prescribing practices by physicians to establish antimicrobial stewardship programs in healthcare facilities that are conducted irrationally. This trend is consistent with reports from various other countries in the African region (47% in Kenya, 71% in South Africa, and 76% in Uganda) and elsewhere (78% in Spain, 83% in the US, 100% in Bangladesh, and 67-90% in several studies from China), indicating the high usage of antibiotics in COVID-19 patients.8,13
The results of this study indicated a 76.98% inappropriate utilization of empirical antibiotics, surpassing the 60% observed in a Sierra Leone study. This discrepancy might be attributed to a higher antibiotic use in Southeast Asian and Middle Eastern countries than in other continents. Additionally, it could be affected by the fact that the subjects in the Sierra Leone study included patients of all ages, while in this study, the average patient age was 55.59 years, and older patients were found to receive more antibiotics. The Sierra Leone study also examined subjects with different categories of suspected and confirmed COVID-19, including asymptomatic, mild, moderate, severe, and critical, which differs from this study where only severe and critical confirmed COVID-19 patients were investigated.8
A study in Singapore reported contrasting results, with a very low antibiotic use rate (5%) and appropriate indications observed in 60.8% of cases. This variance may be attributed to differences in the characteristics of the study subjects; the Singapore study had a higher proportion of male participants (75%) compared to this study (57.2%). The average age of participants was also younger (45.5 years). The low antibiotic use could also be a consequence of the Singaporean study focusing on patients in regular inpatient settings, with only 1.9% of patients admitted to the ICU. Additionally, the study examined white blood cell count, C-reactive protein, and procalcitonin levels, which were not assessed in this study. The evaluation of antibiotic usage was also performed by infectious disease specialists in 42% of cases, contributing to the reduced antibiotic usage outside indications.14 Inappropriate antibiotic use during the COVID-19 pandemic can lead to increased multidrug resistance and is associated with longer hospital stays and higher costs for patients and hospital management.15
The irrational use of definitive antibiotics in this study may be attributed to the absence of blood and sputum culture examinations for all COVID-19 patients admitted to the ICU. Microorganism cultures serve to identify the causative agents of infections in patients, and the omission of these tests results in a less precise assessment of definitive antibiotic appropriateness. Furthermore, differences in the experiences of ICU doctors can also influence the variation in antibiotics administered to patients.
Another study found that the use of antibiotics in COVID-19 patients was common and contributed to more than three-quarters of patients. This percentage aligns with findings in other cohorts and meta-analyses. Only 10% of patients were given antibiotics after confirming the presence of lung infection, while 2% experienced other infections due to catheter-related bacteremia and urinary tract infections.16
The rationality of antibiotics was classified based on Gyssens criteria, with 29 patients (23.02%) received empiric antibiotics that were rational according to the COVID-19 treatment guidelines in Indonesia and the IDSA pneumonia therapy guidelines. The category of irrational empiric antibiotics includes 50 patients (39.68%) in category IVA, indicating the presence of a more effective regimen, 26 patients (20.63%) in category I indicating inappropriate timing, 6 patients (4.76%) in category IIIA indicating longer duration, 14 patients (11.11%) in category IIIB indicating shorter duration, and 1 patient (0.79%) in category IIA indicating inappropriate dosage. Eight patients (6.35%), initially categorized as IIIA, including 2 patients (1.59%) without HAP/VAP and 6 patients (4.76%) with HAP/VAP, were reclassified as rational because these patients were still awaiting culture results to determine the subsequent administration of definitive antibiotics. Among patients receiving definitive antibiotics, 40 patients (45.98%) received rational antibiotics, and 37 (42.52%) received irrational antibiotics. The categories of irrational definitive antibiotics include 29 patients (33.33%) in category V, 12 patients (13.78%) in category IVA, 5 patients (5.46%) in category IIIB, and 1 patient (1.15%) in category I.
The excessive and inappropriate use of antibiotics in COVID-19 patients can lead to increased antibiotic resistance. Prescription of antibiotics inappropriately elevates the risk of toxicity and morbidity, with the benefits of administration not proven to date, even in critically ill COVID-19 patients.15 Inappropriate antibiotic prescriptions result from various factors; management protocols in March and April 2020 recommended doctors to prescribe empirical antibiotics to almost all patients, regardless of the presence of indications.17 However, the Indonesian COVID-19 guidelines recommend the use of ceftriaxone and/or azithromycin for severe/critical cases only.4 The need for establishing specific criteria for antibiotic use in COVID-19 patients has been emphasized, resulting in clinical guidelines for antibiotic prescription in COVID-19 patients. The primary recommendation is to limit drug use, especially upon initial admission when bacterial infections are less common. The guidelines suggest delaying the initial use of antibiotics that might have been started in the emergency department.4,16 An additional measure that could be implemented involves improving education regarding the proper use of antibiotics, both in regular healthcare settings and among individuals with COVID-19.18
This study identified that 23.02% of empirical antibiotic use and 45.98% definitive antibiotic use among COVID-19 patients were rational in the ICU of RSUP Dr. Hasan Sadikin Bandung from January to June 2021. The administration of empirical antibiotics to ICU patients with COVID-19 should adhere more closely to available management guidelines to prevent excessive antibiotic use and mitigate the escalation of antibiotic resistance.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Hospital Dr. Hasan Sadikin, Bandung, Indonesia
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
IDS, EOL: Concept, reviewer important intellectual content, final approver of the version to be published
RIM: Concept, conduction of the study work, statistical analysis, and manuscript editing
Author affiliations:
- Indriasari, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Hospital Dr. Hasan Sadikin, Bandung, Indonesia; E-mail: sari_anestesi@yahoo.co.id
- Ezra Oktaliansah, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Hospital Dr. Hasan Sadikin, Bandung, Indonesia; E-mail: ianoktalian@yahoo.com
- Rikda Irham Munazat, Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Hospital Dr. Hasan Sadikin, Bandung, Indonesia; E-mail: rikdairhammunazat@gmail.com
ABSTRACT
Background and Objectives: Nearly three-quarters of the patients with COVID-19 received antibiotic therapy despite the bacterial coinfection being only less than 10% in many studies and ranging from 8-22% in ICU patients. The use of broad-spectrum antibiotics in COVID-19 patients has not been proven effective. Overuse of antibiotics may be associated with side effects and antibiotic resistance. The purpose of this study was to determine the antibiotic rationality in COVID-19 patients in the ICU of Dr. Hasan Sadikin Hospital, Bandung, Indonesia.
