Sanwal Javaid 1 , Marrium Shafi 2 , Yaseen Lodhi 3
Author affiliations:
Abstract
Objective: Most of the ophthalmic surgery is done under topical anesthesia or nerve blocks. Local anesthetic agents are usually used for both analgesic techniques. We hypothesized that nonsteroidal anti–inflammatory drugs (NSAIDs) could be used preoperatively for postoperative pain, either topically or by oral route. Present study aimed to compare mean reduction in pain scores with oral versus topical NSAIDs following photorefractive keratectomy.
Methodology: This prospective study was conducted at Department of Ophthalmology, Eye Donors Organization (EDO) Hospital, Wah Cantt, for 6 months (March 2019–August 2019). A sample size of 40 patients was calculated using World Health Organization calculator. We selected patients through convenient (non–probability) sampling. We took IRB approval, and written consent form the patients. All patients underwent photorefractive keratectomy. Patients were randomly divided (lottery method) into two groups; Group A was treated with topical NSAIDs while group B was treated with oral NSAIDs. Patients were followed for 3 days. We measured pain scores using visual analogue pain scale (VAS). Data analysis was done using SPSS version 24. T–test and fissure exact test were applied. A p ≤ 0.05 was considered significant.
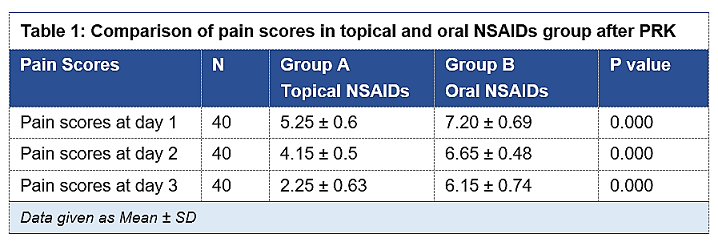
Results: A total of 40 patients were included in study. Mean age of patients was 28.1 ± 2.9 y. There were 21(52.5%) males and 19(46.3%) females. Topical NSAIDs showed significant reduction in pain scores as compared to oral NSAIDs at day 1 (5.25 ± 0.6 vs. 7.20 ± 0.69, p = 0.000), day 2 (4.15 ± 0.5 vs. 6.65 ± 0.48, p = 0.000) day 3 (2.25 ± 0.63 vs. 6.15 ± 0.74, p = 0.000).
Conclusion: Topical nonsteroidal anti–inflammatory drugs are safe and effective for reducing postoperative pain management following photorefractive keratectomy as compared to oral nonsteroidal anti– inflammatory drugs.
Key words: Nonsteroidal anti–inflammatory drugs; Pain; Photorefractive keratectomy
Citation: Javaid S, Shafi M, Lodhi Y. Comparison of postoperative pain in photorefractive keratectomy using topical versus oral nonsteroidal anti–inflammatory drugs. Anaesth. pain intensive care 2021;25(3):324–328. DOI: 10.35975/apic.v25i3.1527
Received: January 29, 2021, Reviewed: February 27, March 13, 2021, Accepted: March 31, 2021
Introduction
Refractive error is the most common cause of the visual impairment (correctable) worldwide.1
According to World Health Organization (WHO), an estimated 285 million individuals were visually impaired with 39 million leading towards blindness globally.2 Literature reported that 90% of visually impaired individuals are resident of developing countries including Pakistan.3 Refractive error can be treated with glasses, contact lenses and surgically.4
Photorefractive keratectomy (PRK) was introduced as first safe and effective surgical treatment of refractive error as surface ablation procedure since 1980s. This procedure includes irradiation of corneal stroma with an ultraviolet beam of 193 nm generated from argon fluoride excimer laser. After epithelium removal, photoablation is used to reshape anterior corneal stroma, and thus correct ametropia. Literature reported that PRK is effective in low to moderate refractive errors (myopia, hypermetropia and astigmatism).5
PRK is indicated in myopia of less than 12 diopter, hypermetropia less than 5 diopters and astigmatism less than 6 diopters. PRK is contraindicated many other eye conditions, in pregnant women and nursing mothers.6
Pain is a common complication of PRK. This sensation is a result of corneal nerve baring after epithelial debridement. However, the condition remains consistent until complete repair of epithelial occur.7 Literature reports several techniques for the pain relieve after PRK, including bandage contact lens, topical morphine, dilute tetracaine eye drops, transepithelial all surface laser ablation, corticosteroids, cycloplegics and nonsteroidal anti–inflammatory drugs (NSAIDs). NSAIDs are the most common drugs used for pain management (e.g. ketorolac tromethamine 0.5% or diclofenac 0.1% for 24–48 h).8
Limited data is available on measuring efficacy of NASIDs in pain management after PRK in Pakistan. Present study aims to compare mean reduction in pain scores of oral vs. topical nonsteroidal anti–inflammatory drugs following photorefractive keratectomy.
