Roshdi R. Al-metwalli1, Summayah M. Fallatah2, Talal M. Alghamdi3
Author affiliations:
Correspondence: Prof. Roshdi R. Al-metwalli, University of Imam Abdulrahman Bin Faisal / Department of Anesthesiology / King Fahad Hospital of University, PO Box 40081; Post Code 31952- Al-Khobar, Saudi Arabia; Tel. 00966138966666-Ext-2152; Mobile; 00966502893485; E-mail: rmetwalli@yahoo.com; Email: grmetwalli@gmail.com
Abstract
The endotracheal tube (ETT) cuff's principal function is to implement proper tracheal sealing at a pressure high enough to prevent both gas leak and fluid aspiration, and low enough to maintain tracheal perfusion. Clinicians are often concerned primarily with the volume of air required to inflate an ETT cuff. However, the most important factor is how much pressure will be exerted on the tracheal mucosa when the cuff is properly distended. Cuff over-inflation complications range from sore throat to tracheal ischemia with tracheal rupture and fistula formation. The ideal ETT cuff pressure has not been defined with a high degree of certainty however most anesthesiologists generally recommend a target pressure of 20 to 30 cmH2O. Although trachea-gas sealing can be achieved at ETT cuff pressure of 20 cmH2O, microaspiration can occur at a cuff pressure of 60 cmH2O. Since the introduction of cuffed ETT in the mid- 20th century, several modifications in the cuff's shape and material have been done to address these challenges. It has been proven that the pressure within the inflated cuff is a dynamic process. As such, various clinical factors will significantly impact the pressure reading. Thus, continuous regulation of ETT cuff pressure should be routine practice. Our review included 158 articles that addressed the background into the development of cuffed ETT, function and anatomy of the ETT cuff system, cuff pressure and sealing characteristics, ETT cuff pressure regulation, microaspiration, and factors affecting ETT cuff pressure.
Key words: Endotracheal Tube; Cuff pressure; Microaspiration
Citation: Al-metwalli RR, Fallatah SM, Alghamdi TM. Endotracheal tube cuff pressure: An overlooked risk. Anaesth. pain intensive care 2021;25(1):88-97;
DOI: 10.35975/apic.v25i1.1445
Received: 2 November 2020, Reviewed: 24 December 2020, Accepted: 1 January 2021
Introduction & research strategy
The cuff's principal function is to ensure proper sealing between the patient's trachea and the cuff wall to prevent the aspiration of fluid down into the trachea, as well as the gas leak during PPV. Another important but less obvious function of the cuff is that when the cuff is inflated uniformly, it will keep the tube central in the trachea and protect against mucosal injury by the tip of the tube.1 Cuff pressure needs to be high enough to seal the trachea to restrict micro-aspiration and allow accurate anesthetic and respiratory gas monitoring. Also, Cuff pressure must be low enough to allow adequate perfusion of tracheal mucosa.2 High cuff pressure decreases regional tracheal blood flow and is usually associated with lesions including post-extubation phenomenon , tracheomalacia, bleeding, tracheal rupture, stenosis, nerve palsy, and tracheoesophageal fistula.3-8
We reviewed the research articles and texts published from 1950 to August 15, 2020, using three bibliographic databases namely PubMed-MEDLINE and EMBASE. The keywords used were “endotracheal tube cuff pressure”, “endotracheal tube cuff pressure monitoring”, “endotracheal tube cuff pressure regulators”,” endotracheal tube cuff pressure changes”,” complications of cuffed endotracheal tube,” and “micro-aspiration and ventilator-associated pneumonia.” Citation search via manual review of references from primary articles was also performed. Several studies and case reports (668 articles) have addressed the endotracheal cuff pressure. However, we recruited 158, publications that studied the history and demonstrated the monitoring and regulation of the endotracheal cuff pressure, as well as the important factors affecting the cuff pressure, and related complications.
History
Trendelenburg (1869) is credited with the development of the first detachable inflatable cuff. He designed a tight seal using a thin rubber bag mounted around the end of a tracheostomy tube which was used to prevent aspiration during anesthesia.9 In 1926 Arthar Guedel experimented with various rubber items, including the dental dam, fingers of rubber gloves, and rubber condoms to construct the first inflatable cuff to Magill's rubber tube. In 1931 his friend Ralph Waters encouraged him to provide a leak-proof ETT seal that would complement Waters's "closed-circuit" for positive pressure ventilation (PPV) and was acknowledged for starting a time of ETT design.10 The optimal position of the cuff was not intuitively obvious at that time. Their first cuffs ranged from three to four inches long and were designed to be placed half above and half below the glottis. Users found that it could not be adequately inflated without disrupting its position. Following rigorous testing for the cuff's best length and location, they created a cuff that was 1.5 inches long and designed to be positioned directly below the vocal cords.11 During the polio epidemic in Europe and the United States (the early 1960s), reusable rubber ETTs and metal tracheotomy tubes with red rubber cuffs classified as high-pressure low-volume (HPLV) were the main airways used.12 In 1968, advancements in polymer technology allowed for the development of a more effective disposable polyvinyl chloride (PVC) tube with a high- pressure low-volume cuff.13
Cuff system
The cuff system (Figure 1) consists of the cuff itself (functions as an inflatable balloon), and the pilot catheter which serves as a method of inflation. A pilot
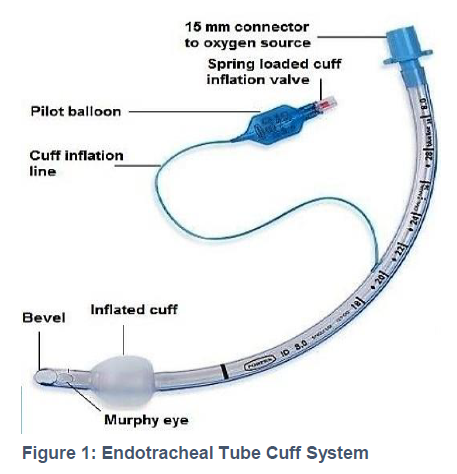
balloon serves as a perceptible gauge of cuff pressure outside the patient, as well as a small pressure vendor to diminish minor changes in intra-cuff pressure. A one-way valve blocks gas from escaping the cuff and functions as a Port to attach a syringe or pressure-monitoring equipment. Salpekar, P. et al. (1966) had introduced a double cuffed tracheostomy tube, which was inflated alternatively at half-hour intervals to minimize the adverse effects of prolonged use of single-cuff rubber endotracheal tube on the larynx and tracheal mucosa. Since then, a double-cuff endotracheal tube has been designed.14
Low-and high-pressure ETT cuffs
The high-pressure low-volume (HPLV) cuff has a small diameter at rest, and for sealing in the trachea, it requires a high intra-cuff pressure to overcome the low compliance of the cuff itself.1 So; prolonged use of HPLV cuff will carry the risk of ischemic damage to the tracheal mucosa with subsequent serious complications.4-8 As the HPVL cuff became identified as a problem, some clinicians began stretching the PVC tube using boiling water to induce an adequate seal at lower tracheal pressures resulting in a high-volume low-pressure (HVLP) cuff.15 In the 1970s an HVLP PVC-cuffed ETT was developed and has become the conventional ETT in use today. The HVLP cuff has a thin compliant wall that, when inflated, conforms easily to the irregular borders of the tracheal wall, sealing the trachea at a lower intra-cuff pressure, which correlates closely with the tracheal mucosal pressure.7 Nevertheless, HVLP cuffs are associated with fewer complications than HPLV cuffs. Potential serious tracheal injuries may occur if the cuff pressure is maintained within the pressure-volume curve's steep part. (the ideal range is 20-30 cmH2O).16
Safe cuff pressure & effective tracheal sealing conflict
As we mentioned earlier, the ETT cuff's principal function is to ensure proper tracheal seal at a pressure high enough to prevent aspiration and gas leak, and low as much as necessary to maintain adequate tracheal perfusion. An intra-cuff pressure greater than 34 cmH2O results in decreased tracheal perfusion, whereas; total cessation of tracheal blood flow occurs at about 50 cmH2O.17 On the other hand, although 20 cmH2O intra-cuff pressure can induce tracheal gas seal, microaspiration still can happen at pressure up to 60 cmH2O.18 Several devices and techniques have been introduced to regulate and control the ETT cuff pressure at a safe level, and others to improve tracheal sealing and reduce microaspiration and subsequent ventilator-associated pneumonia (VAP).
