Akash Nirmal, Yashpal Singh, Sharad Kumar Mathur, Satish Patel
Department of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University (IMS- BHU), Varanasi 22005. (India)
Akash Nirmal [talkwithakash@yahoo.com]
Yashpal Singh [dryashacin1999@rediffmail.com]
Sharad Kumar Mathur [skmathurbhu@gmail.com]
Satish Patel [doc.satish.patel@gmail.com]
Correspondence: Dr Yashpal Singh, Dept. of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University (IMS- BHU), Varanasi-221005, UP, (India);
E-mail: dryashacin1999@rediffmail.com; Phone: +919918424416
Received: 22 August 2019;
Reviewed: 8, 9 October 2019; 6, 7 November 2019;
Revised: 18 November 2019;
Reviewed: 19 November 2019;
Accepted: 20 November 2019
ABSTRACT
Background: Intrathecal ropivacaine is now routinely used for lower limb surgery. Adjuvants e.g. fentanyl, dexmedetomidine or morphine etc. are commonly used to prolong the intraoperative anesthesia or postoperative analgesia. The available literature lacks information on use of butorphanol and nalbuphine as adjuvants with 0.75% isobaric ropivacaine. We aimed to compare nalbuphine and butorphanol as adjuvant with isobaric ropivacaine in lower limb orthopedic surgeries.
Methodology: After institutional ethical committee approval and informed written consent, a total of 108 patients of ages between 18 to 65 y, of either sex, American Society of Anesthesiologists (ASA) grade ӏ & ӏӏ, scheduled for elective lower limb orthopedic surgeries, were enrolled and randomly allocated into two groups: Group RN; to receive isobaric ropivacaine (0.75%, 7.5 mg/ml) 2.5 ml plus nalbuphine 500 µg (0.5 ml), and Group RB; to receive isobaric ropivacaine 2.5 ml plus butorphanol 100 µg (0.5 ml) intrathecally. Primary outcome measure was the duration of sensory‑motor blockade from the time of intrathecal drug administration. Statistical analysis was performed by using t-test and chi-square test as applicable. A p < 0.05 was considered as significant.
Results: Duration of sensory (p < 0.001) and motor blockade (p = 0.02) was significantly prolonged in nalbuphine group than butorphanol group. Onset of blockade was earlier in nalbuphine group. Duration of motor block and sensory analgesia was prolonged in group RN (p < 0.001). Perioperative hemodynamic parameters and the observed side effects including bradycardia, hypotension, nausea and vomiting, sedation and shivering were comparable between the two groups (p = 0.77).
Conclusion: Intrathecal nalbuphine produces prolonged motor blockade as well as postoperative analgesia than intrathecal butorphanol when used as adjuvants to isobaric 0.75% ropivacaine.
Key words: Nalbuphine; Butorphanol; Postoperative analgesia
Citation: Nirmal A, Singh Y, Mathur SK, Patel S. Comparison between intrathecal nalbuphine and butorphanol as adjuvants to isobaric ropivacaine in elective lower limb orthopedic surgeries: A prospective, randomized, double blind study. Anaesth pain & intensive care 2019;23(4):382-386.
DOI: 10.35975/apic.v23i4.1171
INTRODUCTION
With advancement in drugs and technique, spinal anesthesia is now gold standard in lower limb orthopedic surgery. Various studies have clearly demonstrated advantage of neuraxial anesthesia in term of significant reduction in mortality and morbidity in comparison to general anesthesia.1 For the last many years local anesthetic (LA) bupivacaine has been used for spinal anesthesia due to its intense block characteristics. Now-a-days, bupivacaine is slowly being replaced by newer LA including ropivacaine in lower limb and lower abdominal surgeries.2-5 Ropivacaine is a long acting amide LA, structurally very similar to other pipecoloxylidides, first synthesized by Ekenstam.6 It is a pure s-enantiomer having less motor blockade and reduced cardiotoxicity which favors its attractiveness.
