Hisham Nasief1, Amber Hassan2*, Nashwa AlDardeir3, Khalid Khadawardi4, Ahmad B. Alwazzan5, Haneen Alothmani6, Ziyad Hammad7
Author affiliations:
Background & objective: Uterine bleeding is a notable complication that can occur after the surgical removal of uterine fibroids, and oxytocin infusion has been a commonly used method to control blood loss in such cases. The objective of this study was to evaluate the effectiveness of oxytocin infusion in managing surgical bleeding following abdominal myomectomy, as an alternative to immediate blood transfusion.
Methodology: The study population consisted of 120 patients who experienced acute blood loss following abdominal myomectomy. These patients were divided into two groups: Group A, which included 50 patients who received an oxytocin infusion, and Group B, which included 60 patients who received a placebo. All myomectomies were conducted according to department protocols, and various variables related to the study were recorded. Postoperative hemoglobin levels were checked in every patient.
Results: In Group A, the average blood loss was 470.02 ± 81.65 ml, while in Group B, it was 721.42 ml ± 63.55 ml (P < 0.0001). The need for urgent blood transfusion was significantly lower in Group A (3.3%) compared to Group B (20.0%), (P = 0.044). Postoperative hemoglobin levels also showed a significant difference between the two groups, with Group A demonstrating better results than Group B.
Conclusion: Oxytocin infusion can be safely used for managing blood loss in patients undergoing abdominal myomectomy. However, in cases where oxytocin is unable to effectively control the bleeding, blood transfusion may be needed as a means to compensate for the blood loss.
Key Words: Uterine leiomyomas; Myomectomy; Surgical blood loss; Oxytocin
Citation: Nasief H, Hassan A, AlDardeir N, Khadawardi K, Alwazzan AB, Alothmani H, Hammad Z. Oxytocin infusion is a safe uterine bleeding controller alternative to blood transfusion in patients undergoing abdominal myomectomy. Anaesth. pain intensive care 2024;28(1):05−09; DOI: 10.35975/apic.v28i1.2298
Received: October 05, 2023; Reviewed: October 17, 2023; Accepted: November 19, 2023
Uterine leiomyoma, also known as fibroids, is the most common benign tumor found in women of childbearing age, accounting for approximately 25% of all gynecological tumors.1 The presence of fibroids can lead to various complications during both pre-surgical and intraoperative stages, depending on factors such as tumor size, location, and number. Surgical intervention, such as abdominal myomectomy or hysterectomy, is often necessary for patients with multiple or large fibroids, with chronic recurrent uterine bleeding being a primary indication for these procedures. Traditionally, abdominal myomectomy has been performed with a suprapubic incision, but hysterectomy is generally associated with less bleeding, making the choice of surgical approach challenging and dependent on the patient's clinical presentation.2
Uterine bleeding is the most common intraoperative complication following myomectomy, emphasizing the importance of proper hemostasis and layered closure of the uterus to minimize morbidity and mortality rates.3 Standard mechanical methods, such as dissection through the avascular plane, are routinely employed during myomectomy to control blood loss. However, pharmacological approaches using medications like misoprostol, tranexamic acid, ascorbic acid, or dinoprostone have also been utilized to prevent surgical bleeding.4 Additionally, the use of uterine artery tourniquets has shown promising results in significantly reducing blood loss.4 The investigation of specialized surgical techniques versus pharmacological treatments is limited in the existing literature, with one such medical treatment option being oxytocin infusion.5
Synthetic oxytocin is commonly used in medical settings to induce or enhance labor that is not progressing as expected. It helps to strengthen and regulate contractions, making labor more efficient. It can also be used to prevent or treat postpartum hemorrhage by promoting uterine contractions after childbirth. In addition to these uses, synthetic oxytocin may have other medical applications, such as managing incomplete or missed miscarriages or controlling bleeding during certain gynecological procedures.6,7
It is important for healthcare professionals to closely monitor the use of synthetic oxytocin, as it can have unusual side effects like uterine hyperstimulation, fetal distress, and changes in maternal blood pressure. The dosage and administration of synthetic oxytocin should be tailored to each individual patient's needs and supervised by medical experts.