Regulation of ETT cuff pressure Estimation of cuff pressure by Pilot balloon palpation
A common technique used by anesthetists is to palpate the external balloon (contiguous with the cuff) after intubation in order to get a rough estimation of the intra-cuff pressure. However, our previous study, as well as, other sever studies has demonstrated that this unreliable technique puts patients at the risk of unnecessary high intra-cuff pressure with subsequent laryngotracheal complication.19-23
Inflation of the cuff to a sealing pressure (Minimal occlusive volume)
Although it has been reported by several studies that, in absence of reliable monitoring of ETT cuff pressure, the application of sealing pressure was a secure alternative technique.19 Nevertheless, during the utilization of nitrous oxide (N2O) or high positive end-expiratory pressure (PEEP) or in presence of high peak inspiratory pressure (PIP) the sealing pressure can go beyond the safe level (30 cmH2O).21
Inflation of the cuff to a safe target pressure
Although this guarantees tracheal perfusion, it cannot ensure sealing in the presence of high PIP.21
Aneroid Manometer
There are two described aneroid manometers for adjustment of ETT intra-cuff pressure:
Stopcock-pressure gauge (Figure 2).
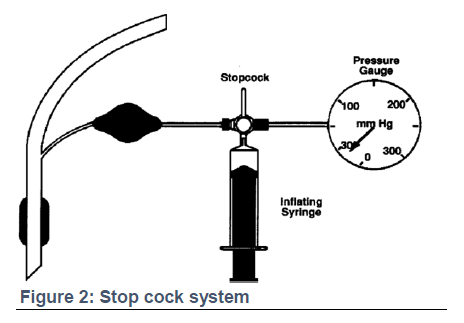
Posey cuff inflator (Figure 3).

Both are popular, precise, and accurate devices, but require frequent calibration, air leak can happen during attachment with a substantial decrease in preset pressure, and they create potential risks of silent aspiration and cross-contamination secondary to the multiple patient use.22
Regulating Valves
They maintain the ETT cuff pressure at a secure limit using internal pressure regulating valve.
Brandt tube system
The Brandt tube system is often useful during a long period of anesthesia, particularly during using N2O because of its effectiveness in stabilizing the intra-cuff pressure via its large pilot balloon reservoir and an internal pressure regulator valve.
Lanz pressure-regulating Valve [Hi-Lo cuff with Lanz valve] (Figure 4).
It limits intra-cuff pressure to approximately 30 cmH2O, however it is only available for adult use and it may not provide an appropriate seal during the use of high PIP or PEEP.

Electronic ETT cuff pressure controller Smith’s Pressure Easy Cuff Controller (Figure 5)
It is designed to monitor tracheal cuff pressure continuously. Its indicator window signals sustained cuff pressure between 20-30 cmH2O. The airway pressure auto-feedback feature increases cuff pressure to assure adequate sealing during periods of high pressures. It is designed for single-patient use; thus, it reduces the potential for infection. However, the precise inflation pressure isn't expected (20, 25, or 30 cmH2O?) and doesn't protect from increasing cuff

pressure (e.g., during coughing, change position, or use of N2O).
VBM- ETT cuff controller (Figure 6)
VBM allows ergonomic handheld cuff pressure gauges and an electronic cuff pressure gauge, which keeps the cuff pressure constant. Small leaks are compensated, and potential pressure rise due to diffusion of anesthetic gases are released to the set value allowing sealing with lowest pressures.

Tracheal tube cuff inflation guided by the pressure-volume loop (PV-L) closure
(PV-L) is frequently used to assess dynamic lung compliance, detection of lung over-inflation, or air leak.23 In a prospective, randomized study, the ETT cuff was inflated initially by increments of 0.5 mL air until complete closure of the PV-L (the expiratory limb reached zero and joined the starting point of inspiratory limb) as an indicator for proper ETT cuff sealing.24
Volume time curve as a guide for accurate cuff inflation
Analysis of the volume time curve, as shown by Bolzan et al., indicated air leak where the descending branch of the time–volume curve did not reach Zero-value. Then gradual inflation of the ETT cuff until the descending limb reached zero value would ensure proper sealing.25
Automated Cuff Pressure Modulator
Chadha et al. demonstrated a significant reduction in the risk of subglottic and tracheal injury in an experimental study using a device to modulate the cuff pressure from 25 cmH2O during inspiration to 7 cmH2O during expiration.26 However, the concern regarding the risk of aspiration during the cuff modulation cycle's deflation stage should be investigated.
Constant monitoring of the intra-cuff pressure
Intra-cuff pressure may be monitored constantly using the transducer of the invasive pressure monitoring device. Krishna et al. successfully used the transducer portion of an invasive arterial pressure monitoring tool without a fluid interface (directly connected to the pilot balloon).27
Optimization of ETT cuff filling by continuous upper airway CO2 monitoring
Efrati et al. continuously assessed the leak across the ETT cuff via monitoring carbon dioxide pressure (PCO2) in the upper airway, at the oropharynx, and in the nose's nares.28 He also introduced an efficient way for ETT cuff pressure optimization, using the automated cuff pressure control, based on subglottic measures of CO2 levels with the use of AnapnoGuard ETT.29
A mobile terminal application program
Recently Wang WZ et al. investigated the use of a mobile terminal application program in endotracheal tube (ETT) cuff pressure measurement to ensure that the pressure falls within the recommended range.30
Prevention of microaspiration
The ETT cuff's incomplete airway seal allows the aspiration of colonized oropharyngeal secretions at the time of intubation or during mechanical ventilation. Such microaspiration represents one of the leading pathogenic pathways to ventilator-associated pneumonia (VAP).31 The following are some of various preventive approaches to decrease the occurrence of VAP.
Cuff pressure
A general method to maintain a safe inflation pressure is inflating the cuff either to a recommended standard pressure between 20 and 30 cmH2O or sealing pressure that fully occludes the airway and prevents a leak during PPV.32-33 Maintaining the cuff pressure within the above-recommended ranges wasn't enough to prevent microaspiration.34 Nevertheless, higher pressure is of worry because of the occlusion of mucosal capillary blood flow.35 The soundest practice is to use the recommended cuff pressure that is not associated with tracheal injury and the application of additional measures that help prevent channeling of fluid past the cuff, such as modifying the ETT and cuff design as well as the mode of mechanical ventilation.
Cuff design
When the standard HVLP- PVC cuff is fully inflated, it reaches a size 1.5 – 2 times larger than an average trachea of an adult.3 The architecture of the trachea is non-uniform, non-cylindrical, irregular, and D-shaped. Unluckily, longitudinal folds are created resulting in microaspirations along these folds when this cuff expands.36 Limiting the number of longitudinal folds that form during cuff expansion is one of the major triggers of developing better cuff design (material and shape).