Various adjuvants have been tried to improve efficacy, duration of action and safety of LAs, but opioids are the most desired due to its prolonged analgesic action. Fentanyl, morphine, buprenorphine, butorphanol, midazolam, clonidine and dexmedetomidine have been used as adjuvants.7,8 Nalbuphine is an opioid, potent analgesic, structurally related to oxymorphone. It is highly lipid soluble with agonist action at κ-receptor and an antagonist activity at µ-receptor. There have been studies of neuraxial administration of nalbuphine, shown to produce significant analgesia with minimal respiratory depression.9,10 There were safety issues regarding intrathecal uses of nalbuphine; however none of the abnormalities had been encountered through all these years and it was found to be safe for neuraxial blockade. Butorphanol is morphine type synthetic opioid analgesic and structurally related to levorphanol. It acts as an agonist on κ and mixed agonist-antagonist action at µ-opioid receptors. It has been shown to improve the analgesic duration of LA and helps in decreasing analgesic utilization.11-12
Review of literature on nalbuphine and butorphanol with isobaric ropivacaine in adult patients is scarce. So we planned this study to compare nalbuphine and butorphanol with intrathecal isobaric ropivacaine in elective lower limb orthopedic surgeries. Primary outcome of our study was a comparison of block characteristics and duration of postoperative analgesia. Secondary outcomes includes comparison of hemodynamic parameters and adverse events, if any.
METHODOLOGY
After institutional ethical approval and written informed consent, this prospective, randomized, double blind, interventional clinical study was conducted at SS Hospital and Trauma Centre, Institute of Medical Sciences, Banaras Hindu University (IMS-BHU) Varanasi, during academic year 2015-17. Patients with a history of hypersensitivity to study drugs, general contraindications to spinal anesthesia, morbid obesity and end organ damage were excluded.
A total of 108 patients of ages between 18 to 65 y, of either sex, American Society of Anesthesiologists (ASA) grade ӏ & ӏӏ, scheduled for elective lower limb orthopedic surgeries, were randomly allocated into two groups: Group RN; to receive isobaric ropivacaine (0.75%, 7.5 mg/ml) 2.5 ml plus nalbuphine 500 µg (0.5 ml), and Group RB; to receive isobaric ropivacaine 2.5 ml plus butorphanol 100 µg (0.5 ml) intrathecally. Randomization was performed by an anesthesiologist involved in studied drug preparation. Further procedure and the monitoring were performed by another investigator unaware of group allocation. Patients were also blinded to the drug regimen utilized for spinal anesthesia. In the sitting position under standard aseptic precautions, lumbar puncture was performed at L3‑L4 intervertebral space in midline approach by 25 gauge Quincke spinal needle. The studied drug solution was injected over a period of 10–15 sec after the confirmation of free flow of CSF and patients were turned to the supine position.
Primary outcome measure was the duration of sensory‑motor blockade from the time of intrathecal drug administration. Sensory level was assessed by pin prick method bilaterally in midclavicular line from T10. Modified Bromage scale was used to assess motor blockade. After spinal anesthesia, block assessment was done every 2 min until T10 dermatomal level and Bromage score of ‘3’ was achieved. After it assessment was done every 20 min till recovery of S2 dermatome (duration of the sensory block) and cessation of motor block. Secondary outcomes included comparison of hemodynamic parameters and adverse events if any. Hemodynamic instability was managed by a protocol including fluid administration, inj. mephentermine 5 mg bolus or inj. atropine 0.6 mg IV stat as required.
Descriptive statistics such as mean, median, range etc. were calculated for the study outcomes. Statistical comparison was made by applying sample t–test and chi-square test as applicable. A p < 0.05 was considered significant.
RESULTS
Out of 120 patients, 108 completed study successfully (Figure 1). Demographic profile and baseline hemodynamic parameters were comparable between two groups (Table 1).