Oxytocin infusion has been found to reduce the need for blood transfusion during gynecological surgeries like abdominal myomectomy or hysterectomy. However, its use during myomectomy is not yet frequent. It stimulates myometrial contractions by acting on G-protein linked receptors, which leads to an increase in intracellular calcium in uterine myofibrils. This repetitive stimulation helps to reduce blood leakage during surgery.8
We investigated the beneficial role of oxytocin infusion in reducing surgical blood loss compared to using blood transfusion during abdominal myomectomy.
2.1. Selection of patients
This study was approved by the institutional review board (IRB), of the Faculty of Medicine, King Abdulaziz University Jeddah, after written informed consent taken from 120 patients (60 in each group) enrolled in this study. Patients were enrolled on the study according to the inclusion criteria. The participants were distributed randomly into two study groups using a computerized random number table generator that provided a trial sequence which was concealed in sealed opaque envelopes with unique numbers.
2.2. Trial methodology
Detailed gynecological history of each patient was obtained. Our study included patients who underwent abdominal myomectomy and met the following criteria: age 18-45 y, confirmed uterine fibroids with a uterus size of less than 18 weeks as determined by ultrasound, and had a single fibroid sized from 5-10 cm. Pre-operative laboratory investigations including complete blood count, liver function tests, renal function tests, viral markers and clotting profiles were done. The patients were divided into two experimental groups: Group A: the main study group that received oxytocin infusion, and Group B: that was given a placebo.
Before the procedure, pre-operative hemoglobin and hematocrit levels were assessed. In Group A, patients received oxytocin 30 IU in 500 ml normal saline at a rate of 85 drops/min after the induction of general anesthesia and before the surgery. Group B patients received normal saline at the same volume and rate. All myomectomies were performed by consultant gynecologists. The blood loss during the myomectomy was estimated by a trained colleague. This estimation was calculated by adding the volume of contents from the suction container (a), to the difference in weight (1g was considered equal to 1 ml) between the dry (b), and wet (c) sponges used during the surgery. The formula used for this calculation was m=a+(c-b). The weight of the sponges was measured using an electronic weighing machine. The patient's vital signs were continuously monitored during the post-operative period. Standard post-operative care was provided to all patients. Postoperative hemoglobin and hematocrit levels were re-evaluated 24 h after the surgery. All patients were closely observed for any side effects such as allergic reactions, hypotension, nausea, and vomiting, and appropriate management was carried out following ward protocols.
2.3. Statistical analysis
Quantitative variables such as age, parity, pre-operative and post-operative hemoglobin (g/dl) and hematocrit were recorded as mean and standard deviation (SD). All the qualitative variables were presented by using frequency and percentage. An Independent sample t-test was used to compare mean blood loss in both groups and a Chi-square test was applied to compare the need for blood transfusion in both groups. Data was stratified for age, obesity and parity. Post stratified Chi-square test was applied for the need of blood transfusion and independent sample t-test was applied for intra-operative blood loss taking P ≤ 0.05 as significant. All collected data were analyzed using SPSS 22.
A total of 120 patients were included in the current study, with 60 patients in Group A and 60 patients in Group B. The mean age of patients in Group A was 35.17 ± 5.41 y, while in Group B it was 34.27 ± 6.22 y. Among the patients, 85% were between the ages of 18-40 y, and 15% were between the ages of 41-45 y (Figure 1). In terms of parity, the majority of patients had 1-2 children, with 32 (53.3%) patients in Group A and 36 (60.0%) patients in Group B (Table 1). The mean blood loss in Group A was 470.02 ± 81.654 ml, while in Group B it was 721.42 ± 63.547 ml, showing a significant difference (P < 0.0001) (Table 2). There was also a significant difference in the requirement for blood transfusion between Group A and Group B (P = 0.044). However, the need for blood transfusion was significantly lower in Group A compared to Group B (3.3% versus 20.0%) (Table 2). There was no significant difference in mean blood loss according to parity and fibroid size (P > 0.05) (Table 3).