Methodology
A prospective study was conducted at Department of Ophthalmology, Eye Donors Organization (EDO) Hospital, Wah Cantt, for 6 months (March 2019–August 2019). A sample size of 40 patients (20 patients in each group) was calculated with µ1 = 5.17, µ2 = 3.21, S.D = 2.25, power of study = 80%, 5% significance level using WHO calculator.9 Patients were selected through non–probability convenient sampling. Institutional review board permission was taken before conduction of study. Written was obtained from all patients before the conduction of study. Patients with age 18–40 years, both genders, low to moderate refractive error (myopia ≤7 D, hypermetropia≤5 D, Astigmatism≤4D) were included in study. Exclusion criteria was based upon keratoconus, significant ocular surface disease, history of allergy, severe side effects to NSAIDs significant asymmetry on corneal mapping, history of ocular herpetic disease, form frusta keratoconus, concurrent therapy with topical/systemic NSAIDs, any ocular pathology except refractive error, history of prior to refractive surgery, predicted residual stromal bed less than 320 microns, any other ocular pathology except refractive error, history of diabetes mellitus and immunological diseases.
Operative Technique
Initially, patients were anaesthetized with the help of 0.5% proparacaine hydrochloride (two drops) and 0.5% tetracaine hydrochloride (preservative free) initially 10 min and then 5 min prior to surgical procedure with povidone iodine solution (5%). The procedure started with central 8.5 mm scoring of corneal epithelium with marker, exposing to balanced salt solution (BSS) with 20% ethanol and placing in 8 mm well (35–40 sec). It was removed from well with the help of surgical sponge and rinsing with 3 ml of BSS. We removed epithelial after residual BSS was dried with sponges. Laser ablation was performed with excimer laser following surgeon’s optimized nomogram. The ocular surface was chilled for 10 sec with BSS after ablation. After 10 sec of chilling, the surface was rinsed with 0.4% ketorolac tromethamine, 1% prednisolone acetate, 0.5% gatifloxacin followed by bandage contact lens placement.
Intervention technique
Patients were randomly (lottery method) divided into two groups; Group A was given topical NSAIDs (ketorolac 0.4%) in both eyes (every 12 h) while group B was given oral naproxen sodium (220 mg) (every 12 h) for 72 h immediately after PRK. Other drugs given to both groups were prednisolone 1% and gatifloxacin 0.5% for one week (4 times a day). However, the bandage contact lens was removed after one week. We recommended oral hydrocodone acetaminophen (5– 325 mg) after every 4 h for breakthrough pain. We used visual analogue scale for pain measurement at 3 consecutive days after surgery
 .
.
 .
.
 .
.
Data analysis
We used SPSS version 24 for data entry and analysis of variables. Descriptive statistics are presented in terms of mean and standard deviation while categorical and nominal data are presented as frequencies and percentages. We controlled general effect modifiers (gender, age) by stratification in SPSS. Post stratification T test and fissure exact test were applied. A p ≤ 0.05 was considered as statistically significant.
Results
A total of 40 patients were included in the study. Mean age of patients was 28.1 ± 2.9 y. There were 21 (52.5%) male and 19 (46.3%) female patients. Among all, 26 (65%) were in age group 18–30 y and 14 (35%) were in age group 31–40 y. Refractive errors were myopia 30 (75%), hypermetropia 7 (17.5%) and astigmatism 3 (7.5%). Duration of refractive error was ≤ 2 y in 11 (27.5%), while > 2 y in 29 (72.5%) patients.