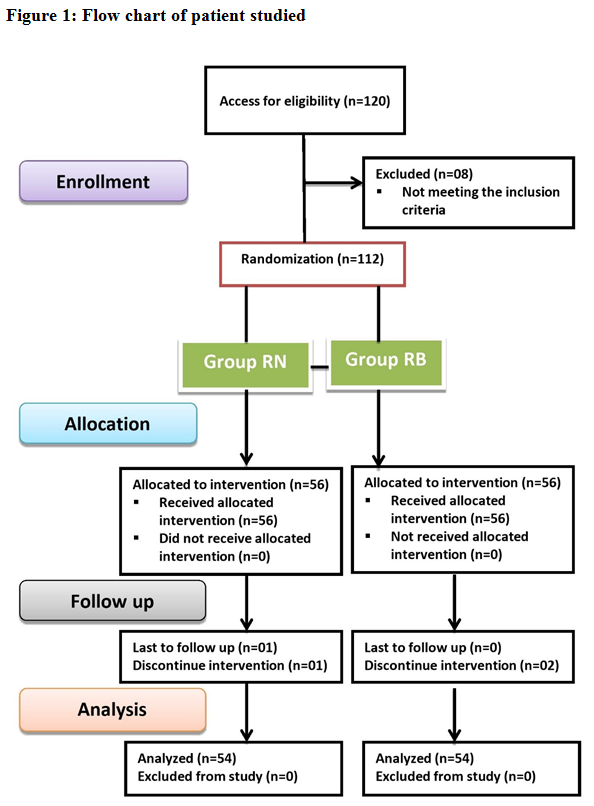
Table 1: Comparison of demographic data and baseline parameters between two groups [mean ± SD]
HR = Heart Rate; NIBP = Non-invasive mean blood pressure
Time of onset of sensory and motor block was earlier in group RN than group RB and this was significant between two groups (p < 0.05) (Table 2). Time required to reach median maximum height of sensory block was comparable between two groups (Table 2).
Table 2: Comparison of block characteristics and post op analgesia between two groups [mean ± SD]
Duration of sensory analgesia (The time required for sensory regression to S2 level) was significantly higher in group RN than group RB (394.62 ± 31.23 vs. 316.61 ± 28.81 min) (p < 0.001) (Table 2). Duration of motor block was more in group RN than group RB (226.63 ± 32.48 vs. 202.23 ± 22.58 min) and this was highly significant between two groups (p < 0.001) (Table 2).
Intra-operative and postoperative hemodynamic parameters were comparable between two groups. Observed side effects included bradycardia, hypotension, nausea and vomiting, sedation and shivering were comparable between the two groups (Table 3).
Table 3: Comparison of side effects between groups
DISCUSSION
Ropivacaine is a new long acting amide LA with lower risk of systemic and cardiotoxicity than bupivacaine. We conducted this trial to study the comparative efficacy of ropivacaine plus two of the adjuvants for major orthopedic lower limb surgeries as an alternative to bupivacaine. The use of adjuvants improves the intraoperative quality of anesthesia and postoperative analgesia. Studies have shown that intrathecal opioids can greatly enhance analgesia of sub-therapeutic doses of LA. We added nalbuphine and butorphanol to respective groups with ropivacaine to find out the duration of sensory analgesia and motor blockade. These drugs possess numerous pharmacologic similarities. They are both agonists of the kappa opioid receptor and partial agonists of the mu receptor. Both are equianalgesic (and nalbuphine is equipotent) with morphine parenterally and codeine orally.
Mean time of onset of sensory and motor block was significantly lower in nalbuphine group than butorphanol group. This is supported by study done by Fournier et al.13 They studied analgesic effects of intrathecal morphine 160 µg and nalbuphine 400 µg in geriatric patients scheduled for elective total hip replacement under continuous spinal anesthesia, given in the postoperative period in the recovery room, and concluded that administration of intrathecal nalbuphine resulted in a significantly faster onset of pain relief.