Uterine leiomyoma or fibroid is the most common gynecological type of benign tumor in women of reproductive age, affecting up to 20% of women over 35 y old. Tumor growth is always asymptomatic; however, it can occasionally cause significant complications in some women such as heavy menstrual bleeding, pelvic pain, anemia, and hypotension in about 20-50% of the patients.10 Myomectomy is the surgery of choice and is considered an essential treatment approach for most of the asymptomatic large fibroids or all types of symptomatic fibroids, particularly for women who want to preserve their fertility.1,5 Although myomectomy can be performed through different surgical approach such as laparotomy, laparoscopy or hysteroscopy,11 the most significant associated complication is uterine bleeding, with increased risk of morbidity and mortality.
Gynecologists undergo a considerable challenge in preventing excessive bleeding during the procedure, despite using various preservative measure to reduce the blood loss. However, 20% of women require blood transfusion during or after the procedure. Nevertheless, researchers have conducted multiple therapeutic trials to reduce the incidence of bleeding during myomectomy using various pharmacological agents such as misoprostol (a synthetic prostaglandin E1 analogue), bupivacaine plus epinephrine, vasopressin injection, and pre-operative administration of gonadotropin-releasing hormone (GnRH) agonist. Unfortunately, most of these agents are expensive and show ineffective results.12
Recently, synthetic oxytocin has emerged as a possible solution to reduce surgical bleeding during myomectomy. Oxytocin is commonly used as a uterotonic agent to control uterine bleeding during postpartum period. It causes repetitive uterine contractions and spasm of uterine vessels through the uterine musculature contractility. This leads to a reduced blood flow to leiomyoma, resulting in less blood loss during myomectomy.13 We investigated the efficacy of oxytocin infusion in patients undergoing abdominal myomectomy. We found that the blood loss was significantly less in Group A compared to Group B (425.30 ± 36.849 ml vs. 843.90 ± 21.903 ml). Some previously published studies have also shown similar results. Niaz et al. (2022)15 reported the blood loss to be 290.463 ± 120.91 ml vs. 424.98 ± 106.21 ml (P < 0.005); and Ahmed et al. (2020)16 reported it to be 406.33 ± 171.67 ml vs. 875.33 ± 284 ml (P < 0.0001). The blood transfusion was required in Group A less than in Group B (3.3% vs. 20.0%). This finding was also supported by results reported by Niaz et al.15 Moreover, the postoperative Hb and hematocrit between the two study groups were significantly different.
Although the current data was stratified for the age and gender, there was no significant difference between the two groups. similarly, the intraoperative blood loss was not associated with age, obesity, parity and fibroid size between the groups.
The strengths of this study were a fairly good sample size and strict inclusion and exclusion criteria. All the patients were treated by the same gynecologist, and all the findings were given by a consultant surgeon and were recorded by the researcher herself. So, the factor of bias in results is at its minimum possible level. However, time constraint and the restriction of a single center was the limitation of this study that needs to be addressed by larger and multicenter studies with a broader spectrum.
The results of our study conclude that oxytocin infusion can be used as a safe alternative to control bleeding in patients undergoing abdominal myomectomy. Its use is associated with less requirement of transfusion, and it helps preserve hemoglobin and hematocrit in these patients. However, blood transfusion can compensate blood loss when oxytocin fails to control the bleeding.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Faculty of Medicine
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
All authors took part in the conduct of this study, literature search, data collection and analysis, and manuscript preparation.
