Salman Shahzad 1 , Tahira Younus 2 , Eitzaz Ud Din Khan 3
Authors affiliations:
Abstract
Bronchobiliary fistula (BBF) is a pathological communication between a bronchus and the biliary tract resulting from various etiologies. Anesthetic management of BBF is challenging because patients may have a repeated chest infection, pleural effusion and perihepatic abdominal collection. These factors affect the safe patient management during controlled mechanical ventilation. We present anesthetic management of a case of a 20-year-old patient requiring endoscopic retrograde cholangiopancreatography (ERCP) to drain the biliary obstruction.
Key words: Bronchobiliary fistula; Moderate Sedation; Bilioptysis; Anesthetic Management, Endoscopic retrograde cholangiopancreatography; Dexmedetomidine
Citation: Shahzad S, Younus T, Khan RU. Anesthetic management for endoscopic retrograde cholangiopancreatography in bronchobiliary fistula – a case report. Anaesth. pain intensive care 2021;25(3):399–401. DOI: 10.35975/apic.v25i3.1517
Received: February 4, 2021; Reviewed: February 19, 2021; Accepted: February 19, 2021
Introduction
Bronchobiliary fistula (BBF) is a rare pathological disorder, reported initially by Peacock in 1850.1 It is an abnormal passage between the biliary tract with a bronchial tree. Etiology includes primary and metastatic tumors, bile duct obstruction secondary to biliary stenosis, cholangiolithiasis, hepatic hydatidosis and trauma.2 The patients usually present with bilioptysis (presence of bile in sputum), persistent cough, chest infections, or respiratory distress due to pleural effusion. Bilioptysis is the pathognomonic clinical feature of BBF. The presence of bilirubin in sputum and pleural effusion fluid is diagnostic for BBF along with imaging studies (CT/MRI), which confirm the presence and help locate the site of BBF. The management depends on the underlying cause, either endoscopic retrograde cholangiopancreatography (ERCP) or surgery.3
Thoracoabdominal trauma can lead to a rare complication of thoracobiliary fistulas, which can present as pleurobiliary or bronchobiliary fistulas.4 Poor pulmonary functions, pleural effusion, subhepatic collection, sepsis, and chronic emaciated condition make this patient difficult and challenging for the anesthesiologists.5 Owing to the disease’s rarity, guidance regarding anesthetic management of BBF is limited. We present anesthetic management of a case of a BBF scheduled for ERCP BBF is limited. We present anesthetic management of a case of a BBF scheduled for ERCP.
Case report
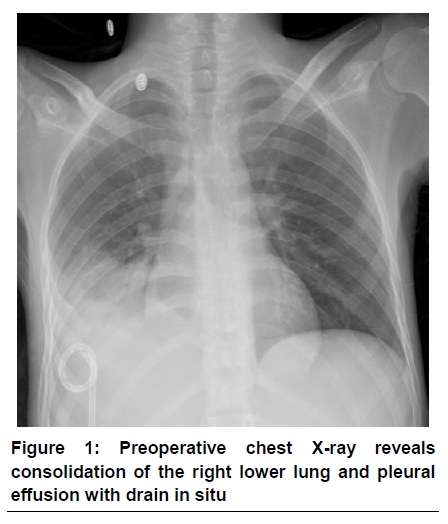
A 20-year-old boy presented with a chronic productive cough associated with green-colored sputum. The patient had a history of exploratory laparotomy and damage control surgery for grade IV liver injury following a blunt abdominal trauma five months ago. An ERCP was performed for the suspected biliary leak after one month. Afterwards, he developed a cough with greenish sputum along with abdominal pain. A laboratory analysis confirmed the presence of bile in the sputum. An ultrasound abdomen showed subdiaphragmatic collection around the surface of the right lobe of the liver. A preoperative chest X-ray demonstrated mild to moderate right-sided pleural effusion without an active lung pathology (Figure 1). CT scan revealed focal collection along the liver’s right lateral margin, which was communicating with one of the right lower lobe bronchi, supporting the diagnosis of a BBF. This had led to right lower lobe collapse and an ERCP was planned to place a biliary stent.
Considering the high risk of developing respiratory complications, full preparations for rapid induction of anesthesia, rapid sequence intubation and possible one lung anesthesia were undertaken. We decided to choose deep sedation as the first option. In case of its failure, general anesthesia was the only option available.