Our study demonstrated that duration of analgesia, sensory and motor blockade is significantly prolonged in nalbuphine group (group RN). In a randomized, double blind, controlled study done by Sapate et al.14 on adding intrathecal nalbuphine to bupivacaine for patients undergoing infraumblical surgeries, they concluded that intrathecal nalbuphine added to bupivacaine provided better quality of block and longer postoperative analgesia by 8–9 h than bupivacaine alone without any significant adverse effects. In a study by Tiwari et al.15 it was shown that addition of 0.4 mg nalbuphine significantly prolongs the duration of sensory block and postoperative analgesia.
Brockway MS et al.16 conducted a study comparing 0.5%, 0.75% and 1% ropivacaine with 0.5% and 0.75% bupivacaine. They found the mean upper limit of sensory block was T6. The above studies concluded that the highest level of sensory block was similar between nalbuphine group and butorphanol group. These findings are similar to our study.
In our study use of 500 µg nalbuphine and 100 µg butorphanol with ropivacaine resulted in moderate hypotension, requiring inj. mephentermine in both the groups after the intrathecal drug administration. Although mephentermine requirement was slightly higher in the nalbuphine group (8 in RN vs. 4 in RB), but they were not statistically significant.
LIMITATION
Our study had few limitations. First, we did not assess the surgeons’ or patients’ satisfaction for intrathecal nalbuphine and butorphanol. Second, the results may vary between different ethnical groups of population due to disparity in weight, height and subjective anesthetic drug sensitivity.
CONCLUSION
Both nalbuphine and butorphanol produce good postoperative analgesia without any significant adverse side effects, when used as adjuvants to isobaric 0.75% ropivacaine for spinal anesthesia in lower limb surgeries. Intrathecal nalbuphine was associated with early onset of sensory and motor block and significantly prolonged postoperative analgesia as compared to butorphanol.
Conflict of interest: Nil declared by the authors
Authors’ contribution: All authors took equal part in concept and design of the study, conduct of study, data collection, literature search, manuscript preparation and editing.
REFERENCES
Department of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University (IMS- BHU), Varanasi 22005. (India)
Akash Nirmal [talkwithakash@yahoo.com]
Yashpal Singh [dryashacin1999@rediffmail.com]
Sharad Kumar Mathur [skmathurbhu@gmail.com]
Satish Patel [doc.satish.patel@gmail.com]
Correspondence: Dr Yashpal Singh, Dept. of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University (IMS- BHU), Varanasi-221005, UP, (India);
E-mail: dryashacin1999@rediffmail.com; Phone: +919918424416
Received: 22 August 2019;
Reviewed: 8, 9 October 2019; 6, 7 November 2019;
Revised: 18 November 2019;
Reviewed: 19 November 2019;
Accepted: 20 November 2019
ABSTRACT
Background: Intrathecal ropivacaine is now routinely used for lower limb surgery. Adjuvants e.g. fentanyl, dexmedetomidine or morphine etc. are commonly used to prolong the intraoperative anesthesia or postoperative analgesia. The available literature lacks information on use of butorphanol and nalbuphine as adjuvants with 0.75% isobaric ropivacaine. We aimed to compare nalbuphine and butorphanol as adjuvant with isobaric ropivacaine in lower limb orthopedic surgeries.
Methodology: After institutional ethical committee approval and informed written consent, a total of 108 patients of ages between 18 to 65 y, of either sex, American Society of Anesthesiologists (ASA) grade ӏ & ӏӏ, scheduled for elective lower limb orthopedic surgeries, were enrolled and randomly allocated into two groups: Group RN; to receive isobaric ropivacaine (0.75%, 7.5 mg/ml) 2.5 ml plus nalbuphine 500 µg (0.5 ml), and Group RB; to receive isobaric ropivacaine 2.5 ml plus butorphanol 100 µg (0.5 ml) intrathecally. Primary outcome measure was the duration of sensory‑motor blockade from the time of intrathecal drug administration. Statistical analysis was performed by using t-test and chi-square test as applicable. A p < 0.05 was considered as significant.