Author affiliations:
- Hisham Nasief, Department of Obstetrics and Gynecology, Faculty of Medicine, King Abdulaziz University Jeddah, Saudi Arabia; E-mail: hnassif@kau.edu.sa
- Amber Hassan, System medicine (Molecular Oncology), European School of Molecular Medicine, Università Degli Studi Di Milano, Milan / Translational Neuroscience Lab, CEINGE Biotecnologie Avanzate S.c.a.rl.Via Gaetano Salvatore, 486, 80145 - Naples, Italy; E-mail; amberhassan7@gmail.com
- Nashwa AlDardeir, Department of Obstetrics and Gynecology, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; E-mail: aahaldardir2@kau.edu.sa
- Khalid Khadawardi, Department of Obstetrics and Gynecology, Faculty of Medicine, Umm-Alqura University, Mecca, Saudi Arabia; E-mail: khadawardi@hotmail.com
- Ahmad B. Alwazzan, Department of Obstetrics and Gynecology, Faculty of Medicine, King Abdulaziz University Jeddah, Saudi Arabia; E-mail: ab_wazzan@yahoo.com
- Haneen Alothmani, Department of Obstetrics and Gynecology, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; E-mail: haneen.alothmani@gmail.com
- Ziyad Hammad, Department of Obstetrics and Gynecology, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; E-mail: zmhammad96@gmail.com
ABSTRACT
Background & objective: Uterine bleeding is a notable complication that can occur after the surgical removal of uterine fibroids, and oxytocin infusion has been a commonly used method to control blood loss in such cases. The objective of this study was to evaluate the effectiveness of oxytocin infusion in managing surgical bleeding following abdominal myomectomy, as an alternative to immediate blood transfusion.
Methodology: The study population consisted of 120 patients who experienced acute blood loss following abdominal myomectomy. These patients were divided into two groups: Group A, which included 50 patients who received an oxytocin infusion, and Group B, which included 60 patients who received a placebo. All myomectomies were conducted according to department protocols, and various variables related to the study were recorded. Postoperative hemoglobin levels were checked in every patient.
Results: In Group A, the average blood loss was 470.02 ± 81.65 ml, while in Group B, it was 721.42 ml ± 63.55 ml (P < 0.0001). The need for urgent blood transfusion was significantly lower in Group A (3.3%) compared to Group B (20.0%), (P = 0.044). Postoperative hemoglobin levels also showed a significant difference between the two groups, with Group A demonstrating better results than Group B.
Conclusion: Oxytocin infusion can be safely used for managing blood loss in patients undergoing abdominal myomectomy. However, in cases where oxytocin is unable to effectively control the bleeding, blood transfusion may be needed as a means to compensate for the blood loss.
Key Words: Uterine leiomyomas; Myomectomy; Surgical blood loss; Oxytocin
Citation: Nasief H, Hassan A, AlDardeir N, Khadawardi K, Alwazzan AB, Alothmani H, Hammad Z. Oxytocin infusion is a safe uterine bleeding controller alternative to blood transfusion in patients undergoing abdominal myomectomy. Anaesth. pain intensive care 2024;28(1):05−09; DOI: 10.35975/apic.v28i1.2298
Received: October 05, 2023; Reviewed: October 17, 2023; Accepted: November 19, 2023
1. INTRODUCTION
Uterine leiomyoma, also known as fibroids, is the most common benign tumor found in women of childbearing age, accounting for approximately 25% of all gynecological tumors.1 The presence of fibroids can lead to various complications during both pre-surgical and intraoperative stages, depending on factors such as tumor size, location, and number. Surgical intervention, such as abdominal myomectomy or hysterectomy, is often necessary for patients with multiple or large fibroids, with chronic recurrent uterine bleeding being a primary indication for these procedures. Traditionally, abdominal myomectomy has been performed with a suprapubic incision, but hysterectomy is generally associated with less bleeding, making the choice of surgical approach challenging and dependent on the patient's clinical presentation.2
Uterine bleeding is the most common intraoperative complication following myomectomy, emphasizing the importance of proper hemostasis and layered closure of the uterus to minimize morbidity and mortality rates.3 Standard mechanical methods, such as dissection through the avascular plane, are routinely employed during myomectomy to control blood loss. However, pharmacological approaches using medications like misoprostol, tranexamic acid, ascorbic acid, or dinoprostone have also been utilized to prevent surgical bleeding.4 Additionally, the use of uterine artery tourniquets has shown promising results in significantly reducing blood loss.4 The investigation of specialized surgical techniques versus pharmacological treatments is limited in the existing literature, with one such medical treatment option being oxytocin infusion.5
Synthetic oxytocin is commonly used in medical settings to induce or enhance labor that is not progressing as expected. It helps to strengthen and regulate contractions, making labor more efficient. It can also be used to prevent or treat postpartum hemorrhage by promoting uterine contractions after childbirth. In addition to these uses, synthetic oxytocin may have other medical applications, such as managing incomplete or missed miscarriages or controlling bleeding during certain gynecological procedures.6,7
It is important for healthcare professionals to closely monitor the use of synthetic oxytocin, as it can have unusual side effects like uterine hyperstimulation, fetal distress, and changes in maternal blood pressure. The dosage and administration of synthetic oxytocin should be tailored to each individual patient's needs and supervised by medical experts.