Cuff material
Cuff material made of ultra-thin (10 microns) polyurethane instead of the standard PVC (50-80 micron) may provide a sufficient seal and less fluid leakage at a lower cuff pressure than PVC cuffs in both bench, and clinical studies.14,37 However, a new study showed that it does not prevent microaspiration.38 Several prototypes of cuffs made of silicone (a low-volume, low-pressure silicone cuff), natural latex rubber (with 0.5 mL of gel between the cuff layers) and lycra-polyurethane (a thin-walled cuff made of Lycra polyurethane) were lately evaluated in vitro and clinical studies.39-40 All these cuffs did not form folds upon their inflation and provided, high sealing efficacy even in the absence of PEEP.41
Cuff Shape
A tapered cuff shape was designed to overcome leakage and folds during cuff expansion. The larger diameter at the top of the cuff is designed in such a
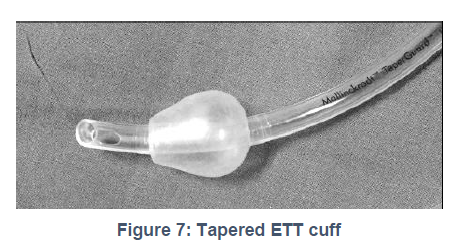
way that as the diameter narrows it matches the internal tracheal diameter preventing longitudinal folding. A bench-top study has proven this tapered cuff shape to significantly decrease leakage during cuff expansion as compared to the conventional cylindrical cuff shape42 (Figure 7).
Aspiration of subglottic secretion
A meta-analysis that included 2442 patients reported a significant reduction in VAP incidence and a reduction in the length of stay in the ICU with the use of subglottic aspiration.43 The early concerns with the aspiration system are the risk of tracheal injury and suction failure.44-45 Recently, Spapen et al. have created a model double cuffed ETT with an auxiliary port between the cuffs.46 This assures continuous positive airway pressure (CPAP) to be delivered. In the inner cuff space, the force of pressure produces total tracheal sealing and efficiently blocked leakage during 24 h mechanical ventilation in an in vitro model.
Manipulation of mechanical ventilation
Pitts et al. believed that PEEP and PIP create a hydrostatic barrier to fluid movement across the ETT cuff to a much lesser extent.47 Generally, expiratory time is about twice the length of inspiratory time. As such, at a PEEP level of 15 cmH2O, PEEP had an overwhelmingly significant effect on fluid leakage that neutralized the effect of PIP. The ventilation mode can also affect leakage of fluid past the ETT cuff. However, this effect was not to the extent observed with PEEP and peak inspiratory pressure. Although the differences were small, the most significant movement of fluid occurred during pressure than volume-controlled ventilation.
ETT cuff pressure in children
For a long time, the cuffed (ETT) was not recommended by most pediatric anesthetists for children younger than 5-8 years.48 Primary because a cuffed ETT's width had to be 1-2 sizes smaller than the un-cuffed tube. Consequently, flow resistance and work of breathing would be dramatically increased in those spontaneously breathing children.49
The second reason was the earlier reports of airway morbidity caused by poor design and material of earlier cuffed ETT.50 With the introduction of a newly developed pediatric tracheal tube designed with an ultrathin (10 m) polyurethane high volume-low pressure (HVLP) cuff (Micro cuff pediatric tracheal tube), as well as, mechanical ventilation became a common practice cuffed tracheal tubes in neonates and smaller children have become more prevalent in pediatric anesthesia during the last decade with advantages similar to those in adults.48
In addition to the fact, the cuff's inflation can compensate for small size tube and minimize repeated intubation to choose the proper size of the tube. However, if the cuffed ETT tube is not large enough, more air can be used to inflate the cuff and seal the trachea. But this would transform the cuff from the intended HVLP cuff to an unwanted HVHP cuff.51 Table 1: Factors affecting ETT cuff pressure
.
Factors affecting ETT cuff pressure
The intra-cuff pressure can be affected by various factors, including environmental factors [high airway pressure (discussed), ventilation with nitrous oxide, duration of surgery, type of surgery, and altitude], patient factors [variations in patient's body, head and neck position] cuff related factors [differences in cuff compliance and diameter], and therapeutic interventions [neuromuscular blockade, and body temperature]. (Table 1)
Summary
The endotracheal tube cuff is designed to provide a tracheal seal at a pressure high enough to prevent aspiration and gas leak and low as much as to maintain adequate tracheal perfusion. Although the recommended safe intra-cuff pressure (20-30 cmH2O) most properly induce tracheal gas seal, microaspiration still can occur at pressure up to 60 cmH2O. Recently, some ETT manufacturers have introduced new cuff designs (with modified shape and/ or material), which help induce effective tracheal sealing and prevent channeling of fluid past the cuff at an intra-cuff pressure within the safe recommended range or even lower. Although the intra-cuff pressure may be assessed initially following the cuff inflation after endotracheal intubation, the intra-cuff pressure can be modified dynamically throughout the case because of the many clinical and environmental factors. So continuous or frequent intermittent monitoring of ETT cuff pressure should be a routine practice in all intubated and ventilated adult or pediatrics.
Acknowledgment
The authors feel grateful to the staff members of the Department of Anesthesiology, King Fahad Hospital of University Imam Abdulrahman Bin Faisal.
Conflict of interest
The authors report no conflicts of interest in this work.
Authors’ contribution
RRA: Concept and design of the study, manuscript editing, final approval
SMF: Concept of study, literature search, revision
TMA: Concept, acquisition of data, drafting the paper
References
Author affiliations:
- Professor of Anesthesia and Intensive Care; E-mail: rmetwalli@yahoo.com
- Assistant professor of Anesthesia and Intensive Care; E-mail: smfallatah@iau.edu.sa
- Demonstrator of Anesthesia and Intensive Care; E-mail: Dr.t.alghamdi@gmail.com
Correspondence: Prof. Roshdi R. Al-metwalli, University of Imam Abdulrahman Bin Faisal / Department of Anesthesiology / King Fahad Hospital of University, PO Box 40081; Post Code 31952- Al-Khobar, Saudi Arabia; Tel. 00966138966666-Ext-2152; Mobile; 00966502893485; E-mail: rmetwalli@yahoo.com; Email: grmetwalli@gmail.com
Abstract
The endotracheal tube (ETT) cuff's principal function is to implement proper tracheal sealing at a pressure high enough to prevent both gas leak and fluid aspiration, and low enough to maintain tracheal perfusion. Clinicians are often concerned primarily with the volume of air required to inflate an ETT cuff. However, the most important factor is how much pressure will be exerted on the tracheal mucosa when the cuff is properly distended. Cuff over-inflation complications range from sore throat to tracheal ischemia with tracheal rupture and fistula formation. The ideal ETT cuff pressure has not been defined with a high degree of certainty however most anesthesiologists generally recommend a target pressure of 20 to 30 cmH2O. Although trachea-gas sealing can be achieved at ETT cuff pressure of 20 cmH2O, microaspiration can occur at a cuff pressure of 60 cmH2O. Since the introduction of cuffed ETT in the mid- 20th century, several modifications in the cuff's shape and material have been done to address these challenges. It has been proven that the pressure within the inflated cuff is a dynamic process. As such, various clinical factors will significantly impact the pressure reading. Thus, continuous regulation of ETT cuff pressure should be routine practice. Our review included 158 articles that addressed the background into the development of cuffed ETT, function and anatomy of the ETT cuff system, cuff pressure and sealing characteristics, ETT cuff pressure regulation, microaspiration, and factors affecting ETT cuff pressure.