Results: Duration of sensory (p < 0.001) and motor blockade (p = 0.02) was significantly prolonged in nalbuphine group than butorphanol group. Onset of blockade was earlier in nalbuphine group. Duration of motor block and sensory analgesia was prolonged in group RN (p < 0.001). Perioperative hemodynamic parameters and the observed side effects including bradycardia, hypotension, nausea and vomiting, sedation and shivering were comparable between the two groups (p = 0.77).
Conclusion: Intrathecal nalbuphine produces prolonged motor blockade as well as postoperative analgesia than intrathecal butorphanol when used as adjuvants to isobaric 0.75% ropivacaine.
Key words: Nalbuphine; Butorphanol; Postoperative analgesia
Citation: Nirmal A, Singh Y, Mathur SK, Patel S. Comparison between intrathecal nalbuphine and butorphanol as adjuvants to isobaric ropivacaine in elective lower limb orthopedic surgeries: A prospective, randomized, double blind study. Anaesth pain & intensive care 2019;23(4):382-386.
DOI: 10.35975/apic.v23i4.1171
INTRODUCTION
With advancement in drugs and technique, spinal anesthesia is now gold standard in lower limb orthopedic surgery. Various studies have clearly demonstrated advantage of neuraxial anesthesia in term of significant reduction in mortality and morbidity in comparison to general anesthesia.1 For the last many years local anesthetic (LA) bupivacaine has been used for spinal anesthesia due to its intense block characteristics. Now-a-days, bupivacaine is slowly being replaced by newer LA including ropivacaine in lower limb and lower abdominal surgeries.2-5 Ropivacaine is a long acting amide LA, structurally very similar to other pipecoloxylidides, first synthesized by Ekenstam.6 It is a pure s-enantiomer having less motor blockade and reduced cardiotoxicity which favors its attractiveness.
Various adjuvants have been tried to improve efficacy, duration of action and safety of LAs, but opioids are the most desired due to its prolonged analgesic action. Fentanyl, morphine, buprenorphine, butorphanol, midazolam, clonidine and dexmedetomidine have been used as adjuvants.7,8 Nalbuphine is an opioid, potent analgesic, structurally related to oxymorphone. It is highly lipid soluble with agonist action at κ-receptor and an antagonist activity at µ-receptor. There have been studies of neuraxial administration of nalbuphine, shown to produce significant analgesia with minimal respiratory depression.9,10 There were safety issues regarding intrathecal uses of nalbuphine; however none of the abnormalities had been encountered through all these years and it was found to be safe for neuraxial blockade. Butorphanol is morphine type synthetic opioid analgesic and structurally related to levorphanol. It acts as an agonist on κ and mixed agonist-antagonist action at µ-opioid receptors. It has been shown to improve the analgesic duration of LA and helps in decreasing analgesic utilization.11-12
Review of literature on nalbuphine and butorphanol with isobaric ropivacaine in adult patients is scarce. So we planned this study to compare nalbuphine and butorphanol with intrathecal isobaric ropivacaine in elective lower limb orthopedic surgeries. Primary outcome of our study was a comparison of block characteristics and duration of postoperative analgesia. Secondary outcomes includes comparison of hemodynamic parameters and adverse events, if any.
METHODOLOGY
After institutional ethical approval and written informed consent, this prospective, randomized, double blind, interventional clinical study was conducted at SS Hospital and Trauma Centre, Institute of Medical Sciences, Banaras Hindu University (IMS-BHU) Varanasi, during academic year 2015-17. Patients with a history of hypersensitivity to study drugs, general contraindications to spinal anesthesia, morbid obesity and end organ damage were excluded.