Mean pain scores at day 1 in Group A were 5.25 ± 0.6 and group B 7.20 ± 0.69 (p = 0.000). Mean pain scores at day 2 in group A were 4.15 ± 0.5, while in group B the scores were 6.65 ± 0.48 (p = 0.000). Mean pain scores at day 3 in group A were 2.25 ± 0.63 and in group B 6.15 ± 0.74 (p = 0.000) as shown in Table 1.
All of the patients in topical NSAIDs group showed mild pain after 3 days of PRK as compared to patients in oral NSAIDs group (100% vs. 0%, p = 0.000) as shown in Table 2. Age and gender showed insignificant association with pain scores (p = 0.132 and p = 0.563 respectively) and pain intensity (p = 0.667 and p = 0.941 respectively). We did not find any adverse event or complication in our patients.
Overall peak pain scores were reported at day 1 as shown in Figure 1.
Discussion
Postoperative pain is potential and significant limitation of PRK. Pain after PRK is due to two main reasons; i) cornea is densely innervated tissue, ii) release of inflammatory mediators leading towards high sensory nerve excitability10. Evidence exists that high pain scores after PRK are significantly associated with dry eyes while insignificantly associated with ablation depth and magnitude of refractive error.11
The phase of pain sensation usually begins after some time of PRK and continues till regeneration of epithelium (at least 5 days).12 However, in our results we found highest mean pain scores at day 1. Sobas et al reported that pain peak level persists after 24–36 hours of PRK.13 Neuffer et al. reported several strategies for pain management after PRK including Bandage contact lens, Postoperative cold patches, topical anesthetic, opioids and NSAIDs.14 In our results, we found significant change in Postoperative pain scores in three days postoperatively with topical NSAIDs as compared to oral NSAIDs (p = 0.000). Cherry et al reported pre–operative topical NSAIDs, BCL are associated with sufficient pain management following PRK.15 Hong et al reported that combination of topical tetracaine with oral coproxamol is effective and safe in reducing pain in PRK patients.16
Evidence exists that ophthalmologist prefer to prescribe short term topical NSAIDs for postoperative PRK pain.17 Moreover, they are approved by FDA and indicated in 0.4% ketorolac, 0.1% diclofenac and 0.5% ketorolac.18 Literature also reported many other regimens of NSAIDs and their efficacy as compared to placebo.19 Topical NSAIDs are associated with several complications such as delayed epithelial healing, irritation, corneal melt and punctuate keratitis.20 We did not find any complication associated with NSAIDs in our study.
We found efficacy of topical NSAIDs more than oral NSAIDs for postoperative PRK pain. Bhala et al. reported similar findings with more emphasis on three days utilization of NSAIDs to minimize chance of adverse events.21 Ripa et al. reported that topical ketorolac eye drops are safe, widely available and inexpensive drugs for controlling pain sensation after PRK as compared to oral naproxen.9 Solomon et al. reported that oral NSAIDs are inferior to topical NSAIDs due to serious renal, gastrointestinal and hepatic side effects in long term outcomes.22
Limitations
Our results are not generalizable to entire population due to small sample size. Large scale comparative studies using different topical agents may allow us to put up reliable guidelines to control postoperative pain after PRK.
Conclusion
Topical nonsteroidal anti–inflammatory drugs are safe and effective for reducing postoperative pain management following photorefractive keratectomy as compared to oral nonsteroidal anti– inflammatory drugs. Further research is required on long term effects of nonsteroidal anti–inflammatory drugs on pain management.
Conflict of interest
None declared by the authors
Authors’ contribution
SJ, MS: Concept, conduct of study, manuscript writing
YL: Supervision, manuscript review
References
Author affiliations:
- Medical Officer, EDO Eye Hospital, Wah Cantt, Pakistan.
- Senior Registrar, Wah Medical College, Wah Cantt, Pakistan.
- Associate Professor, POF Hospital, Wah Cantt, Pakistan.
Abstract
Objective: Most of the ophthalmic surgery is done under topical anesthesia or nerve blocks. Local anesthetic agents are usually used for both analgesic techniques. We hypothesized that nonsteroidal anti–inflammatory drugs (NSAIDs) could be used preoperatively for postoperative pain, either topically or by oral route. Present study aimed to compare mean reduction in pain scores with oral versus topical NSAIDs following photorefractive keratectomy.