Key words: Endotracheal Tube; Cuff pressure; Microaspiration
Citation: Al-metwalli RR, Fallatah SM, Alghamdi TM. Endotracheal tube cuff pressure: An overlooked risk. Anaesth. pain intensive care 2021;25(1):88-97;
DOI: 10.35975/apic.v25i1.1445
Received: 2 November 2020, Reviewed: 24 December 2020, Accepted: 1 January 2021
Introduction & research strategy
The cuff's principal function is to ensure proper sealing between the patient's trachea and the cuff wall to prevent the aspiration of fluid down into the trachea, as well as the gas leak during PPV. Another important but less obvious function of the cuff is that when the cuff is inflated uniformly, it will keep the tube central in the trachea and protect against mucosal injury by the tip of the tube.1 Cuff pressure needs to be high enough to seal the trachea to restrict micro-aspiration and allow accurate anesthetic and respiratory gas monitoring. Also, Cuff pressure must be low enough to allow adequate perfusion of tracheal mucosa.2 High cuff pressure decreases regional tracheal blood flow and is usually associated with lesions including post-extubation phenomenon , tracheomalacia, bleeding, tracheal rupture, stenosis, nerve palsy, and tracheoesophageal fistula.3-8
We reviewed the research articles and texts published from 1950 to August 15, 2020, using three bibliographic databases namely PubMed-MEDLINE and EMBASE. The keywords used were “endotracheal tube cuff pressure”, “endotracheal tube cuff pressure monitoring”, “endotracheal tube cuff pressure regulators”,” endotracheal tube cuff pressure changes”,” complications of cuffed endotracheal tube,” and “micro-aspiration and ventilator-associated pneumonia.” Citation search via manual review of references from primary articles was also performed. Several studies and case reports (668 articles) have addressed the endotracheal cuff pressure. However, we recruited 158, publications that studied the history and demonstrated the monitoring and regulation of the endotracheal cuff pressure, as well as the important factors affecting the cuff pressure, and related complications.
History
Trendelenburg (1869) is credited with the development of the first detachable inflatable cuff. He designed a tight seal using a thin rubber bag mounted around the end of a tracheostomy tube which was used to prevent aspiration during anesthesia.9 In 1926 Arthar Guedel experimented with various rubber items, including the dental dam, fingers of rubber gloves, and rubber condoms to construct the first inflatable cuff to Magill's rubber tube. In 1931 his friend Ralph Waters encouraged him to provide a leak-proof ETT seal that would complement Waters's "closed-circuit" for positive pressure ventilation (PPV) and was acknowledged for starting a time of ETT design.10 The optimal position of the cuff was not intuitively obvious at that time. Their first cuffs ranged from three to four inches long and were designed to be placed half above and half below the glottis. Users found that it could not be adequately inflated without disrupting its position. Following rigorous testing for the cuff's best length and location, they created a cuff that was 1.5 inches long and designed to be positioned directly below the vocal cords.11 During the polio epidemic in Europe and the United States (the early 1960s), reusable rubber ETTs and metal tracheotomy tubes with red rubber cuffs classified as high-pressure low-volume (HPLV) were the main airways used.12 In 1968, advancements in polymer technology allowed for the development of a more effective disposable polyvinyl chloride (PVC) tube with a high- pressure low-volume cuff.13
Cuff system
The cuff system (Figure 1) consists of the cuff itself (functions as an inflatable balloon), and the pilot catheter which serves as a method of inflation. A pilot
balloon serves as a perceptible gauge of cuff pressure outside the patient, as well as a small pressure vendor to diminish minor changes in intra-cuff pressure. A one-way valve blocks gas from escaping the cuff and functions as a Port to attach a syringe or pressure-monitoring equipment. Salpekar, P. et al. (1966) had introduced a double cuffed tracheostomy tube, which was inflated alternatively at half-hour intervals to minimize the adverse effects of prolonged use of single-cuff rubber endotracheal tube on the larynx and tracheal mucosa. Since then, a double-cuff endotracheal tube has been designed.14
Low-and high-pressure ETT cuffs
The high-pressure low-volume (HPLV) cuff has a small diameter at rest, and for sealing in the trachea, it requires a high intra-cuff pressure to overcome the low compliance of the cuff itself.1 So; prolonged use of HPLV cuff will carry the risk of ischemic damage to the tracheal mucosa with subsequent serious complications.4-8 As the HPVL cuff became identified as a problem, some clinicians began stretching the PVC tube using boiling water to induce an adequate seal at lower tracheal pressures resulting in a high-volume low-pressure (HVLP) cuff.15 In the 1970s an HVLP PVC-cuffed ETT was developed and has become the conventional ETT in use today. The HVLP cuff has a thin compliant wall that, when inflated, conforms easily to the irregular borders of the tracheal wall, sealing the trachea at a lower intra-cuff pressure, which correlates closely with the tracheal mucosal pressure.7 Nevertheless, HVLP cuffs are associated with fewer complications than HPLV cuffs. Potential serious tracheal injuries may occur if the cuff pressure is maintained within the pressure-volume curve's steep part. (the ideal range is 20-30 cmH2O).16
Safe cuff pressure & effective tracheal sealing conflict
As we mentioned earlier, the ETT cuff's principal function is to ensure proper tracheal seal at a pressure high enough to prevent aspiration and gas leak, and low as much as necessary to maintain adequate tracheal perfusion. An intra-cuff pressure greater than 34 cmH2O results in decreased tracheal perfusion, whereas; total cessation of tracheal blood flow occurs at about 50 cmH2O.17 On the other hand, although 20 cmH2O intra-cuff pressure can induce tracheal gas seal, microaspiration still can happen at pressure up to 60 cmH2O.18 Several devices and techniques have been introduced to regulate and control the ETT cuff pressure at a safe level, and others to improve tracheal sealing and reduce microaspiration and subsequent ventilator-associated pneumonia (VAP).
Regulation of ETT cuff pressure Estimation of cuff pressure by Pilot balloon palpation
A common technique used by anesthetists is to palpate the external balloon (contiguous with the cuff) after intubation in order to get a rough estimation of the intra-cuff pressure. However, our previous study, as well as, other sever studies has demonstrated that this unreliable technique puts patients at the risk of unnecessary high intra-cuff pressure with subsequent laryngotracheal complication.19-23
Inflation of the cuff to a sealing pressure (Minimal occlusive volume)
Although it has been reported by several studies that, in absence of reliable monitoring of ETT cuff pressure, the application of sealing pressure was a secure alternative technique.19 Nevertheless, during the utilization of nitrous oxide (N2O) or high positive end-expiratory pressure (PEEP) or in presence of high peak inspiratory pressure (PIP) the sealing pressure can go beyond the safe level (30 cmH2O).21
Inflation of the cuff to a safe target pressure
Although this guarantees tracheal perfusion, it cannot ensure sealing in the presence of high PIP.21
Aneroid Manometer
There are two described aneroid manometers for adjustment of ETT intra-cuff pressure:
Stopcock-pressure gauge (Figure 2).
Posey cuff inflator (Figure 3).
Both are popular, precise, and accurate devices, but require frequent calibration, air leak can happen during attachment with a substantial decrease in preset pressure, and they create potential risks of silent aspiration and cross-contamination secondary to the multiple patient use.22
Regulating Valves
They maintain the ETT cuff pressure at a secure limit using internal pressure regulating valve.