A total of 108 patients of ages between 18 to 65 y, of either sex, American Society of Anesthesiologists (ASA) grade ӏ & ӏӏ, scheduled for elective lower limb orthopedic surgeries, were randomly allocated into two groups: Group RN; to receive isobaric ropivacaine (0.75%, 7.5 mg/ml) 2.5 ml plus nalbuphine 500 µg (0.5 ml), and Group RB; to receive isobaric ropivacaine 2.5 ml plus butorphanol 100 µg (0.5 ml) intrathecally. Randomization was performed by an anesthesiologist involved in studied drug preparation. Further procedure and the monitoring were performed by another investigator unaware of group allocation. Patients were also blinded to the drug regimen utilized for spinal anesthesia. In the sitting position under standard aseptic precautions, lumbar puncture was performed at L3‑L4 intervertebral space in midline approach by 25 gauge Quincke spinal needle. The studied drug solution was injected over a period of 10–15 sec after the confirmation of free flow of CSF and patients were turned to the supine position.
Primary outcome measure was the duration of sensory‑motor blockade from the time of intrathecal drug administration. Sensory level was assessed by pin prick method bilaterally in midclavicular line from T10. Modified Bromage scale was used to assess motor blockade. After spinal anesthesia, block assessment was done every 2 min until T10 dermatomal level and Bromage score of ‘3’ was achieved. After it assessment was done every 20 min till recovery of S2 dermatome (duration of the sensory block) and cessation of motor block. Secondary outcomes included comparison of hemodynamic parameters and adverse events if any. Hemodynamic instability was managed by a protocol including fluid administration, inj. mephentermine 5 mg bolus or inj. atropine 0.6 mg IV stat as required.
Descriptive statistics such as mean, median, range etc. were calculated for the study outcomes. Statistical comparison was made by applying sample t–test and chi-square test as applicable. A p < 0.05 was considered significant.
RESULTS
Out of 120 patients, 108 completed study successfully (Figure 1). Demographic profile and baseline hemodynamic parameters were comparable between two groups (Table 1).
Table 1: Comparison of demographic data and baseline parameters between two groups [mean ± SD]
| Parameters | Group RN | Group RB | p value | |
| Age | 39.25 ±15.06 | 38.33 ± 14.92 | 0.85 | |
| Weight | 61.48 ± 7.64 | 62.54 ± 6.00 | 0.43 | |
| Sex | Male (n) | 14 | 16 | 0.85 |
| Female (n) | 38 | 40 | ||
| Baseline HR | 77.96 ± 4.024 | 79.11 ± 5.83 | 0.24 | |
| Baseline NIBP | 112.58 ± 10.30 | 113.66 ± 10.18 | 0.58 | |
Time of onset of sensory and motor block was earlier in group RN than group RB and this was significant between two groups (p < 0.05) (Table 2). Time required to reach median maximum height of sensory block was comparable between two groups (Table 2).
Table 2: Comparison of block characteristics and post op analgesia between two groups [mean ± SD]
| Parameters | Group RN | Group RB | p value |
| Time of onset of sensory block | 3.07 ± 1.06 | 3.79 ± 0.95 | < 0.001 |
| Time of onset of motor block | 6.37 ± 1.73 | 7.06 ± 1.31 | 0.02 |
| Highest level of sensory block | T6-T7 | T6-T7 | |
| Duration of motor block | 226.63 ± 32.48 | 202.23 ± 22.58 | < 0.001 |
| Duration of sensory analgesia | 394.62 ± 31.23 | 316.61 ± 28.81 | < 0.001 |
Intra-operative and postoperative hemodynamic parameters were comparable between two groups. Observed side effects included bradycardia, hypotension, nausea and vomiting, sedation and shivering were comparable between the two groups (Table 3).