Methodology: This prospective study was conducted at Department of Ophthalmology, Eye Donors Organization (EDO) Hospital, Wah Cantt, for 6 months (March 2019–August 2019). A sample size of 40 patients was calculated using World Health Organization calculator. We selected patients through convenient (non–probability) sampling. We took IRB approval, and written consent form the patients. All patients underwent photorefractive keratectomy. Patients were randomly divided (lottery method) into two groups; Group A was treated with topical NSAIDs while group B was treated with oral NSAIDs. Patients were followed for 3 days. We measured pain scores using visual analogue pain scale (VAS). Data analysis was done using SPSS version 24. T–test and fissure exact test were applied. A p ≤ 0.05 was considered significant.
Results: A total of 40 patients were included in study. Mean age of patients was 28.1 ± 2.9 y. There were 21(52.5%) males and 19(46.3%) females. Topical NSAIDs showed significant reduction in pain scores as compared to oral NSAIDs at day 1 (5.25 ± 0.6 vs. 7.20 ± 0.69, p = 0.000), day 2 (4.15 ± 0.5 vs. 6.65 ± 0.48, p = 0.000) day 3 (2.25 ± 0.63 vs. 6.15 ± 0.74, p = 0.000).
Conclusion: Topical nonsteroidal anti–inflammatory drugs are safe and effective for reducing postoperative pain management following photorefractive keratectomy as compared to oral nonsteroidal anti– inflammatory drugs.
Key words: Nonsteroidal anti–inflammatory drugs; Pain; Photorefractive keratectomy
Citation: Javaid S, Shafi M, Lodhi Y. Comparison of postoperative pain in photorefractive keratectomy using topical versus oral nonsteroidal anti–inflammatory drugs. Anaesth. pain intensive care 2021;25(3):324–328. DOI: 10.35975/apic.v25i3.1527
Received: January 29, 2021, Reviewed: February 27, March 13, 2021, Accepted: March 31, 2021
Introduction
Refractive error is the most common cause of the visual impairment (correctable) worldwide.1
According to World Health Organization (WHO), an estimated 285 million individuals were visually impaired with 39 million leading towards blindness globally.2 Literature reported that 90% of visually impaired individuals are resident of developing countries including Pakistan.3 Refractive error can be treated with glasses, contact lenses and surgically.4
Photorefractive keratectomy (PRK) was introduced as first safe and effective surgical treatment of refractive error as surface ablation procedure since 1980s. This procedure includes irradiation of corneal stroma with an ultraviolet beam of 193 nm generated from argon fluoride excimer laser. After epithelium removal, photoablation is used to reshape anterior corneal stroma, and thus correct ametropia. Literature reported that PRK is effective in low to moderate refractive errors (myopia, hypermetropia and astigmatism).5
PRK is indicated in myopia of less than 12 diopter, hypermetropia less than 5 diopters and astigmatism less than 6 diopters. PRK is contraindicated many other eye conditions, in pregnant women and nursing mothers.6
Pain is a common complication of PRK. This sensation is a result of corneal nerve baring after epithelial debridement. However, the condition remains consistent until complete repair of epithelial occur.7 Literature reports several techniques for the pain relieve after PRK, including bandage contact lens, topical morphine, dilute tetracaine eye drops, transepithelial all surface laser ablation, corticosteroids, cycloplegics and nonsteroidal anti–inflammatory drugs (NSAIDs). NSAIDs are the most common drugs used for pain management (e.g. ketorolac tromethamine 0.5% or diclofenac 0.1% for 24–48 h).8
Limited data is available on measuring efficacy of NASIDs in pain management after PRK in Pakistan. Present study aims to compare mean reduction in pain scores of oral vs. topical nonsteroidal anti–inflammatory drugs following photorefractive keratectomy.