Brandt tube system
The Brandt tube system is often useful during a long period of anesthesia, particularly during using N2O because of its effectiveness in stabilizing the intra-cuff pressure via its large pilot balloon reservoir and an internal pressure regulator valve.
Lanz pressure-regulating Valve [Hi-Lo cuff with Lanz valve] (Figure 4).
It limits intra-cuff pressure to approximately 30 cmH2O, however it is only available for adult use and it may not provide an appropriate seal during the use of high PIP or PEEP.
Electronic ETT cuff pressure controller Smith’s Pressure Easy Cuff Controller (Figure 5)
It is designed to monitor tracheal cuff pressure continuously. Its indicator window signals sustained cuff pressure between 20-30 cmH2O. The airway pressure auto-feedback feature increases cuff pressure to assure adequate sealing during periods of high pressures. It is designed for single-patient use; thus, it reduces the potential for infection. However, the precise inflation pressure isn't expected (20, 25, or 30 cmH2O?) and doesn't protect from increasing cuff
pressure (e.g., during coughing, change position, or use of N2O).
VBM- ETT cuff controller (Figure 6)
VBM allows ergonomic handheld cuff pressure gauges and an electronic cuff pressure gauge, which keeps the cuff pressure constant. Small leaks are compensated, and potential pressure rise due to diffusion of anesthetic gases are released to the set value allowing sealing with lowest pressures.
Tracheal tube cuff inflation guided by the pressure-volume loop (PV-L) closure
(PV-L) is frequently used to assess dynamic lung compliance, detection of lung over-inflation, or air leak.23 In a prospective, randomized study, the ETT cuff was inflated initially by increments of 0.5 mL air until complete closure of the PV-L (the expiratory limb reached zero and joined the starting point of inspiratory limb) as an indicator for proper ETT cuff sealing.24
Volume time curve as a guide for accurate cuff inflation
Analysis of the volume time curve, as shown by Bolzan et al., indicated air leak where the descending branch of the time–volume curve did not reach Zero-value. Then gradual inflation of the ETT cuff until the descending limb reached zero value would ensure proper sealing.25
Automated Cuff Pressure Modulator
Chadha et al. demonstrated a significant reduction in the risk of subglottic and tracheal injury in an experimental study using a device to modulate the cuff pressure from 25 cmH2O during inspiration to 7 cmH2O during expiration.26 However, the concern regarding the risk of aspiration during the cuff modulation cycle's deflation stage should be investigated.
Constant monitoring of the intra-cuff pressure
Intra-cuff pressure may be monitored constantly using the transducer of the invasive pressure monitoring device. Krishna et al. successfully used the transducer portion of an invasive arterial pressure monitoring tool without a fluid interface (directly connected to the pilot balloon).27
Optimization of ETT cuff filling by continuous upper airway CO2 monitoring
Efrati et al. continuously assessed the leak across the ETT cuff via monitoring carbon dioxide pressure (PCO2) in the upper airway, at the oropharynx, and in the nose's nares.28 He also introduced an efficient way for ETT cuff pressure optimization, using the automated cuff pressure control, based on subglottic measures of CO2 levels with the use of AnapnoGuard ETT.29
A mobile terminal application program
Recently Wang WZ et al. investigated the use of a mobile terminal application program in endotracheal tube (ETT) cuff pressure measurement to ensure that the pressure falls within the recommended range.30
Prevention of microaspiration
The ETT cuff's incomplete airway seal allows the aspiration of colonized oropharyngeal secretions at the time of intubation or during mechanical ventilation. Such microaspiration represents one of the leading pathogenic pathways to ventilator-associated pneumonia (VAP).31 The following are some of various preventive approaches to decrease the occurrence of VAP.
Cuff pressure
A general method to maintain a safe inflation pressure is inflating the cuff either to a recommended standard pressure between 20 and 30 cmH2O or sealing pressure that fully occludes the airway and prevents a leak during PPV.32-33 Maintaining the cuff pressure within the above-recommended ranges wasn't enough to prevent microaspiration.34 Nevertheless, higher pressure is of worry because of the occlusion of mucosal capillary blood flow.35 The soundest practice is to use the recommended cuff pressure that is not associated with tracheal injury and the application of additional measures that help prevent channeling of fluid past the cuff, such as modifying the ETT and cuff design as well as the mode of mechanical ventilation.
Cuff design
When the standard HVLP- PVC cuff is fully inflated, it reaches a size 1.5 – 2 times larger than an average trachea of an adult.3 The architecture of the trachea is non-uniform, non-cylindrical, irregular, and D-shaped. Unluckily, longitudinal folds are created resulting in microaspirations along these folds when this cuff expands.36 Limiting the number of longitudinal folds that form during cuff expansion is one of the major triggers of developing better cuff design (material and shape).
Cuff material
Cuff material made of ultra-thin (10 microns) polyurethane instead of the standard PVC (50-80 micron) may provide a sufficient seal and less fluid leakage at a lower cuff pressure than PVC cuffs in both bench, and clinical studies.14,37 However, a new study showed that it does not prevent microaspiration.38 Several prototypes of cuffs made of silicone (a low-volume, low-pressure silicone cuff), natural latex rubber (with 0.5 mL of gel between the cuff layers) and lycra-polyurethane (a thin-walled cuff made of Lycra polyurethane) were lately evaluated in vitro and clinical studies.39-40 All these cuffs did not form folds upon their inflation and provided, high sealing efficacy even in the absence of PEEP.41
Cuff Shape
A tapered cuff shape was designed to overcome leakage and folds during cuff expansion. The larger diameter at the top of the cuff is designed in such a
way that as the diameter narrows it matches the internal tracheal diameter preventing longitudinal folding. A bench-top study has proven this tapered cuff shape to significantly decrease leakage during cuff expansion as compared to the conventional cylindrical cuff shape42 (Figure 7).
Aspiration of subglottic secretion
A meta-analysis that included 2442 patients reported a significant reduction in VAP incidence and a reduction in the length of stay in the ICU with the use of subglottic aspiration.43 The early concerns with the aspiration system are the risk of tracheal injury and suction failure.44-45 Recently, Spapen et al. have created a model double cuffed ETT with an auxiliary port between the cuffs.46 This assures continuous positive airway pressure (CPAP) to be delivered. In the inner cuff space, the force of pressure produces total tracheal sealing and efficiently blocked leakage during 24 h mechanical ventilation in an in vitro model.
Manipulation of mechanical ventilation
Pitts et al. believed that PEEP and PIP create a hydrostatic barrier to fluid movement across the ETT cuff to a much lesser extent.47 Generally, expiratory time is about twice the length of inspiratory time. As such, at a PEEP level of 15 cmH2O, PEEP had an overwhelmingly significant effect on fluid leakage that neutralized the effect of PIP. The ventilation mode can also affect leakage of fluid past the ETT cuff. However, this effect was not to the extent observed with PEEP and peak inspiratory pressure. Although the differences were small, the most significant movement of fluid occurred during pressure than volume-controlled ventilation.