The patient was monitored by electrocardiogram, pulse oximetry, non-invasive blood pressure, bi-spectral index (BIS), and end-tidal CO2 (EtCO2). Topical pharyngeal anesthesia was provided with 4% xylocaine spray before sedation. Intravenous access was established. The patient was placed in the prone position, and supplemental oxygen at 2 L/min was provided with a nasal cannula. A side-stream EtCO2 tubing was placed near the nostril to monitor ventilation. Sedation was initiated with midazolam 2 mg IV, followed by fentanyl 50 µg IV. A bolus dose of 1 µg/kg dexmedetomidine was given over 10 min followed by infusion of 0.2-0.8 µg/kg/h with the target of BIS around 60 to 70. ERCP scope was inserted with ease, and there was no belching and retching during endoscopy. An additional supplementation was given once with propofol 10 mg bolus. The patient maintained spontaneous respiration during (Figure 2) procedure. The procedure lasted for one hour and the patient remained hemodynamically stable. After the conclusion of ERCP, recovery was quick, and the patient was eye-opening within one minute. He was discharged from PACU in stable condition.
Discussion
BBF is challenging for anesthesiologists in terms of poor lung functions, sepsis, malnutrition, requiring one-lung ventilation and postoperative mechanical ventilation. It is imperative to optimize the patient preoperatively by antibiotics, nutritional support, chest physiotherapy and spirometry, and effective bile drainage by placing biliary stent through ERCP. Correction of fluid and electrolyte imbalance is also important.6
Both medical and surgical options have been applied to treat BBF. Conservative management includes antibiotics, correction of electrolyte imbalance, physiotherapy, and nutritional support. Endoscopic retrograde biliary drainage (ERBD) or sphincterotomy through ERCP, endoscopic nasobiliary drainage (ENBD) or percutaneous transhepatic cholangiography (PTC) are less invasive procedures frequently used.7 Surgical management is reserved for cases that fail conservative or less invasive treatments.8
Anesthetic management for BBF has been reported in the literature as case reports. The Royal College of Anesthetists (RCA) recommends double-lumen tube (DLT), invasive blood pressure and central venous pressure monitoring, thoracic epidural analgesia, and postoperative care in an intensive care unit (ICU).9 The major anesthetic challenge for patients with BBF is avoiding positive-pressure ventilation (PPV) and preventing contamination of unaffected lung. It is achieved through rapid sequence anesthesia in reverse Trendelenburg position and by using a DLT.6
Procedural sedation in patients with BBF requires careful planning and implementation to avoid apnea and positive pressure ventilation. Dexmedetomidine is an alpha2-adrenergic agonist used for procedural sedation. It has analgesic properties and causes dose-dependent sedation which is readily reversible. It does not impair respiratory drive and rarely causes apnea.10 We used dexmedetomidine for procedural sedation for ERCP in BBF. Our patient was temporarily hypotensive initially, was managed with a bolus of Ringer’s lactate solution, and thereafter remained hemodynamically stable. Despite prone and slight head-up positioning, the patient maintained spontaneous ventilation maintaining normocapnia.
Conclusion
In summary, BBF is a rare but serious condition that can cause significant respiratory disturbances. Anesthesiologist should be prepared for both procedural sedation and major thoracoabdominal surgery for the management of BBF to prevent spillage of disease from unhealthy to healthy lung and complications such as pneumothorax.
Conflict of interest
None declared by the authors.
Authors’ contribution
SS: Conceptualization, visualization, manuscript writing
TY: Data curation, writing, review & editing
EK: Visualization, writing, review & editing, supervision
References
Authors affiliations:
- Consultant Anesthesiologist, Pakistan Kidney and Liver Institute and Research Centre, Knowledge City, 1 PKLI Avenue, Lahore, Pakistan.
- Senior Registrar, Department of Anesthesiology, Pakistan Kidney and Liver Institute and Research Centre, Knowledge City, 1 PKLI Avenue, Lahore, Pakistan.
- Consultant and Chairman, Department of Anesthesiology, Pakistan Kidney and Liver Institute and Research Centre, Knowledge City, 1 PKLI Avenue, Lahore, Pakistan. | Anesthesia
Abstract
Bronchobiliary fistula (BBF) is a pathological communication between a bronchus and the biliary tract resulting from various etiologies. Anesthetic management of BBF is challenging because patients may have a repeated chest infection, pleural effusion and perihepatic abdominal collection. These factors affect the safe patient management during controlled mechanical ventilation. We present anesthetic management of a case of a 20-year-old patient requiring endoscopic retrograde cholangiopancreatography (ERCP) to drain the biliary obstruction.