Methodology: This descriptive, retrospective cohort study was carried out by analyzing medical records of COVID-19 patients admitted in the ICU of Dr. Hasan Sadikin Hospital from January-June 2021.
Results: There were 138 patients who met the inclusion criteria. A total of 126 (91.3%) patients received antibiotics. A total of 12 (8.7%) severe/critical patients did not receive antibiotics and 79 (62.70%) received inappropriate antibiotic duration. Inappropriate regimen was found in 59 patients (74.68%) with COVID-19 without HAP/VAP and 15 patients (31.92%) with HAP/VAP. The primary issue identified was the inappropriate regimen of antibiotics, Gyssens category 4a.
Conclusion: This study concludes that 23.02% patients used rational empirical antibiotics and 45.98% used rational definitive antibiotics in COVID-19 patients in the ICU at RSUP Dr. Hasan Sadikin Bandung during January-June 2021.
Abbreviations: ACE- Angiotensin Converting Enzyme; ICU- Intensive Care Unit; HAI- Hospital-Associated Infections; HAP- Hospital-Acquired Pneumonia; IDSA- Infectious Diseases Society of America VAP- Ventilator-Associated Pneumonia
Key words: Antibiotics; Antimicrobial Resistance; COVID-19; Intensive Care Units; Prescribing Pattern
Citation: Indriasari, Oktaliansah E, Munazat RI. Rationality of antibiotic use in COVID-19 patients in the ICU of Dr. Hasan Sadikin General Hospital Bandung; a cohort study. Anaesth. pain intensive care 2024;28(1):115−125.
DOI: 10.35975/apic.v28i1.2384
Received: November 20, 2023; Reviewed: December 03, 2023; Accepted: December 26, 2023
1. INTRODUCTION
COVID-19 was officially designated as a pandemic in March 2020, resulting from the SARS-CoV-2 virus, which gains access to human cells by means of the spike protein interacting with the angiotensin-converting enzyme 2 (ACE-2) receptor. The management strategy for mild and moderate cases of COVID-19 primarily encompass home care and self-isolation. However, 14% of severe cases and 5% of critical cases necessitate hospitalization and admission to the intensive care unit (ICU).1
COVID-19 patients undergoing treatment in the ICU are susceptible to hospital-acquired infections due to invasive interventions, such as mechanical ventilation, central venous catheters, and Foley catheters, which can elevate the risk of hospital-associated infections (HAI). Nearly three-quarters of COVID-19 patients receive irrational antibiotic therapy, despite the prevalence of bacterial coinfections being as low as <10% in some studies and ranging from 8-22% among ICU patients.2,3
The Indonesian COVID-19 guidelines recommend empiric antibiotic therapy for severe and critical cases of COVID-19 and do not recommend its use in mild to moderate cases unless there is suspicion of bacterial infection. The choice and duration of empiric antibiotic therapy align with community-acquired pneumonia treatment guidelines. For patients with Ventilator-Associated Pneumonia (VAP) or Hospital-Acquired Pneumonia (HAP), the choice of empiric antibiotics follows established guidelines for HAP/VAP inpatient cases.4,5
Evaluating the use of definitive antibiotics in COVID-19 pneumonia patients is crucial to reduce drug toxicity and antimicrobial resistance. Microbiological culture results should be obtained before administering definitive antibiotics, and therapy should be adjusted based on culture results. Blood and sputum cultures are performed on patients to identify the causative microorganisms of the infection and serve as a reference for prescribing the appropriate definitive antibiotics. Sputum culture is a straightforward method that can be used to detect respiratory pathogens associated with COVID-19 pneumonia.3,6
During COVID-19 pandemic, the establishment of the COVID ICU is a recent development, and there is currently a paucity of comprehensive data concerning microbial patterns derived from the results of microorganism cultures within the COVID ICU. The administration of antibiotics in the COVID ICU at Dr. Hasan Sadikin General Hospital Bandung adheres to the guidelines set forth by the Ministry of Health for the management of COVID-19. As a result, the author aims to gain a deeper understanding of the rationale of antibiotic administration, guided by the established protocols. This investigation focuses on evaluating the appropriateness of indications, the selection of antibiotic regimens, duration of treatment, the chosen method of administration, dosing intervals, and the dosages employed in the care of COVID-19 patients within the COVID ICU at Dr. Hasan Sadikin General Hospital.
2. METHODOLOGY
This study is an observational descriptive study. The study subjects include all severe or critical COVID-19 patients treated in the COVID ICU at Dr. Hasan Sadikin General Hospital Bandung from January to June 2021 who meet the inclusion criteria, are over 18 years old, and have been diagnosed with COVID-19 based on PCR swab results. Exclusion criteria for this study are incomplete medical records.
| Table 1: Characteristics of research subject | |
| Patient Characteristics | n (%) |
| Gender
· Men · Women |
79 (57.2%) 59 (42.3%) |
| Age (y)
· Average ± SD · Range |
55.9 ± 16.5 18-87 |
| Ventilator Use
· Yes · No |
68 (49.3%) 70 (50.7%) |
This research has been approved with research permit number DP.04.03/X2.2.1/4065/2023 and ethical permit number LB.02.01/X.6.5/40/2023 from the institutional Ethics Committee. This research was conducted retrospectively on the medical records of COVID-19 patients treated in the ICU at RSUP Dr. Hasan Sadikin Bandung from January to June 2021. Subsequently, research data was collected from patient medical records, including gender, age, ventilator use, COVID-19 severity, case criteria with or without HAP/VAP, empiric antibiotic regimen, definitive antibiotic regimen, antibiotic duration, antibiotic dosage, antibiotic interval, antibiotic route, blood culture results, sputum culture results, and patient outcomes.