Table 3: Comparison of side effects between groups
| Parameters | Group RN | Group RB | p value | ||
| No | % | No. | % | ||
| Bradycardia | 4 | 7.7% | 5 | 8.9% | 0.77 |
| Hypotension | 8 | 15.4% | 5 | 8.9% | |
| Nausea | 4 | 7.7% | 7 | 12.5% | |
| Sedation | 1 | 1.9% | 1 | 1.8% | |
| Shivering | 4 | 7.7% | 2 | 3.6% | |
Ropivacaine is a new long acting amide LA with lower risk of systemic and cardiotoxicity than bupivacaine. We conducted this trial to study the comparative efficacy of ropivacaine plus two of the adjuvants for major orthopedic lower limb surgeries as an alternative to bupivacaine. The use of adjuvants improves the intraoperative quality of anesthesia and postoperative analgesia. Studies have shown that intrathecal opioids can greatly enhance analgesia of sub-therapeutic doses of LA. We added nalbuphine and butorphanol to respective groups with ropivacaine to find out the duration of sensory analgesia and motor blockade. These drugs possess numerous pharmacologic similarities. They are both agonists of the kappa opioid receptor and partial agonists of the mu receptor. Both are equianalgesic (and nalbuphine is equipotent) with morphine parenterally and codeine orally.
Mean time of onset of sensory and motor block was significantly lower in nalbuphine group than butorphanol group. This is supported by study done by Fournier et al.13 They studied analgesic effects of intrathecal morphine 160 µg and nalbuphine 400 µg in geriatric patients scheduled for elective total hip replacement under continuous spinal anesthesia, given in the postoperative period in the recovery room, and concluded that administration of intrathecal nalbuphine resulted in a significantly faster onset of pain relief.
Our study demonstrated that duration of analgesia, sensory and motor blockade is significantly prolonged in nalbuphine group (group RN). In a randomized, double blind, controlled study done by Sapate et al.14 on adding intrathecal nalbuphine to bupivacaine for patients undergoing infraumblical surgeries, they concluded that intrathecal nalbuphine added to bupivacaine provided better quality of block and longer postoperative analgesia by 8–9 h than bupivacaine alone without any significant adverse effects. In a study by Tiwari et al.15 it was shown that addition of 0.4 mg nalbuphine significantly prolongs the duration of sensory block and postoperative analgesia.
Brockway MS et al.16 conducted a study comparing 0.5%, 0.75% and 1% ropivacaine with 0.5% and 0.75% bupivacaine. They found the mean upper limit of sensory block was T6. The above studies concluded that the highest level of sensory block was similar between nalbuphine group and butorphanol group. These findings are similar to our study.
In our study use of 500 µg nalbuphine and 100 µg butorphanol with ropivacaine resulted in moderate hypotension, requiring inj. mephentermine in both the groups after the intrathecal drug administration. Although mephentermine requirement was slightly higher in the nalbuphine group (8 in RN vs. 4 in RB), but they were not statistically significant.
LIMITATION
Our study had few limitations. First, we did not assess the surgeons’ or patients’ satisfaction for intrathecal nalbuphine and butorphanol. Second, the results may vary between different ethnical groups of population due to disparity in weight, height and subjective anesthetic drug sensitivity.
CONCLUSION
Both nalbuphine and butorphanol produce good postoperative analgesia without any significant adverse side effects, when used as adjuvants to isobaric 0.75% ropivacaine for spinal anesthesia in lower limb surgeries. Intrathecal nalbuphine was associated with early onset of sensory and motor block and significantly prolonged postoperative analgesia as compared to butorphanol.
Conflict of interest: Nil declared by the authors
Authors’ contribution: All authors took equal part in concept and design of the study, conduct of study, data collection, literature search, manuscript preparation and editing.