ETT cuff pressure in children
For a long time, the cuffed (ETT) was not recommended by most pediatric anesthetists for children younger than 5-8 years.48 Primary because a cuffed ETT's width had to be 1-2 sizes smaller than the un-cuffed tube. Consequently, flow resistance and work of breathing would be dramatically increased in those spontaneously breathing children.49
The second reason was the earlier reports of airway morbidity caused by poor design and material of earlier cuffed ETT.50 With the introduction of a newly developed pediatric tracheal tube designed with an ultrathin (10 m) polyurethane high volume-low pressure (HVLP) cuff (Micro cuff pediatric tracheal tube), as well as, mechanical ventilation became a common practice cuffed tracheal tubes in neonates and smaller children have become more prevalent in pediatric anesthesia during the last decade with advantages similar to those in adults.48
In addition to the fact, the cuff's inflation can compensate for small size tube and minimize repeated intubation to choose the proper size of the tube. However, if the cuffed ETT tube is not large enough, more air can be used to inflate the cuff and seal the trachea. But this would transform the cuff from the intended HVLP cuff to an unwanted HVHP cuff.51 Table 1: Factors affecting ETT cuff pressure
| I. Patient factors | |
| Variations in patient's body head and neck positions | Lizy et al. reported significant deviations in cuff pressure occurred with all 16 different changes in the body, head, and neck positions (P<0 .05) in 12 orally intubated and mechanically ventilated ICU patients. They could not guess which patient would have high cuff pressure in particular positions.52 |
| II. Environmental factors | |
| 1. Use of nitrous oxide | N2O is highly insoluble in hemoglobin and exhibits a low blood-gas coefficient. As such, a large gradient develops between blood and an inflated cuff. N2O diffuses into the cuff at a greater rate than nitrogen diffuses out of the cuff. This results in excessive cuff pressure. Thus, the cuff's inflation with either an anesthetic gas or distilled water can overcome the disproportionate increase in ETT cuff volumes/pressures during N2O anesthesia.53 |
| 2. Altitude
|
Patients transported via helicopter and unpressurized aircraft often receive ventilation through a cuffed ETT inflated before the flight, owing to decreasing barometric pressure at a rate of approximately 30 mbar/1000 feet.54 Mann. Et al have advised reducing the ETT cuff volume by 0.06 ml per 1000 foot ascent per one ml of initial cuff inflation. The cuff should be re-inflated with the same amount of air on the descent to avoid air leakage. This rule of thumb is appropriate for use with all ETTs regardless of size or manufacturer.55 However, Weisberg N et al. failed to demonstrate the expected linear relationship between ETT cuff pressures and the maximum altitude achieved during typical air-medical transportation.56 He stated that the effect of altitude change on ETT at altitudes less than 3,000 is insignificant and as such does not require a modification in practice to saline-filled cuffs. |
| 3. Type of surgery | Tracheal shortening during the laparoscopic surgery could be due to cephalad movement of the carina and the conformational change of the trachea by abdominal insufflation, which may result in elevated cuff pressure. Increases in cuff pressure were neither correlated with BMI nor the commonly used range of intra-abdominal pressure (10 to 15 mmHg).57 |
| 4. Duration of surgery | Care must be exercised when modulating the intra-cuff pressure as the potential risk of over or under inflation during a prolonged surgery is higher due to the dynamic factors influencing the pressure within the inflated cuff. The changes in ETT cuff pressure from the baseline pressure values after initial inflation may take 6 hours.55 |
| III. Cuff related factors | |
| 5. Differences in cuff compliance and diameter. | As discussed earlier (Page3) |
| 6. Measurement procedure. | An experimental study demonstrated an average decrease in cuff pressure by 6.6 ± 1.9 cmH2O when connecting the cuff inflator to the pilot balloon. The cuff pressure decreased more when an extension tube was used. The cuff pressure decreased more with ETTs of smaller size and with those with pyriform cuffs.58 |
| IV. Therapeutic interventions | |
| 1. Neuromuscular blockade | Girling et al. assessed the extent of neuromuscular block (NMB) at the larynx by measuring the cuff pressure in an ETT placed between the vocal cords.59 They evaluated the decrease in resting cuff pressure (RCP) after the administration of rocuronium and the effect of this decrease on the assessment of NB. The mean RCP decreased from 21 ± 4 to 12 ± 5 mm Hg after rocuronium. At 50% of NMB at the hand, the RCP reduced to 62% ± 18%, and At 75% block at the hand, the RCP reduced to 52% ± 11%. They conclude that a muscle relaxant-induced decrease in resting tension at the larynx perhaps confounds the assessment of NMB via cuff pressure measurement. |
| 2. Body temperature | Inada et al. measured intracuff pressure in 29 consecutive patients undergoing cardiac surgery with CPB using mild to deep hypothermia. Cuff pressure decreased significantly during hypothermic CPB from the mean baseline value of 20 (SE 0.2) to 8.0 (1.0) mm Hg (p < 0.01) and then increased to baseline value after discontinuation of CPB.60 They concluded that the decrease in ICP during the hypothermic phase of CPB may protect the tracheal mucosa against hypotensive ischemic injury. |
Factors affecting ETT cuff pressure
The intra-cuff pressure can be affected by various factors, including environmental factors [high airway pressure (discussed), ventilation with nitrous oxide, duration of surgery, type of surgery, and altitude], patient factors [variations in patient's body, head and neck position] cuff related factors [differences in cuff compliance and diameter], and therapeutic interventions [neuromuscular blockade, and body temperature]. (Table 1)
Summary
The endotracheal tube cuff is designed to provide a tracheal seal at a pressure high enough to prevent aspiration and gas leak and low as much as to maintain adequate tracheal perfusion. Although the recommended safe intra-cuff pressure (20-30 cmH2O) most properly induce tracheal gas seal, microaspiration still can occur at pressure up to 60 cmH2O. Recently, some ETT manufacturers have introduced new cuff designs (with modified shape and/ or material), which help induce effective tracheal sealing and prevent channeling of fluid past the cuff at an intra-cuff pressure within the safe recommended range or even lower. Although the intra-cuff pressure may be assessed initially following the cuff inflation after endotracheal intubation, the intra-cuff pressure can be modified dynamically throughout the case because of the many clinical and environmental factors. So continuous or frequent intermittent monitoring of ETT cuff pressure should be a routine practice in all intubated and ventilated adult or pediatrics.
Acknowledgment
The authors feel grateful to the staff members of the Department of Anesthesiology, King Fahad Hospital of University Imam Abdulrahman Bin Faisal.
Conflict of interest
The authors report no conflicts of interest in this work.