Empiric antibiotic data were then compared to the COVID-19 management guidelines in Indonesia, which refer to the WHO and Infectious Diseases Society of America (IDSA) COVID-19 guidelines. According to the Indonesian COVID-19 guidelines, recommended empiric antibiotics for severe/critical COVID-19 patients are intravenous ceftriaxone 50-100 mg/kg/24 h or intravenous azithromycin 10 mg/kg/24 h for 5 days. The 2016 IDSA guidelines recommend antibiotics for COVID-19 patients with HAP/VAP, including piperacillin-tazobactam, cefepime, ceftazidime, levofloxacin, ciprofloxacin, imipenem, meropenem, aztreonam, amikacin, gentamicin, tobramycin, vancomycin, and linezolid for 7 days. The definitive antibiotic data were analyzed for rationality based on blood and sputum culture results and antibiotic sensitivity. Subsequently, the rationality of the data was categorized based on Gyssens criteria.
3. RESULTS
This study was conducted on 138 severely or critically ill patients in the COVID ICU at Hasan Sadikin General Hospital, Bandung, during the period of January to June 2021.
The characteristics of severe and critical COVID-19 patients in the COVID-19 Intensive Care Unit at Hasan Sadikin Hospital in Bandung can be seen in Table 1. The average age is 55.9 years, with a minimum age of 18 and a maximum of 87 years. A total of 68 patients used a ventilator (49.3%).
| Table 2: Empirical Antibiotic Administration | ||
| Empirical Antibiotic Indication | Receiving antibiotic (%) | Not receiving antibiotic (%) |
| Classification of COVID-19
Severe Critical |
56 (40.58) 70 (50.72%) |
10 (7.25%) 2 (1.45%) |
| Case Criteria
COVID-19 without HAP/VAP COVID-19 with HAP COVID-19 with VAP |
79 (57,25 %) 10 (7,25%) 37 (26,81%) |
12 (8,69%) 0 0 |
| HAP: Hospital-acquired pneumonia; VAP: Ventilator-associated pneumonia | ||
| Table 3: Duration of antibiotic use | |
| Duration (days) | N (%) |
| COVID-19 without HAP/VAP (n = 79) | |
| 5 days < 5 days > 5 days |
4 (5.06%) 36 (45.57%) 39 (49.37%) |
| COVID-19 with HAP/VAP (n = 47) | |
| 7 days < 7 days > 7 days |
9 (19.15%%) 9 (19.15%) 29 (61.70%) |
| Appropriateness of antibiotic duration (n = 126) | |
| Appropriate duration Inappropriate duration |
47 (37.30%) 79 (62.70%) |
The indication for antibiotic administration in COVID-19 patients in the COVID-19 Intensive Care Unit at Hasan Sadikin Hospital in Bandung revealed that out of 126 patients receiving antibiotics, 56 (40.58%) received antibiotics for severe COVID-19 and 70 (50.72%) for critical cases (51.70%). Meanwhile, 10 (7.25%) severe cases and 2 (1.45%) critical cases did not receive antibiotics (Table 2). Based on Hospital-Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia (VAP) criteria, 10 (7.25%) were diagnosed with HAP, and 37 were diagnosed with VAP (26.81%) According to Table 3 which illustrates the duration of antibiotic use, there were 4 patients (5.06%) without Hospital-Acquired Pneumonia (HAP)/Ventilator-Associated Pneumonia (VAP) who received medication for the appropriate 5 days duration and 9 patients (19.15%) with HAP/VAP who received treatment for the appropriate 7 days duration (Table 3).
| Table 4: Overview of Antibiotic Regimen, Dosage, and Administration Interval | |
| Antibiotic regimen, dosage, and administration interval | N (%) |
| A. COVID-19 without HAP/VAP (N = 79) | |
| Appropriate regimen according to guideline
Ceftriaxone 50-100 mg/kg/24 h Azithromycin 10 mg/kg |
N = 20 (25.32)
19 (24.05) 1 (1.27) |
| Inappropriate regimen according to guideline
Levofloxacin 750 mg/day Meropenem 1 g/8 h Cefotaxime 2g/8 h Ceftriaxone 50-100 mg/kg/24 h + levofloxacin 1x750 mg Levofloxacin 750 mg/day + meropenem 1 g/8 h Meropenem 1 g/8 h + amikacin 15-20 mg/day Ceftriaxone 50-100 mg/kg/24 h + meropenem 1 g/8 h Levofloxacin 750 mg/day + azithromycin 10 mg/kg Meropenem 1 g/8 h + ceftazidime 1 g/8 h + levofloxacin 750 mg/day |
N = 59 (74.68)
10 (12.66) 2 (2.53) 1 (1.27) 24 (30,38) 14 (17,72) 5 (6,33) 1 (1,27) 1 (1,27) 1 (1,27) |
| Inappropriate dosage according to guideline | 0 (0) |
| Inappropriate interval according to guideline | 0 (0) |
| B. COVID-19 with HAP/VAP (N = 47) | |
| Appropriate regimen according to guideline
Meropenem 1 g/8 h Levofloxacin 750 mg/day Meropenem 1 g/8 h + levofloxacin 750 mg/day Meropenem 1 g/8 h + amikacin 15-20 mg/day Meropenem 1 g/8 h + vancomycin 15 mg/kg/8-12 h Piperacillin taxobactam 4,5 g/6 h + Vancomycin 15 mg/kg/8-12 h |
N = 32 (68.08)
10 (21.28) 1 (2.13) 11 (23.4) 7 (14.89) 4 (8.51) 1 (2.13) |
| Inappropriate regimen according to guideline
Ceftriaxone 50-100 mg/kg/24 h Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/day Amikacin 15-20 mg/day + Tigecycline 50 mg/12 h Vancomycin 15 mg/kg/8-12 h + tigecycline 50 mg/12 h Meropenem 1 g/8 h + ceftriaxone 50-100 mg/kg/24 h Meropenem 1 g/8 h + ceftriaxone 50-100 mg/kg/24 h + Levofloxacin 750 mg/day |
N = 15 (31.92)
2 (4.26) 5 (10.64) 5 (10.64) 1 (2.13) 1 (2.13) 1 (2.13) |
| Inappropriate dosage according to guideline
Piperacillin |
1 (2.13) |
| Inappropriate interval according to guideline | 0 |
| Data presented as n (%) | |
Cultures were conducted for 87 patients, including 55 blood cultures only, 23 sputum cultures only, and 9 patients underwent both examinations. Among the 30 patients receiving antibiotics based on blood culture results, 14 patients (21.88%) continued with empirical antibiotics, 12 patients (18.75%) were discontinued upon receiving antibiotics due to the absence of microorganisms, and in 4 patients (6.25%) antibiotic was changed based on the culture results. Among the 19 patients receiving antibiotics based on sputum culture results, 9 patients (25%) continued with the same empirical antibiotics, and 10 patients (31.25%) received different antibiotics than the empirical regimen.