Oxytocin infusion has been found to reduce the need for blood transfusion during gynecological surgeries like abdominal myomectomy or hysterectomy. However, its use during myomectomy is not yet frequent. It stimulates myometrial contractions by acting on G-protein linked receptors, which leads to an increase in intracellular calcium in uterine myofibrils. This repetitive stimulation helps to reduce blood leakage during surgery.8
We investigated the beneficial role of oxytocin infusion in reducing surgical blood loss compared to using blood transfusion during abdominal myomectomy.
2. METHODOLOGY
2.1. Selection of patients
This study was approved by the institutional review board (IRB), of the Faculty of Medicine, King Abdulaziz University Jeddah, after written informed consent taken from 120 patients (60 in each group) enrolled in this study. Patients were enrolled on the study according to the inclusion criteria. The participants were distributed randomly into two study groups using a computerized random number table generator that provided a trial sequence which was concealed in sealed opaque envelopes with unique numbers.
2.2. Trial methodology
Detailed gynecological history of each patient was obtained. Our study included patients who underwent abdominal myomectomy and met the following criteria: age 18-45 y, confirmed uterine fibroids with a uterus size of less than 18 weeks as determined by ultrasound, and had a single fibroid sized from 5-10 cm. Pre-operative laboratory investigations including complete blood count, liver function tests, renal function tests, viral markers and clotting profiles were done. The patients were divided into two experimental groups: Group A: the main study group that received oxytocin infusion, and Group B: that was given a placebo.
Before the procedure, pre-operative hemoglobin and hematocrit levels were assessed. In Group A, patients received oxytocin 30 IU in 500 ml normal saline at a rate of 85 drops/min after the induction of general anesthesia and before the surgery. Group B patients received normal saline at the same volume and rate. All myomectomies were performed by consultant gynecologists. The blood loss during the myomectomy was estimated by a trained colleague. This estimation was calculated by adding the volume of contents from the suction container (a), to the difference in weight (1g was considered equal to 1 ml) between the dry (b), and wet (c) sponges used during the surgery. The formula used for this calculation was m=a+(c-b). The weight of the sponges was measured using an electronic weighing machine. The patient's vital signs were continuously monitored during the post-operative period. Standard post-operative care was provided to all patients. Postoperative hemoglobin and hematocrit levels were re-evaluated 24 h after the surgery. All patients were closely observed for any side effects such as allergic reactions, hypotension, nausea, and vomiting, and appropriate management was carried out following ward protocols.
2.3. Statistical analysis
Quantitative variables such as age, parity, pre-operative and post-operative hemoglobin (g/dl) and hematocrit were recorded as mean and standard deviation (SD). All the qualitative variables were presented by using frequency and percentage. An Independent sample t-test was used to compare mean blood loss in both groups and a Chi-square test was applied to compare the need for blood transfusion in both groups. Data was stratified for age, obesity and parity. Post stratified Chi-square test was applied for the need of blood transfusion and independent sample t-test was applied for intra-operative blood loss taking P ≤ 0.05 as significant. All collected data were analyzed using SPSS 22.