Authors’ contribution
RRA: Concept and design of the study, manuscript editing, final approval
SMF: Concept of study, literature search, revision
TMA: Concept, acquisition of data, drafting the paper
References
- Alian AA, Shelley KH. Understanding Anesthesia Equipment, 5th Edition. Anesthesiology. 2008;109:754–755. [Free full text] DOI:1097/ALN.0b013e3181863209
- Mehta S, Mickiewicz M. Pressure in large volume, low pressure cuffs: its significance, measurement and regulation. Intensive Care Med. 1985;11(5):267-272. [PubMed] DOI: 1007/BF00260364
- Combes X, Schauvliege F, Peyrouset O, Motamed C, Kiro K, Dhonneur G, et al. Intracuff pressure and tracheal morbidity: Influence of filling cuff with saline during nitrous oxide anesthesia. Anesthesiology. 2001;95(5):1120-1124. [PubMed] DOI: 1097/00000542-200111000-00015
- Fan CM, Ko PCI, Tsai KC, Chiang WC, Chang YC, Chen WJ, et al. Tracheal rupture complicating emergent endotracheal intubation. Am J Emerg Med. 2004;22(4):289-293. [PubMed] DOI: 1016/j.ajem.2004.04.012
- Terashima H, Sakurai T, Takahashi S, Saitoh M, Hirayama K. Postintubation tracheal stenosis; problems associated with choice of management. Kyobu Geka. 2002;55(10):837-842. [PubMed]
- Lu YH. Unilateral Vocal Cord Paralysis following Endotracheal Intubation - A Case Report. Acta Anaesthesiol Sin. 1999;37(4):221-224. [PubMed]
- Otani S, Fujii H, Kurasako N, Ishizu T, Tanaka T, Kousogabe Y, et al. Recurrent nerve palsy after endotracheal intubation. Japanese J Anesthesiol. 1998;47(3):350-355. [PubMed]
- Pelc P, Prigogine T, Bisschop P, Jortay A. Tracheoesophageal fistula: Case report and review of literature. Acta Otorhinolaryngol Belg. 2001;55(4):273-278. [PubMed]
- White GMJ. Evolution of endotracheal and endobronchial intubation. Br J Anaesth. 1960;32:235-246. [PubMed] DOI: 1093/bja/32.5.235
- Watson WF. Development of the PVC endotracheal tube. Biomaterials. 1980;1(1):41-6. [PubMed] DOI: 1016/0142-9612(80)90058-7
- Efrati S, Deutsch I, Gurman GM. Endotracheal tube cuff-small important part of a big issue. J Clin Monit Comput. 2012;26(1):53-60. [PubMed] DOI: 1007/s10877-011-9333-x
- Cooper JD, Grillo HC. Analysis of problems related to cuffs on intratracheal tubes. Chest. 1972;62(2):Suppl:21S-27S. [PubMed] DOI: 1378/chest.62.2_Supplement.21S
- Colice GL. Technical standards for tracheal tubes. Clin Chest Med. 1991;12(3):433-448. [PubMed]
- Salpekar PD. Double-cuff endotracheal tube. Br Med J. 1971;3(5773):525. [PubMed] DOI: 1136/bmj.3.5773.525
- Geffin B, Pontoppidan H. Reduction of tracheal damage by the prestretching of inflatable cuffs. Anesthesiology. 1969;31(5):462-463. [PubMed] DOI: 1097/00000542-196911000-00019
- Riley E, Degroot K, Hannallah M. The high-pressure characteristics of the cuff of the intubating laryngeal mask endotracheal tube. Anesth Analg. 1999;89(6):1588. [PubMed] DOI: 1097/00000539-199912000-00062
- Seegobin RD, Van Hasselt GL. Endotracheal cuff pressure and tracheal mucosal blood flow: endoscopic study of effects of four large volume cuffs. Br Med J. 1984; [PubMed] DOI: 1136/bmj.288.6422.965
- Dullenkopf A, Gerber A, Weiss M. Fluid leakage past tracheal tube cuffs: Evaluation of the new Microcuff endotracheal tube. Intensive Care Med. 2003;29(10):1849-1853. [PubMed] DOI: 1007/s00134-003-1933-6
- Al-Metwalli RR, Al-Ghamdi AA, Mowafi HA, Sadek S, Abdulshafi M, Mousa WF. Is sealing cuff pressure, easy, reliable and safe technique for endotracheal tube cuff inflation: A comparative study. Saudi J Anaesth. 2011;5(2):185-189. [PubMed] DOI: 4103/1658-354X.82795
- Fernandez R, Blanch L, Mancebo J, Bonsoms N, Artigas A. Endotracheal tube cuff pressure assessment: Pitfalls of finger estimation and need for objective measurement. Crit Care Med. 1990;18(12):1423-1426. [PubMed]
- Sengupta P, Sessler DI, Maglinger P, Wells S, Vogt A, Durrani J, et al. Endotracheal tube cuff pressure in three hospitals, and the volume required to produce an appropriate cuff pressure. BMC Anesthesiol. 2004;4(1):8. [PubMed] DOI: 1186/1471-2253-4-8
- Aeppli N, Lindauer B, Steurer MP, Weiss M, Dullenkopf A. Endotracheal tube cuff pressure changes during manual cuff pressure control manoeuvres: An in-vitro assessment. Acta Anaesthesiol Scand. 2019;63(1):55-60. [PubMed] DOI: 1111/aas.13249
- Sinha SK, Nicks JJ, Donn SM. Graphic analysis of pulmonary mechanics in neonates receiving assisted ventilation. Arch Dis Child Fetal Neonatal Ed. 1996;75(3):F213-218. [PubMed] DOI: 1136/fn.75.3.f213
- Almarakbi WA, Kaki AM. Tracheal tube cuff inflation guided by pressure volume loop closure associated with lower postoperative cuff-related complications: Prospective, randomized clinical trial. Saudi J Anaesth. 2014;8(3):328-334. [PubMed] DOI: 4103/1658-354X.136422
- Bolzan DW, Gomes WJ, Peixoto TCA, Faresin SM, Carvalho ACDC, De Paola ÂAV, et al. Clinical use of the volume-time curve for endotracheal tube cuff management. Respir Care. 2014;59(11):1628-1635. [PubMed] DOI: 4187/respcare.02683
- Chadha NK, Gordin A, Luginbuehl I, Patterson G, Campisi P, Taylor G, et al. Automated cuff pressure modulation: A novel device to reduce endotracheal tube injury. Arch Otolaryngol Head Neck Surg. 2011;137(1):30-34. [PubMed] DOI: 1001/archoto.2010.228
- Krishna SG, Ramesh AS, Jatana KR, Elmaraghy C, Merz M, Ruda J, et al. A technique to measure the intracuff pressure continuously: An in vivo demonstration of its accuracy. Paediatr Anaesth. 2014;24(9):999-1004. [PubMed] DOI: 1111/pan.12437
- Efrati S, Leonov Y, Oron A, Siman-Tov Y, Averbukh M, Lavrushevich A, et al. Optimization of endotracheal tube cuff filling by continuous upper airway carbon dioxide monitoring. Anesth Analg. 2005;101(4):1081-1088. [PubMed] DOI: 1213/01.ane.0000167641.64815.1a
- Efrati S, Bolotin G, Levi L, Zaaroor M, Guralnik L, Weksler N, et al. Optimization of Endotracheal Tube Cuff Pressure by Monitoring CO2 Levels in the Subglottic Space in Mechanically Ventilated Patients: A Randomized Controlled Trial. Anesth Analg. 2017;125(4):1309-1315. [PubMed] DOI: 1213/ANE.0000000000002358
- Wang WZ, Zhou YY, Wang ZJ, Zhu ML, Yao XY, Yu J Di, et al. A mobile terminal application program was used for endotracheal tube cuff pressure measurement. J Clin Monit Comput. 2020;1–6. [PubMed] DOI: 1007/s10877-020-00499-7
- Valencia M, Torres A. Ventilator-associated pneumonia. Curr Opin Crit Care. 2009 Feb;15(1):30-35. [PubMed] DOI: 1097/mcc.0b013e3283220e78