All patients (100%) received antibiotics through the appropriate intravenous route according to guidelines.
Table 4 describes the appropriate empirical antibiotic regimen in patients without HAP/VAP was found in 20 (25.32%) patients. A total of 59 (74.68%) patients received an inappropriate regimen, with levofloxacin being the most commonly administered antibiotic, followed by the combination of ceftriaxone and levofloxacin. No instance of inaccurate dosages and intervals of medications was identified. Within the cohort of COVID-19 patients afflicted with HAP/VAP, a total of 32 individuals (68.08%) received an appropriate therapeutic regimen, primarily comprising meropenem and levofloxacin. Nonetheless, it is noteworthy that one patient (2.13%) was prescribed piperacillin with a dosage deemed inappropriate. A total of 64 patients underwent blood culture, and 32 patients underwent sputum culture. The most common result in blood culture was the absence of microorganisms (60.9%), while Acinetobacter baumannii was found in 46.38% of sputum cultures (Table 5).
| Table 5: Microorganism culture results | |
| Blood Culture | n = 64 |
| No microorganism Staphylococcus sp. MRSA Acinetobacter baumannii Enterobacter Candida sp. Pseudomonas aeruginosa Aeromonas hydrophila Klebsiella sp. |
39 (60.9) 7 (10.9) 6 (9.3) 4 (6.25) 2 (3.2) 2 (3.2) 2 (3.2) 1 (1.5) 1 (1.5) |
| Sputum Culture | n = 32 |
| Acinetobacter baumannii Klebsiella sp. Candica albicans Pseudomonas sp. Staphylococcus sp. Stenotrophomonas maltophilia Enterobacter MRSA No microorganism |
15 (46.88) 6 (18.75) 2 (6.25) 2 (6.25) 2 (6.25) 2 (6.25) 1 (3.13) 1 (3.13) 1 (3.13) |
| Data presented as n (%) | |
The categorization of the rationality of empirical and definitive antibiotic use based on the Gyssens criteria can be observed in Table 8. Patients receiving rational antibiotics were identified in 29 cases (23.02%) for empirical antibiotics and 40 cases (45.98%) for definitive antibiotics. The most common Gyssens category for empirical antibiotics was category IVA, indicating the presence of another more effective regimen in 50 patients (39.68%), and category V, signifying inappropriate indications in 29 patients (33.33%).
4. DISCUSSION
In the ICU, nosocomial infections are observed in up to 30% of patients, representing an incidence 5-10 times higher than in non-ICU patients. Antibiotic use in the ICU is, therefore ten times higher than in traditional inpatient settings. The ICU, characterized by a substantial infectious disease burden, exhibits the highest antibiotic consumption, accounting for an estimated 71% of patients receiving antibiotics. Nonetheless, around one-third of antibiotic prescriptions in the ICU are considered inappropriate. Antibiotic prescription rates were higher in adults aged 18-39 and 40-64 compared to younger age groups. The presence of comorbidities was positively correlated with an increased rate of antibiotic prescription. These findings were consistent with the outcomes of the present study, where the mean patient age is 56.49 years, aligning with the prevalence of severe and critical cases. Notably, empirical antibiotics were administered to only 126 patients (91.3%) with severe and critical COVID-19 treated in the ICU in this study. Studies conducted in the United States have documented a relationship between antibiotic use and prolonged hospital stay, particularly in ICU patients requiring mechanical ventilation.2,3,7
In this study, antibiotics were administered based on indications in 56 patients (40.58%) with severe COVID-19 and 70 patients (50.72%) with critical COVID-19. A study conducted in Sierra Leone found a significantly higher prevalence of antibiotic use in patients with mild, moderate, and severe COVID-19 compared to asymptomatic patients. The prevalence of antibiotic use was higher in older patients compared to younger ones.8
The recommended antibiotic regimen for COVID-19 in Indonesia is ceftriaxone and azithromycin for cases without HAP/VAP. Ceftriaxone was the most commonly used antibiotic in patients without HAP/VAP (24.05%). This aligns with a literature review of 19 studies on antibiotic use in COVID-19 patients, which found that fluoroquinolones were the most commonly used antibiotics in 56.8% of patients, followed by ceftriaxone in 39.5% of patients, and azithromycin in 29.1% of patients. Only 2 patients were found to be using carbapenems. Duration of antibiotic administration ranged from 3 to 17 days, with a median of 5 days. A total of 59 patients (74.68%) without HAP/VAP did not receive antibiotic regimens according to guidelines. Additionally, 24 patients (30.38%) received a combination of ceftriaxone and levofloxacin.