3. RESULTS
A total of 120 patients were included in the current study, with 60 patients in Group A and 60 patients in Group B. The mean age of patients in Group A was 35.17 ± 5.41 y, while in Group B it was 34.27 ± 6.22 y. Among the patients, 85% were between the ages of 18-40 y, and 15% were between the ages of 41-45 y (Figure 1). In terms of parity, the majority of patients had 1-2 children, with 32 (53.3%) patients in Group A and 36 (60.0%) patients in Group B (Table 1). The mean blood loss in Group A was 470.02 ± 81.654 ml, while in Group B it was 721.42 ± 63.547 ml, showing a significant difference (P < 0.0001) (Table 2). There was also a significant difference in the requirement for blood transfusion between Group A and Group B (P = 0.044). However, the need for blood transfusion was significantly lower in Group A compared to Group B (3.3% versus 20.0%) (Table 2). There was no significant difference in mean blood loss according to parity and fibroid size (P > 0.05) (Table 3).
| Table 1: Baseline information of patients | |||
| Parameter | Group A | Group B | P-value |
| Age (y) | 35.17 ± 5.41 | 34.27 ± 6.22 | 0.399 |
| BMI (kg/m2) | 25.59 ± 3.62 | 25.95 ± 3.20 | 0.56 |
| Parity | |||
| 1-2 | 32 (53.3) | 36 (60.0) | 0.46 |
| 3-4 | 28 (46.7) | 24 (40.0) | |
| Data presented as mean ± SD or n (%) | |||
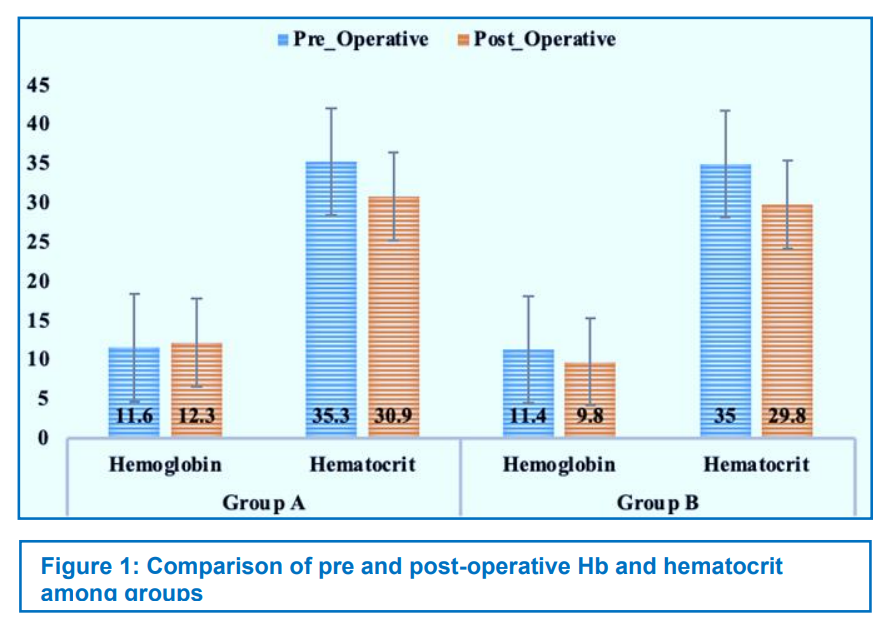
| Table 2: Comparison of blood loss, Post-operative Hb and hematocrit among groups | |||
| Variable | Group A | Group B | P-value |
| Blood Loss (ml) | 470.02 ± 81.654 | 721.42 ± 63.547 | 0.0001 |
| Post-operative hemoglobin (g/dl) | 10.417 ± 1.2253 | 9.832 ± 0.6032 | 0.001 |
| Post-operative hematocrit (%) | 30.922 ± 1.6376 | 29.887 ± 1.5619 | 0.001 |
| Need for Blood Transfusion | 2 (3.3) | 12 (20.0) | 0.004 |
| Data presented as mean ± SD or n (%) | |||
| Table 3: Comparison of blood loss, according to parity and fibroid size | ||
| Parity | Blood loss (ml)
Mean ± SD |
p-value |
| 1-2 | 583.82 ± 14.4 | 0.641 |
| 3-4 | 596.87 ± 15.0 | |
| Fibroid Size | ||
| < 7 | 560.3 ± 13.5 | 0.38 |
| > 7 | 580.9 ± 15.4 | |
4. DISCUSSION
Uterine leiomyoma or fibroid is the most common gynecological type of benign tumor in women of reproductive age, affecting up to 20% of women over 35 y old. Tumor growth is always asymptomatic; however, it can occasionally cause significant complications in some women such as heavy menstrual bleeding, pelvic pain, anemia, and hypotension in about 20-50% of the patients.10 Myomectomy is the surgery of choice and is considered an essential treatment approach for most of the asymptomatic large fibroids or all types of symptomatic fibroids, particularly for women who want to preserve their fertility.1,5 Although myomectomy can be performed through different surgical approach such as laparotomy, laparoscopy or hysteroscopy,11 the most significant associated complication is uterine bleeding, with increased risk of morbidity and mortality.