Methodology
A prospective study was conducted at Department of Ophthalmology, Eye Donors Organization (EDO) Hospital, Wah Cantt, for 6 months (March 2019–August 2019). A sample size of 40 patients (20 patients in each group) was calculated with µ1 = 5.17, µ2 = 3.21, S.D = 2.25, power of study = 80%, 5% significance level using WHO calculator.9 Patients were selected through non–probability convenient sampling. Institutional review board permission was taken before conduction of study. Written was obtained from all patients before the conduction of study. Patients with age 18–40 years, both genders, low to moderate refractive error (myopia ≤7 D, hypermetropia≤5 D, Astigmatism≤4D) were included in study. Exclusion criteria was based upon keratoconus, significant ocular surface disease, history of allergy, severe side effects to NSAIDs significant asymmetry on corneal mapping, history of ocular herpetic disease, form frusta keratoconus, concurrent therapy with topical/systemic NSAIDs, any ocular pathology except refractive error, history of prior to refractive surgery, predicted residual stromal bed less than 320 microns, any other ocular pathology except refractive error, history of diabetes mellitus and immunological diseases.
Operative Technique
Initially, patients were anaesthetized with the help of 0.5% proparacaine hydrochloride (two drops) and 0.5% tetracaine hydrochloride (preservative free) initially 10 min and then 5 min prior to surgical procedure with povidone iodine solution (5%). The procedure started with central 8.5 mm scoring of corneal epithelium with marker, exposing to balanced salt solution (BSS) with 20% ethanol and placing in 8 mm well (35–40 sec). It was removed from well with the help of surgical sponge and rinsing with 3 ml of BSS. We removed epithelial after residual BSS was dried with sponges. Laser ablation was performed with excimer laser following surgeon’s optimized nomogram. The ocular surface was chilled for 10 sec with BSS after ablation. After 10 sec of chilling, the surface was rinsed with 0.4% ketorolac tromethamine, 1% prednisolone acetate, 0.5% gatifloxacin followed by bandage contact lens placement.
Intervention technique
Patients were randomly (lottery method) divided into two groups; Group A was given topical NSAIDs (ketorolac 0.4%) in both eyes (every 12 h) while group B was given oral naproxen sodium (220 mg) (every 12 h) for 72 h immediately after PRK. Other drugs given to both groups were prednisolone 1% and gatifloxacin 0.5% for one week (4 times a day). However, the bandage contact lens was removed after one week. We recommended oral hydrocodone acetaminophen (5– 325 mg) after every 4 h for breakthrough pain. We used visual analogue scale for pain measurement at 3 consecutive days after surgery
...Data analysis
We used SPSS version 24 for data entry and analysis of variables. Descriptive statistics are presented in terms of mean and standard deviation while categorical and nominal data are presented as frequencies and percentages. We controlled general effect modifiers (gender, age) by stratification in SPSS. Post stratification T test and fissure exact test were applied. A p ≤ 0.05 was considered as statistically significant.
Results
A total of 40 patients were included in the study. Mean age of patients was 28.1 ± 2.9 y. There were 21 (52.5%) male and 19 (46.3%) female patients. Among all, 26 (65%) were in age group 18–30 y and 14 (35%) were in age group 31–40 y. Refractive errors were myopia 30 (75%), hypermetropia 7 (17.5%) and astigmatism 3 (7.5%). Duration of refractive error was ≤ 2 y in 11 (27.5%), while > 2 y in 29 (72.5%) patients.
Mean pain scores at day 1 in Group A were 5.25 ± 0.6 and group B 7.20 ± 0.69 (p = 0.000). Mean pain scores at day 2 in group A were 4.15 ± 0.5, while in group B the scores were 6.65 ± 0.48 (p = 0.000). Mean pain scores at day 3 in group A were 2.25 ± 0.63 and in group B 6.15 ± 0.74 (p = 0.000) as shown in Table 1.
All of the patients in topical NSAIDs group showed mild pain after 3 days of PRK as compared to patients in oral NSAIDs group (100% vs. 0%, p = 0.000) as shown in Table 2. Age and gender showed insignificant association with pain scores (p = 0.132 and p = 0.563 respectively) and pain intensity (p = 0.667 and p = 0.941 respectively). We did not find any adverse event or complication in our patients.
Overall peak pain scores were reported at day 1 as shown in Figure 1.