The selection of empirical antibiotics for VAP/HAP is guided by the microbiological and resistance patterns specific to each hospital. According to the 2016 IDSA guidelines, recommended antibiotics for cases of HAP/VAP include piperacillin-tazobactam, cefepime, ceftazidime, levofloxacin, ciprofloxacin, meropenem, imipenem, aztreonam, and vancomycin.5 In patients with HAP/VAP in this study, meropenem emerged as the predominant antibiotic, administered to 10 patients (21.28%). A total of 15 (31.92%) patients received antibiotic regimens that did not adhere to the guidelines, with 5 (10.64%) patients receiving a combination of levofloxacin and ceftriaxone, and another 5 patients (10.64%) receiving a combination of amikacin and tigecycline.
A total of 79 (62.70%) patients were prescribed antibiotics with duration that did not align with the recommended guidelines. Among them, 45 (35.71%) patients received antibiotics for a duration shorter than recommendation, resulting in 32 (25.39%) of them recovered, 3 (2.38%) passed away during 5 days of treatment, and 10 (7.94%) with an unknown cause for discontinuation.
| Table 6: Definitive antibiotic regimen based on blood culture (Contd) | ||||||
| Blood culture | Antibiotic pre culture | N (%) | Antibiotic post culture | N (%) | Rational | Irrational |
| No microorganism | Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/24 h | 17 (26.56) | Same regimen | 9 (14.06) | 9 (14.06) |
|
| Antibiotic discontinued | 2 (3.13) | 2 (3.13) | ||||
| Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 1 (1.56) | 1 (1.56) | ||||
| Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 10 (15.63) | Same regimen | 5 (7.81) | 5 (7.81) | ||
| Antibiotic discontinued | 5 (7.81) | 5 (7.81) | ||||
| Meropenem 1 g/8 h | 2 (3.13) | Same regimen | 1 (1.56) | 1 (1.56) | ||
| Meropenem 1 g/8 h + Vancomycin 1 g/24 h | 1 (1.56) | 1 (1.56) | ||||
| Meropenem 1 g/8 h + Amikacin 1 g/24 h | 3 (4.69) | Same regimen | 1 (1.56) | 1 (1.56) | 1 (1.56) | |
| Amikacin 1 g/24 h + Cefepime 2g/8 h | 1 (1.56) | 1 (1.56) | ||||
| Levofloxacin 750 mg/day + | 4 (6.25) | Same regimen | 1 (1,56) | 1 (1,56) | ||
| Antibiotic discontinued | 3 (4.69) | 3 (4.69) | ||||
| Ceftriaxone 50-100 mg/kg/24 h | 6 (9.38) | Same regimen | 3 (4.69) | 3 (4.69) | ||
| Antibiotic discontinued | 2 (3.13) | 2 (3.13) | ||||
| Meropenem 1 g/8 h | 1 (1.56) | 1 (1,56) | ||||
| Ceftriaxone 50-100 mg/kg/24 h + Meropenem 1 g/8 h | 1 (1.56) | Same regimen | 1 (1.56) | 1 (1.56) | ||
| Meropenem 1 g/8 h + Vancomycin 1 g/24 h | 1 (1.56) | Vancomycin 1 g/24 h + Cefepime 2g/8 h | 1 (1.56) | 1 (1.56) | ||
| Total | Rationality | 30 (46.88) | 34 (53.12) | |||
| Same regimen: 39 (60.94) Antibiotic discontinued: 12 (18.75) Switched regimen: 13 (20.31) |
||||||
This study identified prolonged antibiotic use beyond guideline recommendations in 68 (53.97%) patients Within these cases, 34 (26.98%) were awaiting culture results, 11 (8.73%) demonstrated resistance to the prescribed empirical antibiotics, 20 (15.87%) continued antibiotic treatment despite the absence of microorganisms in culture results, and 3 (2.38%) patients had an unknown reason for continuation of antibiotics. The 34 patients awaiting culture results were classified into the category of appropriate treatment duration, consisting of 16 patients without HAP/VAP and 18 patients with HAP/VAP.