Gynecologists undergo a considerable challenge in preventing excessive bleeding during the procedure, despite using various preservative measure to reduce the blood loss. However, 20% of women require blood transfusion during or after the procedure. Nevertheless, researchers have conducted multiple therapeutic trials to reduce the incidence of bleeding during myomectomy using various pharmacological agents such as misoprostol (a synthetic prostaglandin E1 analogue), bupivacaine plus epinephrine, vasopressin injection, and pre-operative administration of gonadotropin-releasing hormone (GnRH) agonist. Unfortunately, most of these agents are expensive and show ineffective results.12
Recently, synthetic oxytocin has emerged as a possible solution to reduce surgical bleeding during myomectomy. Oxytocin is commonly used as a uterotonic agent to control uterine bleeding during postpartum period. It causes repetitive uterine contractions and spasm of uterine vessels through the uterine musculature contractility. This leads to a reduced blood flow to leiomyoma, resulting in less blood loss during myomectomy.13 We investigated the efficacy of oxytocin infusion in patients undergoing abdominal myomectomy. We found that the blood loss was significantly less in Group A compared to Group B (425.30 ± 36.849 ml vs. 843.90 ± 21.903 ml). Some previously published studies have also shown similar results. Niaz et al. (2022)15 reported the blood loss to be 290.463 ± 120.91 ml vs. 424.98 ± 106.21 ml (P < 0.005); and Ahmed et al. (2020)16 reported it to be 406.33 ± 171.67 ml vs. 875.33 ± 284 ml (P < 0.0001). The blood transfusion was required in Group A less than in Group B (3.3% vs. 20.0%). This finding was also supported by results reported by Niaz et al.15 Moreover, the postoperative Hb and hematocrit between the two study groups were significantly different.
Although the current data was stratified for the age and gender, there was no significant difference between the two groups. similarly, the intraoperative blood loss was not associated with age, obesity, parity and fibroid size between the groups.
The strengths of this study were a fairly good sample size and strict inclusion and exclusion criteria. All the patients were treated by the same gynecologist, and all the findings were given by a consultant surgeon and were recorded by the researcher herself. So, the factor of bias in results is at its minimum possible level. However, time constraint and the restriction of a single center was the limitation of this study that needs to be addressed by larger and multicenter studies with a broader spectrum.
5. CONCLUSION
The results of our study conclude that oxytocin infusion can be used as a safe alternative to control bleeding in patients undergoing abdominal myomectomy. Its use is associated with less requirement of transfusion, and it helps preserve hemoglobin and hematocrit in these patients. However, blood transfusion can compensate blood loss when oxytocin fails to control the bleeding.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Acknowledgement
We gratefully thank Faculty of Medicine
8. Conflict of interest
The study utilized the hospital resources only, and no external or industry funding was involved.
9. Authors’ contribution
All authors took part in the conduct of this study, literature search, data collection and analysis, and manuscript preparation.
10. REFERENCES
- Akinyemi BO, Adewoye BR, Fakoya TA. Uterine fibroid: a review. Niger J Med. 2004 Oct-Dec;13(4):318-29. [PubMed]
- Orlando MS, Kho RM. Laparoscopic Myomectomy. In: Atlas of Robotic, Conventional, and Single-Port Laparoscopy: A Practical Approach in Gynecology. Springer; 2022. p. 27-41.