Discussion
Postoperative pain is potential and significant limitation of PRK. Pain after PRK is due to two main reasons; i) cornea is densely innervated tissue, ii) release of inflammatory mediators leading towards high sensory nerve excitability10. Evidence exists that high pain scores after PRK are significantly associated with dry eyes while insignificantly associated with ablation depth and magnitude of refractive error.11
The phase of pain sensation usually begins after some time of PRK and continues till regeneration of epithelium (at least 5 days).12 However, in our results we found highest mean pain scores at day 1. Sobas et al reported that pain peak level persists after 24–36 hours of PRK.13 Neuffer et al. reported several strategies for pain management after PRK including Bandage contact lens, Postoperative cold patches, topical anesthetic, opioids and NSAIDs.14 In our results, we found significant change in Postoperative pain scores in three days postoperatively with topical NSAIDs as compared to oral NSAIDs (p = 0.000). Cherry et al reported pre–operative topical NSAIDs, BCL are associated with sufficient pain management following PRK.15 Hong et al reported that combination of topical tetracaine with oral coproxamol is effective and safe in reducing pain in PRK patients.16
Evidence exists that ophthalmologist prefer to prescribe short term topical NSAIDs for postoperative PRK pain.17 Moreover, they are approved by FDA and indicated in 0.4% ketorolac, 0.1% diclofenac and 0.5% ketorolac.18 Literature also reported many other regimens of NSAIDs and their efficacy as compared to placebo.19 Topical NSAIDs are associated with several complications such as delayed epithelial healing, irritation, corneal melt and punctuate keratitis.20 We did not find any complication associated with NSAIDs in our study.
We found efficacy of topical NSAIDs more than oral NSAIDs for postoperative PRK pain. Bhala et al. reported similar findings with more emphasis on three days utilization of NSAIDs to minimize chance of adverse events.21 Ripa et al. reported that topical ketorolac eye drops are safe, widely available and inexpensive drugs for controlling pain sensation after PRK as compared to oral naproxen.9 Solomon et al. reported that oral NSAIDs are inferior to topical NSAIDs due to serious renal, gastrointestinal and hepatic side effects in long term outcomes.22
Limitations
Our results are not generalizable to entire population due to small sample size. Large scale comparative studies using different topical agents may allow us to put up reliable guidelines to control postoperative pain after PRK.
Conclusion
Topical nonsteroidal anti–inflammatory drugs are safe and effective for reducing postoperative pain management following photorefractive keratectomy as compared to oral nonsteroidal anti– inflammatory drugs. Further research is required on long term effects of nonsteroidal anti–inflammatory drugs on pain management.
Conflict of interest
None declared by the authors
Authors’ contribution
SJ, MS: Concept, conduct of study, manuscript writing
YL: Supervision, manuscript review
References
- Evans BJ, Rowlands G. Correctable visual impairment in older people: a major unmet need. Ophthalmic Physiol Opt. 2004;24(3):161–180. [PubMed] DOI: 1111/j.1475-1313.2004.00197.x
- WHO Universal eye health: a global action plan 2014–2019. Available at: http://wwwwhoint/blindness/actionplan/en/
- Williams KM, Verhoeven VJ, Cumberland P, et al. Prevalence of refractive error in Europe: the European Eye Epidemiology (E(3)) Consortium. Eur J Epidemiol. 2015;30(4):305–315. [PubMed] DOI: 1007/s10654-015-0010-0
- Haegerstrom–Portnoy G, Schneck ME, Lott LA, Hewlett SE, Brabyn JA. Longitudinal increase in anisometropia in older adults. Optom Vision Sci. 2014;91(1):60–67. [PubMed] DOI: 1097/OPX.0000000000000114