REFERENCES
- Basques BA, Toy JO, Bohl DD, Golinvaux NS, Grauer JN. General compared with spinal anesthesia for total hip arthroplasty. J Bone Joint Surg Am. 2015;97(6):455-61. [PubMed] DOI: 2106/JBJS.N.00662
- McNamee DA, Parks L, McClelland AM, Scott S, Milligan KR, Ahlén K, et al. Intrathecal ropivacaine for total hip arthroplasty: double-blind comparative study with isobaric 7.5 mg/ml and 10 mg/ml solutions. Br J Anaesth. 2001;87:743–7. [PubMed] DOI: 1093/bja/87.5.743
- Kallio H, Snall EVT, Tuomas CA, Rosenberg PH. Comparison of hyperbaric and plain ropivacaine 15 mg in spinal anaesthesia for lower limb surgery. Br J Anaesth. 2004;93(5):664–9. [PubMed] DOI: 1093/bja/aeh257
- Mantouvalou M, Ralli S, Arnaoutoglou H, Tziris G, Papadopoulos G. Spinal anesthesia: comparison of plain ropivacaine, bupivacaine and levobupivacaine for lower abdominal surgery. Acta Anaesthesiol Belg. 2008;59(2):65-71. [PubMed]
- Danelli G, Fanelli G, Berti M, Cornini A, Lacava L, Nuzzi M and et al. Spinal ropivacaine or bupivacaine for caesarean delivery: A prospective, randomized, doubleblind comparison. Reg Anesth Pain Med. 2004;29(3):221–6. [PubMed] DOI: 1016/j.rapm.2004.02.003
- Ekenstam AF, Petersson G, Egner B. Local anaesthetics: I. N- alkyl pyrrolodine and N-alkyl piperidine carboxylic amides. Acta Chem Sand. 1957;2:1183-90. DOI: 3891/acta.chem.scand.11-1183
- Forster JG, Rosenberg PH, Clinically useful adjuvants in regional anaesthesia, Curr Opin Anaesthesiol. 2003;16(5):477-86. [PubMed] DOI: 1097/00001503-200310000-00007
- Singh AK, Singh Y, Jain G, Verma RK. Comparison of two different doses of intrathecal dexmedetomidine as adjuvant with isobaric ropivacaine in lower abdominal surgery. Anesth Essays Res. 2015;9:343-47. [PubMed] DOI: 4103/0259-1162.158009
- Mukherjee A, Pal A, Agrawal J, Mehrotra A, Dawar N. Intrathecal nalbuphine as an adjuvant to subarachnoid block: what is the most effective dose? Anesth Essays Res. 2011;5:171-5. [PubMed] DOI: 4103/0259-1162.94759
- Shakooh S, Bhosle P. Intrathecal nalbuphine: An effective adjuvant for post-operative analgesia. Innovative J Med Health Sci. 2004;4:79-82. [Free Full Text]
- Singh V, Gupta LK, Singh GP. Comparison among intrathecal fentanyl and butorphanol in combination with bupivacaine for lower limb surgeries. J Anesth Clin Pharmacol. 2006;22(4):371–5. [Free Full Text]
- Bhagwat S, Sanjay N. Postoperative analgesia: A comparative study of epidural butorphanol and epidural tramadol. J Adv Res Biol Sci. 2011;3:86–9.
- Fournier R, Gamulin Z, Macksay M, Van Gessel E. Intrathecal morphine versus nalbuphine for post-operative pain relief after total hip replacement. Anesthesiology. 1998;89:867.
- Sapate M, Sahu P, Thatte WS, Dubey R. A randomized, double blind, control study of the effects of adding nalbuphine to spinal bupivacaine for lower abdominal surgeries in elderly patients. Anaesth. Pain Intensive Care 2013;17(2):145-8. [Free Full Text]
- Tiwari AK, Tomar GS, Agrawal J. Intrathecal bupivacaine in comparison with a combination of nalbuphine and bupivacaine for subarachnoid block: A randomized prospective double blind clinical study. Am. J Ther. 2013;20(6):592-5. [PubMed] DOI: 1097/MJT.0b013e31822048db
- Brockway MS, Bannister J, McClure JH, McKeown D, Wildsmith JA. Comparison of extradural ropivacaine and bupivacaine. Br J Anaesth. 1991;66(1):31-7. [PubMed] DOI: 1093/bja/66.1.31