- Lee SR, Kim JH, Kim S, Kim SH, Chae HD. The number of myomas is the most important risk factor for blood loss and total operation time in robotic myomectomy: analysis of 242 cases. J Clin Med. 2021 Jun 30;10(13):2930. [PubMed] DOI: 3390/jcm10132930
- de Barros Lopes A, Spirtos NM, Hilton P, Monaghan JM, editors. Uterine fibroids. In: Bonney’s Gynaecological Surgery. 12th ed. John Wiley & Sons Ltd; 2018. p. 127.
- Taylor A, Sharma M, Tsirkas P, Di Spiezio Sardo A, Setchell M, Magos A. Reducing blood loss at open myomectomy using triple tourniquets: a randomised controlled trial. BJOG. 2005 Mar;112(3):340-5. [PubMed] DOI: 1111/j.1471-0528.2004.00430.x
- Albazee E, Sayad R, Elrashedy AA, Samy Z, Faraag E, Baradwan S, et al. Efficacy of oxytocics on reducing intraoperative blood loss during abdominal myomectomy: A systematic review and meta-analysis of randomized placebo-controlled trials. J Gynecol Obstet Hum Reprod. 2022 May;51(5):102358. [PubMed] DOI: 1016/j.jogoh.2022.102358
- Aslan Çetin B, Aydoğan Mathyk B, Köroğlu N, Soydar A, Demirayak G, Çift T. Oxytocin infusion reduces bleeding during abdominal myomectomies: a randomized controlled trial. Arch Gynecol Obstet. 2019 Jan;299(1):151-157. [PubMed] DOI: 1007/s00404-018-4944-9
- Atashkhoei S, Fakhari S, Pourfathi H, Bilehjani E, Garabaghi PM, Asiaei A. Effect of oxytocin infusion on reducing the blood loss during abdominal myomectomy: a double-blind randomised controlled trial. BJOG. 2017 Jan;124(2):292-298. [PubMed] DOI: 1111/1471-0528.14416
- Bahadur A, Khoiwal K, Bhattacharya N, Chaturvedi J, Kumari R. The effect of intrauterine misoprostol on blood loss during caesarean section. J Obstet Gynaecol. 2019 Aug;39(6):753-756. [PubMed] DOI: 1080/01443615.2019.1581743
- Ahmad A, Kumar M, Bhoi NR, Badruddeen, Akhtar J, Khan MI, et al. Diagnosis and management of uterine fibroids: current trends and future strategies. J Basic Clin Physiol Pharmacol. 2023 Mar 30;34(3):291-310. [PubMed] DOI: 1515/jbcpp-2022-0219
- Tinelli A, Favilli A, Lasmar RB, Mazzon I, Gerli S, Xue X, et al. The importance of pseudocapsule preservation during hysteroscopic myomectomy. Eur J Obstet Gynecol Reprod Biol. 2019 Dec;243:179-184. [PubMed] DOI: 1016/j.ejogrb.2019.09.008
- Tinelli A, Vinciguerra M, Sparić R, Hatırnaz Ş, Güler O, Kosmas I, et al. Fibroids in Obstetrics and Gynecology: Training and Skill in Myomectomy. Practical Guide to Simulation in Delivery Room Emergencies: Springer; 2023. p. 981-1025.
- Vinciguerra M, Sparic R, Hartinaz S, Trojano G, Tinelli A. Cesarean myomectomy technique: a critical review J Interdisciplinary Res Appl Med. 2020;4(1):25-36. [FreeFullText]
- Ahmed M, Baqai S, Khushdil A, Ahmed F. Effect of oxytocin infusion on reducing blood loss during abdominal myomectomy: A randomized controlled trial. J Pak Med Assoc. 2020 Jun;70(6):969-972. [PubMed] DOI: 5455/JPMA.14026
- Niaz S, Abid S, Ashraf A, Mumtaz N, editors. Efficacy of Oxytocin in Reducing Blood Loss During Abdominal Myomectomy. Proceedings; 2022.
- Ahmed M, Baqai S, Khushdil A, Ahmed F. Effect of oxytocin infusion on reducing blood loss during abdominal myomectomy: A randomized controlled trial. J Pak Med Assoc. 2020 Jun;70(6):969-972. [PubMed] DOI: 10.5455/JPMA.14026