| Table 7: Definitive Antibiotic Regimen Based on Sputum Culture | ||||||
| Blood culture | Antibiotic pre culture | N (%) | Antibiotic post culture | N (%) | Rational | Irrational |
| Acinetobacter baumannii | Meropenem 1 g/8 h + Amikacin 1 g/24 h | 7 (21.8) |
Same regimen | 5(15,6) | 3 (9,4) | 2 (6,25) |
| Meropenem 1 g/8 h + Tigecycline 100 mg/day |
1 (3.1) | 1 (3.1) | ||||
| Vancomycin 1 g/day + Tigecycline 100 mg/day | 1 (3.1) | 1 (3.1) | ||||
| Amikacin 1 g/day+ Tigecycline 100 mg/day | 2 (6.25) | Same regimen | 2 6.25) | 2 (6.25) | ||
| Meropenem 1 g/8 h + Vancomycin 1 g/day | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1) | ||
| Vancomycin 1 g/12 h + Tigecycline 100g/day | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1) | ||
| Meropenem 1 g/8 h | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1) | ||
| Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 2 (6.25) | Same regimen | 2(6.25) | 2 (6.25) | ||
| Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/day | 1 (3.1) | Meropenem 1 g/8 h + Amikacin 1 g/day | 1 (3.1) | 1 (3.1) | ||
| Candida albicans | Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/24h | 1(3.1) | Same regimen | 1 (3.1) | 1 (3.1) | |
| Meropenem 1 g/8 h + Vancomycin 1 g/24 h | 1 (3.1) | Vancomycin 1 g/day + Cefepime 2 g/8 h | 1 (3.1) | 1 (3.1) | ||
| Enterobacter | Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1) | |
| Klebsiella pneumoniae | Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/24h | 3 (9.3) | Same regimen | 3 (3.1) | 2 (6.25) | 1 (3.1) |
| Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 2 (6.25) | Same regimen | 1 (3.1) | 1 (3.1) | ||
| Tigecycline 50 mg/12 h + Fosfomycin 2 g/12 h | 1 (3.1) | 1 (3.1) | ||||
| Meropenem 1 g/8 h | 1 (3.1) | Same regimen | 1 (3,1) | 1 (3,1) | ||
| MRSA | Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1) | |
| Pseudomonas aeruginosa | Ceftriaxone 50-100 mg/kg/24 h | 2 (6.25) | Same regimen | 2 (6.25) | 2 (6.25) | |
| Staphylococcus sp. | Levofloxacin 750 mg/day | 1 (3.1) | Meropenem 1 g/8 h + Levofloxacin 750 mg/day | 1(3.1) | 1 (3.1) | |
| Ceftriaxone 50-100 mg/kg/24 h | 1 (3.1) | Amikacin 15-20 mg/kg/day + Vancomycin 15 mg/kg/8-12 h | 1 (3.1) | 1 (3.1%) | ||
| Stenotrophomonas maltophilia | Levofloxacin 750 mg/day + Ceftriaxone 50-100 mg/kg/24 h | 1 (3.1) | Same regimen | 1 (3.1) | 1 (6.25%) | |
| Ceftriaxone 50-100 mg/kg/24 h + Azithromycin 10 mg/kg | 1 (3.1) | Meropenem 1 g/8 h + Amikacin 15-20 mg/kg/day | 1 (3.1) | 1 (3.1%) | ||
| No microorganism | Levofloxacin 750 mg/day | 1 (3.1) | Same regimen | 1 (3.1) | 1 (3.1%) | |
| Total | Same regimen Switching regimen |
22 (68.75) 10 (31.25) |
19 (59.38) | 13 (40.62) | ||
The decision to extend antibiotic treatment beyond the recommended duration is made when the patient's condition has not shown improvement, resistance to the prescribed antibiotics, or the availability of alternative antibiotic option deemed more suitable based on the culture results. Research on patients with bacteremia revealed that 25% of patients received irrational antibiotic prescriptions. Patient comorbidities, the identification of multidrug-resistant microorganisms, non-compliance with guidelines, and errors in clinical assessment influence the administration of rational antibiotic therapy.9
| Table 8: Rationality of antibiotic administration according to Gyssens Criteria | ||
| Rationality According to Gyssens Criteria | Empiric
(n = 126) |
Definitive
(n = 87) |
| Rational Irrational Category I Irrational Category IIA Irrational Category IIB Irrational Category IIC Irrational Category IIIA Irrational Category IIIB Irrational Category IVA Irrational Category IVB Irrational Category IVC Irrational Category IVD Irrational Category V Irrational Category VI |
29 (23.02) 26 (20.63) 1 (0.79) 0 0 6 (4.76) 14 (11.11) 50 (39.68) 0 0 0 0 0 |
40 (45.98) 1(1.15) 0 0 0 0 5 (5.46) 12 (13.78) 0 0 0 29 (33.33) 0 |
Pneumonia poses challenges for definitive therapy, even in cohort studies with regularly scheduled cultures, where microorganisms are only identified in a subset of cases. Consequently, the majority of antibiotic prescriptions for pneumonia are based on regional microbial trends or syndromic presentations, guideline recommendations, or established prescription practices, rather than targeting the specific infecting organisms. There are three examinations employed to determine the etiology of bacterial pneumonia: respiratory tract cultures, blood cultures, and serum or urine antigen tests. Each testing modality has limitations, including the high rate of oral flora contamination in respiratory tract cultures (low specificity), low positive rates in blood cultures (low sensitivity), and the limited target range of antigenic testing.10
Blood and sputum cultures were conducted in this study to identify the microorganisms causing infections in patients and serve as a reference for prescribing the appropriate definitive antibiotics. A total of 87 patients (69.04%) underwent microbial cultures. Among the 87 patients, 55 (43.65%) had blood cultures only, 23 (18.25%) had sputum cultures only, and 9 (7.14%) had both examinations. Sputum culture was essential for identifying the microorganisms causing pneumonia in this study, but it was only performed on 32 patients. This is attributed to the fact that some patients, comprising 37 individuals (29.4%) recovered with empirical antibiotics, whereas 46 patients (36.5%) died, and the cause remained unidentified in 11 patients (8.7%).
Sputum culture is easily conducted and can be utilized to detect respiratory pathogens associated with COVID-19 pneumonia. A notably high rate of bacterial co-infection and secondary infections was identified in a retrospective study, accounting for 23.3% and 16.95%, respectively. Various studies have reported a widely varying prevalence of bacterial superinfection in COVID-19 patients, ranging from 1% to 50%, which can be attributed to differences in criteria and diagnostic tests. In this study, Pseudomonas aeruginosa emerged as the most commonly identified pathogenic bacterium in sputum samples, followed by Klebsiella pneumoniae and Escherichia coli. This is attributed to the frequent need for mechanical ventilation in critically ill COVID-19 patients in the ICU, combined with prolonged periods of heavy sedation, supine positioning, and muscle relaxant use, all of which can elevate the risk of secondary nosocomial infections, particularly Ventilator-Associated Pneumonia (VAP). Pulmonary microbiome studies have reported an increase in Staphylococcus, Streptococcus, and Enterobacter in patients with COVID-19.11,12
Definitive antibiotics in this case were administered after receiving blood and sputum culture results to determine the appropriate antibiotic for the patient. A total of 30 patients (46.88%) received antibiotics in accordance with blood culture results, and 19 patients (59.37%) received antibiotics based on sputum culture results. Inappropriate antibiotic treatment in 29 patients (33.33%) occurred when antibiotics were administered to patients with fungal and no microorganisms were identified in culture examination. Additionally, 12 patients (12.78%) received inappropriate antibiotic regimens because there was no replacement of the antibiotic regimen that was identified resistant to culture results.