Key words: Bronchobiliary fistula; Moderate Sedation; Bilioptysis; Anesthetic Management, Endoscopic retrograde cholangiopancreatography; Dexmedetomidine
Citation: Shahzad S, Younus T, Khan RU. Anesthetic management for endoscopic retrograde cholangiopancreatography in bronchobiliary fistula – a case report. Anaesth. pain intensive care 2021;25(3):399–401. DOI: 10.35975/apic.v25i3.1517
Received: February 4, 2021; Reviewed: February 19, 2021; Accepted: February 19, 2021
Introduction
Bronchobiliary fistula (BBF) is a rare pathological disorder, reported initially by Peacock in 1850.1 It is an abnormal passage between the biliary tract with a bronchial tree. Etiology includes primary and metastatic tumors, bile duct obstruction secondary to biliary stenosis, cholangiolithiasis, hepatic hydatidosis and trauma.2 The patients usually present with bilioptysis (presence of bile in sputum), persistent cough, chest infections, or respiratory distress due to pleural effusion. Bilioptysis is the pathognomonic clinical feature of BBF. The presence of bilirubin in sputum and pleural effusion fluid is diagnostic for BBF along with imaging studies (CT/MRI), which confirm the presence and help locate the site of BBF. The management depends on the underlying cause, either endoscopic retrograde cholangiopancreatography (ERCP) or surgery.3
Thoracoabdominal trauma can lead to a rare complication of thoracobiliary fistulas, which can present as pleurobiliary or bronchobiliary fistulas.4 Poor pulmonary functions, pleural effusion, subhepatic collection, sepsis, and chronic emaciated condition make this patient difficult and challenging for the anesthesiologists.5 Owing to the disease’s rarity, guidance regarding anesthetic management of BBF is limited. We present anesthetic management of a case of a BBF scheduled for ERCP BBF is limited. We present anesthetic management of a case of a BBF scheduled for ERCP.
Case report
A 20-year-old boy presented with a chronic productive cough associated with green-colored sputum. The patient had a history of exploratory laparotomy and damage control surgery for grade IV liver injury following a blunt abdominal trauma five months ago. An ERCP was performed for the suspected biliary leak after one month. Afterwards, he developed a cough with greenish sputum along with abdominal pain. A laboratory analysis confirmed the presence of bile in the sputum. An ultrasound abdomen showed subdiaphragmatic collection around the surface of the right lobe of the liver. A preoperative chest X-ray demonstrated mild to moderate right-sided pleural effusion without an active lung pathology (Figure 1). CT scan revealed focal collection along the liver’s right lateral margin, which was communicating with one of the right lower lobe bronchi, supporting the diagnosis of a BBF. This had led to right lower lobe collapse and an ERCP was planned to place a biliary stent.
Considering the high risk of developing respiratory complications, full preparations for rapid induction of anesthesia, rapid sequence intubation and possible one lung anesthesia were undertaken. We decided to choose deep sedation as the first option. In case of its failure, general anesthesia was the only option available.
The patient was monitored by electrocardiogram, pulse oximetry, non-invasive blood pressure, bi-spectral index (BIS), and end-tidal CO2 (EtCO2). Topical pharyngeal anesthesia was provided with 4% xylocaine spray before sedation. Intravenous access was established. The patient was placed in the prone position, and supplemental oxygen at 2 L/min was provided with a nasal cannula. A side-stream EtCO2 tubing was placed near the nostril to monitor ventilation. Sedation was initiated with midazolam 2 mg IV, followed by fentanyl 50 µg IV. A bolus dose of 1 µg/kg dexmedetomidine was given over 10 min followed by infusion of 0.2-0.8 µg/kg/h with the target of BIS around 60 to 70. ERCP scope was inserted with ease, and there was no belching and retching during endoscopy. An additional supplementation was given once with propofol 10 mg bolus. The patient maintained spontaneous respiration during (Figure 2) procedure. The procedure lasted for one hour and the patient remained hemodynamically stable. After the conclusion of ERCP, recovery was quick, and the patient was eye-opening within one minute. He was discharged from PACU in stable condition.