- Coffin SE, Klompas M, Classen D, Arias KM, Podgorny K, Anderson DJ, et al. Strategies to Prevent Ventilator-Associated Pneumonia in Acute Care Hospitals. Infect Control Hosp Epidemiol. 2008;35(8):915-936. [PubMed] DOI: 1086/677144
- Sultan P, Carvalho B, Rose BO, Cregg R. Endotracheal tube cuff pressure monitoring: a review of the evidence. J Perioper Pract. 2011;21(11):379-386. [PubMed] DOI: 1177/175045891102101103
- Valencia M, Ferrer M, Farre R, Navajas D, Badia JR, Nicolas JM, et al. Automatic control of tracheal tube cuff pressure in ventilated patients in semirecumbent position: A randomized trial. Crit Care Med. 2007;35(6):1543-1549. [PubMed] DOI: 1097/01.CCM.0000266686.95843.7D
- Bernhard WN, Cottrell JE, Sivakumaran C, Patel K, Yost L, Turndorf H. Adjustment of intracuff pressure to prevent aspiration. Anesthesiology. 1979;50(4):363-366. [PubMed] DOI: 1097/00000542-197904000-00018
- Pavlin EG, VanNimwegan D, Hornbein TF. Failure of a high compliance low pressure cuff to prevent aspiration. Anesthesiology. 1975;42(2):216-219. [PubMed] DOI: 11097/00000542-197502000-00019
- Liu S hong, Yan X xin, Cao S qing, An S chang, Zhang L juan. The effect of subglottic secretion drainage on prevention of ventilator-associated lower airway infection. Zhonghua Jie He He Hu Xi Za Zhi. 2006;29(1):19-22. [PubMed]
- Miller MA, Arndt JL, Konkle MA, Chenoweth CE, Iwashyna TJ, Flaherty KR, et al. A polyurethane cuffed endotracheal tube is associated with decreased rates of ventilator-associated pneumonia. J Crit Care. 2011;26(3):280-286. [PubMed] DOI: 1016/j.jcrc.2010.05.035
- Zanella A, Cressoni M, Epp M, Stylianou M, Kolobow T. A double-layer tracheal tube cuff designed to prevent leakage: A bench-top study. Intensive Care Med. 2008;34(6):1145-1149. [PubMed] DOI: 1007/s00134-008-1016-9
- Young PJ, Pakeerathan S, Blunt MC, Subramanya S. A low-volume, low-pressure tracheal tube cuff reduces pulmonary aspiration. Crit Care Med. 2006;34(3):632-639. [PubMed] DOI: 1097/01.CCM.0000201406.57821.5B
- Kolobow T, Cressoni M, Epp M, Corti I, Cadringher P, Zanella A. Comparison of a novel Lycra endotracheal tube cuff to standard polyvinyl chloride cuff and polyurethane cuff for fluid leak prevention. Respir Care. 2011;56(8):1095-1099. [PubMed] DOI: 4187/respcare.01099
- Zanella A, Scaravilli V, Isgrò S, Milan M, Cressoni M, Patroniti N, et al. Fluid leakage across tracheal tube cuff, effect of different cuff material, shape, and positive expiratory pressure: A bench-top study. Intensive Care Med. 2011;37(2):343-347. [PubMed] DOI: 1007/s00134-010-2106-z
- Muscedere J, Rewa O, McKechnie K, Jiang X, Laporta D, Heyland DK. Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: A systematic review and meta-analysis. Crit Care Med. 2011 Aug;39(8):1985-1991. [PubMed] DOI: 1097/CCM.0b013e318218a4d9
- Harvey RC, Miller P, Lee JA, Bowton DL, MacGregor DA. Potential mucosal injury related to continuous aspiration of subglottic secretion device. Anesthesiology. 2007;107(4):666-669. [PubMed] DOI: 1097/01.anes.0000282083.83319.5f
- Dragoumanis CK, Vretzakis GI, Papaioannou VE, Didilis VN, Vogiatzaki TD, Pneumatikos IA. Investigating the failure to aspirate subglottic secretions with the evac endotracheal tube. Anesth Analg. 2007;105(4):1083-1085. [PubMed] DOI: 1213/01.ane.0000278155.19911.67
- Spapen H, Suys E, De Regt J, Troubleyn J, Jonckheer J, De Waele E. An endotracheal tube providing “pressurized sealing” prevents fluid leakage in mechanically ventilated critically ill patients: a pilot study. J Anesth. 2020;34(1):144-148. [PubMed] DOI: 1007/s00540-019-02707-4
- Pitts R, Fisher D, Sulemanji D, Kratohvil J, Jiang Y, Kacmarek R. Variables affecting leakage past endotracheal tube cuffs: A bench study. Intensive Care Med. 2010;36(12):2066-2073. [PubMed] DOI: 1007/s00134-010-2048-5
- Uejima T. Cuffed endotracheal tubes in pediatric patients. Anesth Analg. 1989;68:423. [PubMed] DOI: 1213/00000539-198903000-00062
- Hawkins DB. Glottic and subglottic stenosis from endotracheal intubation. Laryngoscope. 1977;87(3):339-346. [PubMed] DOI: 10.1288/00005537-197703000-00006
- Weiss M, Dullenkopf A, Gysin C, Dillier CM, Gerber AC. Shortcomings of cuffed paediatric tracheal tubes. Br J Anaesth. 2004;92(1):78-88. [PubMed] DOI: 1093/bja/aeh023
- Krishna SG, Hakim M, Sebastian R, Dellinger HL, Tumin D, Tobias JD. Cuffed endotracheal tubes in children: the effect of the size of the cuffed endotracheal tube on intracuff pressure. Paediatr Anaesth. 2017;27(5):494-500. [PubMed] DOI: 1111/pan.13099
- Lizy C, Swinnen W, Labeau S, Poelaert J, Vogelaers D, Vandewoude K, et al. Cuff pressure of endotracheal tubes after changes in body position in critically ill patients treated with mechanical ventilation. Am J Crit Care. 2014;23(1):e1-8. [PubMed] DOI: 4037/ajcc2014489
- Stanley TH, Kawamura R, Graves C. Effects of nitrous oxide on volume and pressure of endotracheal tube cuffs. Anesthesiology. 1974;41(3):256-262. [PubMed] DOI: 1097/00000542-197409000-00007
- Mann C, Parkinson N, Bleetman A. Endotracheal tube and laryngeal mask airway cuff volume changes with altitude: A rule of thumb for aeromedical transport. Emerg Med J. 2007;4(3):165-167. [PubMed] DOI: 1136/emj.2006.039933
- Kako H, Goykhman A, Ramesh AS, Krishna SG, Tobias JD. Changes in intracuff pressure of a cuffed endotracheal tube during prolonged surgical procedures. Int J Pediatr Otorhinolaryngol. 2015;79(1):76-79 [PubMed] DOI: 1016/j.ijporl.2014.11.017
- Weisberg SN, McCall JC, Tennyson J. Altitude-Related Change in Endotracheal Tube Cuff Pressures in Helicopter EMS. West J Emerg Med. 2017;18(4):624-629. [PubMed] DOI: 5811/westjem.2017.3.32078
- Yildirim ZB, Uzunkoy A, Cigdem A, Ganidagli S, Ozgonul A. Changes in cuff pressure of endotracheal tube during laparoscopic and open abdominal surgery. Surg Endosc. 2012;26(2):398-401. [PubMed] DOI: 1007/s00464-011-1886-8
- Asai S, Motoyama A, Matsumoto Y, Konami H, Imanaka H, Nishimura M. Decrease in cuff pressure during the measurement procedure: An experimental study. J Intensive Care. 2014;2(1):34. [PubMed] DOI: 1186/2052-0492-2-34
- Girling KJ, Bedforth NM, Spendlove JL, Mahajan RP. Assessing neuromuscular block at the larynx: The effect of change in resting cuff pressure and a comparison with video imaging in anesthetized humans. Anesth Analg. 1999;88(2):426-431. [PubMed] DOI: 1097/00000539-199902000-00038
- Inada T, Kawachi S, Kuroda M. Tracheal tube cuff pressure during cardiac surgery using cardiopulmonary bypass. Br J Anaesth. 1995;74(3):283-286. [PubMed] DOI: 1093/bja/74.3.283