Research in Sierra Leone found that nearly half of all confirmed COVID-19 patients received antibiotics. Approximately six out of ten suspected COVID-19 patients were prescribed antibiotics without proper indication according to WHO guidelines and national case management protocols. Besides the misuse of antibiotics among COVID-19 patients, researchers could draw conclusions about the importance of relevant prescribing practices by physicians to establish antimicrobial stewardship programs in healthcare facilities that are conducted irrationally. This trend is consistent with reports from various other countries in the African region (47% in Kenya, 71% in South Africa, and 76% in Uganda) and elsewhere (78% in Spain, 83% in the US, 100% in Bangladesh, and 67-90% in several studies from China), indicating the high usage of antibiotics in COVID-19 patients.8,13
The results of this study indicated a 76.98% inappropriate utilization of empirical antibiotics, surpassing the 60% observed in a Sierra Leone study. This discrepancy might be attributed to a higher antibiotic use in Southeast Asian and Middle Eastern countries than in other continents. Additionally, it could be affected by the fact that the subjects in the Sierra Leone study included patients of all ages, while in this study, the average patient age was 55.59 years, and older patients were found to receive more antibiotics. The Sierra Leone study also examined subjects with different categories of suspected and confirmed COVID-19, including asymptomatic, mild, moderate, severe, and critical, which differs from this study where only severe and critical confirmed COVID-19 patients were investigated.8
A study in Singapore reported contrasting results, with a very low antibiotic use rate (5%) and appropriate indications observed in 60.8% of cases. This variance may be attributed to differences in the characteristics of the study subjects; the Singapore study had a higher proportion of male participants (75%) compared to this study (57.2%). The average age of participants was also younger (45.5 years). The low antibiotic use could also be a consequence of the Singaporean study focusing on patients in regular inpatient settings, with only 1.9% of patients admitted to the ICU. Additionally, the study examined white blood cell count, C-reactive protein, and procalcitonin levels, which were not assessed in this study. The evaluation of antibiotic usage was also performed by infectious disease specialists in 42% of cases, contributing to the reduced antibiotic usage outside indications.14 Inappropriate antibiotic use during the COVID-19 pandemic can lead to increased multidrug resistance and is associated with longer hospital stays and higher costs for patients and hospital management.15
The irrational use of definitive antibiotics in this study may be attributed to the absence of blood and sputum culture examinations for all COVID-19 patients admitted to the ICU. Microorganism cultures serve to identify the causative agents of infections in patients, and the omission of these tests results in a less precise assessment of definitive antibiotic appropriateness. Furthermore, differences in the experiences of ICU doctors can also influence the variation in antibiotics administered to patients.
Another study found that the use of antibiotics in COVID-19 patients was common and contributed to more than three-quarters of patients. This percentage aligns with findings in other cohorts and meta-analyses. Only 10% of patients were given antibiotics after confirming the presence of lung infection, while 2% experienced other infections due to catheter-related bacteremia and urinary tract infections.16
The rationality of antibiotics was classified based on Gyssens criteria, with 29 patients (23.02%) received empiric antibiotics that were rational according to the COVID-19 treatment guidelines in Indonesia and the IDSA pneumonia therapy guidelines. The category of irrational empiric antibiotics includes 50 patients (39.68%) in category IVA, indicating the presence of a more effective regimen, 26 patients (20.63%) in category I indicating inappropriate timing, 6 patients (4.76%) in category IIIA indicating longer duration, 14 patients (11.11%) in category IIIB indicating shorter duration, and 1 patient (0.79%) in category IIA indicating inappropriate dosage. Eight patients (6.35%), initially categorized as IIIA, including 2 patients (1.59%) without HAP/VAP and 6 patients (4.76%) with HAP/VAP, were reclassified as rational because these patients were still awaiting culture results to determine the subsequent administration of definitive antibiotics. Among patients receiving definitive antibiotics, 40 patients (45.98%) received rational antibiotics, and 37 (42.52%) received irrational antibiotics. The categories of irrational definitive antibiotics include 29 patients (33.33%) in category V, 12 patients (13.78%) in category IVA, 5 patients (5.46%) in category IIIB, and 1 patient (1.15%) in category I.