- Alio JL, Soria FA, Abbouda A, Peña–García P. Fifteen years follow–up of photorefractive keratectomy up to 10 D of myopia: outcomes and analysis of the refractive regression. Br J Ophthalmol. 2016 May;100(5):626–32. [PubMed] DOI: 1136/bjophthalmol-2014-306459
- Roszkowska AM, Urso M, Signorino GA, Spadea L, Aragona P. Photorefractive keratectomy after cataract surgery in uncommon cases: long–term results. Int J Ophthalmol. 2018;11(4):612–615. [PubMed] DOI: 18240/ijo.2018.04.12
- Ohana O, Kaiserman I, Domniz Y, Cohen E, Franco O, Sela T, et al. Outcomes of simultaneous photorefractive keratectomy and collagen crosslinking. Can J Ophthalmol. 2018 Oct;53(5):523–528. [PubMed] DOI: 1016/j.jcjo.2017.12.003
- Fay J, Juthani V. Current trends in pain management after photorefractive and phototherapeutic keratectomy. Curr Opin Ophthalmol. 2015 Jul;26(4):255–9. [PubMed] DOI: 1097/ICU.0000000000000170
- Ripa M, Betts B, Dhaliwal S, Wang K, Pouly S, Chen D et al. Survey of postoperative pain in photorefractive keratectomy using topical versus oral nonsteroidal anti–inflammatory drugs. Clin Ophthalmol. 2020;14:1459–1466. [PubMed] DOI: 10.2147/OPTH.S255441
- Müller LJ, Marfurt CF, Kruse F, Tervo TM. Corneal nerves: structure, contents and function. Exp Eye Res. 2003 May;76(5):521-42. [PubMed] DOI: 1016/s0014-4835(03)00050-2
- Rabina G, Boguslavsky II, Mimouni M, Kaiserman I. The association between preoperative dry eye symptoms and postoperative discomfort in patients underwent photorefractive keratectomy. J Ophthalmol. 2019 Feb 18;2019:7029858. [PubMed] DOI: 1155/2019/7029858
- Golan O, Randleman JB. Pain management after photorefractive keratectomy. Curr Opin Ophthalmol. 2018;29(4):306–312. [PubMed] DOI: 1097/ICU.0000000000000486
- Sobas EM, Videla S, Vázquez A, Fernández I, Maldonado JM, Pastor Pain perception description after advanced surface ablation. Clin Ophthalmol. 2017;11:647–655. [PubMed] DOI: 10.2147/OPTH.S134542
- Neuffer MC, Khalifa YM, Moshirfar M, Miffin DM. Prospective comparison of chilled versus room temperature saline irrigation in alcohol–assisted photorefractive keratectomy. Nepal J Ophthalmol. 2013;5(10):154–160. [PubMed] DOI: 3126/nepjoph.v5i2.8706
- Cherry PM. The treatment of pain following excimer laser photorefractive keratectomy: additive effect of local anesthetic drops, topical diclofenac, and bandage soft contact. Ophthalmic Surg Lasers. 1996;27(5 Suppl):S477–S480. [PubMed]
- Hong JP, Nam SM, Im CY, Yoon S, KimIT, Kim KE. Comparison of analgesic effect of preoperative topical diclofenac and ketorolac on postoperative pain after photorefractive keratectomy. J Cataract Refract Surg. 2014;40(10):1689–1696. [PubMed] DOI: 1016/j.jcrs.2014.05.029
- Kontadakis GA, Chronopoulou KG, Tsopouridou R, Tabibian D, Kymionis Nepafenac ophthalmic suspension 0.3% for the management of ocular pain after photorefractive keratectomy.J Refract Surg. 2018;34(3):171–176. [PubMed] DOI: 10.3928/1081597X-20180123-03
- Woreta FA, Gupta A, Hochstetler B, Bower SK. Management of post–photorefractive keratectomy pain. Surv Ophthalmol. 2013;58(6):529–535. [PubMed] DOI: 1016/j.survophthal.2012.11.004
- Verma S, Marshall J. Control of pain after photorefractive keratectomy. J Refract Surg. 1996;12(3):358–364. [PubMed]
- Kim SJ, Flach AJ, Jampol LM. Nonsteroidal anti–inflammatory drugs in ophthalmology. Surv Ophthalmol. 2010;55(2):108–133. [PubMed] DOI: 1016/j.survophthal.2009.07.005
- Bhala N, Emberson J, Merhi A, Abramson S, Arber N, Baron JA, et al. Vascular and upper gastrointestinal effects of nonsteroidal anti–inflammatory drugs: meta–analysis of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779. [PubMed] DOI: 1016/S0140-6736(13)60900-9
- Solomon DH, Husni ME, Libby PA, Yeomans DN, Lincoff MA, Lϋscher FT. The Risk of major NSAID toxicity with celecoxib, ibuprofen, or naproxen: a secondary analysis of the PRECISION trial. Am J Med. 2017;130(12):1415–1422. [PubMed] DOI: 10.1016/j.amjmed.2017.06.028