Discussion
BBF is challenging for anesthesiologists in terms of poor lung functions, sepsis, malnutrition, requiring one-lung ventilation and postoperative mechanical ventilation. It is imperative to optimize the patient preoperatively by antibiotics, nutritional support, chest physiotherapy and spirometry, and effective bile drainage by placing biliary stent through ERCP. Correction of fluid and electrolyte imbalance is also important.6
Both medical and surgical options have been applied to treat BBF. Conservative management includes antibiotics, correction of electrolyte imbalance, physiotherapy, and nutritional support. Endoscopic retrograde biliary drainage (ERBD) or sphincterotomy through ERCP, endoscopic nasobiliary drainage (ENBD) or percutaneous transhepatic cholangiography (PTC) are less invasive procedures frequently used.7 Surgical management is reserved for cases that fail conservative or less invasive treatments.8
Anesthetic management for BBF has been reported in the literature as case reports. The Royal College of Anesthetists (RCA) recommends double-lumen tube (DLT), invasive blood pressure and central venous pressure monitoring, thoracic epidural analgesia, and postoperative care in an intensive care unit (ICU).9 The major anesthetic challenge for patients with BBF is avoiding positive-pressure ventilation (PPV) and preventing contamination of unaffected lung. It is achieved through rapid sequence anesthesia in reverse Trendelenburg position and by using a DLT.6
Procedural sedation in patients with BBF requires careful planning and implementation to avoid apnea and positive pressure ventilation. Dexmedetomidine is an alpha2-adrenergic agonist used for procedural sedation. It has analgesic properties and causes dose-dependent sedation which is readily reversible. It does not impair respiratory drive and rarely causes apnea.10 We used dexmedetomidine for procedural sedation for ERCP in BBF. Our patient was temporarily hypotensive initially, was managed with a bolus of Ringer’s lactate solution, and thereafter remained hemodynamically stable. Despite prone and slight head-up positioning, the patient maintained spontaneous ventilation maintaining normocapnia.
Conclusion
In summary, BBF is a rare but serious condition that can cause significant respiratory disturbances. Anesthesiologist should be prepared for both procedural sedation and major thoracoabdominal surgery for the management of BBF to prevent spillage of disease from unhealthy to healthy lung and complications such as pneumothorax.
Conflict of interest
None declared by the authors.
Authors’ contribution
SS: Conceptualization, visualization, manuscript writing
TY: Data curation, writing, review & editing
EK: Visualization, writing, review & editing, supervision
References
- Peacock TB. Case in Which Hydatids Were Expectorated, and One of Suppuration in a Hydatid Cyst of the Liver Communicating with the Lungs. Edinb Med Surg J. 1850;74(184):33–46. [PubMed]
- Liao G-Q, Wang H, Zhu G-Y, Zhu K-B, Lv F-X, Tai S. Management of acquired bronchobiliary fistula: A systematic literature review of 68 cases published in 30 years. World J Gastroenterol. 2011 Sep 7;17(33):3842–9. [PubMed] DOI: 3748/wjg.v17.i33.3842
- Crnjac A, Pivec V, Ivanecz A. Thoracobiliary fistulas: literature review and a case report of fistula closure with omentum majus. Radiol Oncol. 2013;47(1):77–85. [PubMed] DOI: 2478/raon-2013-0003
- Prodromos P, Condilis N. Thoracobiliary fistula. A rare complication of thoracoabdominal trauma. Ann Ital Chir. 2009 Dec;80(6):467–70. [PubMed]
- Mitra S, Bhatia N, Dey N, Dalal U. Bronchobiliary fistula: an anesthetic challenge! J Clin Anesth. 2009;21(5):360–2. [PubMed] DOI: 1016/j.jclinane.2008.08.029
- Lee J, Jung SM, Lee Y, Kim SY. Anesthetic management for a patient with bronchobiliary fistula after pancreaticoduodenectomy: A case report. Medicine (Baltimore). 2019;98(19):e15694. [PubMed] DOI: 1097/MD.0000000000015694
- Joh HK, Park SY. Surgical Treatment of Bronchobiliary Fistula with Pulmonary Resection and Omentopexy. Korean J Thorac Cardiovasc Surg. 2020 ;53(1):38–40. [PubMed] DOI: 5090/kjtcs.2020.53.1.38
- Rabiou S, Lakranbi M, Ouadnouni Y, Panaro F, Smahi M. Surgical management of hydatid Bilio-bronchial fistula by exclusive thoracotomy. Int J Surg Lond Engl. 2017;41:112–8. [PubMed] DOI: 1016/j.ijsu.2017.03.074
- Anaesthesia UK: Thoracic anaesthesia [Internet]. [cited 2020 Dec 27]. Available from: https://www.frca.co.uk/article.aspx?articleid=100675
- Miller RD. Miller’s Anesthesia. 8th ed. Philadelphia: Churchill-Livingstone, Elsevier; 2015.