The excessive and inappropriate use of antibiotics in COVID-19 patients can lead to increased antibiotic resistance. Prescription of antibiotics inappropriately elevates the risk of toxicity and morbidity, with the benefits of administration not proven to date, even in critically ill COVID-19 patients.15 Inappropriate antibiotic prescriptions result from various factors; management protocols in March and April 2020 recommended doctors to prescribe empirical antibiotics to almost all patients, regardless of the presence of indications.17 However, the Indonesian COVID-19 guidelines recommend the use of ceftriaxone and/or azithromycin for severe/critical cases only.4 The need for establishing specific criteria for antibiotic use in COVID-19 patients has been emphasized, resulting in clinical guidelines for antibiotic prescription in COVID-19 patients. The primary recommendation is to limit drug use, especially upon initial admission when bacterial infections are less common. The guidelines suggest delaying the initial use of antibiotics that might have been started in the emergency department.4,16 An additional measure that could be implemented involves improving education regarding the proper use of antibiotics, both in regular healthcare settings and among individuals with COVID-19.18
5. CONCLUSION
This study identified that 23.02% of empirical antibiotic use and 45.98% definitive antibiotic use among COVID-19 patients were rational in the ICU of RSUP Dr. Hasan Sadikin Bandung from January to June 2021. The administration of empirical antibiotics to ICU patients with COVID-19 should adhere more closely to available management guidelines to prevent excessive antibiotic use and mitigate the escalation of antibiotic resistance.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Department of Anesthesiology and Intensive Therapy, Faculty of Medicine, Padjadjaran University, Hospital Dr. Hasan Sadikin, Bandung, Indonesia
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
IDS, EOL: Concept, reviewer important intellectual content, final approver of the version to be published
RIM: Concept, conduction of the study work, statistical analysis, and manuscript editing
10. REFERENCES
- Hajjar LA, Costa IBS da S, Rizk SI, Biselli B, Gomes BR, Bittar CS, et al. Intensive care management of patients with COVID-19: a practical approach. Ann Intensive Care. 2021;11(1):36. [PubMed] DOI: 1186/s13613-021-00820-w
- Petteys MM, Medaris LA, Williamson JE, Soman RS, Denmeade TA, Anderson WE, et al. Outcomes and antibiotic use in patients with coronavirus disease 2019 (COVID-19) admitted to an intensive care unit. Antimicrob Steward Healthc Epidemiol. 2022;2(1):e12. [PubMed] DOI: 1017/ash.2021.248
- Langford BJ, So M, Raybardhan S, Leung V, Soucy JR, Westwood D, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect. 2021;27(4):520–31. [PubMed] DOI: 1016/j.cmi.2020.12.018
- Perhimpunan Dokter Paru Indonesia (PDPI), Perhimpunan Dokter Spesialis Kardiovaskular Indonesia (PERKI), Perhimpunan Dokter Spesialis Penyakit Dalam Indonesia (PAPDI), Perhimpunan Dokter Anestesiologi dan Terapi Intensif Indonesia (PERDATIN), Ikatan Dokter Anak Indonesia (IDAI). Pedoman Tatalaksana COVID-19. PDPI, PERKI, PAPDI, PERDATIN, IDAI; 2022.
- Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–67. [PubMed] DOI: 1164/rccm.201908-1581ST
- Sutrisno E. Impact of irrational antibiotic therapy to hospital cost of care of pneumonia in patients in Dr. Sardjito Hospital. Acta Interna J Intern Med. 2013;3(2):67–71. [FreeFullText]
- Martin AJ, Shulder S, Dobrzynski D, Quartuccio K, Pillinger KE. Antibiotic use and associated risk factors for antibiotic prescribing in COVID-19 hospitalized patients. J Pharm Pract. 2023;36(2):256–63. [PubMed] DOI: 1177/08971900211030248
- Kamara IF, Kumar AM V, Maruta A, Fofanah BD, Njuguna CK, Shongwe S, et al. Antibiotic use in suspected and confirmed COVID-19 patients admitted to health facilities in Sierra Leone in 2020–2021: Practice does not follow policy. Int J Environ Res Public Health. 2022;19(7):4005. [PubMed] DOI: 3390/ijerph19074005
- Dietl B, Boix-Palop L, Gisbert L, Mateu A, Garreta G, Xercavins M, et al. Risk factors associated with inappropriate empirical antimicrobial treatment in bloodstream infections. A cohort study. Front Pharmacol. 2023;14:1132530. [PubMed] DOI: 3389/fphar.2023.1132530
- Haessler S, Lindenauer PK, Zilberberg MD, Imrey PB, Yu PC, Higgins T, et al. Blood cultures versus respiratory cultures: 2 different views of pneumonia. Clin Infect Dis. 2020;71(7):1604–12. [PubMed] DOI: 1093/cid/ciz1049
- Cut TG, Mavrea A, Cumpanas AA, Novacescu D, Oancea CI, Bratosin F, et al. A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients. Pathogens. 2023;12(4):620. [PubMed] DOI: 3390/pathogens12040620
- Luciana T, Andrajati R, Rianti A, Khan AH. Rational antimicrobial use in an Intensive Care Unit in Jakarta, Indonesia: A hospital-based, cross-sectional study. Trop J Pharm Res. 2015;14(4):707–14. DOI: 4314/tjpr.v14i4.21
- Molla MMA, Yeasmin M, Islam MK, Sharif MM, Amin MR, Nafisa T, et al. Antibiotic prescribing patterns at COVID-19 dedicated wards in Bangladesh: Findings from a single center study. Infect Prev Pract. 2021;3(2):100134. [PubMed] DOI: 1016/j.infpip.2021.100134
- Tan SH, Ng TM, Tay HL, Yap MY, Heng ST, Loo AYX, et al. A point prevalence survey to assess antibiotic prescribing in patients hospitalized with confirmed and suspected coronavirus disease 2019 (COVID-19). J Glob Antimicrob Resist. 2021;24:45–7. [PubMed] DOI: 11016/j.jgar.2020.11.025
- Malik SS, Mundra S. Increasing consumption of antibiotics during the COVID-19 pandemic: Implications for patient health and emerging anti-microbial resistance. Antibiotics. 2022;12(1):45. [PubMed] DOI: 3390/antibiotics12010045
- Garcia-Vidal C, Sanjuan G, Moreno-García E, Puerta-Alcalde P, Garcia-Pouton N, Chumbita M, et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: a retrospective cohort study. Clin Microbiol Infect. 2021;27(1):83–8. [PubMed] DOI: 1016/j.cmi.2020.07.041
- Calderón-Parra J, Muiño-Miguez A, Bendala-Estrada AD, Ramos-Martínez A, Muñez-Rubio E, Fernández Carracedo E, et al. Inappropriate antibiotic use in the COVID-19 era: Factors associated with inappropriate prescribing and secondary complications. Analysis of the registry SEMI-COVID. PLoS One. 2021;16(5):e0251340. [PubMed] DOI: 1371/journal.pone.0251340
- Di Gennaro F, Marotta C, Amicone M, Bavaro DF, Bernaudo F, Frisicale EM, et al. Italian young doctors’ knowledge, attitudes and practices on antibiotic use and resistance: A national cross-sectional survey. J Glob Antimicrob Resist. 2020;23:167–73. [PubMed] DOI: 1016/j.jgar.2020.08.022